Infliximab Induced a Dissociated Response of Severe Periodontal Biomarkers in Rheumatoid Arthritis Patients




Abstract
1. Introduction
2. Patients and methods
2.1. Patients and Controls
2.2. Methods
2.2.1. Determination of Anti-P. gingivalis and Anti-P. intermedia Whole Extract Antibodies by ELISA
2.2.2. Assessments of ACPA, R.F., and MMP-3
2.3. Statistical Analysis
3. Results
3.1. RA Population
3.2. Immunity Against Oral Pathogens is Related to Established RA
3.3. Anti-P. gingivalis and anti-P. Intermedia Antibodies and RA Specificity
3.4. Differential Implication of P. Gingivalis and P. Intermedia Antibodies in Immune Response in RA Patients
3.5. Clinical Response to Infliximab Therapy and Joint or Periodontal Destructions
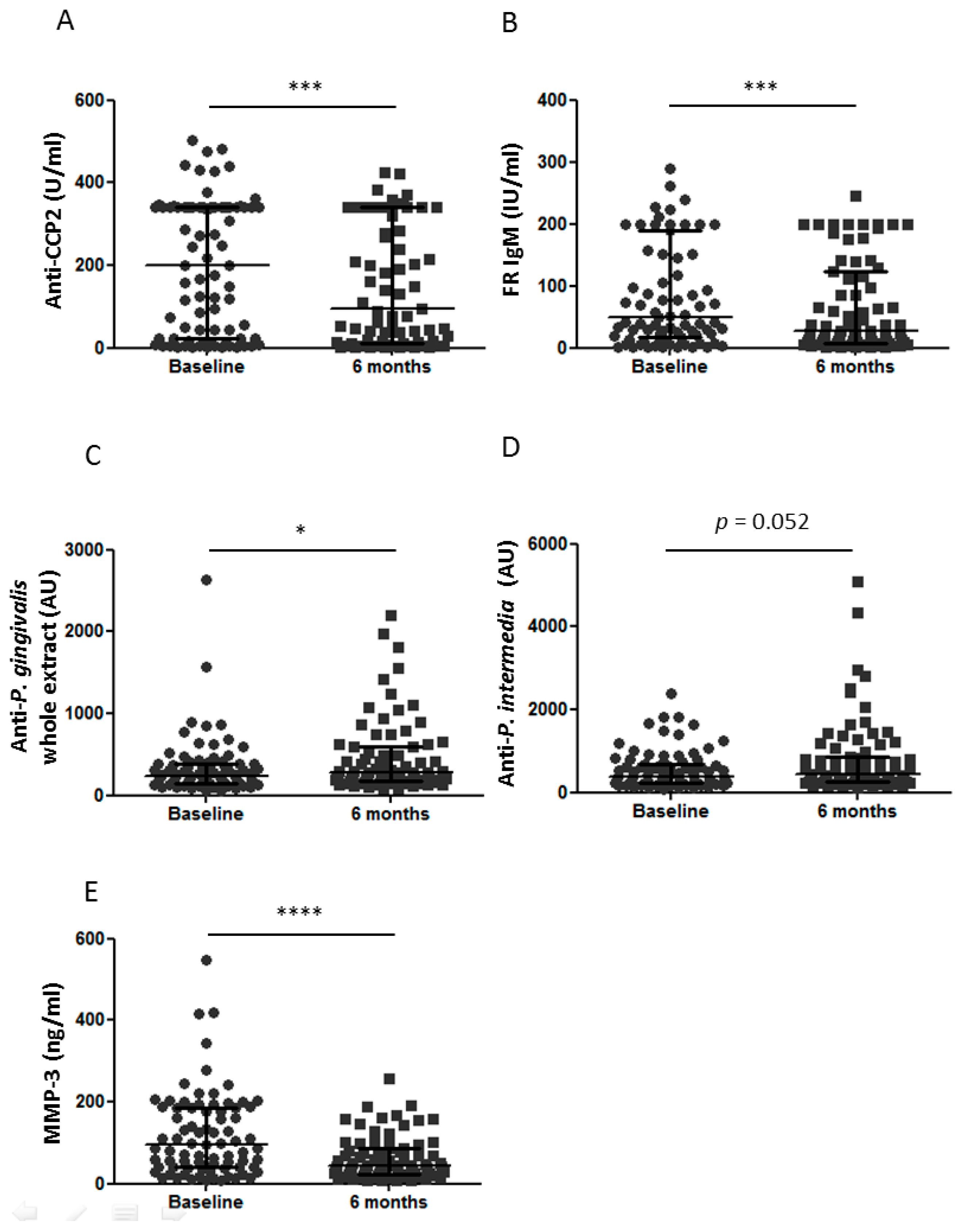
3.6. Dissociated Effect of Infliximab Therapy on PD Biological Markers
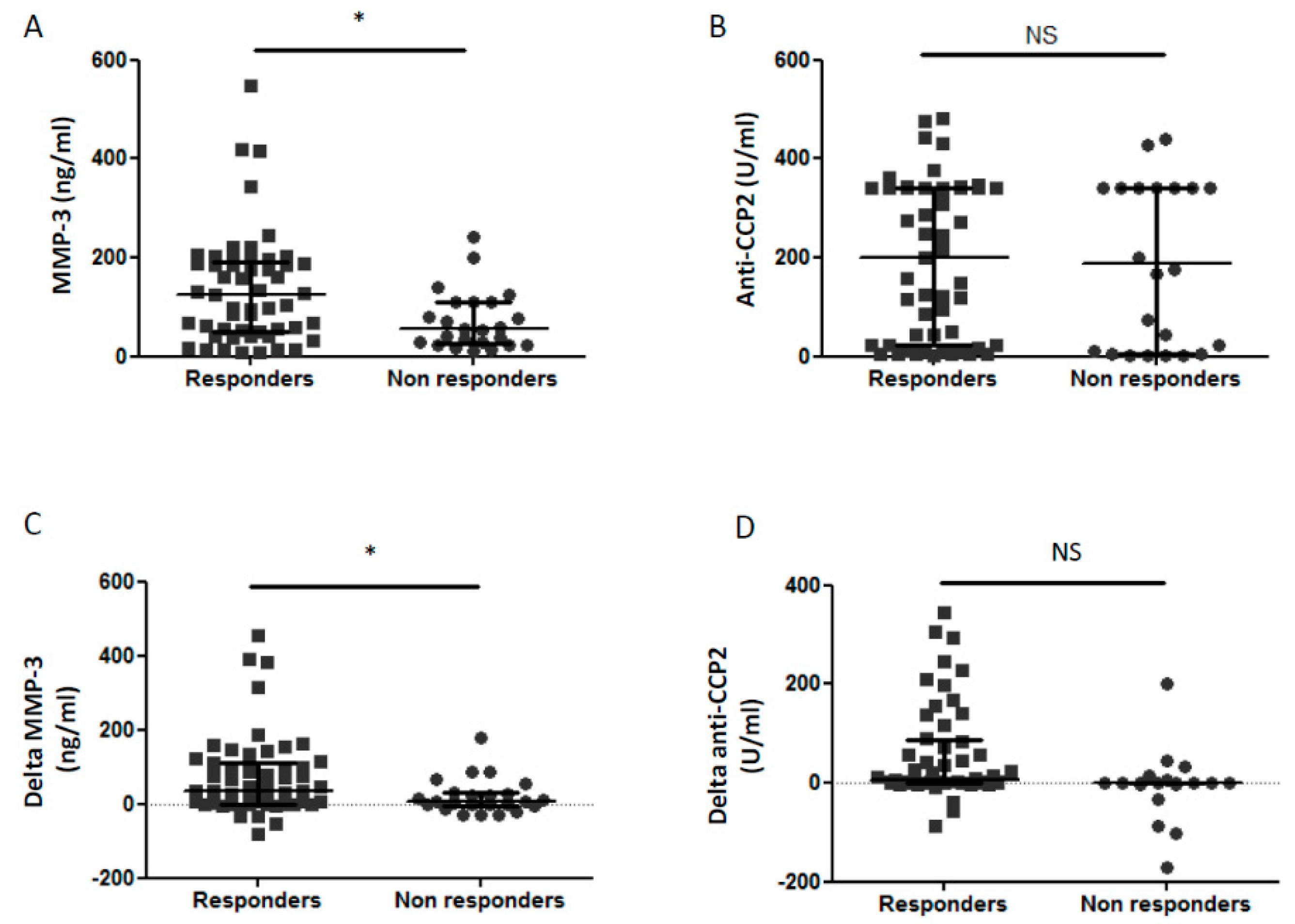
3.7. Biological Markers and Prediction of Clinical Response
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Fuggle, N.R.; Smith, T.O.; Kaul, A.; Sofat, N. Hand to Mouth: A Systematic Review and Meta-Analysis of the Association between Rheumatoid Arthritis and Periodontitis. Front. Immunol. 2016, 7, 80. [Google Scholar] [CrossRef]
- Marotte, H.; Farge, P.; Gaudin, P.; Alexandre, C.; Mougin, B.; Miossec, P. The association between periodontal disease and joint destruction in rheumatoid arthritis extends the link between the HLA-DR shared epitope and severity of bone destruction. Ann. Rheum. Dis. 2006, 65, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, E.D.; Greenwald, R.A.; Kushner, L.J.; Weissmann, G. Hypothesis: The humoral immune response to oral bacteria provides a stimulus for the development of rheumatoid arthritis. Inflammation 2004, 28, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Courbon, G.; Rinaudo-Gaujous, M.; Blasco-Baque, V.; Auger, I.; Caire, R.; Mijola, L.; Vico, L.; Paul, S.; Marotte, H. Porphyromonas gingivalis experimentally induces periodontis and an anti-CCP2-associated arthritis in the rat. Ann. Rheum. Dis. 2019, 78, 594–599. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, D.; Jia, H.; Feng, Q.; Wang, D.; Liang, D.; Wu, X.; Li, J.; Tang, L.; Li, Y.; et al. The oral and gut microbiomes are perturbed in rheumatoid arthritis and partly normalized after treatment. Nat. Med. 2015, 21, 895–905. [Google Scholar] [CrossRef] [PubMed]
- György, B.; Tóth, E.; Tarcsa, E.; Falus, A.; Buzás, E.I. Citrullination: A posttranslational modification in health and disease. Int. J. Biochem. Cell Biol. 2006, 38, 1662–1677. [Google Scholar] [CrossRef]
