Clinical Relevance of Serum Galactose Deficient IgA1 in Patients with IgA Nephropathy

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Clinical and Pathological Parameters
2.3. Measurement of Serum Gd-IgA1
2.4. Treatment and Clinical Outcome
2.5. Statistical Analysis
3. Results
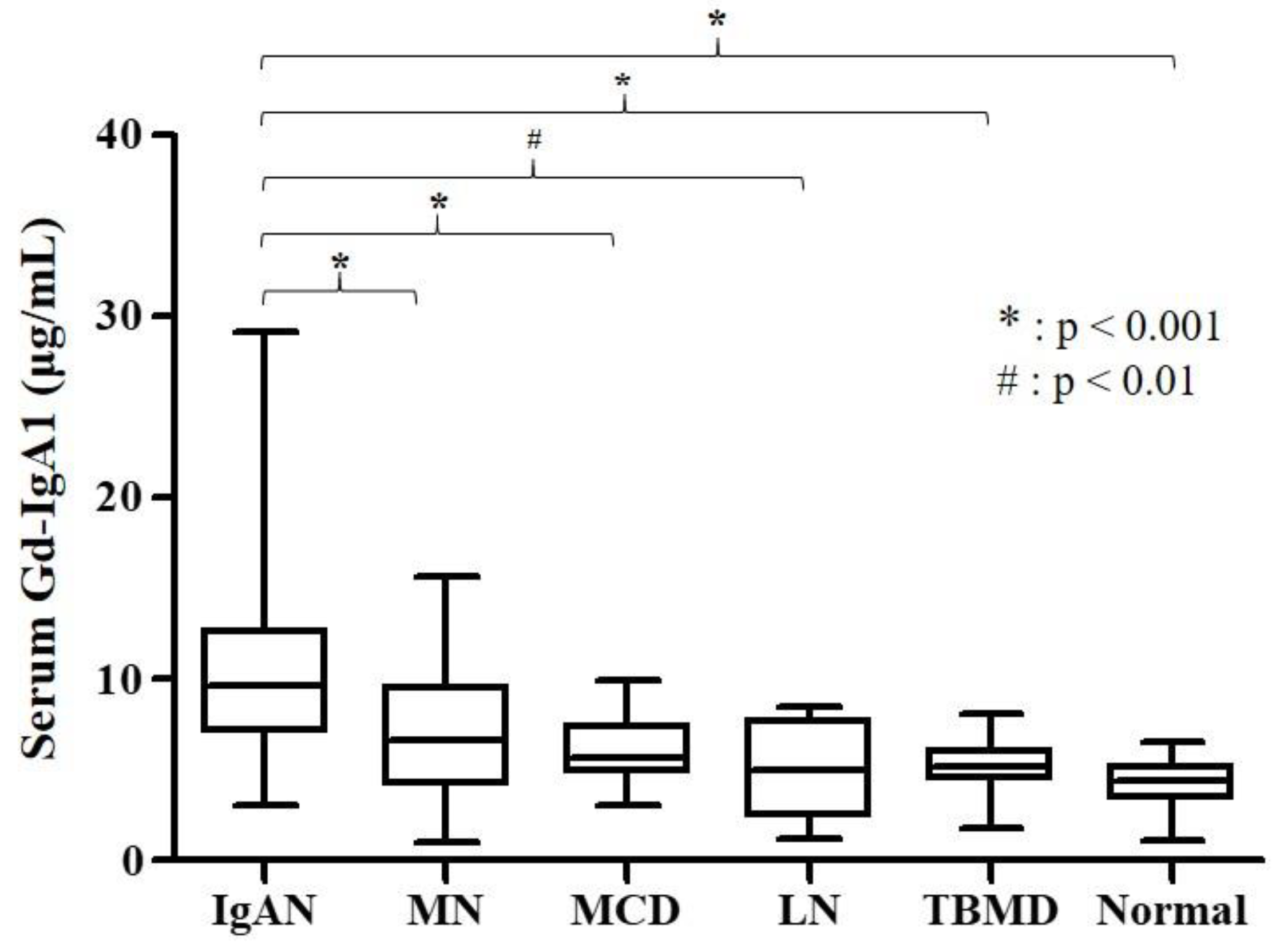
3.1. Baseline Characteristics of Study Population
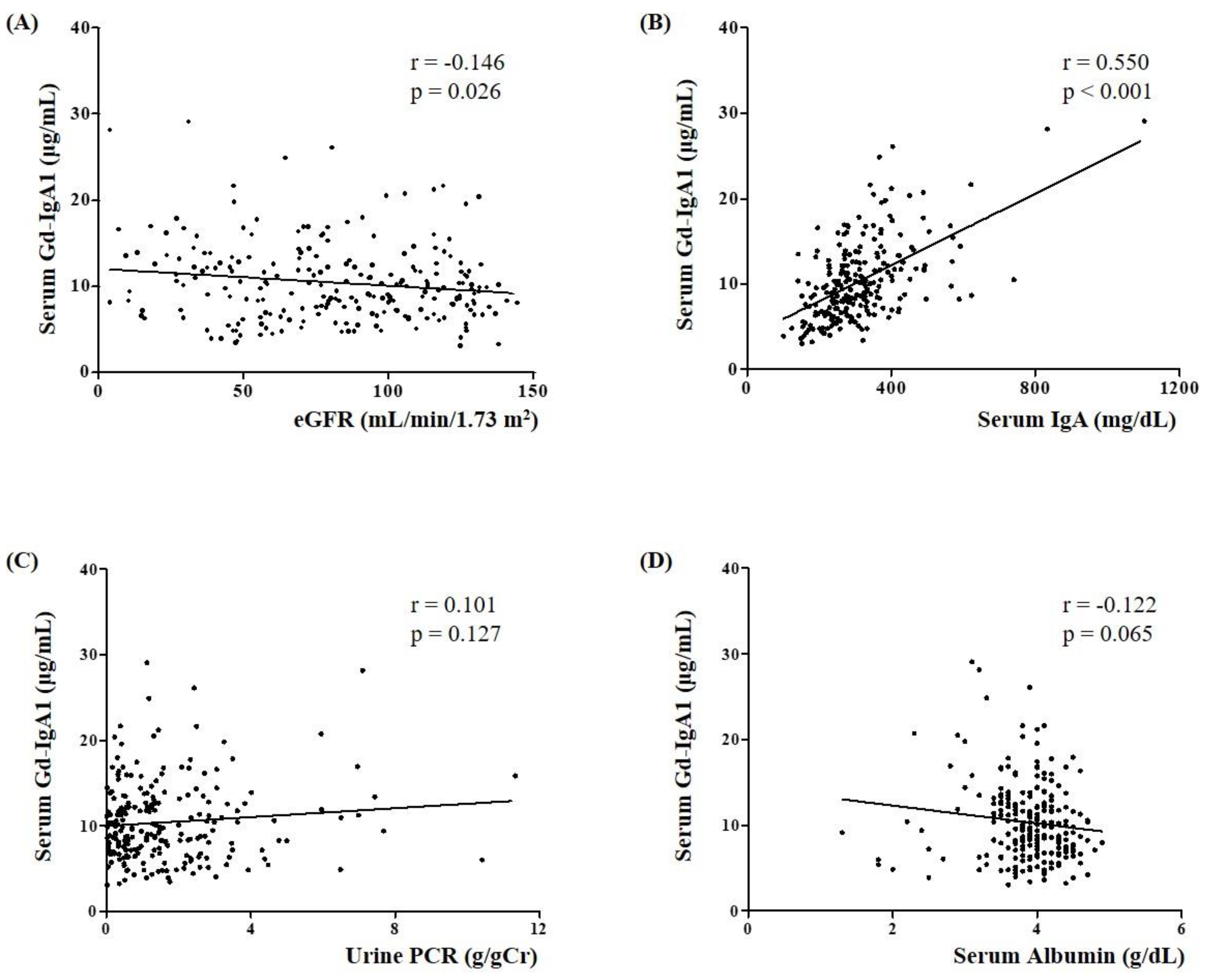
3.2. Association of Serum Gd-IgA1 Level with Clinical and Pathological Parameters in IgAN Patients
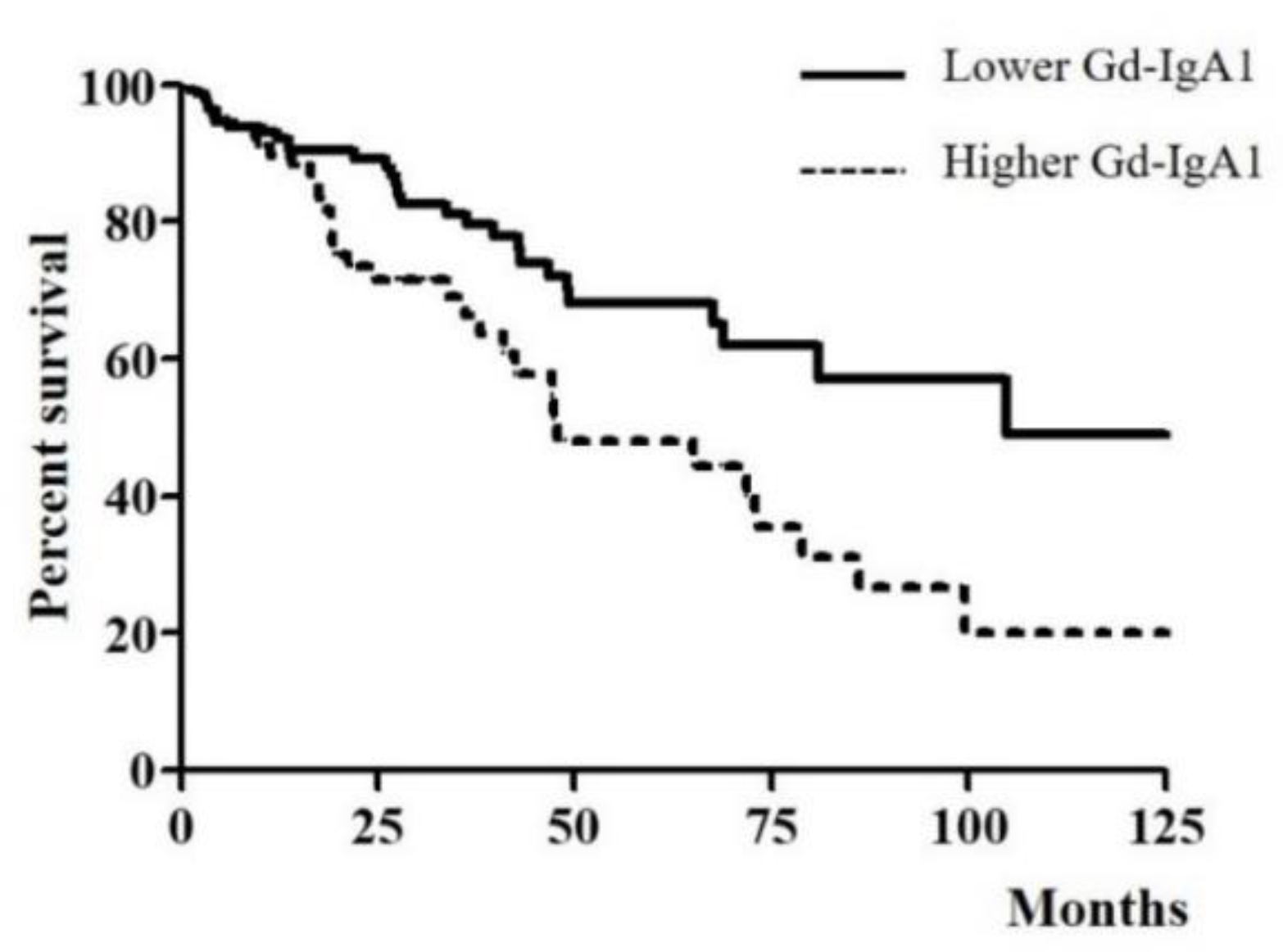
3.3. Association of Serum Gd-IgA1 Level and CKD Progression in IgAN Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wyatt, R.J.; Julian, B.A. IgA nephropathy. N. Engl. J. Med. 2013, 368, 2402–2414. [Google Scholar] [CrossRef] [PubMed]
- Berthoux, F.C.; Mohey, H.; Afiani, A. Natural history of primary IgA nephropathy. Semin. Nephrol. 2008, 28, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Barratt, J.; Feehally, J. IgA nephropathy. J. Am. Soc. Nephrol. 2005, 16, 2088–2097. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H. Biomarkers for IgA nephropathy on the basis of multi-hit pathogenesis. Clin. Exp. Nephrol. 2019, 23, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Schena, F.P.; Cox, S.N. Biomarkers and Precision Medicine in IgA Nephropathy. Semin. Nephrol. 2018, 38, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.C.; Harper, S.J.; Feehally, J. Galactosylation of N- and O-linked carbohydrate moieties of IgA1 and IgG in IgA nephropathy. Clin. Exp. Immunol. 1995, 100, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Coppo, R.; Amore, A. Aberrant glycosylation in IgA nephropathy (IgAN). Kidney Int. 2004, 65, 1544–1547. [Google Scholar] [CrossRef]
