Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Experimental Section
2.1. Materials and Methods
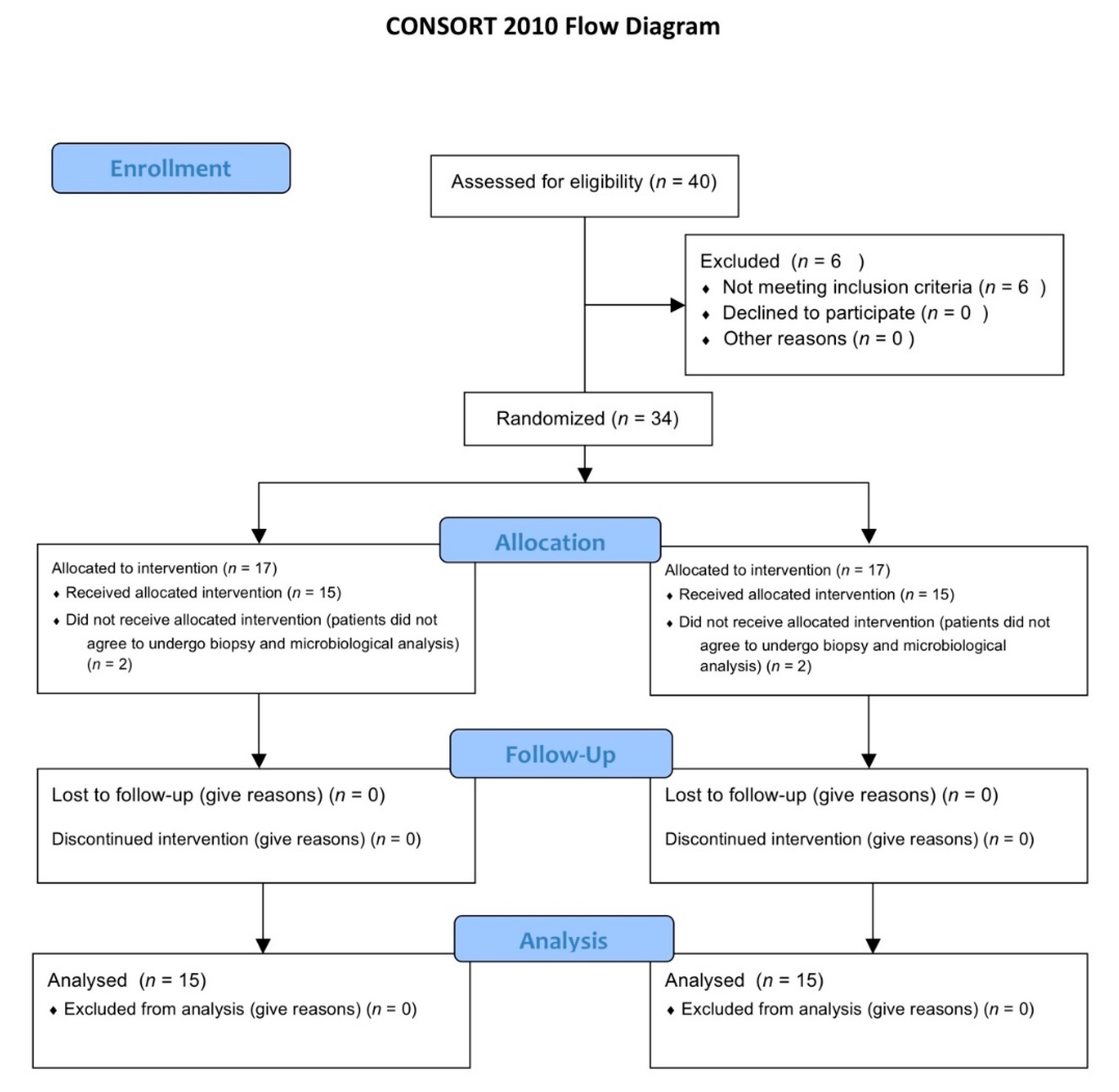
2.1.1. Study Design, Patient Selection and Randomization
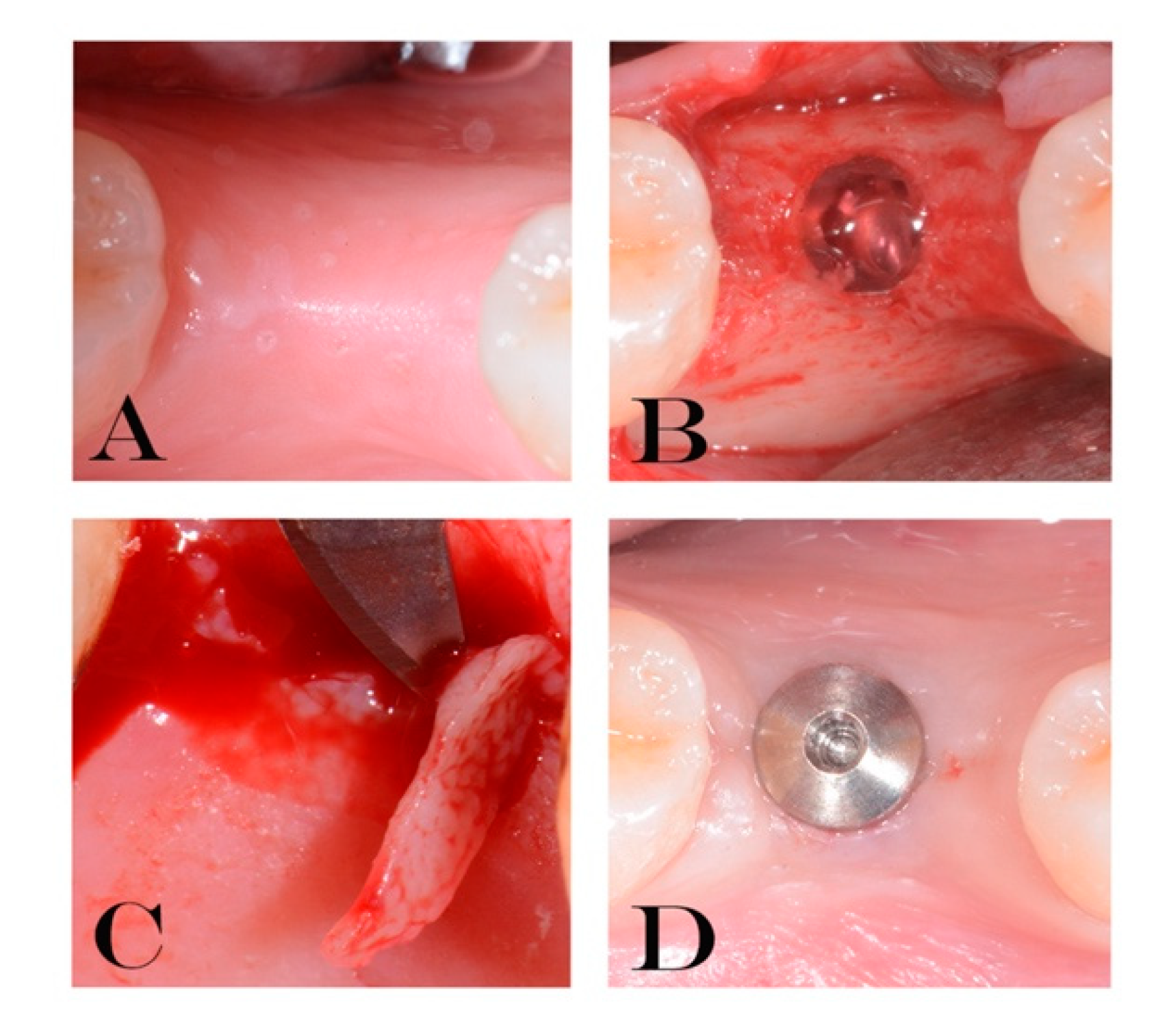
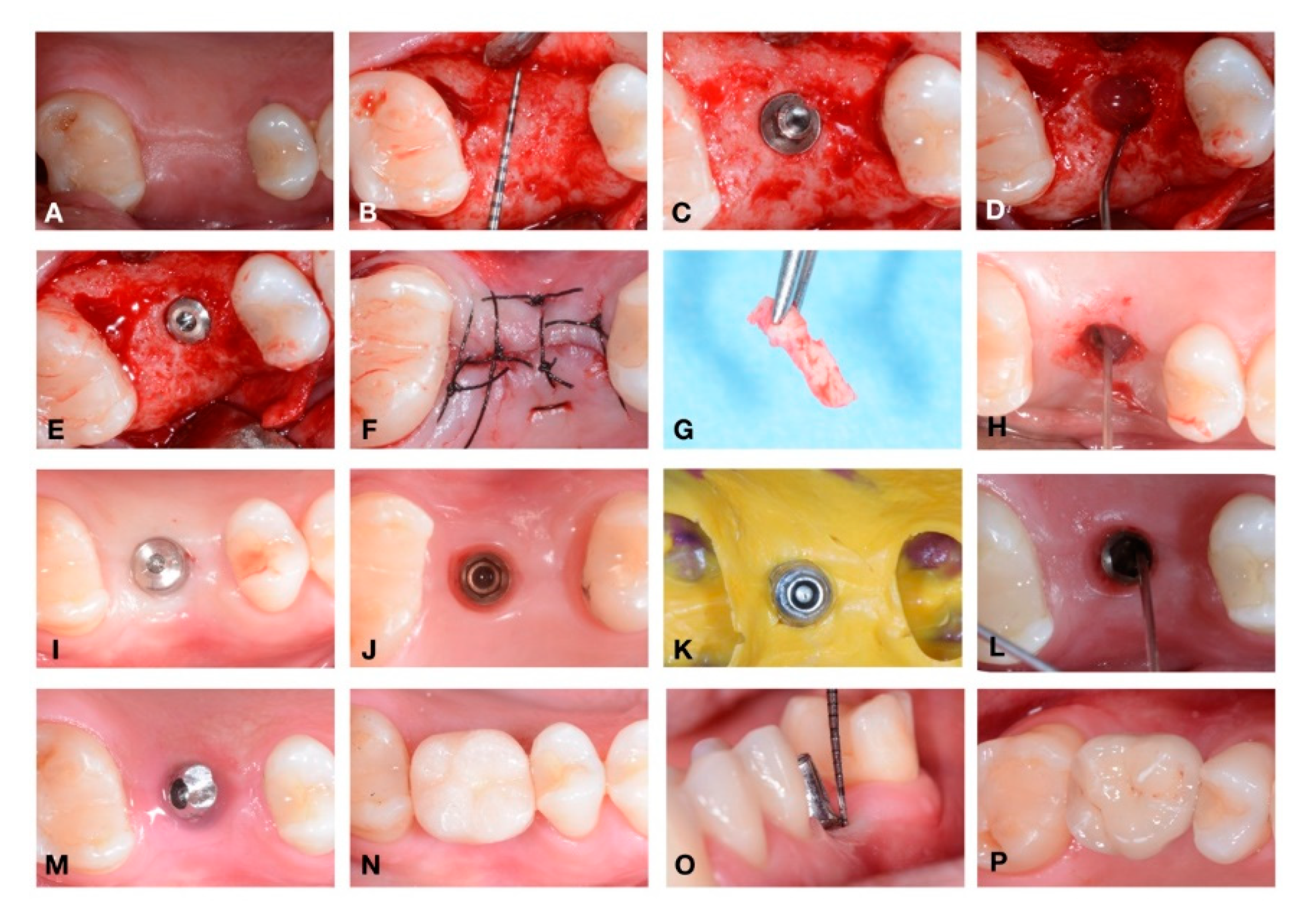
2.1.2. Surgical Treatment
2.1.3. Preparation of Total Genomic DNA
2.1.4. TaqMan Polymerase Chain Reaction (PCR)
2.1.5. Immunohistochemical Analysis
2.1.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Brakel, R.V.; Cune, M.S.; Winkelhoff, A.J.V.; Putter, C.D.; Verhoeven, J.W.; Reijden, W.V.D. Early bacterial colonization and soft tissue health around zirconia and titanium abutments: An in vivo study in man. Clin. Oral Implants Res. 2011, 22, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Murmura, G.; Sinjari, B.; Sollazzo, V.; Spinelli, G.; Carinci, F. Analysis and structural examination of screw loosening in oral implants. Int. J. Immunopathol. Pharm. 2011, 24, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D’Addazio, G.; Traini, T.; Varvara, G.; Scarano, A.; Murmura, G.; Caputi, S. A 10-year retrospective comparative human study on screw-retained versus cemented dental implant abutments. J. Biol. Regul. Homeost. Agents 2019, 33, 787–797. [Google Scholar]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Preethanath, R.S.; AlNahas, N.W.; Bin Huraib, S.M.; Al-Balbeesi, H.O.; Almalik, N.K.; Dalati, M.H.N.; Divakar, D.D. Microbiome of dental implants and its clinical aspect. Microb. Pathog. 2017, 106, 20–24. [Google Scholar] [CrossRef]
- Quirynen, M.; Vogels, R.; Peeters, W.; van Steenberghe, D.; Naert, I.; Haffajee, A. Dynamics of initial subgingival colonization of “pristine” peri-implant pockets. Clin. Oral Implants Res. 2006, 17, 25–37. [Google Scholar] [CrossRef]
- De Angelo, S.J.; Kumar, P.S.; Beck, F.M.; Tatakis, D.N.; Leblebicioglu, B. Early soft tissue healing around one-stage dental implants: Clinical and microbiologic parameters. J. Periodontol. 2007, 78, 1878–1886. [Google Scholar] [CrossRef]