- Klareskog, L.; Rönnelid, J.; Lundberg, K.; Padyukov, L.; Alfredsson, L. Immunity to citrullinated proteins in rheumatoid arthritis. Annu. Rev. Immunol. 2008, 26, 651–675. [Google Scholar] [CrossRef] [PubMed]
- Nielen, M.M.J.; Van Schaardenburg, D.; Reesink, H.W.; Van De Stadt, R.J.; Van Der Horst-Bruinsma, I.E.; De Koning, M.H.M.T.; Habibuw, M.R.; Vandenbroucke, J.P.; Dijkmans, B.A.C.; Van Der Horst-Bruinsma, I.E. Specific autoantibodies precede the symptoms of rheumatoid arthritis: A study of serial measurements in blood donors. Arthritis Rheum. 2004, 50, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, K.; Wegner, N.; Yucel-Lindberg, T.; Venables, P.J. Periodontitis in RA-the citrullinated enolase connection. Nat. Rev. Rheumatol. 2010, 6, 727–730. [Google Scholar] [CrossRef]
- Mangat, P.; Wegner, N.; Venables, P.J.; Potempa, J. Bacterial and human peptidylarginine deiminases: Targets for inhibiting the autoimmune response in rheumatoid arthritis? Arthritis Res. Ther. 2010, 12, 209. [Google Scholar] [CrossRef] [PubMed]
- Wegner, N.; Wait, R.; Sroka, A.; Eick, S.; Nguyen, K.-A.; Lundberg, K.; Kinloch, A.; Culshaw, S.; Potempa, J.; Venables, P.J.; et al. Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and α-enolase: Implications for autoimmunity in rheumatoid arthritis. Arthritis Rheum. 2010, 62, 2662–2672. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Le Gall-David, S.; Bonnaure-Mallet, M.; Schaeverbeke, T.; Cantagrel, A.; Minet, J.; Gottenberg, J.-E.; Chanson, P.; Ravaud, P.; Mariette, X. Association of Anti-Porphyromonas gingivalis Antibody Titers with Nonsmoking Status in Early Rheumatoid Arthritis: Results from the Prospective French Cohort of Patients with Early Rheumatoid Arthritis: Anti-Porphyromonas Gingivalis Antibody and Early RA. Arthritis Rheumatol. 2015, 67, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Mikuls, T.R.; Payne, J.B.; Yu, F.; Thiele, G.M.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis and Porphyromonas gingivalis in Patients with Rheumatoid Arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Mikuls, T.R.; Payne, J.B.; Reinhardt, R.A.; Thielea, G.M.; Maziarz, E.; Cannell, A.C.; Holers, V.M.; Kuhnc, K.A.; O’Dell, J.R. Antibody responses to Porphyromonas gingivalis (P. gingivalis) in subjects with rheumatoid arthritis and periodontitis. Int. Immunopharmacol. 2009, 9, 38–42. [Google Scholar] [CrossRef]
- Okada, Y.; Nagase, H.; Harris, E.D. A metalloproteinase from human rheumatoid synovial fibroblasts that digests connective tissue matrix components. Purification and characterization. J. Biol. Chem. 1986, 261, 14245–14255. [Google Scholar]
