Factors Associated with Successful Response to Balloon Decompressive Adhesiolysis Neuroplasty in Patients with Chronic Lumbar Foraminal Stenosis

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
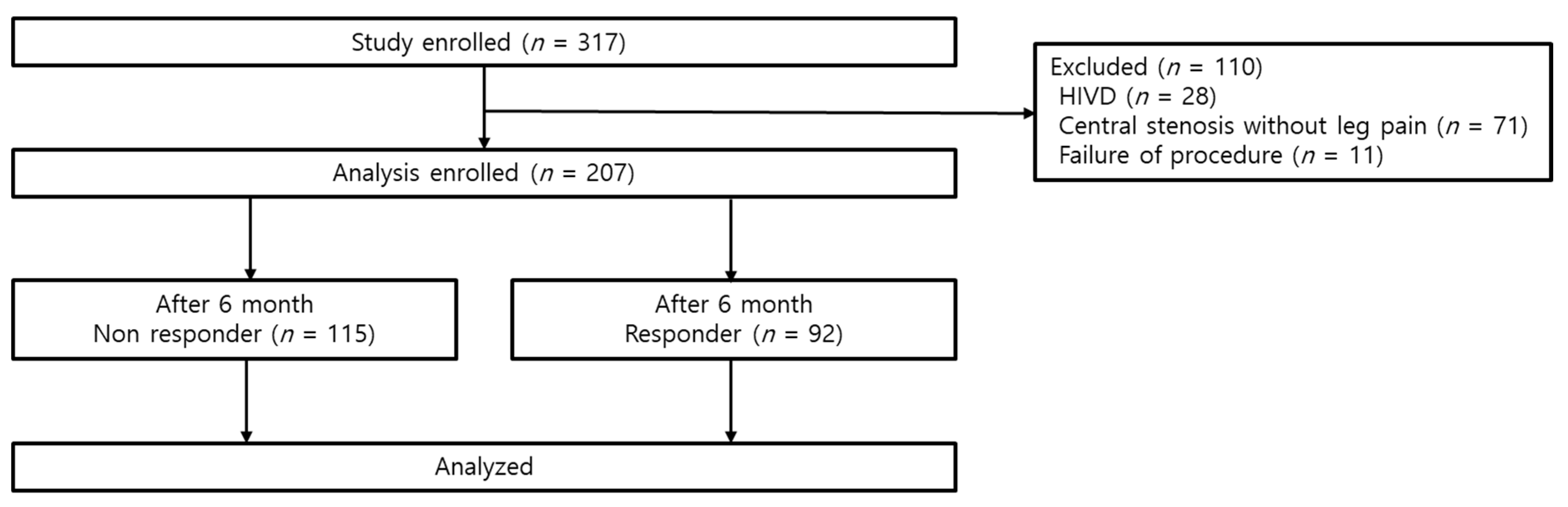
2.1. Participants
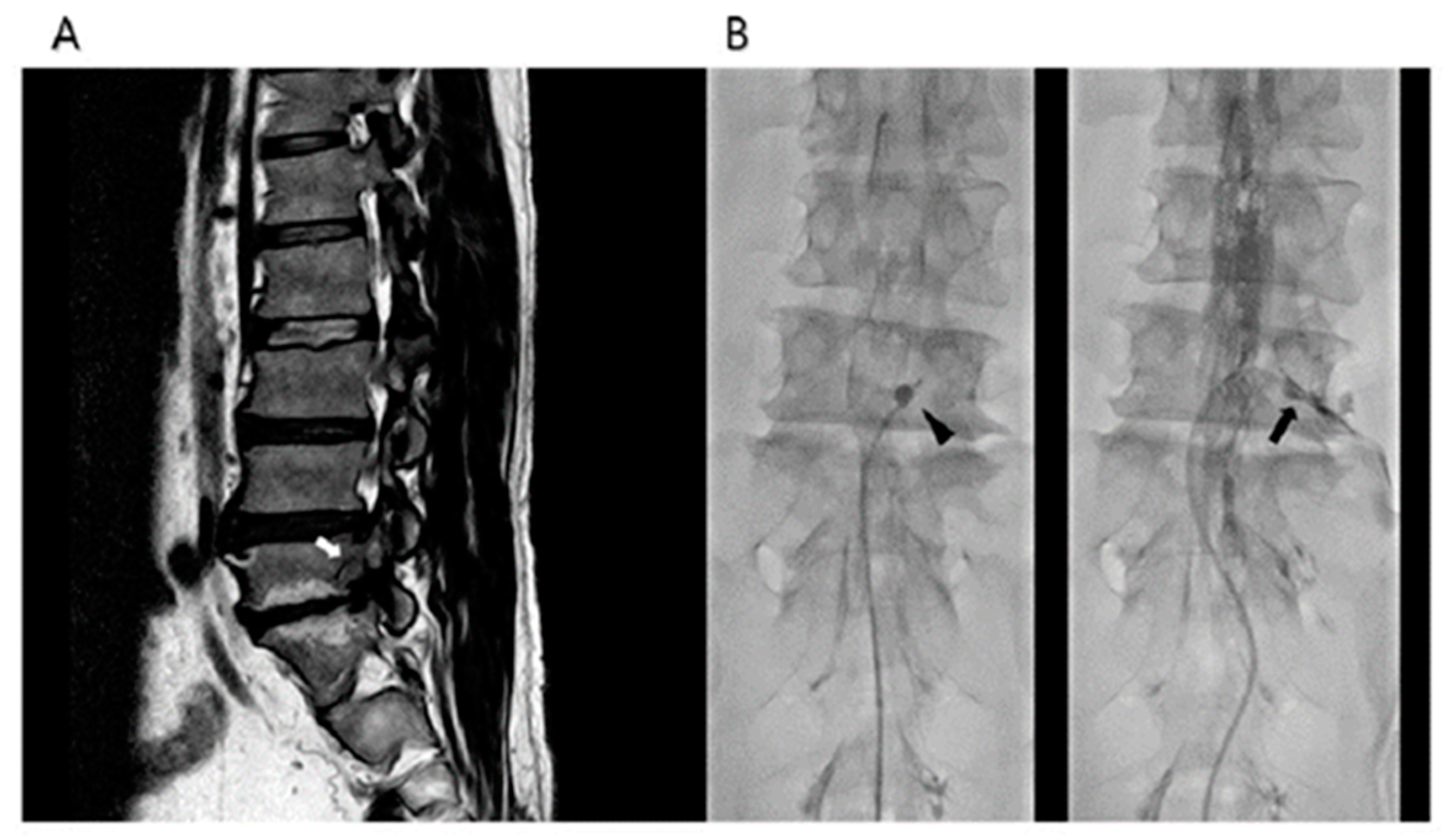
2.2. Procedure: Percutaneous Epidural Neuroplasty Using an Inflatable Balloon Catheter
2.3. Outcome Assessments
2.4. Definition of Successful Responses
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cuckler, J.M.; Bernini, P.A.; Wiesel, S.W.; Booth, R.E., Jr.; Rothman, R.H.; Pickens, G.T. The use of epidural steroids in the treatment of lumbar radicular pain. A prospective, randomized, double-blind study. J. Bone Joint Surg. Am. 1985, 67, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Fukusaki, M.; Kobayashi, I.; Hara, T.; Sumikawa, K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin. J. Pain 1998, 14, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, S.H. Clinical effectiveness of percutaneous adhesiolysis and predictive factors of treatment efficacy in patients with lumbosacral spinal stenosis. Pain Med. 2013, 14, 1497–1504. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Racz, G.B.; Heavner, J.E.; Trescot, A. Percutaneous lysis of epidural adhesions--evidence for safety and efficacy. Pain Pract. 2008, 8, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Rim, B.C.; Lim, J.W.; Park, N.K.; Kang, T.W.; Sohn, M.K.; Beom, J.; Kang, S. Efficacy of epidural neuroplasty versus transforaminal epidural steroid injection for the radiating pain caused by a herniated lumbar disc. Ann. Rehabil. Med. 2013, 37, 824–831. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Helm, S.; Knezevic, N.N. A review of the role of epidural percutaneous neuroplasty. Pain Manag. 2019, 9, 53–62. [Google Scholar] [CrossRef]
- Lee, F.; Jamison, D.E.; Hurley, R.W.; Cohen, S.P. Epidural lysis of adhesions. Korean J. Pain 2014, 27, 3–15. [Google Scholar] [CrossRef]
- Karm, M.H.; Yoon, S.H.; Seo, D.K.; Lee, S.; Lee, Y.; Cho, S.S.; Choi, S.S. Combined epidural adhesiolysis and balloon decompression can be effective in intractable lumbar spinal stenosis patients unresponsive to previous epidural adhesiolysis. Medicine 2019. [Google Scholar] [CrossRef]