- Furst, M.M.; Salvi, G.E.; Lang, N.P.; Persson, G.R. Bacterial colonization immediately after installation on oral titanium implants. Clin. Oral Implants Res. 2007, 18, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Heuer, W.; Elter, C.; Demling, A.; Neumann, A.; Suerbaum, S.; Hannig, M.; Heidenblut, T.; Bach, F.W.; Stiesch-Scholz, M. Analysis of early biofilm formation on oral implants in man. J. Oral Rehabil. 2007, 34, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Tzach-Nahman, R.; Mizraji, G.; Shapira, L.; Nussbaum, G.; Wilensky, A. Oral infection with Porphyromonas gingivalis induces peri-implantitis in a murine model: Evaluation of bone loss and the local inflammatory response. J. Clin. Periodontol. 2017, 44, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Liang, S.; Payne, M.A.; Hashim, A.; Jotwani, R.; Eskan, M.A.; McIntosh, M.L.; Alsam, A.; Kirkwood, K.L.; Lambris, J.D.; et al. Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microb. 2011, 10, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G. The inflammophilic character of the periodontitis-associated microbiota. Mol. Oral Microbiol. 2014, 29, 248–257. [Google Scholar] [CrossRef] [PubMed]
- How, K.Y.; Song, K.P.; Chan, K.G. Porphyromonas gingivalis: An Overview of Periodontopathic Pathogen below the Gum Line. Front. Microbiol. 2016, 7, 53. [Google Scholar] [CrossRef]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Lamont, R.J. Beyond the red complex and into more complexity: The polymicrobial synergy and dysbiosis (PSD) model of periodontal disease aetiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Peri-Implantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef]
- Jiao, Y.; Hasegawa, M.; Inohara, N. The Role of Oral Pathobionts in Dysbiosis during Periodontitis Development. J. Dent. Res. 2014, 93, 539–546. [Google Scholar] [CrossRef]
- Maekawa, T.; Krauss, J.L.; Abe, T.; Jotwani, R.; Triantafilou, M.; Triantafilou, K.; Hashim, A.; Hoch, S.; Curtis, M.A.; Nussbaum, G.; et al. Porphyromonas gingivalis manipulates complement and TLR signalling to un couple bacterial clearance from inflammation and promote dysbiosis. Cell Host Microb. 2014, 15, 768–778. [Google Scholar] [CrossRef]