- Toyman, U.; Tüter, G.; Kurtiş, B.; Kıvrak, E.; Bozkurt, Ş.; Yücel, A.A.; Serdar, M. Evaluation of gingival crevicular fluid levels of tissue plasminogen activator, plasminogen activator inhibitor 2, matrix metalloproteinase-3 and interleukin 1-β in patients with different periodontal diseases. J. Periodontal Res. 2015, 50, 44–51. [Google Scholar] [CrossRef]
- Zhao, Y.; Jin, Y.; Ren, Y.; Song, L.M.; Li, J.; Lin, X.P. Expression of matrix metalloproteinase-3 in patients with rheumatoid arthritis and its correlation with chronic periodontitis and rheumatoid arthritis. Zhonghua Kou Qiang Yi Xue Za Zhi 2019, 54, 164–169. [Google Scholar]
- da Silva, M.K.; de Carvalho, A.C.G.; Alves, E.H.P.; da Silva, F.R.P.; Pessoa, L.D.S.; Vasconcelos, D.F.P. Genetic Factors and the Risk of Periodontitis Development: Findings from a Systematic Review Composed of 13 Studies of Meta-Analysis with 71,531 Participants. Int. J. Dent. 2017, 2017, 1914073. [Google Scholar] [CrossRef]
- Urata, Y.; Uesato, R.; Tanaka, D.; Nakamura, Y.; Motomura, S. Treating to target matrix metalloproteinase 3 normalisation together with disease activity score below 2.6 yields better effects than each alone in rheumatoid arthritis patients: T-4 Study. Ann. Rheum. Dis. 2012, 71, 534–540. [Google Scholar] [CrossRef]
- Marotte, H.; Miossec, P. Biomarkers for prediction of TNFalpha blockers response in rheumatoid arthritis. Jt. Bone Spine 2010, 77, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Savioli, C.; Ribeiro, A.C.M.; Fabri, G.M.C.; Calich, A.L.; Carvalho, J.; Silva, C.A.; Viana, V.S.; Bonfá, E.; Siqueira, J.T.T. Persistent periodontal disease hampers anti-tumor necrosis factor treatment response in rheumatoid arthritis. J. Clin. Rheumatol. 2012, 18, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Yoshida, S.; Takeuchi, T.; Yoshikawa, A.; Hiramatsu, Y.; Ishida, T.; Makino, S.; Takasugi, Y.; Hanafusa, T. Periodontal pathogens participate in synovitis in patients with rheumatoid arthritis in clinical remission: A retrospective case–control study. Rheumatology 2015. [Google Scholar] [CrossRef] [PubMed]
- Marotte, H. Tooth-brushing: An impact on rheumatoid arthritis. Jt. Bone Spine 2016, 83, 619–621. [Google Scholar] [CrossRef]
- Pers, J.-O.; Saraux, A.; Pierre, R.; Youinou, P. Anti-TNF-alpha immunotherapy is associated with increased gingival inflammation without clinical attachment loss in subjects with rheumatoid arthritis. J. Periodontol. 2008, 79, 1645–1651. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lozano, B.; González-Febles, J.; Garnier-Rodríguez, J.L.; Dadlani, S.; Bustabad-Reyes, S.; Sanz, M.; Sánchez-Alonso, F.; Sánchez-Piedra, C.; González-Dávila, E.; Díaz-González, F. Association between severity of periodontitis and clinical activity in rheumatoid arthritis patients: A case-control study. Arthritis Res. Ther. 2019, 21, 27. [Google Scholar] [CrossRef]
