Split-Liver Ex Situ Machine Perfusion: A Novel Technique for Studying Organ Preservation and Therapeutic Interventions

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials & Methods
2.1. Donor Liver Selection
2.2. Donor Liver Procurement
2.3. Split-Liver Technique
2.4. Ex Situ Subnormothermic Machine Perfusion (SNMP)
2.5. Biochemical Profiling
2.6. Evaluation of Hepatic Energy Charge
2.7. Histological Evaluation
2.8. Statistical Analysis
3. Results
3.1. Donor Characteristics
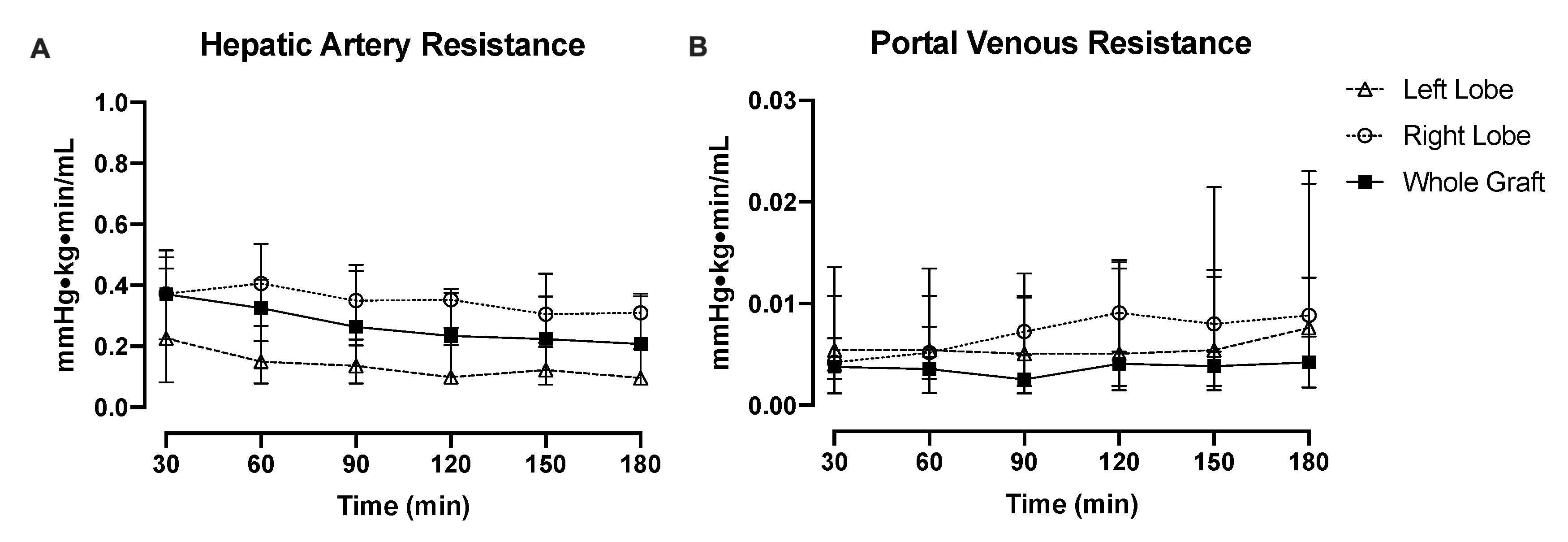
3.2. Perfusion Hemodynamics
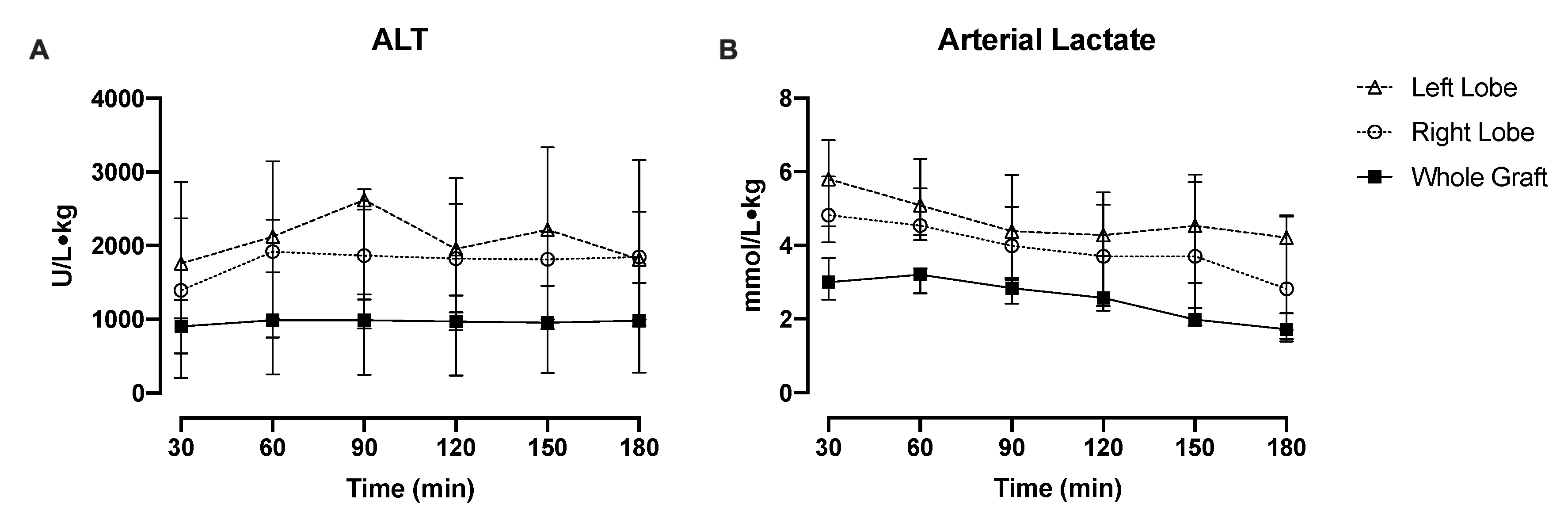
3.3. Injury and Functional Recovery