- Mason, M.R.; Preshaw, P.M.; Nagaraj, H.N.; Dabdoub, S.M.; Rahman, A.; Kumar, P.S. The subgingival microbiome of clinically healthy current and never smokers. ISME J. 2015, 9, 268–272. [Google Scholar] [CrossRef]
- Lasserre, J.F.; Brecx, M.C.; Toma, S. Oral microbes, biofilms and their role in periodontal and peri-Implant diseases. Materials 2018, 11, 1802. [Google Scholar] [CrossRef]
- Ericsson, I.; Persson, L.G.; Berglundh, T.; Marinello, C.P.; Lindhe, J.; Klinge, B. Different types of inflammatory reactions in peri-implant soft tissues. J. Clin. Periodontol. 1995, 22, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Gualini, F.; Berglundh, T. Immuno-histochemical characteristics of inflammatory lesions at implants. J. Clin. Periodontol. 2003, 30, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Artese, L.; Piattelli, A.; Scarano, A.; Shibli, J.A.; Piccirilli, M.; Perrotti, V.; Iezzi, G. Histological and immunohistochemical evaluation of the peri-implant soft tissues around machined and acid-etched titanium healing abutments: A prospective randomised study. Clin. Oral Investig. 2012, 16, 857–866. [Google Scholar] [CrossRef]
- Assenza, B.; Tripodi, D.; Scarano, A.; Perrotti, V.; Piattelli, A.; Iezzi, G.; D’Ercole, S. Bacterial leakage in implants with different implant-abutment connections: An in vitro study. J. Clin. Periodontol. 2012, 83, 491–497. [Google Scholar] [CrossRef]
- D’Ercole, S.; Scarano, A.; Perrotti, V.; Mulatinho, J.; Piattelli, A.; Iezzi, G.; Tripodi, D. Implants with internal hexagon and conical implant-abutment connections: An in vitro study of the bacterial contamination. J. Oral Implant. 2014, 40, 30–36. [Google Scholar] [CrossRef]
- D’Ercole, S.; Tripodi, D.; Marzo, G.; Bernardi, S.; Continenza, M.A.; Piattelli, A.; Iaculli, F.; Mummolo, S. Micro leakage of bacteria in different implant-abutment assemblies: An in vitro study. J. Appl. Biomater. Funct. Mater. 2015, 13, e174–e180. [Google Scholar]
- Paolantonio, M.; Perinetti, G.; D’Ercole, S.; Graziani, F.; Catamo, G.; Sammartino, G.; Piccolomini, R. Internal decontamination of dental implants: An in vivo randomized microbiologic 6-month trial on the effects of a chlorhexidine gel. J. Periodontol. 2008, 79, 1419–1425. [Google Scholar] [CrossRef]