- Moldoveanu, Z.; Wyatt, R.J.; Lee, J.Y.; Tomana, M.; Julian, B.A.; Mestecky, J.; Huang, W.Q.; Anreddy, S.R.; Hall, S.; Hastings, M.C.; et al. Patients with IgA nephropathy have increased serum galactose-deficient IgA1 levels. Kidney Int. 2007, 71, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Kiryluk, K.; Novak, J.; Moldoveanu, Z.; Herr, A.B.; Renfrow, M.B.; Wyatt, R.J.; Scolari, F.; Mestecky, J.; Gharavi, A.G.; et al. The pathophysiology of IgA nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1795–1803. [Google Scholar] [CrossRef]
- Zhang, K.; Li, Q.; Zhang, Y.; Shang, W.; Wei, L.; Li, H.; Gao, S.; Yan, T.; Jia, J.; Liu, Y.; et al. Clinical Significance of Galactose-Deficient IgA1 by KM55 in Patients with IgA Nephropathy. Kidney Blood Press. Res. 2019, 44, 1196–1206. [Google Scholar] [CrossRef]
- Wada, Y.; Matsumoto, K.; Suzuki, T.; Saito, T.; Kanazawa, N.; Tachibana, S.; Iseri, K.; Sugiyama, M.; Iyoda, M.; Shibata, T. Clinical significance of serum and mesangial galactose-deficient IgA1 in patients with IgA nephropathy. PLoS ONE 2018, 13, e0206865. [Google Scholar] [CrossRef]
- Bagchi, S.; Lingaiah, R.; Mani, K.; Barwad, A.; Singh, G.; Balooni, V.; Bhowmik, D.; Agarwal, S.K. Significance of serum galactose deficient IgA1 as a potential biomarker for IgA nephropathy: A case control study. PLoS ONE 2019, 14, e0214256. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Trimarchi, H.; Barratt, J.; Cattran, D.C.; Cook, H.T.; Coppo, R.; Haas, M.; Liu, Z.H.; Roberts, I.S.; Yuzawa, Y.; Zhang, H.; et al. Oxford Classification of IgA nephropathy 2016: An update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017, 91, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef]
