A Prediction Equation to Assess Resting Energy Expenditure in Japanese Patients with COPD


 and
and
Abstract
1. Introduction
2. Experimental Section
2.1. Patients
2.2. Ethical Statement
2.3. Anthropometry
2.4. Laboratory Analysis
2.5. Pulmonary Function Test
2.6. Indirect Calorimetry
2.7. Predicted REE
2.8. Statistical Analysis
3. Results
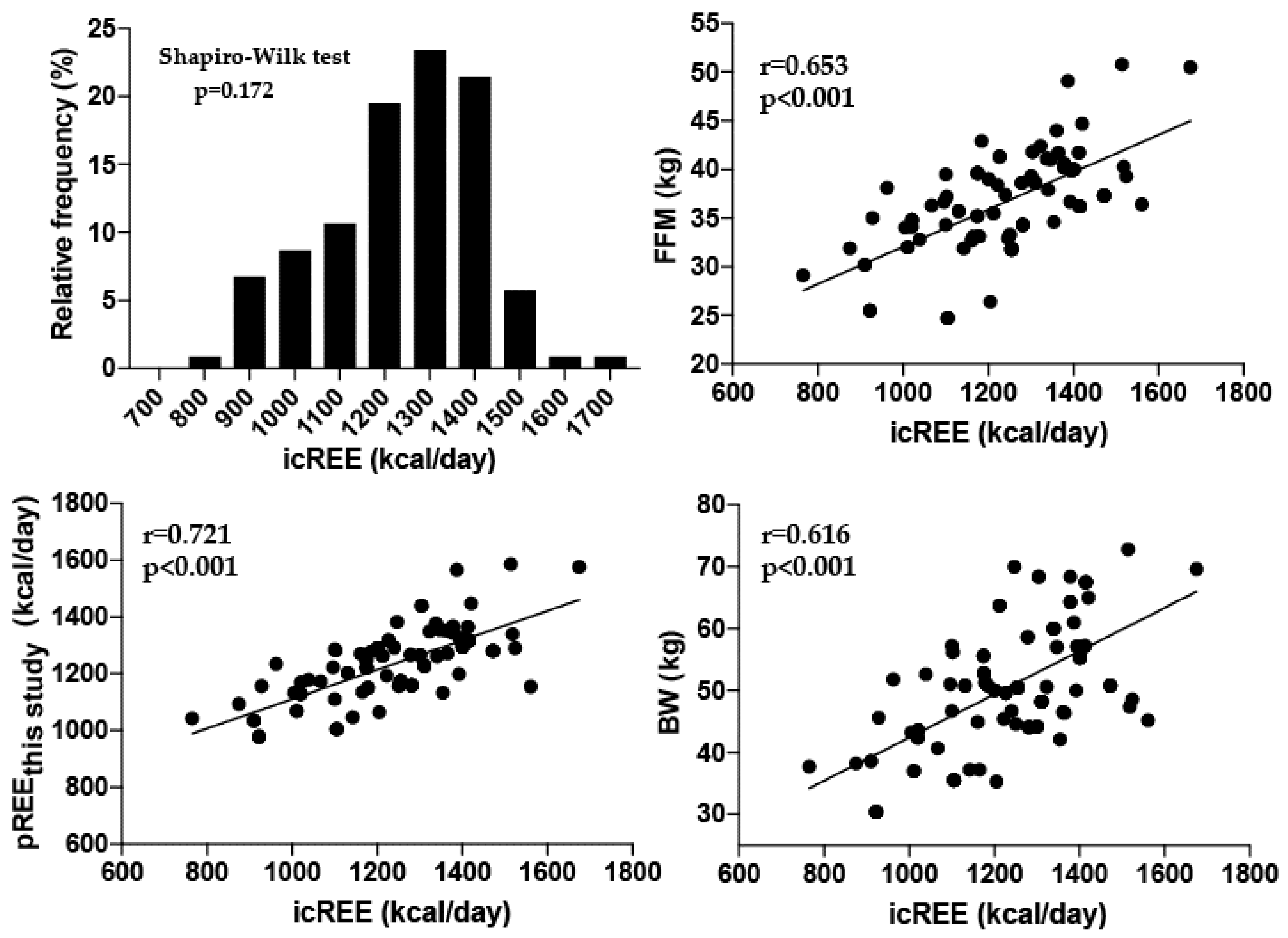
3.1. Relationship of icREE with Clinical Variables by Univariate Analysis
3.2. Relationship of icREE with Clinical Variables by Stepwise Linear Regression Analysis
3.3. Concordance Rate of icREE with Predicted REE
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Diaz-Guzman, E.; Mannino, D.M. Epidemiology and prevalence of chronic obstructive pulmonary disease. Clin. Chest. Med. 2014, 35, 7–16. [Google Scholar] [CrossRef]
- Fukuchi, Y.; Nishimura, M.; Ichinose, M.; Adachi, M.; Nagai, A.; Kuriyama, T.; Takahashi, K.; Nishimura, K.; Ishioka, S.; Aizawa, H.; et al. COPD in Japan: The Nippon COPD Epidemiology study. Respirology 2004, 9, 458–465. [Google Scholar] [CrossRef]
- Hallin, R.; Gudmundsson, G.; Suppli Ulrik, C.; Nieminen, M.M.; Gislason, T.; Lindberg, E.; Brondum, E.; Aine, T.; Bakke, P.; Janson, C. Nutritional status and long-term mortality in hospitalised patients with chronic obstructive pulmonary disease (COPD). Respir. Med. 2007, 101, 1954–1960. [Google Scholar] [CrossRef]
- King, D.A.; Cordova, F.; Scharf, S.M. Nutritional aspects of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 519–523. [Google Scholar] [CrossRef]
- Schols, A.M.; Soeters, P.B.; Dingemans, A.M.; Mostert, R.; Frantzen, P.J.; Wouters, E.F. Prevalence and characteristics of nutritional depletion in patients with stable COPD eligible for pulmonary rehabilitation. Am. Rev. Respir. Dis. 1993, 147, 1151–1156. [Google Scholar] [CrossRef]
- Creutzberg, E.C.; Wouters, E.F.; Mostert, R.; Weling-Scheepers, C.A.; Schols, A.M. Efficacy of nutritional supplementation therapy in depleted patients with chronic obstructive pulmonary disease. Nutrition 2003, 19, 120–127. [Google Scholar] [CrossRef]
- Sridhar, M.K.; Galloway, A.; Lean, M.E.; Banham, S.W. An out-patient nutritional supplementation programme in COPD patients. Eur. Respir. J. 1994, 7, 720–724. [Google Scholar] [CrossRef]