- D’Ercole, S.; Tetè, S.; Catamo, G.; Sammartino, G.; Femminella, B.; Tripodi, D.; Spoto, G.; Paolantonio, M. Microbiological and biochemical effectiveness of an antiseptic gel on the bacterial contamination of the inner space of dental implants: A 3-month human longitudinal study. Int. J. Immunopathol. Pharm. 2009, 22, 1019–1026. [Google Scholar] [CrossRef]
- Persson, G.R.; Roos-Jansaker, A.M.; Lindahl, C.; Renvert, S. Microbiologic results after non-surgical erbium-doped:yttrium, aluminum, and garnet laser or air-abrasive treatment of peri-implantitis: A randomized clinical trial. J. Periodontol. 2011, 82, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D’Addazio, G.; De Tullio, I.; Traini, T.; Caputi, S. Peri-implant bone resorption during healing abutment placement: The effect of a 0.20% Chlorhexidine gel vs. placebo-A randomized double blind controlled human study. BioMed Res. Int. 2018, 2018, 5326340. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.Y.; Shi, J.Y.; Zhu, Y.; Qian, S.J.; Lai, H.C.; Gu, Y.X. The effect of photodynamic therapy on pathogenic bacteria around peri-implant sulcus and in the cavity between abutment and implant after healing phase: A prospective clinical study. Lasers Surg Med. 2018, 50, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Sheen, S.; Addy, M. An in vitro evaluation of the availability of cetylpyridinium chloride and chlorhexidine in some commercially available mouthrinse products. Br. Dent. J. 2003, 194, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Basrani, B.; Lemonie, C. Chlorhexidine gluconate. Aust. Endod. J. 2005, 3, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Cataldo, M.A.; Dancer, S.J.; De Angelis, G.; Falcone, M.; Frank, U.; Kahlmeter, G.; Pan, A.; Petrosillo, N.; Rodríguez-Baño, J.; et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin. Microbiol. Infect. 2014, 20, 1–55. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Annibali, S.; Bignozzi, I.; Cristalli, M.P.; Graziani, F.; La Monaca, G.; Polimeni, A. Peri-implant marginal bone level: A systematic review and meta-analysis of studies comparing platform switching versus conventionally restored implants. J. Clin. Periodontol. 2012, 39, 1097–1113. [Google Scholar] [CrossRef]