- Berger, J.; Hinglais, N. Intercapillary deposits of IgA-IgG. J. Urol. Nephrol. 1968, 74, 694–695. [Google Scholar]
- Hastings, M.C.; Moldoveanu, Z.; Suzuki, H.; Berthoux, F.; Julian, B.A.; Sanders, J.T.; Renfrow, M.B.; Novak, J.; Wyatt, R.J. Biomarkers in IgA nephropathy: Relationship to pathogenetic hits. Expert Opin. Med. Diagn. 2013, 7, 615–627. [Google Scholar] [CrossRef]
- Moriyama, T. Clinical and histological features and therapeutic strategies for IgA nephropathy. Clin. Exp. Nephrol. 2019, 23, 1089–1099. [Google Scholar] [CrossRef]
- Lafayette, R.A.; Kelepouris, E. Immunoglobulin A Nephropathy: Advances in Understanding of Pathogenesis and Treatment. Am. J. Nephrol. 2018, 47 (Suppl. S1), 43–52. [Google Scholar] [CrossRef]
- Zhao, N.; Hou, P.; Lv, J.; Moldoveanu, Z.; Li, Y.; Kiryluk, K.; Gharavi, A.G.; Novak, J.; Zhang, H. The level of galactose-deficient IgA1 in the sera of patients with IgA nephropathy is associated with disease progression. Kidney Int. 2012, 82, 790–796. [Google Scholar] [CrossRef]
- Xu, L.X.; Zhao, M.H. Aberrantly glycosylated serum IgA1 are closely associated with pathologic phenotypes of IgA nephropathy. Kidney Int. 2005, 68, 167–172. [Google Scholar] [CrossRef][Green Version]
- Lai, K.N.; Chan, L.Y.; Leung, J.C. Mechanisms of tubulointerstitial injury in IgA nephropathy. Kidney Int. 2005, 67, S110–S115. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.C.K.; Lai, K.N.; Tang, S.C.W. Role of Mesangial-Podocytic-Tubular Cross-Talk in IgA Nephropathy. Semin. Nephrol. 2018, 38, 485–495. [Google Scholar] [CrossRef]