- Kim, D.H.; Cho, S.S.; Moon, Y.J.; Kwon, K.; Lee, K.; Leem, J.G.; Shin, J.W.; Park, J.H.; Choi, S.S. Factors Associated with Successful Responses to Transforaminal Balloon Adhesiolysis for Chronic Lumbar Foraminal Stenosis: Retrospective Study. Pain Physician 2017, 20, E841–E848. [Google Scholar]
- Choi, S.S.; Lee, J.H.; Kim, D.; Kim, H.K.; Lee, S.; Song, K.J.; Park, J.K.; Shim, J.H. Effectiveness and Factors Associated with Epidural Decompression and Adhesiolysis Using a Balloon-Inflatable Catheter in Chronic Lumbar Spinal Stenosis: 1-Year Follow-Up. Pain Med. 2016, 17, 476–487. [Google Scholar] [CrossRef][Green Version]
- Park, J.Y.; Ji, G.Y.; Lee, S.W.; Park, J.K.; Ha, D.; Park, Y.; Cho, S.S.; Moon, S.H.; Shin, J.W.; Kim, D.J.; et al. Relationship of Success Rate for Balloon Adhesiolysis with Clinical Outcomes in Chronic Intractable Lumbar Radicular Pain: A Multicenter Prospective Study. J. Clin. Med. 2019, 8, 606. [Google Scholar] [CrossRef]
- Lee, S.; Lee, J.W.; Yeom, J.S.; Kim, K.J.; Kim, H.J.; Chung, S.K.; Kang, H.S. A practical MRI grading system for lumbar foraminal stenosis. AJR Am. J. Roentgenol. 2010, 194, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Choi, W.J.; Suh, J.H.; Jeon, S.R.; Hwang, C.J.; Koh, W.U.; Lee, C.; Leem, J.G.; Lee, S.C.; Shin, J.W. Effects of transforaminal balloon treatment in patients with lumbar foraminal stenosis: A randomized, controlled, double-blind trial. Pain Physician 2013, 16, 213–224. [Google Scholar] [PubMed]
- Gallizzi, M.; Gagnon, C.; Harden, R.N.; Stanos, S.; Khan, A. Medication Quantification Scale Version III: Internal validation of detriment weights using a chronic pain population. Pain Pract. 2008, 8, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Norman, G. Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. Theory Pract. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- Karm, M.H.; Choi, S.S.; Kim, D.H.; Park, J.Y.; Lee, S.; Park, J.K.; Suh, Y.J.; Leem, J.G.; Shin, J.W. Percutaneous Epidural Adhesiolysis Using Inflatable Balloon Catheter and Balloon-less Catheter in Central Lumbar Spinal Stenosis with Neurogenic Claudication: A Randomized Controlled Trial. Pain Physician 2018, 21, 593–606. [Google Scholar]
- Choi, E.; Nahm, F.S.; Lee, P.B. Evaluation of prognostic predictors of percutaneous adhesiolysis using a Racz catheter for post lumbar surgery syndrome or spinal stenosis. Pain Physician 2013, 16, E531–E536. [Google Scholar]