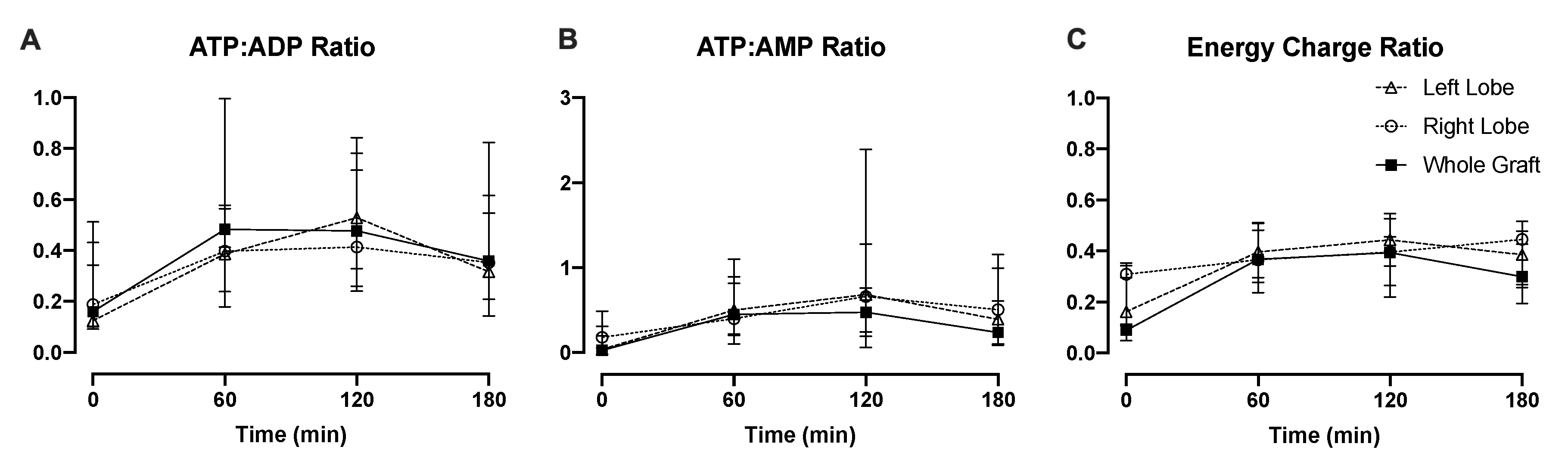
3.4. Liver Energy Status
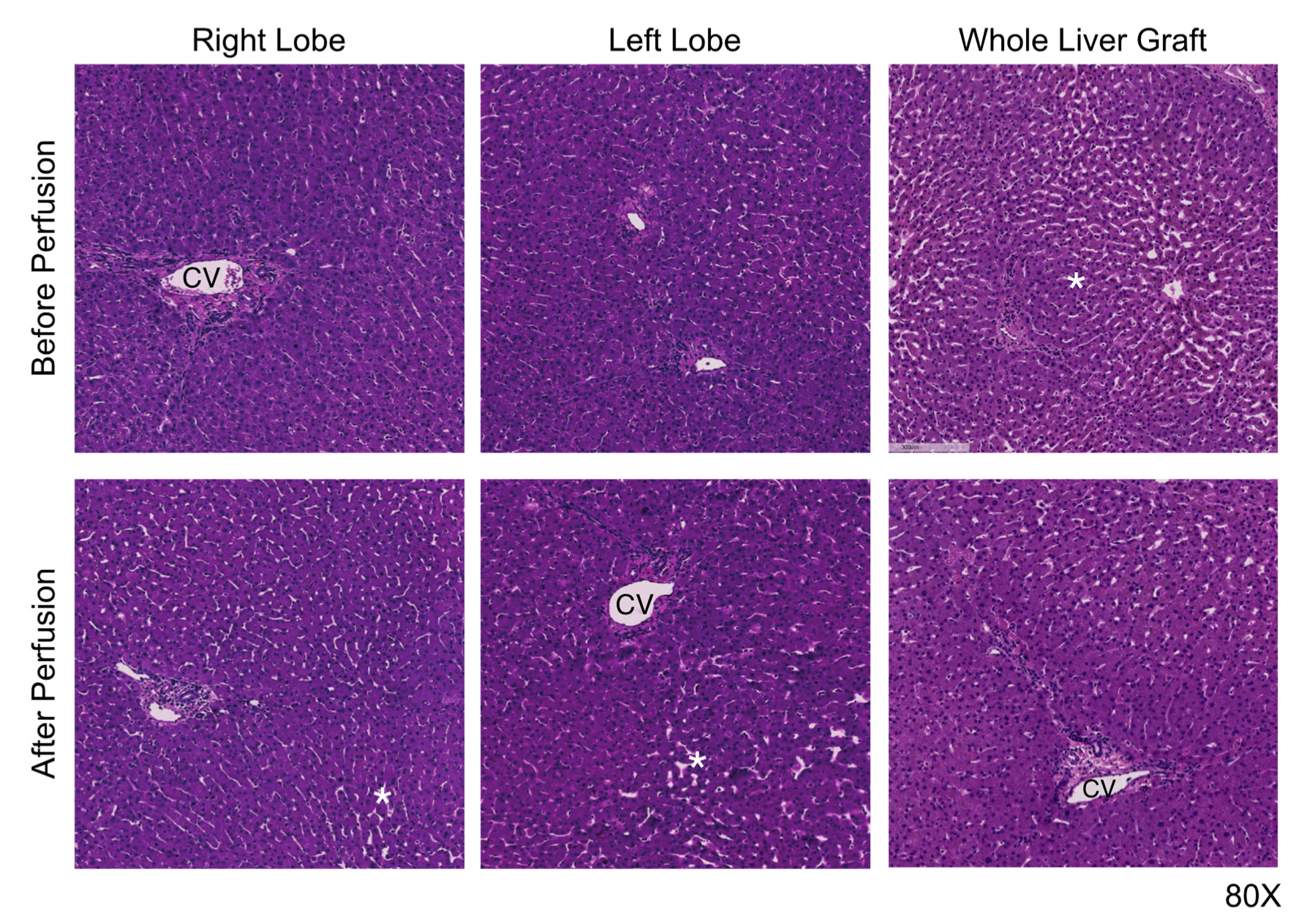
3.5. Preservation Histology
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- OPTN: Organ Procurement & Transplantation Network. Available online: https://optn.transplant.hrsa.gov/ (accessed on 15 February 2019).
