Relationship between Alcohol Hangover and Physical Endurance Performance: Walking the Samaria Gorge

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
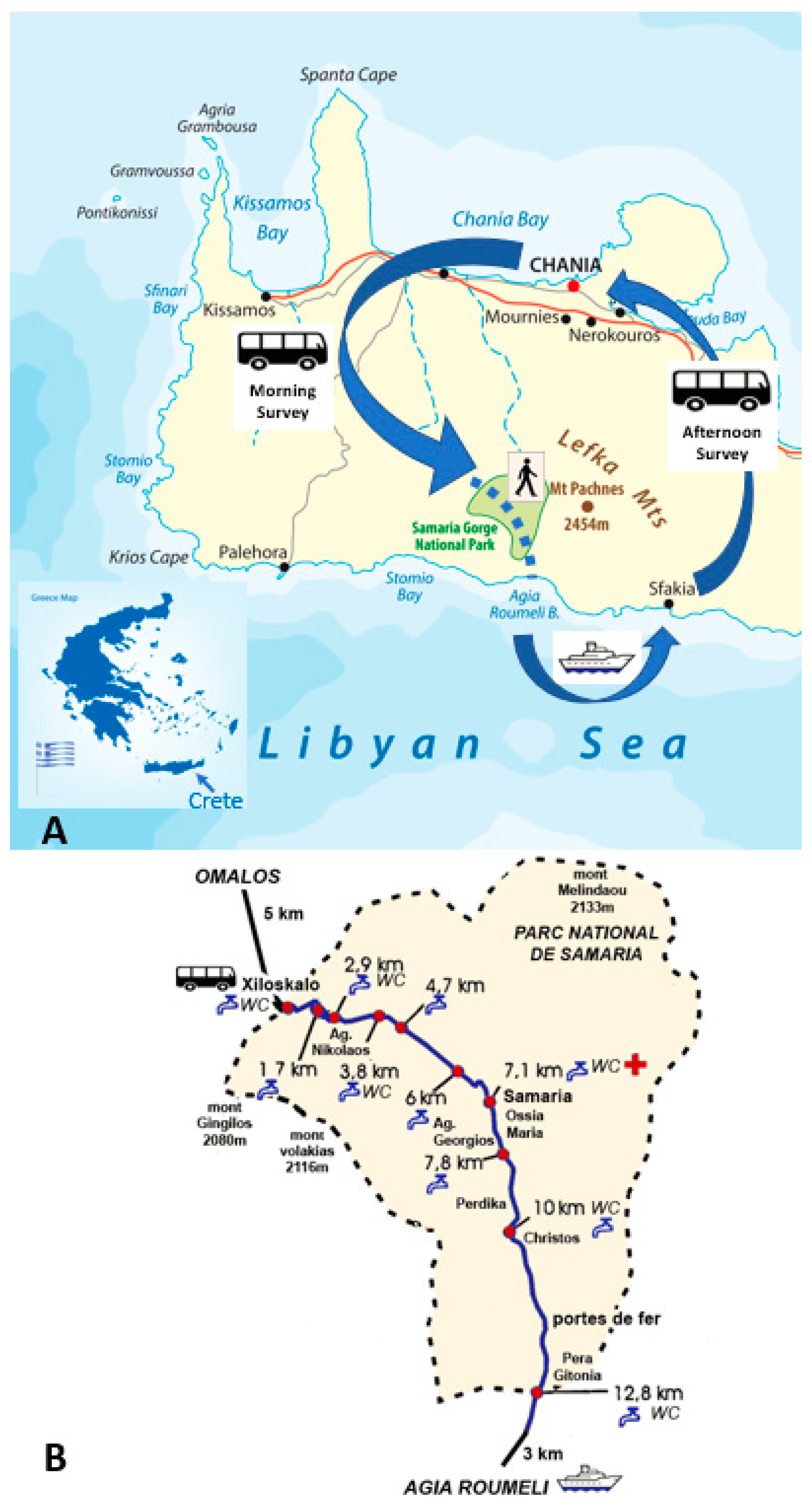
2.1. The Walk
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographics and Physical Activity Levels
3.2. Drinking Characteristics and Hangover Symptom Severity
3.3. Walking Performance
3.4. Correlates of Walking Performance
3.5. Sex Differences
3.6. The Association of Water Consumption and Hangover Severity
3.7. The Association of Alcohol Consumption and Smoking after Walking and Hangover Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Van Schrojenstein Lantman, M.; van de Loo, A.J.; Mackus, M.; Verster, J.C. Development of a definition for the alcohol hangover: Consumer descriptions and expert consensus. Curr. Drug Abuse Rev. 2016, 9, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Gunn, C.; Mackus, M.; Griffin, C.; Munafò, M.R.; Adams, S. A systematic review of the next-day effects of heavy alcohol consumption on cognitive performance. Addiction 2018, 113, 2182–2193. [Google Scholar] [CrossRef] [PubMed]
- McKinney, A. A review of the next day effects of alcohol on subjective mood ratings. Curr. Drug Abuse Rev. 2010, 3, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Frone, M.R. Employee psychoactive substance involvement: Historical context, key findings, and future directions. Annu. Rev. Organ. Psychol. Organ. Behav. 2019, 6, 273–297. [Google Scholar] [CrossRef]
- Bhattacharya, A. Financial Headache. The Cost of Workplace Hangovers and Intoxication to the UK Economy; Institute of Alcohol Studies: London, UK, 2019. [Google Scholar]
- Hartung, B.; Schwender, H.; Mindiashvili, N.; Ritz-Timme, S.; Malczyk, A.; Daldrup, T. The effect of alcohol hangover on the ability to ride a bicycle. Int. J. Legal Med. 2015, 129, 751–758. [Google Scholar] [CrossRef]
- Verster, J.C. Alcohol hangover effects on driving and flying. Int. J. Disabil. Hum. Dev. 2007, 6, 361–367. [Google Scholar] [CrossRef]
- Verster, J.C.; Bervoets, A.C.; de Klerk, S.; Vreman, R.A.; Olivier, B.; Roth, T.; Brookhuis, K.A. Effects of alcohol hangover on simulated highway driving performance. Psychopharmacology 2014, 231, 2999–3008. [Google Scholar] [CrossRef]
- Verster, J.C.; van der Maarel, M.; McKinney, A.; Olivier, B.; de Haan, L. Driving during alcohol hangover among Dutch professional truck drivers. Traffic Inj. Prev. 2014, 15, 434–438. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Mackus, M.; van de Loo, A.J.A.E.; Verster, J.C. The impact of alcohol hangover symptoms on cognitive and physical functioning, and mood. Hum. Psychopharm. 2017, 32, e2623. [Google Scholar] [CrossRef]
- Nelson, D.O. Effects of ethyl alcohol on the performance of a selection of gross motor tests. Res. Q. 1959, 30, 312–320. [Google Scholar]