- Coat, J.; Demoersman, J.; Beuzit, S.; Cornec, D.; Devauchelle-Pensec, V.; Saraux, A.; Pers, J.-O.; Devauchelle-Pensec, V. Anti-B lymphocyte immunotherapy is associated with improvement of periodontal status in subjects with rheumatoid arthritis. J. Clin. Periodontol. 2015, 42, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Okada, M.; Ito, S.; Kobayashi, D.; Ishida, K.; Kojima, A.; Narita, I.; Murasawa, A.; Yoshie, H. Assessment of interleukin-6 receptor inhibition therapy on periodontal condition in patients with rheumatoid arthritis and chronic periodontitis. J. Periodontol. 2014, 85, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Kobayashi, T.; Ito, S.; Yokoyama, T.; Abe, A.; Murasawa, A.; Yoshie, H. Periodontal Treatment Decreases Levels of Antibodies to Porphyromonas gingivalis and Citrulline in Patients with Rheumatoid Arthritis and Periodontitis. J. Periodontol. 2013, 84, e74–e84. [Google Scholar] [CrossRef] [PubMed]
- Burt, B. Research, Science and Therapy Committee of the American Academy of Periodontology. Position paper: Epidemiology of periodontal diseases. J. Periodontol. 2005, 76, 1406–1419. [Google Scholar] [CrossRef] [PubMed]
- Scher, J.U.; Ubeda, C.; Equinda, M.; Khanin, R.; Buischi, Y.; Viale, A.; Lipuma, L.; Attur, M.; Pillinger, M.H.; Weissmann, G.; et al. Periodontal disease and the oral microbiota in new-onset rheumatoid arthritis. Arthritis Rheum. 2012, 64, 3083–3094. [Google Scholar] [CrossRef]
- Ogrendik, M.; Kokino, S.; Ozdemir, F.; Bird, P.S.; Hamlet, S. Serum antibodies to oral anaerobic bacteria in patients with rheumatoid arthritis. MedGenMed 2005, 7, 2. [Google Scholar] [PubMed]
- Bender, P.; Bürgin, W.B.; Sculean, A.; Eick, S. Serum antibody levels against Porphyromonas gingivalis in patients with and without rheumatoid arthritis—A systematic review and meta-analysis. Clin. Oral Investig. 2017, 21, 33–42. [Google Scholar] [CrossRef]
- Cheng, Z.; Meade, J.; Mankia, K.; Emery, P.; Devine, D.A. Periodontal disease and periodontal bacteria as triggers for rheumatoid arthritis. Best Pr. Res. Clin. Rheumatol. 2017, 31, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; van Deuren, M.; Kullberg, B.J.; Cavaillon, J.M.; Van der Meer, J.W. Does the shape of lipid A determine the interaction of LPS with Toll-like receptors? Trends Immunol. 2002, 23, 135–139. [Google Scholar] [CrossRef]