- Weekes, C.E.; Emery, P.W.; Elia, M. Dietary counselling and food fortification in stable COPD: A randomised trial. Thorax 2009, 64, 326–331. [Google Scholar] [CrossRef]
- McDoniel, S.O. Systematic review on use of a handheld indirect calorimeter to assess energy needs in adults and children. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 491–500. [Google Scholar] [CrossRef]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Human Basal Metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef]
- Moore, J.A.; Angelillo, V.A. Equations for the prediction of resting energy expenditure in chronic obstructive lung disease. Chest 1988, 94, 1260–1263. [Google Scholar] [CrossRef] [PubMed]
- Nordenson, A.; Gronberg, A.M.; Hulthen, L.; Larsson, S.; Slinde, F. A validated disease specific prediction equation for resting metabolic rate in underweight patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2010, 5, 271–276. [Google Scholar] [PubMed]
- Hogman, M.; Sulku, J.; Stallberg, B.; Janson, C.; Broms, K.; Hedenstrom, H.; Lisspers, K.; Malinovschi, A.N. 2017 Global Initiative for Chronic Obstructive Lung Disease reclassifies half of COPD subjects to lower risk group. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Sasaki, M.; Takaoka, A.; Kurihara, M.; Iwakawa, H.; Bamba, S.; Ban, H.; Andoh, A. Changes in energy metabolism after induction therapy in patients with severe or moderate ulcerative colitis. J. Clin. Biochem. Nutr. 2015, 56, 215–219. [Google Scholar] [CrossRef]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef]
- Frankenfield, D.; Roth-Yousey, L.; Compher, C. Comparison of predictive equations for resting metabolic rate in healthy nonobese and obese adults: A systematic review. J. Am. Diet. Assoc. 2005, 105, 775–789. [Google Scholar] [CrossRef]
- Weijs, P.J. Validity of predictive equations for resting energy expenditure in U.S. and Dutch overweight and obese class I and II adults aged 18–65 y. Am. J. Clin. Nutr. 2008, 88, 959–970. [Google Scholar] [CrossRef]
- Creutzberg, E.C.; Schols, A.M.; Bothmer-Quaedvlieg, F.C.; Wouters, E.F. Prevalence of an elevated resting energy expenditure in patients with chronic obstructive pulmonary disease in relation to body composition and lung function. Eur. J. Clin. Nutr. 1998, 52, 396–401. [Google Scholar] [CrossRef]