- Karvinen, E.; Miettinen, M.; Ahlman, K. Physical performance during hangover. Q. J. Stud. Alcohol. 1962, 23, 208–215. [Google Scholar] [PubMed]
- Kruisselbrink, L.D.; Martin, K.L.; Megeney, M.; Fowles, J.R.; Murphy, R.J. Physical and psychomotor functioning of females the morning after consuming low to moderate quantities of beer. J. Stud. Alcohol. 2006, 67, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Devenney, L.E.; Coyle, K.B.; Roth, T.; Verster, J.C. Sleep after heavy alcohol consumption and physical activity levels during alcohol hangover. J. Clin. Med. 2019, 8, E752. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.E.; Watson, I.D.; Batt, R.D. Prediction of blood alcohol concentrations in human subjects. Updating the Widmark Equation. J. Stud. Alcohol. Drugs 1981, 42, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Benjaminsen, J.M.E.; van Lanen, J.H.M.; van Stavel, N.M.D.; Olivier, B. Effects of mixing alcohol with energy drink on objective and subjective intoxication: Results from a Dutch on-premise study. Psychopharmacology 2015, 232, 835–842. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; van Andel, N.; van Gelder, C.A.G.H.; Janssen, B.S.G.; Titulaer, J.; Jansen, J.; Verster, J.C. The effects of alcohol mixed with energy drink (AMED) on subjective intoxication and alertness: Results from a double-blind placebo-controlled clinical trial. Hum. Psychopharmacol. 2016, 31, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.M.; Rohsenow, D.J.; Piasecki, T.M.; Howland, J.; Richardson, A.E. Role of tobacco smoking in hangover symptoms among university students. J. Stud. Alcohol. Drugs 2013, 74, 41–49. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Mackus, M.; Roth, T.; Verster, J.C. Total sleep time, alcohol consumption and the duration and severity of alcohol hangover. Nat. Sci. Sleep 2017, 9, 181–186. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Roth, T.; Roehrs, T.; Verster, J.C. Alcohol hangover, sleep quality, and daytime sleepiness. Sleep Vigil. 2017, 1, 37–41. [Google Scholar] [CrossRef]
- Donners, A.A.M.T.; Tromp, M.D.P.; Garssen, J.; Roth, T.; Verster, J.C. Perceived immune status and sleep: A survey among Dutch students. Sleep Disord. 2015, 2015, 721607. [Google Scholar] [CrossRef]
- Abdulahad, S.; Huls, H.; Balikji, S.; van de Loo, A.J.A.E.; Roth, T.; Verster, J.C. Irritable bowel syndrome, immune fitness and insomnia: Results from an online survey among people with sleep complaints. Sleep Vigil. 2019, 3, 121–129. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Hogewoning, A.; van de Loo, A.J.A.E.; Mackus, M.; Raasveld, S.J.; de Zeeuw, R.; Bosma, E.R.; Bouwmeester, N.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Characteristics of social drinkers with and without a hangover after heavy alcohol consumption. Subst. Abuse Rehab. 2016, 7, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Wilod Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Kraneveld, A.D.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Otten, L.S.; Mackus, M.; de Kruijff, D.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef]