- Yasutake, J.; Suzuki, Y.; Suzuki, H.; Hiura, N.; Yanagawa, H.; Makita, Y.; Kaneko, E.; Tomino, Y. Novel lectin-independent approach to detect galactose-deficient IgA1 in IgA nephropathy. Nephrol. Dial. Transplant. 2015, 30, 1315–1321. [Google Scholar] [CrossRef]
- Suzuki, H.; Yasutake, J.; Makita, Y.; Tanbo, Y.; Yamasaki, K.; Sofue, T.; Kano, T.; Suzuki, Y. IgA nephropathy and IgA vasculitis with nephritis have a shared feature involving galactose-deficient IgA1-oriented pathogenesis. Kidney Int. 2018, 93, 700–705. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| IgAN (n = 230) | MN (n = 35) | MCD (n = 21) | LN (n = 8) | TBMD (n = 10) | Heathy Controls (n = 15) | |
|---|---|---|---|---|---|---|
| Age (years) | 41.00 (31.00–52.00) b | 53.00 (41.25–63.75) a | 48.00 (21.00–62.00) | 44.00 (22.00–53.00) | 40.00 (20.50–46.50) b | 25.00 (21.75–50.50) b |
| Male (n, %) | 115 (50.0%) | 23 (65.7%) | 13 (61.9%) | 0 (0.0%) | 5 (50.0%) | 12 (80.0%) |
| BMI (kg/m2) | 23.50 (21.28–25.68) | 23.19 (22.12–24.28) | 25.20 (21.79–28.25) | 21.75 (19.90–22.47) | 23.29 (21.75–24.77) | 22.32 (20.95–24.23) |
| Albumin (g/dL) | 3.90 (3.60–4.20) b,c,d,f | 3.35 (2.57–4.10) a,c,e,f | 2.20 (1.90–2.40) a,b,e,f | 2.90(2.22–3.60) a,e,f | 4.50(4.15–4.65) b,c,d | 4.60 (4.33–4.73) a,b,c,d |
| Creatinine (mg/dL) | 0.94 (0.74–1.38) | 0.80 (0.60–1.03) | 0.90 (0.70–1.45) | 0.60 (0.56–1.87) | 0.73 (0.55–0.85) | 0.76 (0.67–0.99) |
| eGFR (mL/min/1.73 m2) | 84.18 (52.50–113.91) e | 90.90 (77.91–115.59) | 85.32 (53.20–112.16) | 110.89 (31.06–132.90) | 121.75 (110.69–130.39) a | 125.29 (87.29–137.78) |
| C3 (mg/dL) | 107.00 (92.00–121.00) d | 112.00 (95.52–125.25) d | 114.00 (105.50–129.00) d | 45.95 (32.83–56.75) a,b,c,e,f | 97.40 (89.45–105.00) d | 102.00 (84.07–111.25) d |