- Smith, A.R.; Rule, S.; Price, P.C. Sample size bias in retrospective estimates of average duration. Acta Psychol. 2017, 176, 39–46. [Google Scholar] [CrossRef]
- Splettstosser, A.; Khan, M.F.; Zimmermann, B.; Vogl, T.J.; Ackermann, H.; Middendorp, M.; Maataoui, A. Correlation of lumbar lateral recess stenosis in magnetic resonance imaging and clinical symptoms. World J. Radiol. 2017, 9, 223–229. [Google Scholar] [CrossRef]
- Tsubosaka, M.; Kaneyama, S.; Yano, T.; Kasahara, K.; Kanemura, A.; Takabatake, M.; Hirata, H.; Sumi, M. The factors of deterioration in long-term clinical course of lumbar spinal canal stenosis after successful conservative treatment. J. Orthop. Surg. Res. 2018. [Google Scholar] [CrossRef]
- Pratt, R.K.; Fairbank, J.C.; Virr, A. The reliability of the Shuttle Walking Test, the Swiss Spinal Stenosis Questionnaire, the Oxford Spinal Stenosis Score, and the Oswestry Disability Index in the assessment of patients with lumbar spinal stenosis. Spine 2002, 27, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.B.; Mathieson, S.; Eyles, J.; Maher, C.G.; Van Gelder, J.M.; Tomkins-Lane, C.C.; Ammendolia, C.; Bella, V.; Ferreira, M.L. Measurement properties of walking outcome measures for neurogenic claudication: A systematic review and meta analysis. Spine J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Vagaska, E.; Litavcova, A.; Srotova, I.; Vlckova, E.; Kerkovsky, M.; Jarkovsky, J.; Bednarik, J.; Adamova, B. Do lumbar magnetic resonance imaging changes predict neuropathic pain in patients with chronic non-specific low back pain? Medicine 2019. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Responder (n = 115) | Responder (n = 92) | p Value | |
|---|---|---|---|
| Age (years) | 64.1 ± 12.5 | 60.9 ± 13.1 | 0.077 |
| Sex (male/female) | 64/51 (55.6/44.3) | 48/44 (52.1/47.9) | 0.618 |
| Height (cm) | 161.3 ± 17.8 | 161.2 ± 19.3 | 0.943 |
| Weight (kg) | 65.3 ± 12.1 | 65.1 ± 9.3 | 0.887 |
| Body mass index (kg/m2) | 24.1 ± 4.3 | 24.2 ± 3.7 | 0.843 |
| Pain duration (months) | 12.0 (6.0–24.0) | 12.0 (8.5–24.0) | 0.468 |
| Foraminal stenosis grade, n (%) | 0.005 | ||
| Mild | 36 (31.3) | 49 (53.3) | |
| Moderate | 44 (38.3) | 27 (29.3) | |
| Severe | 35 (30.4) | 16 (24.6) | |
| Baseline pain intensity (NRS) | |||
| Back | 5.7 ± 2.3 | 6.1 ± 1.9 | 0.149 |
| Leg | 6.7 ± 1.8 | 6.5 ± 1.8 | 0.426 |
| Oswestry Disability Index | 31.8 ± 11.4 | 29.1 ± 9.9 | 0.081 |