- Mackus, M.; de Kruijff, D.; Otten, L.S.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Differential gender effects in the relationship between perceived immune functioning and autism spectrum disorder scores. Int. J. Environ. Res. Public Health 2017, 14, 409. [Google Scholar] [CrossRef]
- Verster, J.C.; van de Loo, A.J.A.E.; Adams, S.; Stock, A.-K.; Benson, S.; Alford, C.; Scholey, A.; Bruce, G. Naturalistic study design in alcohol hangover research: Advantages, limitations, and solutions. J. Clin. Med. 2019, 8, 2160. [Google Scholar] [CrossRef]
- Verster, J.C.; Stephens, R.; Penning, R.; Rohsenow, D.; McGeary, J.; Levy, D.; McKinney, A.; Finnigan, F.; Piasecki, T.M.; Adan, A.; et al. The Alcohol Hangover Research Group consensus statement on best practice in alcohol hangover research. Curr. Drug Abuse Rev. 2010, 3, 116–127. [Google Scholar] [CrossRef]
- Verster, J.C.; Kruisselbrink, L.D.; Slot, K.A.; Anogeianaki, A.; Adams, S.; Alford, C.; Arnoldy, L.; Ayre, E.; Balikji, S.; Benson, S.; et al. Sensitivity to experiencing alcohol hangovers: Reconsideration of the 0.11% blood alcohol concentration (BAC) threshold for having a hangover. J. Clin. Med. 2019, 9, 179. [Google Scholar]
- Van de Loo, A.J.A.E.; Mackus, M.; van Schrojenstein Lantman, M.; Kraneveld, A.D.; Garssen, J.; Scholey, A.; Verster, J.C. Susceptibility to alcohol hangovers: The association with self-reported immune status. Int. J. Environ. Res. Public Health 2018, 15, 1286. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; van Schrojenstein Lantman, M.; Mackus, M.; Scholey, A.; Verster, J.C. Impact of mental resilience and perceived immune functioning on the severity of alcohol hangover. BMC Res. Notes 2018, 11, 526. [Google Scholar] [CrossRef] [PubMed]
- Kösem, Z.; van de Loo, A.J.A.E.; Fernstrand, A.M.; Garssen, J.; Verster, J.C. The impact of consuming food or drinking water on alcohol hangover. Eur. Neuropsychopharm. 2015, 25, S604. [Google Scholar] [CrossRef]
- Verster, J.C. The “hair of the dog”: A useful hangover remedy or a predictor of future problem drinking? Curr. Drug Abuse Rev. 2009, 2, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hunt-Carter, E.E.; Slutske, W.S.; Piasecki, T.M. Characteristics and correlates to relieve hangover in a college sample. Alcohol. Clin. Exp. Res. 2005, 29, 152A. [Google Scholar]
- Penning, R.; McKinney, A.; Bus, L.D.; Olivier, B.; Slot, K.; Verster, J.C. Measurement of alcohol hangover severity: Development of the alcohol hangover severity scale (AHSS). Psychopharmacology 2013, 225, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Slutske, W.S.; Piasecki, T.M.; Hunt-Carter, E.E. Development and initial validation of the Hangover Symptoms Scale: Prevalence and correlate of hangover symptoms in college students. Alcohol. Clin. Exp. Res. 2003, 27, 1442–1450. [Google Scholar] [CrossRef]