| IgA (mg/dL) | 287.0 (240.00–361.50) e,f | 214.00 (175.50–283.75) | 264.00 (220.00–353.00) | 264.00 (220.00–353.00) | 177.00 (151.00–199.50) a | 171.00 (124.00–204.50) a |
| Urine PCR (g/gCr) | 1.24 (0.46–2.34) b,c | 3.89 (1.64–6.22) a,c,e,f | 8.63 (4.81–13.95) a,b,d,e,f | 2.28 (0.62–4.09) c | 0.60 (0.03–0.63) b,c | 0.04 (0.19–0.07) b,c |
| Urine RBC grade | ||||||
| <5/HPF | 45 (19.6%) | 17 (48.6%) | 12 (57.1%) | 1 (12.5%) | 1 (10.0%) | – |
| 5–9/HPF | 30 (13.0%) | 6 (17.1%) | 6 (28.6%) | 2 (25.0%) | 3 (30.0%) | – |
| 10–29/HPF | 59 (25.7%) | 6 (17.1%) | 1 (4.8%) | 2 (25.0%) | 5 (50.0%) | – |
| ≥30/HPF | 96 (41.7%) | 6 (17.1%) | 2 (9.5%) | 3 (37.5%) | 1 (10.0%) | – |
| Serum Gd–IgA1 (μg/mL) | 9.66 (7.14–12.60)b,c,d,e,f | 6.65 (4.21–9.51) a | 5.60 (4.86–7.38) a | 4.95 (2.40–7.71) a | 5.19 (4.71–6.16) a | 4.43 (3.44–5.15) a |
| Oxford Classification | n (%) | Serum Gd-IgA1 (μg/mL) | p | |
|---|---|---|---|---|
| M | 0 | 135 (58.7%) | 8.77 (6.64–12.17) | 0.414 |
| 1 | 95 (41.3%) | 10.57 (7.94–13.46) | ||
| E | 0 | 174 (76.5%) | 9.41 (7.12–13.29) | 0.898 |
| 1 | 56 (23.5%) | 9.91 (7.61–12.17) | ||
| S | 0 | 167 (72.6%) | 9.73 (7.19–12.47) | 0.672 |
| 1 | 63 (27.4%) | 9.42 (7.12–12.95) | ||
| T | 0 | 193 (83.9%) | 9.15 (6.93–12.18) | 0.024 |
| 1,2 | 37 (16.1%) | 10.93 (8.45–16.69) | ||
| C | 0 | 170 (73.9%) | 9.89 (7.19–13.00) | 0.268 |
| 1,2 | 60 (26.1%) | 8.69 (6.22–12.16) |
| Lower Gd-IgA1 (<11.31 μg/mL) n = 148 | Higher Gd-IgA1 (≥11.31 μg/mL) n = 82 | p | |
|---|---|---|---|
| Age (years) | 40.00 (26.50–52.00) | 42.00 (34.00–49.00) | 0.238 |
| Male (n, %) | 74 (50%) | 41 (50%) | 0.999 |
| BMI (kg/m2) | 23.50 (21.16–25.71) | 23.44 (21.48–25.65) | 0.794 |