- Goh, C.E.; Kopp, J.; Papapanou, P.N.; Molitor, J.A.; Demmer, R.T. Association Between Serum Antibodies to Periodontal Bacteria and Rheumatoid Factor in the Third National Health and Nutrition Examination Survey: Periodontal Bacteria Antibodies and Rheumatoid Factor. Arthritis Rheumatol. 2016, 68, 2384–2393. [Google Scholar] [CrossRef]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Transl. Med. 2016, 8, 369ra176. [Google Scholar] [CrossRef]
- Omura, K.; Takahashi, M.; Omura, T.; Miyamoto, S.; Kushida, K.; Sano, Y.; Nagano, A. Changes in the concentration of plasma matrix metalloproteinases (MMPs) and tissue inhibitor of metalloproteinases-1 (TIMP-1) after total joint replacement in patients with arthritis. Clin. Rheumatol. 2002, 21, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Reddy, N.R.; Roopa, D.; Babu, D.S.M.; Kumar, P.M.; Raju, C.M.; Kumar, N.S.; Reddy, N.; Raju, C.; Kumar, P.; Reddy, N.R.; et al. Estimation of matrix metalloproteinase-3 levels in gingival crevicular fluid in periodontal disease, health and after scaling and root planing. J. Indian Soc. Periodontol. 2012, 16, 549–552. [Google Scholar] [CrossRef]
- Ban, A.; Inaba, M.; Furumitsu, Y.; Okamoto, K.; Yukioka, K.; Goto, H.; Nishizawa, Y. Time-course of health status in patients with rheumatoid arthritis during the first year of treatment with infliximab. Biomed. Pharmacother. 2010, 64, 107–112. [Google Scholar] [CrossRef]
- Kawashiri, S.-Y.; Kawakami, A.; Ueki, Y.; Imazato, T.; Iwamoto, N.; Fujikawa, K.; Aramaki, T.; Tamai, M.; Nakamura, H.; Origuchi, T.; et al. Decrement of serum cartilage oligomeric matrix protein (COMP) in rheumatoid arthritis (RA) patients achieving remission after 6 months of etanercept treatment: Comparison with CRP., IgM-RF., MMP-3 and anti-CCP Ab. Jt. Bone Spine 2010, 77, 418–420. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Arvikar, S.L.; Collier, D.S.; Fisher, M.C.; Unizony, S.; Cohen, G.L.; McHugh, G.; Kawai, T.; Strle, K.; Steere, A.C. Clinical correlations with Porphyromonas gingivalis antibody responses in patients with early rheumatoid arthritis. Arthritis Res. Ther. 2013, 15, R109. [Google Scholar] [CrossRef]
- Kaur, S.; Bright, R.; Proudman, S.M.; Bartold, P.M. Does periodontal treatment influence clinical and biochemical measures for rheumatoid arthritis? A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Bobbio-Pallavicini, F.; Alpini, C.; Caporali, R.; Avalle, S.; Bugatti, S.; Montecucco, C. Autoantibody profile in rheumatoid arthritis during long-term infliximab treatment. Arthritis Res. Ther. 2004, 6, R264–R272. [Google Scholar] [CrossRef] [PubMed]