- Rohsenow, D.J.; Howland, J.; Minsky, S.J.; Greece, J.; Almeida, A.; Roehrs, T.A. The acute hangover scale: A new measure of immediate hangover symptoms. Addict. Behav. 2007, 32, 1314–1320. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Overall | No Alcohol | Alcohol, No Hangover | Alcohol, Hangover | p-Value |
|---|---|---|---|---|---|
| N | 299 | 76 | 47 | 176 | |
| Age (years) | 38.9 (11.0) | 39.4 (12.1) | 37.5 (11.4) | 39.0 (10.3) | 0.506 |
| BMI (kg/m2) | 23.9 (2.4) | 23.5 (2.4) | 24.4 (2.7) | 24.0 (2.4) | 0.061 |
| ISQ | 8.6 (1.9) | 8.8 (1.9) | 7.6 (2.5) ‡ | 8.7 (1.5) | 0.006 |
| General health | 7.4 (1.1) | 7.5 (1.0) | 7.9 (1.2) | 7.3 (1.0) | 0.005 |
| Weekly alcohol consumption at home | 4.8 (3.6) | 2.0 (1.7) | 4.5 (4.0) ‡ | 5.9 (3.3) *Χ | 0.000 |
| Physical activity at home | |||||
| Vigorous (MET-min/w) | 961 (1728) | 879 (1937) | 1351 (1757) ‡ | 883 (1617) * | 0.035 |
| Moderate (MET-min/w) | 1869 (2470) | 1928 (3048) | 2004 (3868) | 1806 (1551) | 0.100 |
| Walking (MET-min/w) | 3298 (2240) | 3511 (1913) | 2937 (3725) ‡ | 3305 (1810) * | 0.004 |
| Total (MET-min/w) | 5972 (4231) | 6124 (4130) | 6201 (6008) | 5843 (3666) | 0.637 |
| Time spent sitting (min) | 385 (119) | 404 (121) | 382 (150) | 377 (108) | 0.490 |
| On holiday in Crete | |||||
| Vigorous (MET-min/w) | 708 (1432) | 823 (1722) | 892 (1406) | 611 (1299) | 0.258 |
| Moderate (MET-min/w) | 1588 (1531) | 1665 (1766) | 1319 (1981) | 1627 (1273) * | 0.019 |
| Walking (MET-min/w) | 3409 (2361) | 4099 (2964) | 3319 (2953) ‡ | 3141 (1788) Χ | 0.028 |
| Total (MET-min/w) | 5588 (3937) | 6498 (4569) | 5536 (4979) | 5219 (4274) | 0.155 |
| Time spent sitting (min) | 353 (111) | 355 (114) | 291 (117) ‡ | 369 (102) | 0.000 |
| Evening before | |||||
| Number of cigarettes smoked | 3.7 (5.9) | 0.8 (2.8) | 1.3 (3.1) ‡ | 5.6 (6.6) * Χ | 0.000 |
| Total sleep time (h) | 6.1 (0.8) | 6.3 (0.8) | 6.2 (1.2) | 5.9 (0.6) * Χ | 0.000 |
| Number of nightly awakenings | 1.1 (1.0) | 0.9 (1.0) | 1.1 (1.2) | 1.3 (0.9) Χ | 0.006 |
| Sleep quality | 6.1 (1.9) | 7.2 (1.9) | 7.1 (1.6) | 5.4 (1.6) * Χ | 0.000 |
| No Alcohol | No Hangover | Hangover | p-Value | |
|---|---|---|---|---|
| Evening before walking | ||||
| Number of alcoholic drinks | 0.0 (0.0) | 0.9 (1.6) | 3.0 (1.8) | 0.000 * |
| Subjective intoxication | --- | 1.3 (1.9) | 4.6 (2.4) | 0.000 * |
| Start time drinking (h.min) | --- | 19.10 (2.4) | 17.40 (1.8) | 0.000 * |
| Stop time drinking (h.min) | --- | 21.45 (1.9) | 20.13 (1.9) | 0.000 * |
| Duration of drinking (h) | --- | 2.6 (2.4) | 2.5 (1.5) | 0.157 |
| Estimated BAC (%) | --- | 0.02 (0.03) | 0.03 (0.03) | 0.001 * |
| Test day | ||||
| Overall hangover severity before walking | --- | 0.0 (0.0) | 4.6 (2.1) | 0.000 * |