| Serum albumin (g/dL) | 4.00 (3.70–4.30) | 3.80 (3.50–4.10) | 0.012 |
| Serum creatinine (mg/dL) | 0.90 (0.74–1.19) | 1.10 (0.80–1.70) | 0.001 |
| eGFR (mL/min/1.73 m2) | 92.96 (59.44–118.15) | 72.59 (41.83–108.38) | 0.001 |
| C3 (mg/dL) | 107.00 (95.05–120.50) | 107.0 (92.00–423.00) | 0.478 |
| Serum IgA (mg/dL) | 269.00 (228.50–324.00) | 354.0 (278.00–423.00) | <0.001 |
| Urine PCR (g/gCr) | 1.11 (0.36–2.33) | 1.22 (0.51–2.44) | 0.337 |
| Prior medications (n, %) | |||
| ARB or ACEi | 33 (22.3%) | 22 (26.8%) | 0.440 |
| CCB | 23 (15.5%) | 9 (11.0%) | 0.226 |
| Beta blocker | 6 (4.1%) | 3 (3.7%) | 0.593 |
| Statin | 10 (6.8%) | 5 (6.1%) | 0.543 |
| Urine RBC grade (n, %) | 0.867 | ||
| <5/HPF | 28 (18.9%) | 17 (20.7%) | |
| 5–9/HPF | 21 (14.2%) | 9 (11.0%) | |
| 10–29/HPF | 39 (26.4%) | 20 (24.4%) | |
| ≥30/HPF | 60; (40.5%) | 36 (43.9%) | |
| Serum Gd–IgA1 (μg/mL) | 7.95 (6.23–9.36) | 13.84 (12.44–16.73) | <0.001 |
| Therapeutic strategies (n, %) | |||
| ARB or ACEi | 103 (69.6%) | 57 (69.5%) | 0.990 |
| Immunosuppressant | 28 (55.4%) | 46 (56.1%) | 0.515 |
| Follow–up duration (months) | 22.55 (11.68–45.83) | 22.41 (13.05–42.32) | 0.998 |
| CKD progression | 31 (20.9%) | 33 (40.2%) | 0.002 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age (years) | 1.029 (1.012–1.046) | 0.001 | 1.016 (0.996–1.035) | 0.111 |
| Male (vs. Female) | 1.076 (0.659–1.759) | 0.769 | ||
| BMI (kg/m2) | 0.997 (0.921–1.079) | 0.939 | ||
| eGFR (mL/min/1.73 m2) | 0.985 (0.978–0.991) | <0.001 | 0.991 (0.982–0.999) | 0.048 |
| Urine PCR(g/g) | 1.191 (1.081–1.313) | <0.001 | 1.116 (0.991–1.256) | 0.070 |
| Prior medications | ||||
| ARB or ACEi | 1.587 (00.903–2.789) | 0.109 | ||
| CCB | 1.420 (0.698–2.888) | 0.333 | ||