- Scarano, A.; Murmura, G.; Sinjari, B.; Assenza, B.; Sollazzo, V.; Spinelli, G.; Carinci, F. Expansion of the alveolar bone crest with ultrasonic surgery device: Clinical study in mandible. Int. J. Immunopathol. Pharm. 2011, 24, 71–75. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef]
- Bizhang, M.; Ellerbrock, B.; Preza, D.; Raab, W.; Singh, P.; Beikler, T.; Henrich, B.; Zimmer, S. Detection of nine microorganisms from the initial carious root lesions using a TaqMan-based real-time PCR. Oral Dis. 2011, 17, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Becker, K.; Rahn, S.; Hegewald, A.; Pfeffer, K.; Henrich, B. Real-time PCR analysis of fungal organisms and bacterial species at peri-implantitis sites. Int. J. Implant Dent. 2015, 1, 9. [Google Scholar] [CrossRef] [PubMed]
- Henrich, B.; Hermann, I.; Di Giulio, M.; Köhrer, K.; Deenen, R.; Sivalingam, S.; Peters, U.; Beikler, T.; Janda, R.; Rüttermann, S. Reexamination In Vitro and In Situ of an Antibacterially Modified Experimental Dental Resin Composite with Molecular Methods: A Pilot Study. Adv. Mater. Sci. Eng. 2016, 2016, 1–13. [Google Scholar] [CrossRef]
- D’Addazio, G.; Artese, L.; Traini, T.; Rubini, C.; Caputi, S.; Sinjari, B. Immunohistochemical study of osteopontin in oral squamous cell carcinoma allied to fractal dimension. J. Biol. Regul. Homeost. Agents 2018, 32, 1033–1038. [Google Scholar]
- Spreadborough, P.; Lort, S.; Pasquali, S.; Popplewell, M.; Owen, A.; Kreis, I.; Tucker, O.; Vohra, R.S. Preventing Postoperative Pneumonia Study Group and the West Midlands Research Collaborative. A systematic review and meta-analysis of perioperative oral decontamination in patients undergoing major elective surgery. Perioper. Med. 2016, 22, 5–6. [Google Scholar]
- Mellado-Valero, A.; Buitrago-Vera, P.; Solá-Ruiz, M.F.; Ferrer-García, J.C. Decontamination of dental implant surface in peri-implantitis treatment: A literature review. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e869–e876. [Google Scholar] [CrossRef]