- Kim, W.R.; Lake, J.R.; Smith, J.M.; Skeans, M.A.; Schladt, D.P.; Edwards, E.B.; Harper, A.M.; Wainright, J.L.; Snyder, J.J.; Israni, A.K.; et al. OPTN/SRTR 2014 Annual Data Report: Liver. Am. J. Transplant. 2016, 16, 69–98. [Google Scholar] [CrossRef] [Green Version]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; Garcia-Valdecasas, J.C.; Heaton, N.; et al. A randomized trial of normothermic preservation in liver transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Dutkowski, P.; Polak, W.G.; Muiesan, P.; Schlegel, A.; Verhoeven, C.J.; Scalera, I.; DeOliveira, M.L.; Kron, P.; Clavien, P.-A. First Comparison of Hypothermic Oxygenated PErfusion versus Static Cold Storage of Human Donation after Cardiac Death Liver Transplants: An International-matched Case Analysis. Ann. Surg. 2015, 262, 764–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarrera, J.V.; Henry, S.D.; Samstein, B.; Reznik, E.; Musat, C.; Lukose, T.I.; Ratner, L.E.; Brown, R.S.; Kato, T.; Emond, J.C. Hypothermic machine preservation facilitates successful transplantation of “orphan” extended criteria donor livers. Am. J. Transplant. 2015, 15, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Mergental, H.; Perera, M.T.P.R.; Laing, R.W.; Muiesan, P.; Isaac, J.R.; Smith, A.; Stephenson, B.T.F.; Cilliers, H.; Neil, D.A.H.; Hübscher, S.G.; et al. Transplantation of Declined Liver Allografts Following Normothermic Ex-Situ Evaluation. Am. J. Transplant. 2016, 16, 3235–3245. [Google Scholar] [CrossRef] [Green Version]
- Ravikumar, R.; Jassem, W.; Mergental, H.; Heaton, N.; Mirza, D.; Perera, M.T.P.R.; Quaglia, A.; Holroyd, D.; Vogel, T.; Coussios, C.C.; et al. Liver Transplantation After Ex Vivo Normothermic Machine Preservation: A Phase 1 (First-in-Man) Clinical Trial. Am. J. Transplant. 2016, 16, 1779–1787. [Google Scholar] [CrossRef]
- Selzner, M.; Goldaracena, N.; Echeverri, J.; Kaths, J.M.; Linares, I.; Selzner, N.; Serrick, C.; Marquez, M.; Sapisochin, G.; Renner, E.L.; et al. Normothermic ex vivo liver perfusion using steen solution as perfusate for human liver transplantation: First North American results. Liver Transplant. 2016, 22, 1501–1508. [Google Scholar] [CrossRef] [Green Version]
- Watson, C.J.E.; Kosmoliaptsis, V.; Randle, L.V.; Russell, N.K.; Griffiths, W.J.H.; Davies, S.; Mergental, H.; Butler, A.J. Preimplant normothermic liver perfusion of a suboptimal liver donated after circulatory death. Am. J. Transplant. 2016, 16, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Bral, M.; Gala-Lopez, B.; Bigam, D.; Kneteman, N.; Malcolm, A.; Livingstone, S.; Andres, A.; Emamaullee, J.; Russell, L.; Coussios, C.; et al. Preliminary Single-Center Canadian Experience of Human Normothermic Ex Vivo Liver Perfusion: Results of a Clinical Trial. Am. J. Transplant. 2017, 17, 1071–1080. [Google Scholar] [CrossRef]
- Schlegel, A.; Muller, X.; Kalisvaart, M.; Muellhaupt, B.; Perera, M.; Isaac, J.R.; Clavien, P.-A.; Muiesan, P.; Dutkowski, P. Outcomes of DCD liver transplantation using organs treated by hypothermic oxygenated perfusion before implantation. J. Hepatol. 2019, 70, 50–57. [Google Scholar] [CrossRef]