- Schols, A.M.; Fredrix, E.W.; Soeters, P.B.; Westerterp, K.R.; Wouters, E.F. Resting energy expenditure in patients with chronic obstructive pulmonary disease. Am. J. Clin. Nutr. 1991, 54, 983–987. [Google Scholar] [CrossRef]
- Broekhuizen, R.; Wouters, E.F.; Creutzberg, E.C.; Schols, A.M. Raised CRP levels mark metabolic and functional impairment in advanced COPD. Thorax 2006, 61, 17–22. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Bedu, M.; Caillaud, D.; Beaufrere, B.; Beaujon, G.; Vasson, M.; Coudert, J.; Ritz, P. Increased resting energy expenditure is related to plasma TNF-alpha concentration in stable COPD patients. Clin. Nutr. 1999, 18, 269–274. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All Patients | Staging I | Staging II | Staging III | Staging IV |
|---|---|---|---|---|---|
| Number of patients | 102 | 9 | 21 | 45 | |
| Age (year) | 78.4 ± 6.3 | 78.7 ± 5.4 | 81.5 ± 5.7 | 79.1 ± 5.6 | 74.4 ± 6.8 |
| Gender (M/F) | 94/8 | 9/0 | 19/2 | 40/5 | 26/1 |
| Height (cm) | 159.0 ± 5.9 | 159.8 ± 3.5 | 159.2 ± 4.5 | 158.9 ± 7.2 | 158.7 ± 5.6 |
| Body weight (kg) | 51.7 ± 10.1 | 54.2 ± 8.0 | 53.5 ± 7.8 | 52.2 ± 10.8 | 44.3 ± 7.3 |
| BMI (kg/m2) | 20.4 ± 4.0 | 21.3 ± 3.5 | 21.1 ± 2.6 | 20.6 ± 4.0 | 17.5 ± 2.2 |
| FFM (kg) | 36.6 ± 5.1 | 37.6 ± 3.2 | 38.4 ± 3.3 | 36.5 ± 5.6 | 34.9 ± 5.5 |
| VC (%pred) | 75.5 ± 17.9 | 94.0 ± 18.9 | 87.3 ± 6.5 | 72.6 ± 15.1 | 62.9 ± 17.4 |
| FVC (%pred) | 74.3 ± 18.5 | 97.6 ± 18.3 | 86.4 ± 9.4 | 71.5 ± 16.2 | 60.6 ± 12.8 |
| FEV₁/FVC (%pred) | 47.6 ± 16.6 | 68.6 ± 6.7 | 57.6 ± 9.4 | 44.9 ± 13.3 | 29.8 ± 6.1 |
| %FEV₁ (%pred) | 46.7 ± 39.7 | 90.7 ± 5.7 | 64.3 ± 10.2 | 38.6 ± 5.5 | 24.3 ± 4.2 |
| WBC (/μL) | 7621 ± 2400 | 5742 ± 1340 | 7080 ± 1706 | 8549 ± 2548 | 7288 ± 2337 |
| ALB (mg/dL) | 3.3 ± 0.5 | 3.3 ± 0.7 | 3.0 ± 0.5 | 3.3 ± 0.5 | 3.4 ± 0.5 |
| CRP (mg/dL) | 0.73 ± 1.04 | 0.58 ± 0.57 | 0.92 ± 0.86 | 0.65 ± 0.66 | 0.79 ± 1.75 |
| icREE (kcal) | 1239 ± 173 | 1303 ± 207 | 1223 ±176 | 1248 ± 159 | 1205 ± 176 |
| Correlation Coefficients | p Values | |
|---|---|---|
| FFM (kg) | 0.653 | <0.001 |
| Body weight (kg) | 0.616 | <0.001 |
| BMI (kg/m2) | 0.546 | <0.001 |
| Height (cm) | 0.305 | 0.002 |
| Gender (m/f) | –0.222 | 0.007 |
| %VC (%predicted) | 0.270 | 0.006 |
| %FVC (%predicted) | 0.223 | 0.024 |
| FEV₁/FVC (%predicted) | 0.150 | 0.131 |
| %FEV₁ (%predicted) | 0.138 | 0.165 |
| Age (years) | −0.172 | 0.128 |