- Di Giulio, M.; Traini, T.; Sinjari, B.; Nostro, A.; Caputi, S.; Cellini, L. Porphyromonas gingivalis biofilm formation in different titanium surfaces, an in vitro study. Clin. Oral Implant Res. 2016, 27, 918–925. [Google Scholar] [CrossRef]
- Chen, Z.; Chen, D.; Zhang, S.; Tang, L.; Li, Q. Antibiotic prophylaxis for preventing dental implant failure and postoperative infection: A systematic review of randomized controlled trials. Am. J. Dent. 2017, 30, 89–95. [Google Scholar]
- Barbour, M.E.; Gandhi, N.; el-Turki, A.; O’Sullivan, D.J.; Jagger, D.C. Differential adhesion of Streptococcus gordonii to anatase and rutile titanium dioxide surfaces with and without functionalization with chlorhexidine. J. Biomed. Mater. Res. Part A 2009, 90, 993–998. [Google Scholar] [CrossRef]
- Faggion, C.M., Jr.; Chambrone, L.; Listl, S.; Tu, Y.K. Network meta-analysis for evaluating interventions in implant dentistry: The case of peri-implantitis treatment. Clin. Implant Dent. Relat. Res. 2013, 15, 576–588. [Google Scholar] [CrossRef] [PubMed]
- De Waal, Y.C.; Raghoebar, G.M.; Meijer, H.J.; Winkel, E.G.; van Winkelhoff, A.J. Implant decontamination with 2% chlorhexidine during surgical peri-implantitis treatment: A randomized, double-blind, controlled trial. Clin. Oral Implant Res. 2015, 26, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennström, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Podhorsky, A.; Putzier, S.; Rehmann, P.; Streckbein, P.; Domann, E.; Wöstmann, B. Bacterial Contamination of the Internal Cavity of Dental Implants After Application of Disinfectant or Sealant Agents Under Cyclic Loading in vitro. Int. J. Prosthodont. 2016, 29, 493–495. [Google Scholar] [CrossRef]
- Jervøe-Storm, P.M.; Jepsen, S.; Jöhren, P.; Mericske-Stern, R.; Enkling, N. Internal bacterial colonization of implants: Association with peri-implant bone loss. Clin. Oral Implant Res. 2015, 26, 957–963. [Google Scholar] [CrossRef]
- Canullo, L.; Peñarrocha-Oltra, D.; Covani, U.; Botticelli, D.; Serino, G.; Penarrocha, M. Clinical and microbiological findings in patients with peri-implantitis: A cross-sectional study. Clin. Oral Implant Res. 2016, 27, 376–382. [Google Scholar] [CrossRef]