- Watson, C.J.E.; Kosmoliaptsis, V.; Randle, L.V.; Gimson, A.E.; Brais, R.; Klinck, J.R.; Hamed, M.; Tsyben, A.; Butler, A.J. Normothermic perfusion in the assessment and preservation of declined livers prior to transplantation. Transplantation 2017, 101, 1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Rijn, R.; Karimian, N.; Matton, A.P.M.; Burlage, L.C.; Westerkamp, A.C.; van den Berg, A.P.; de Kleine, R.H.J.; de Boer, M.T.; Lisman, T.; Porte, R.J. Dual hypothermic oxygenated machine perfusion in liver transplants donated after circulatory death. Br. J. Surg. 2017, 104, 907–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raigani, S.; Markmann, J.F.; Yeh, H. Rehabilitation of Discarded Steatotic Livers Using Ex Situ Normothermic Machine Perfusion: A Future Source of Livers for Transplantation. Liver Transplant. 2019, 25, 991–992. [Google Scholar] [CrossRef] [PubMed]
- Op den Dries, S.; Karimian, N.; Sutton, M.E.; Westerkamp, A.C.; Nijsten, M.W.N.; Gouw, A.S.H.; Wiersema-Buist, J.; Lisman, T.; Leuvenink, H.G.D.; Porte, R.J. Ex vivo normothermic machine perfusion and viability testing of discarded human donor livers. Am. J. Transplant. 2013, 13, 1327–1335. [Google Scholar] [CrossRef]
- Bruinsma, B.G.; Yeh, H.; Özer, S.; Martins, P.N.; Farmer, A.; Wu, W.; Saeidi, N.; Op den Dries, S.; Berendsen, T.A.; Smith, R.N.; et al. Subnormothermic Machine Perfusion for Ex Vivo Preservation and Recovery of the Human Liver for Transplantation. Am. J. Transplant. 2014, 14, 1400–1409. [Google Scholar] [CrossRef] [Green Version]
- Bruinsma, B.G.; Avruch, J.H.; Weeder, P.D.; Sridharan, G.V.; Uygun, B.E.; Karimian, N.G.; Porte, R.J.; Markmann, J.F.; Yeh, H.; Uygun, K. Functional human liver preservation and recovery by means of subnormothermic machine perfusion. J. Vis. Exp. 2015, 98, e52777. [Google Scholar] [CrossRef] [Green Version]
- Bruinsma, B.G.; Sridharan, G.V.; Weeder, P.D.; Avruch, J.H.; Saeidi, N.; Özer, S.; Geerts, S.; Porte, R.J.; Heger, M.; van Gulik, T.M.; et al. Metabolic profiling during ex vivo machine perfusion of the human liver. Sci. Rep. 2016, 6, 22415. [Google Scholar] [CrossRef] [Green Version]
- Bruinsma, B.G.; Avruch, J.H.; Sridharan, G.V.; Weeder, P.D.; Jacobs, M.L.; Crisalli, K.; Amundsen, B.; Porte, R.J.; Markmann, J.F.; Uygun, K.; et al. Peritransplant Energy Changes and Their Correlation to Outcome after Human Liver Transplantation. Transplantation 2017, 101, 1637–1644. [Google Scholar] [CrossRef] [Green Version]
- Karimian, N.; Matton, A.P.M.; Westerkamp, A.C.; Burlage, L.C.; Op den Dries, S.; Leuvenink, H.G.D.; Lisman, T.; Uygun, K.; Markmann, J.F.; Porte, R.J. Ex Situ Normothermic Machine Perfusion of Donor Livers. J. Vis. Exp. 2015, 99, e52688. [Google Scholar] [CrossRef] [Green Version]