| Medication quantification scale | 5.9 ± 5.9 | 7.0 ± 6.0 | 0.402 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age | 0.981 | 0.960–1.002 | 0.078 | 0.994 | 0.970–1.019 | 0.642 |
| Sex | ||||||
| Male | 1 (Ref) | |||||
| Female | 1.150 | 0.664–1.994 | 0.618 | |||
| BMI | 1.007 | 0.940–1.079 | 0.842 | |||
| Pain Duration | 1.003 | 0.995–1.011 | 0.492 | |||
| Foraminal Stenosis Grade | ||||||
| Severe | 1 (Ref) | 1 (Ref) | ||||
| Moderate | 1.342 | 0.627–2.874 | 0.448 | 1.289 | 0.592–2.808 | 0.523 |
| Mild | 2.977 | 1.433–6.187 | 0.003 | 2.829 | 1.351–5.923 | 0.006 |
| Pain Intensity (NRS) | ||||||
| Back | 1.100 | 0.966–1.251 | 0.149 | |||
| Leg | 0.939 | 0.806–1.095 | 0.424 | |||
| Oswestry Disability Index | 0.976 | 0.950–1.003 | 0.083 | 0.980 | 0.952–1.009 | 0.181 |
| MQS | 1.033 | 0.958–1.114 | 0.398 | |||
| Complication | Number (%) |
|---|---|
| Suspected Dura Puncture | 8 (3.9) |
| Subdural Injection | 4 (1.9) |
| Vascular Injection | 3 (1.4) |
| Disc Injection | 4 (1.9) |
| Hypotension | 4 (1.9) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, Y.; Kim, D.-H.; Park, J.-Y.; Ji, G.Y.; Shin, D.A.; Lee, S.W.; Park, J.K.; Shin, J.-W.; Choi, S.-S. Factors Associated with Successful Response to Balloon Decompressive Adhesiolysis Neuroplasty in Patients with Chronic Lumbar Foraminal Stenosis. J. Clin. Med. 2019, 8, 1766. https://doi.org/10.3390/jcm8111766
Oh Y, Kim D-H, Park J-Y, Ji GY, Shin DA, Lee SW, Park JK, Shin J-W, Choi S-S. Factors Associated with Successful Response to Balloon Decompressive Adhesiolysis Neuroplasty in Patients with Chronic Lumbar Foraminal Stenosis. Journal of Clinical Medicine. 2019; 8(11):1766. https://doi.org/10.3390/jcm8111766
Chicago/Turabian StyleOh, Yul, Doo-Hwan Kim, Jun-Young Park, Gyu Yeul Ji, Dong Ah Shin, Sang Won Lee, Jin Kyu Park, Jin-Woo Shin, and Seong-Soo Choi. 2019. "Factors Associated with Successful Response to Balloon Decompressive Adhesiolysis Neuroplasty in Patients with Chronic Lumbar Foraminal Stenosis" Journal of Clinical Medicine 8, no. 11: 1766. https://doi.org/10.3390/jcm8111766
APA StyleOh, Y., Kim, D.-H., Park, J.-Y., Ji, G. Y., Shin, D. A., Lee, S. W., Park, J. K., Shin, J.-W., & Choi, S.-S. (2019). Factors Associated with Successful Response to Balloon Decompressive Adhesiolysis Neuroplasty in Patients with Chronic Lumbar Foraminal Stenosis. Journal of Clinical Medicine, 8(11), 1766. https://doi.org/10.3390/jcm8111766