- Stokman, M.A.; van Winkelhoff, A.J.; Vissink, A.; Spijkervet, F.K.; Raghoebar, G.M. Bacterial colonization of the peri-implant sulcus in dentate patients: A prospective observational study. Clin. Oral Investig. 2017, 21, 717–724. [Google Scholar] [CrossRef]
- Canullo, L.; Peñarrocha-Oltra, D.; Covani, U.; Rossetti, P.H. Microbiologic and Clinical Findings of Implants in Healthy Condition and with Peri-Implantitis. Int. J. Oral Maxillofac. Implants 2015, 30, 834–842. [Google Scholar] [CrossRef]
- Cugini, C.; Klepac-Ceraj, V.; Rackaityte, E.; Riggs, J.E.; Davey, M.E. Porphyromonas gingivalis: Keeping the pathos out of the biont. J. Oral Microbiol 2013, 5, 19804. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Muzafferiy, F.; Anderson, A.C.; Wölber, J.P.; Ratka-Krüger, P.; Fretwurst, T.; Nelson, K.; Vach, K.; Hellwig, E. Shift of microbial composition of peri-implantitis-associated oral biofilm as revealed by 16S rRNA gene cloning. J. Med. Microbiol. 2018, 67, 332–340. [Google Scholar] [CrossRef]
- Lang, N.P.; Bosshardt, D.D.; Lulic, M. Do mucositis lesions around implants differ from gingivitis lesions around teeth? J. Clin. Periodontol. 2011, 38, 182–187. [Google Scholar] [CrossRef]
- Liu, J.X.; Werner, J.; Kirsch, T.; Zuckerman, J.D.; Virk, M.S. Cytotoxicity evaluation of chlorhexidine gluconate on human fibroblasts, myoblasts, and osteoblasts. J. Bone Jt. Infect. 2018, 10, 165–172. [Google Scholar] [CrossRef]
- Haydari, M.; Bardakci, A.G.; Koldsland, O.C.; Aass, A.M.; Sandvik, L.; Preus, H.R. Comparing the effect of 0.06% -, 0.12% and 0.2% Chlorhexidine on plaque, bleeding and side effects in an experimental gingivitis model: A parallel group, double masked randomized clinical trial. BMC Oral Health 2017, 17, 118. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
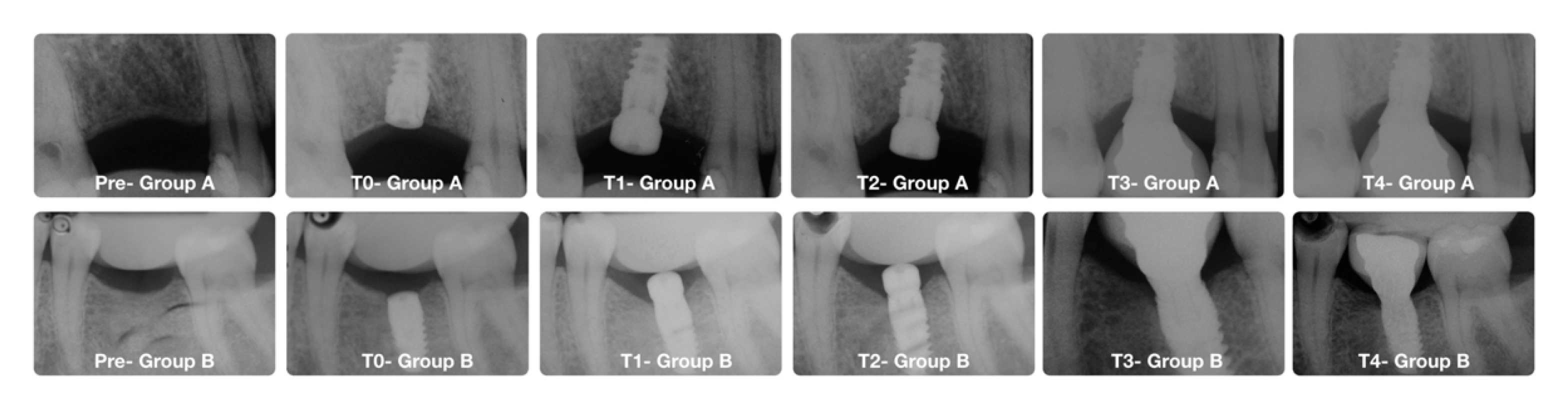
| Timeline Stages | |||
|---|---|---|---|
| Stage | Time Point | Clinical Procedures | Experimental Procedure |
| T0 | 0 weeks | Implant insertion | Soft-tissue biopsy |
| T1 | 8 weeks | Second surgical stage | Soft-tissue biopsy |
| T2 | 10 weeks | Implant impression | collection of healing abutment for microbiological analysis |