- Westerkamp, A.C.; Karimian, N.; Matton, A.P.M.; Mahboub, P.; van Rijn, R.; Wiersema-Buist, J.; de Boer, M.T.; Leuvenink, H.G.D.; Gouw, A.S.H.; Lisman, T.; et al. Oxygenated Hypothermic Machine Perfusion after Static Cold Storage Improves Hepatobiliary Function of Extended Criteria Donor Livers. Transplantation 2016, 100, 825–835. [Google Scholar] [CrossRef] [Green Version]
- Sutton, M.E.; Op Den Dries, S.; Karimian, N.; Weeder, P.D.; De Boer, M.T.; Wiersema-Buist, J.; Gouw, A.S.H.; Leuvenink, H.G.D.; Lisman, T.; Porte, R.J. Criteria for Viability Assessment of Discarded Human Donor Livers during Ex Vivo Normothermic Machine Perfusion. PLoS ONE 2014, 9, e110642. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.; Brockmann, J.G.; Quaglia, A.; Morovat, A.; Jassem, W.; Heaton, N.D.; Coussios, C.C.; Friend, P.J. The 24-h normothermic machine perfusion of discarded human liver grafts. Liver Transplant. 2017, 23, 207–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, N.; Mizuta, K.; Oshima, M.; Yamada, N.; Sanada, Y.; Ihara, Y.; Urahashi, T.; Ishikawa, J.; Tsuji, T.; Hishikawa, S.; et al. A novel split liver protocol using the subnormothermic oxygenated circuit system in a porcine model of a marginal donor procedure. Transplant. Proc. 2015, 47, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, J.G.; Vogel, T.; Coussios, C.; Friend, P.J. Liver splitting during normothermic organ preservation. Liver Transplant. 2017, 23, 701–706. [Google Scholar] [CrossRef]
- Boteon, Y.L.; Laing, R.W.; Schlegel, A.; Wallace, L.; Smith, A.; Attard, J.; Bhogal, R.H.; Neil, D.A.H.; Hubscher, S.; Perera, M.; et al. Combined Hypothermic and Normothermic Machine Perfusion Improves Functional Recovery of Extended Criteria Donor Livers. Liver Transplant. 2018, 24, 1699–1715. [Google Scholar] [CrossRef] [Green Version]
- Berendsen, T.A.; Bruinsma, B.G.; Lee, J.; D’Andrea, V.; Liu, Q.; Izamis, M.-L.; Uygun, K.; Yarmush, M.L.; D ‘andrea, V. A simplified subnormothermic machine perfusion system restores ischemically damaged liver grafts in a rat model of orthotopic liver transplantation. Transplant. Res. 2012, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Fontes, P.; Lopez, R.; Van Der Plaats, A.; Vodovotz, Y.; Minervini, M.; Scott, V.; Soltys, K.; Shiva, S.; Paranjpe, S.; Sadowsky, D.; et al. Liver preservation with machine perfusion and a newly developed cell-free oxygen carrier solution under subnormothermic conditions. Am. J. Transplant. 2015, 15, 381–394. [Google Scholar] [CrossRef]
- Westerkamp, A.C.; Mahboub, P.; Meyer, S.L.; Hottenrott, M.; Ottens, P.J.; Wiersema-Buist, J.; Gouw, A.S.H.; Lisman, T.; Leuvenink, H.G.D.; Porte, R.J. End-ischemic machine perfusion reduces bile duct injury in donation after circulatory death rat donor livers independent of the machine perfusion temperature. Liver Transplant. 2015, 21, 1300–1311. [Google Scholar] [CrossRef] [Green Version]
- Furukori, M.; Matsuno, N.; Meng, L.T.; Shonaka, T.; Nishikawa, Y.; Imai, K.; Obara, H.; Furukawa, H. Subnormothermic Machine Perfusion Preservation with Rewarming for Donation after Cardiac Death Liver Grafts in Pigs. Transplant. Proc. 2016, 48, 1239–1243. [Google Scholar] [CrossRef]