| CRP (mg/dL | 0.141 | 0.160 |
| WBC (/μL) | 0.114 | 0.253 |
| ALB (mg/dL) | −0.026 | 0.797 |
| Model 1 | ||||
| Variable | SPRC | SPRC SE | β | p-value |
| Constant | 423.1 | 95.5 | <0.001 | |
| FFM | 22.3 | 2.6 | 0.653 | <0.001 |
| R2 = 0.421 | ||||
| MODEL 2 | ||||
| Variable | SPRC | SPRC SE | β | p-value |
| Constant | 409.2 | 91.4 | <0.001 | |
| FFM | 14.9 | 3.4 | 0.436 | <0.001 |
| BW | 5.6 | 1.8 | 0.318 | 0.002 |
| R2 = 0.470 | ||||
| MODEL 3 | ||||
| Variable | SPRC | SPRC SE | β | p-value |
| Constant | 851.9 | 179.4 | <0.001 | |
| FFM | 12.8 | 3.3 | 0.376 | <0.001 |
| BW | 7.1 | 1.8 | 0.404 | <0.001 |
| Age | −5.7 | 2.0 | 0.208 | 0.006 |
| R2 = 0.505 | ||||
| Mean | ± SD | p Value | Concordance Rate (%) with icREE | |
|---|---|---|---|---|
| icREE | 1238 ± 173 | |||
| pREEthis study | 1234 ± 124 | 0.701 | 74.5 | |
| pREEHB | 1038 ± 135 | p < 0.001 | 23.5 | |
| pREEMoore | 1510 ± 163 | p < 0.001 | 14.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morikawa, K.; Tabira, K.; Takemura, H.; Inaba, S.; Kusuki, H.; Hashitsume, Y.; Suzuki, Y.; Tenpaku, Y.; Yasuma, T.; D’Alessandro-Gabazza, C.N.; et al. A Prediction Equation to Assess Resting Energy Expenditure in Japanese Patients with COPD. J. Clin. Med. 2020, 9, 3455. https://doi.org/10.3390/jcm9113455
Morikawa K, Tabira K, Takemura H, Inaba S, Kusuki H, Hashitsume Y, Suzuki Y, Tenpaku Y, Yasuma T, D’Alessandro-Gabazza CN, et al. A Prediction Equation to Assess Resting Energy Expenditure in Japanese Patients with COPD. Journal of Clinical Medicine. 2020; 9(11):3455. https://doi.org/10.3390/jcm9113455
Chicago/Turabian StyleMorikawa, Keisuke, Kazuyuki Tabira, Hiroyuki Takemura, Shogo Inaba, Haruka Kusuki, Yu Hashitsume, Yuta Suzuki, Yosuke Tenpaku, Taro Yasuma, Corina N. D’Alessandro-Gabazza, and et al. 2020. "A Prediction Equation to Assess Resting Energy Expenditure in Japanese Patients with COPD" Journal of Clinical Medicine 9, no. 11: 3455. https://doi.org/10.3390/jcm9113455
APA StyleMorikawa, K., Tabira, K., Takemura, H., Inaba, S., Kusuki, H., Hashitsume, Y., Suzuki, Y., Tenpaku, Y., Yasuma, T., D’Alessandro-Gabazza, C. N., Gabazza, E., & Hataji, O. (2020). A Prediction Equation to Assess Resting Energy Expenditure in Japanese Patients with COPD. Journal of Clinical Medicine, 9(11), 3455. https://doi.org/10.3390/jcm9113455