| Clinical indexes. | Group A (n = 15) (PLACEBO). | Group B (n = 15) (CHX) |
|---|---|---|
| BOP mean at implant placement | 9.2% | 8.15% |
| BOP mean at second surgical stage | 11.32% | 12.21% |
| Plaque score at implant placement | 17.45% | 17.32% |
| Plaque score at second surgical stage | 19.34% | 18.45% |
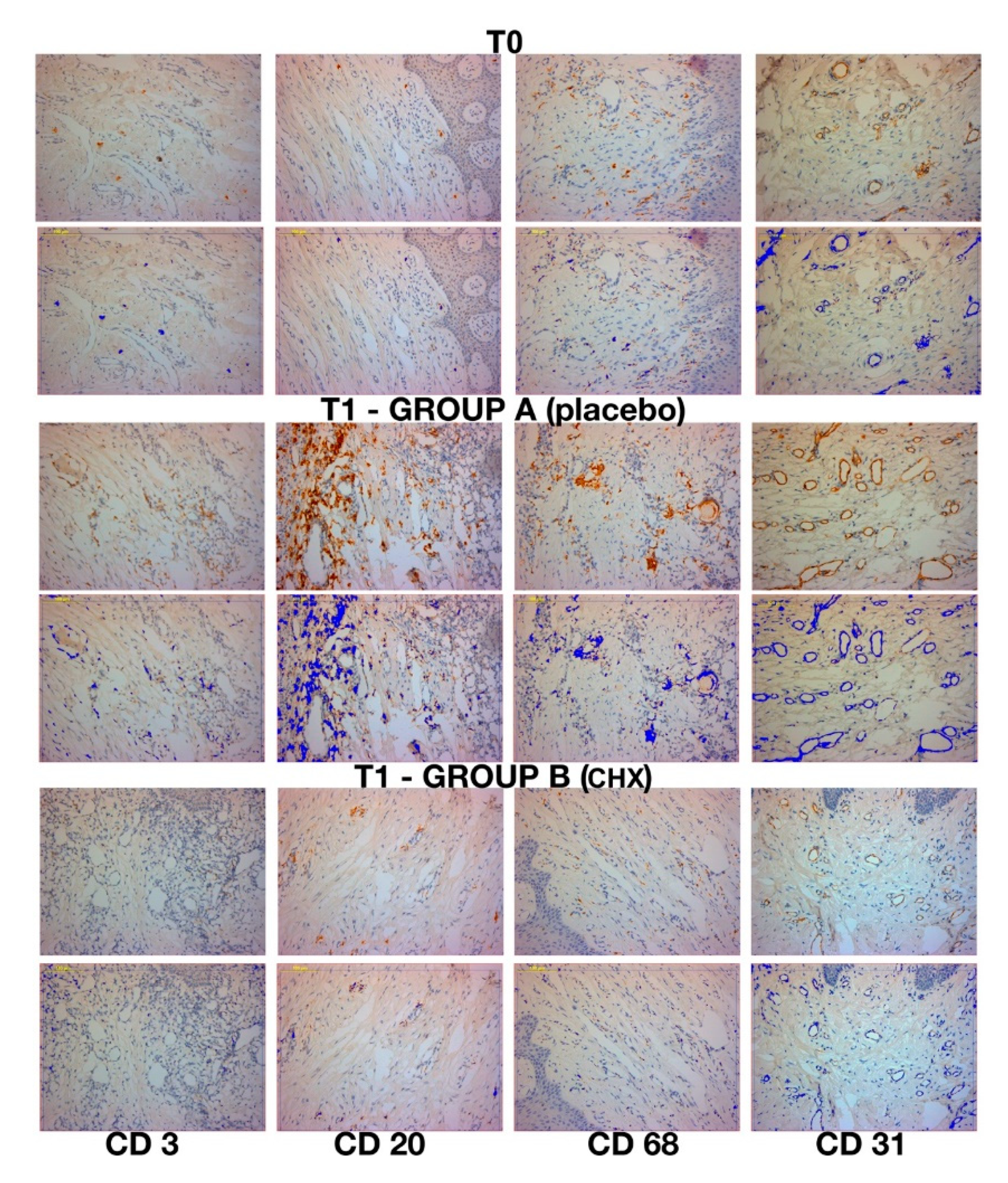
| Markers | CD 3 | CD 20 | CD 68 | CD 31 |
|---|---|---|---|---|
| GROUP A (PLACEBO) | ||||
| No. | 15 | 15 | 15 | 15 |
| Mean (SD) | 7.02% ± 1.4 | 13.78% ± 2.0 | 5.41% ± 0.8 | 32.61 ± 3.4 |
| Range | (4.086–10.264) | (10.74–17.708) | (4.042–6.97) | (22–36) |
| SEM | 0.375 | 0.527 | 0.225 | 0.881 |
| GROUP B (CHX) | ||||
| No. | 15 | 15 | 15 | 15 |
| Mean (SD) | 2.91% ± 1.1 | 4.96% ± 1.9 | 2.53% ± 0.9 | 21.8 ± 3.0 |
| Range | (1.36–4.55) | (2.636–9.778) | (0.824–4.01) | (17–27) |
| SEM | 0.309 | 0.508 | 0.225 | 0.786 |
| Difference | 4.111 | 8.825 | 2.877 | 10.733 |
| T (with 28 degree of freedom) (p < 0.001) | 8.455 | 12.056 | 8.455 | 9.093 |
| 95% confidence interval for difference of mean | 3.115–5.107 | 7.326–10.324 | 2.180–3.574 | 8.315–13.151 |
| p value | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ercole, S.; D’Addazio, G.; Di Lodovico, S.; Traini, T.; Di Giulio, M.; Sinjari, B. Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study. J. Clin. Med. 2020, 9, 284. https://doi.org/10.3390/jcm9010284
D’Ercole S, D’Addazio G, Di Lodovico S, Traini T, Di Giulio M, Sinjari B. Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study. Journal of Clinical Medicine. 2020; 9(1):284. https://doi.org/10.3390/jcm9010284
Chicago/Turabian StyleD’Ercole, Simonetta, Gianmaria D’Addazio, Silvia Di Lodovico, Tonino Traini, Mara Di Giulio, and Bruna Sinjari. 2020. "Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study" Journal of Clinical Medicine 9, no. 1: 284. https://doi.org/10.3390/jcm9010284
APA StyleD’Ercole, S., D’Addazio, G., Di Lodovico, S., Traini, T., Di Giulio, M., & Sinjari, B. (2020). Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study. Journal of Clinical Medicine, 9(1), 284. https://doi.org/10.3390/jcm9010284