| Overall hangover severity during walking | --- | 1.1 (1.8) | 3.4 (2.3) | 0.000 * |
| Overall hangover severity after walking | --- | 1.1 (2.1) | 3.5 (2.4) | 0.000 * |
| Afternoon after walking | ||||
| Number of alcoholic drinks | 0.4 (0.9) | 1.0 (1.7) | 1.0 (1.3) | 0.112 |
| Subjective intoxication | 0.6 (1.6) | 0.9 (2.1) | 1.5 (2.0) | 0.010 * |
| Number of cigarettes smoked | 0.4 (1.5) | 1.0 (2.3) | 3.4 (4.5) | 0.000 * |
| Group | No Alcohol N = 76 | No Hangover (in the Morning) N = 47 | Hangover (in the Morning) N = 176 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Symptom | Before | During | After | Before | During | After | Before | During | After |
| Fatigue | 3.6 (2.0) | 5.0 (2.4) bd | 5.3 (2.3) | 2.6 (1.9) | 5.9 (2.7) bd | 6.1 (2.5) ba | 6.1 (1.7) *, Χ | 6.3 (1.6) Χ | 6.3 (1.7) Χ |
| Sleepiness | 4.0 (2.5) | 3.6 (2.5) | 4.1 (2.4) | 2.5 (2.3) | 3.7 (3.1) | 4.2 (3.0) | 6.5 (2.0) *, Χ | 4.8 (2.6) bd | 5.3 (2.3) Χ, ba |
| Thirst | 2.1 (2.3) | 3.8 (2.8) bd | 4.1 (2.9) | 2.3 (2.2) | 5.1 (2.8) bd | 5.1 (2.5) ba | 5.6 (2.8) *, Χ | 5.1 (2.6) | 5.2 (2.6) |
| Headache | 0.7 (1.7) | 0.6 (1.4) | 1.0 (2.1) | 0.4 (0.9) | 1.6 (2.6) | 0.8 (1.4) | 2.2 (3.0) Χ | 0.9 (1.7) bd | 1.1 (2.0) ba |
| Nausea | 0.3 (0.7) | 0.3 (0.9) | 0.3 (1.1) | 0.1 (0.3) | 0.5 (1.2) | 0.3 (0.9) | 0.8 (1.6) | 0.4 (0.9) bd | 0.4 (1.3) |
| Dizziness | 0.4 (1.2) | 0.4 (1.0) | 0.7 (1.5) | 1.0 (1.8) | 0.6 (1.2) | 0.9 (1.7) | 1.3 (1.7) *, Χ | 0.6 (1.2) bd | 0.9 (1.6) |
| Stomach pain | 0.6 (1.4) | 0.4 (1.1) | 0.7 (1.5) | 0.3 (0.8) | 0.6 (1.1) | 0.8 (1.5) | 2.1 (2.2) *, Χ | 0.9 (1.5) bd | 1.0 (1.4) ba |
| Heart racing | 0.7 (1.6) | 1.5 (2.0) | 1.2 (2.0) | 0.3 (0.7) | 2.8 (2.7) bd | 2.6 (2.3) ba, ‡ | 2.3 (2.1) *, Χ | 2.1 (2.0) | 1.9 (1.7) Χ |
| Weakness | 0.6 (1.2) | 2.2 (2.2) bd | 2.0 (2.1) | 0.5 (0.8) | 2.8 (2.1) bd | 2.6 (2.5) | 2.3 (1.9) Χ | 2.9 (1.9) | 2.4 (1.9) |
| Loss of appetite | 1.0 (1.9) | NA | 0.6 (1.6) | 1.4 (1.8) | NA | 1.1 (1.6) | 1.0 (1.7) | NA | 0.5 (1.2) |
| Anxiety | 0.6 (1.1) | NA | 0.5 (1.3) | 0.7 (1.6) | NA | 0.2 (0.6) | 1.2 (1.6) | NA | 0.8 (1.2) |
| Depression | 0.1 (0.5) | NA | 0.2 (0.8) | 0.3 (1.0) | NA | 0.0 (0.3) | 0.3 (1.0) | NA | 0.1 (0.5) |
| Tension, stress | 0.6 (1.5) | NA | 0.6 (1.7) | 0.7 (1.5) | NA | 0.5 (1.6) | 0.4 (1.0) | NA | 0.4 (0.9) |
| Anger, hostility | 0.2 (0.7) | NA | 0.3 (0.7) | 0.6 (1.5) | NA | 0.4 (1.0) | 0.3 (0.9) | NA | 0.3 (0.7) |
| No Alcohol | Alcohol, no Hangover | Alcohol, Hangover | p-Value | |
|---|---|---|---|---|
| Assessed before walking | ||||
| Immune fitness | 7.5 (1.3) | 8.3 (1.5) ‡ | 7.3 (1.2) * | 0.000 |
| Mental fitness | 8.6 (1.3) | 8.6 (1.2) | 8.5 (1.2) | 0.628 |
| Physical fitness | 6.9 (1.5) | 7.4 (1.8) | 6.8 (1.4) | 0.057 |
| Expected effort to walk the Gorge | 8.0 (1.9) | 6.6 (1.9) ‡ | 8.4 (1.4) | 0.000 |
| Assessed after walking | ||||
| Immune fitness | 6.9 (1.2) | 6.8 (1.7) | 6.3 (1.4) Χ | 0.003 |