- Hoyer, D.P.; Paul, A.; Luer, S.; Reis, H.; Efferz, P.; Minor, T. End-ischemic reconditioning of liver allografts: Controlling the rewarming. Liver Transplant. 2016, 22, 1223–1230. [Google Scholar] [CrossRef]
- Nassar, A.; Liu, Q.; Farias, K.; Buccini, L.; Baldwin, W.; Bennett, A.; Mangino, M.; Irefin, S.; Cywinski, J.; Okamoto, T.; et al. Impact of Temperature on Porcine Liver Machine Perfusion from Donors after Cardiac Death. Artif. Organs 2016, 40, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Spetzler, V.N.; Goldaracena, N.; Echiverri, J.; Kaths, J.M.; Louis, K.S.; Adeyi, O.A.; Yip, P.M.; Grant, D.R.; Selzner, N.; Selzner, M. Subnormothermic ex vivo liver perfusion is a safe alternative to cold static storage for preserving standard criteria grafts. Liver Transplant. 2016, 22, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Split-Liver Grafts (n = 11) | Whole-Liver Grafts (n = 4) | |
|---|---|---|
| Age (years) | 51 (36–59) | 49 (41–50) |
| Gender (male) | 8 (73%) | 4 (100%) |
| Body mass index (kg/m2) | 28.9 (25–32.4) | 28.2 (26.5–30.7) |
| DCD recovery | 9 (82%) | 4 (100%) |
| Reasons for declining livers for transplantation |
|
|
| Warm ischemia (min) | 31 (24–37) | 26 (24–30) |
| Cold ischemia (min) | Right lobe: 697 (611–760) Left lobe: 669 (543–708) | 724 (694–788) |
| Weight of liver (g) | Right lobe: 1027 (893–1329) Left lobe: 553 (499–677) | 2139 (1892–2376) |
| Donor risk index | 2.14 (1.55–2.37) | 2.06 (1.73–2.47) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, V.; Karimian, N.; Detelich, D.; Raigani, S.; Geerts, S.; Beijert, I.; Fontan, F.M.; Aburawi, M.M.; Ozer, S.; Banik, P.; et al. Split-Liver Ex Situ Machine Perfusion: A Novel Technique for Studying Organ Preservation and Therapeutic Interventions. J. Clin. Med. 2020, 9, 269. https://doi.org/10.3390/jcm9010269
Huang V, Karimian N, Detelich D, Raigani S, Geerts S, Beijert I, Fontan FM, Aburawi MM, Ozer S, Banik P, et al. Split-Liver Ex Situ Machine Perfusion: A Novel Technique for Studying Organ Preservation and Therapeutic Interventions. Journal of Clinical Medicine. 2020; 9(1):269. https://doi.org/10.3390/jcm9010269
Chicago/Turabian StyleHuang, Viola, Negin Karimian, Danielle Detelich, Siavash Raigani, Sharon Geerts, Irene Beijert, Fermin M. Fontan, Mohamed M. Aburawi, Sinan Ozer, Peony Banik, and et al. 2020. "Split-Liver Ex Situ Machine Perfusion: A Novel Technique for Studying Organ Preservation and Therapeutic Interventions" Journal of Clinical Medicine 9, no. 1: 269. https://doi.org/10.3390/jcm9010269
APA StyleHuang, V., Karimian, N., Detelich, D., Raigani, S., Geerts, S., Beijert, I., Fontan, F. M., Aburawi, M. M., Ozer, S., Banik, P., Lin, F., Karabacak, M., Hafiz, E. O. A., Porte, R. J., Uygun, K., Markmann, J. F., & Yeh, H. (2020). Split-Liver Ex Situ Machine Perfusion: A Novel Technique for Studying Organ Preservation and Therapeutic Interventions. Journal of Clinical Medicine, 9(1), 269. https://doi.org/10.3390/jcm9010269