- Lequerré, T.; Jouen, F.; Brazier, M.; Clayssens, S.; Klemmer, N.; Ménard, J.-F.; Mejjad, O.; Daragon, A.; Tron, F.; Le Loët, X.; et al. Autoantibodies, metalloproteinases and bone markers in rheumatoid arthritis patients are unable to predict their responses to infliximab. Rheumatology 2007, 46, 446–453. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 6 Months | p Values | |
|---|---|---|---|
| Sex (female/male) | 63/16 | ||
| Age, years | 52.8 (43.3–59.4) | ||
| Disease duration (years) | 9 (5–13) | ||
| No destruction, n (%) | 12 (15.2%) | ||
| Wrist destruction, n (%) | 56 (70.9%) | ||
| Periodontal disease, n (%) | 51 (64.6%) | ||
| DAS28 | 5.1 (4.1–5.7) | 3.5 (2.7–4.3) | <0.0001 |
| ESR (mm/h) | 34 (20–49) | 18 (10–32) | <0.0001 |
| CRP (mg/L) | 18 (7–33) | 7 (2–17) | <0.05 |
| Anti–CCP2 (U/mL) | 97 (9–275) | 43 (5–189) | <0.001 |
| RF IgM (IU/mL) | 38 (11–96) | 22 (6–66) | <0.0001 |
| RF IgA (IU/mL) | 25 (10–61) | 17 (8–47) | 0.0001 |
| MMP–3 (ng/mL) | 90 (40–177) | 45 (24–91) | <0.0001 |
| Anti–P. gingivalis whole extract (AU) | 238 (148–377) | 274 (173–557) | <0.01 |
| Anti–P. gingivalis LPS (AU) | 86 (67–146) | 97 (77–152) | NS |
| Anti–P. intermedia whole extract (AU) | 390 (131–1558) | 436 (246–853) | <0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinaudo-Gaujous, M.; Blasco-Baque, V.; Miossec, P.; Gaudin, P.; Farge, P.; Roblin, X.; Thomas, T.; Paul, S.; Marotte, H. Infliximab Induced a Dissociated Response of Severe Periodontal Biomarkers in Rheumatoid Arthritis Patients. J. Clin. Med. 2019, 8, 751. https://doi.org/10.3390/jcm8050751
Rinaudo-Gaujous M, Blasco-Baque V, Miossec P, Gaudin P, Farge P, Roblin X, Thomas T, Paul S, Marotte H. Infliximab Induced a Dissociated Response of Severe Periodontal Biomarkers in Rheumatoid Arthritis Patients. Journal of Clinical Medicine. 2019; 8(5):751. https://doi.org/10.3390/jcm8050751
Chicago/Turabian StyleRinaudo-Gaujous, Mélanie, Vincent Blasco-Baque, Pierre Miossec, Philippe Gaudin, Pierre Farge, Xavier Roblin, Thierry Thomas, Stephane Paul, and Hubert Marotte. 2019. "Infliximab Induced a Dissociated Response of Severe Periodontal Biomarkers in Rheumatoid Arthritis Patients" Journal of Clinical Medicine 8, no. 5: 751. https://doi.org/10.3390/jcm8050751
APA StyleRinaudo-Gaujous, M., Blasco-Baque, V., Miossec, P., Gaudin, P., Farge, P., Roblin, X., Thomas, T., Paul, S., & Marotte, H. (2019). Infliximab Induced a Dissociated Response of Severe Periodontal Biomarkers in Rheumatoid Arthritis Patients. Journal of Clinical Medicine, 8(5), 751. https://doi.org/10.3390/jcm8050751