| Mental fitness | 7.9 (1.4) | 7.8 (1.7) | 7.7 (1.5) | 0.636 |
| Physical fitness | 6.8 (1.3) | 6.4 (1.8) | 6.1 (1.4) Χ | 0.004 |
| Effort to walk the Gorge | 8.1 (1.4) | 7.9 (1.7) | 8.3 (1.5) | 0.135 |
| Exhaustion | 8.3 (1.4) | 7.8 (2.2) | 8.8 (1.4) * Χ | 0.002 |
| Walking time (hours) | 6.1 (0.7) | 6.1 (0.9) | 6.0 (0.6) | 0.734 |
| Number of breaks | 4.3 (1.7) | 4.4 (1.9) | 4.0 (1.1) | 0.666 |
| Total duration of breaks (minutes) | 24.3 (12.5) | 26.7 (19.0) | 25.6 (8.7) | 0.227 |
| Water consumed during the walk (liters) | 2.3 (0.9) | 2.4 (0.8) | 2.7 (0.7) * Χ | 0.001 |
| Predictive Validity of the Model | Contribution of Individual Variables | |
|---|---|---|
| Exhaustion | 11.0% | Physical fitness rate before walking (6.3%) Group (2.6%) Physical activity (total METs) in Crete (2.1%) |
| Effort | 29.6% | Physical activity (total METs) in Crete (14.5%) Physical fitness rate before walking (6.7%) Number of cigarettes smoked (3.4%) Group (1.9%) Number of alcoholic drinks consumed (1.6%) BMI (1.5%) |
| Duration of the walk | 29.2% | Physical fitness rate before walking (11.0%) Physical activity (total METs) in Crete (5.1%) BMI (3.7%) Past year’s immune status (ISQ) (3.7%) Usual weekly alcohol consumption (3.0%) Time spent sitting on a week day in Crete (2.7%) |
| Number of breaks | 19.9% | Time spent sitting on a week day at home (7.9%) BMI (3.7%) Physical activity (total METs) in Crete (3.5%) Sex (2.9%) Group (1.9%) |
| Total duration of breaks | 17.5% | Usual weekly alcohol consumption (6.5%) BMI (6.2%) Duration of drinking evening before (4.8%) |
| Amount of water consumed | 21.1% | Sex (15.1%) Physical activity (total METs) in Crete (7.2%) Past year’s immune status (ISQ) (5.2%) BMI (3.2%) Physical fitness rate before walking (1.4%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verster, J.C.; Anogeianaki, A.; Kruisselbrink, D.; Alford, C.; Stock, A.-K. Relationship between Alcohol Hangover and Physical Endurance Performance: Walking the Samaria Gorge. J. Clin. Med. 2020, 9, 114. https://doi.org/10.3390/jcm9010114
Verster JC, Anogeianaki A, Kruisselbrink D, Alford C, Stock A-K. Relationship between Alcohol Hangover and Physical Endurance Performance: Walking the Samaria Gorge. Journal of Clinical Medicine. 2020; 9(1):114. https://doi.org/10.3390/jcm9010114
Chicago/Turabian StyleVerster, Joris C, Aikaterini Anogeianaki, Darren Kruisselbrink, Chris Alford, and Ann-Kathrin Stock. 2020. "Relationship between Alcohol Hangover and Physical Endurance Performance: Walking the Samaria Gorge" Journal of Clinical Medicine 9, no. 1: 114. https://doi.org/10.3390/jcm9010114
APA StyleVerster, J. C., Anogeianaki, A., Kruisselbrink, D., Alford, C., & Stock, A.-K. (2020). Relationship between Alcohol Hangover and Physical Endurance Performance: Walking the Samaria Gorge. Journal of Clinical Medicine, 9(1), 114. https://doi.org/10.3390/jcm9010114