| Beta blocker | 2.540 (0.783–8.268) | 0.120 | ||
| Statin | 1.070 (0.333–3.438) | 0.909 | ||
| Oxford classification | ||||
| M | 1.226 (0.747–2.012) | 0.420 | ||
| S | 1.502 (0.885–2.550) | 0.132 | ||
| E | 1.340 (0.733–2.451) | 0.341 | ||
| T | 1.698 (0.955–3.018) | 0.071 | 1.151 (0.614–2.158) | 0.661 |
| C | 1.532 (0.870–2.699) | 0.140 | ||
| Therapeutic strategies | ||||
| ARB or ACEi | 1.523 (0.857–2.706) | 0.151 | ||
| Immunosuppressant | 1.344 (0.796–2.269) | 0.268 | ||
| Lower serum Gd–IgA1 level | 1 | |||
| Higher serum Gd–IgA1 level | 2.283 (1.388–3.756) | 0.001 | 1.933 (1.164–3.208) | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.S.; Hwang, H.S.; Lee, S.H.; Kim, Y.G.; Moon, J.-Y.; Kong, J.Y.; Jeong, K.H. Clinical Relevance of Serum Galactose Deficient IgA1 in Patients with IgA Nephropathy. J. Clin. Med. 2020, 9, 3549. https://doi.org/10.3390/jcm9113549
Kim JS, Hwang HS, Lee SH, Kim YG, Moon J-Y, Kong JY, Jeong KH. Clinical Relevance of Serum Galactose Deficient IgA1 in Patients with IgA Nephropathy. Journal of Clinical Medicine. 2020; 9(11):3549. https://doi.org/10.3390/jcm9113549
Chicago/Turabian StyleKim, Jin Sug, Hyeon Seok Hwang, Sang Ho Lee, Yang Gyun Kim, Ju-Young Moon, Ji Yoon Kong, and Kyung Hwan Jeong. 2020. "Clinical Relevance of Serum Galactose Deficient IgA1 in Patients with IgA Nephropathy" Journal of Clinical Medicine 9, no. 11: 3549. https://doi.org/10.3390/jcm9113549
APA StyleKim, J. S., Hwang, H. S., Lee, S. H., Kim, Y. G., Moon, J.-Y., Kong, J. Y., & Jeong, K. H. (2020). Clinical Relevance of Serum Galactose Deficient IgA1 in Patients with IgA Nephropathy. Journal of Clinical Medicine, 9(11), 3549. https://doi.org/10.3390/jcm9113549