Less Is More: Ulnar Lengthening Alone without Radial Corrective Osteotomy in Forearm Deformity Secondary to Hereditary Multiple Exostoses

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Sandell, L.J. Multiple hereditary exostosis, EXT genes, and skeletal development. J. Bone Jt. Surg. Am. 2009, 91, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Chhina, H.; Davis, J.C.; Alvarez, C.M. Health-related quality of life in people with hereditary multiple exostoses. J. Pediatr. Orthop. 2012, 32, 210–214. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Ragone, V.; Caldarini, C.; Serra, N.; Usuelli, F.G.; Facchini, R.M. The impact of hereditary multiple exostoses on quality of life, satisfaction, global health status, and pain. Arch. Orthop. Trauma Surg. 2017, 137, 209–215. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Caldarini, C.; Ragone, V.; Facchini, R.M. Effect of multiple hereditary exostoses on sports activity in children. J. Orthop. 2018, 15, 927–930. [Google Scholar] [CrossRef]
- Schmale, G.A.; Conrad, E.U., 3rd; Raskind, W.H. The natural history of hereditary multiple exostoses. J. Bone Jt. Surg. Am. 1994, 76, 986–992. [Google Scholar] [CrossRef]
- Solomon, L. Bone growth in diaphysial aclasis. J. Bone Jt. Surg. Br. 1961, 43-B, 700–716. [Google Scholar] [CrossRef]
- Shin, E.K.; Jones, N.F.; Lawrence, J.F. Treatment of multiple hereditary osteochondromas of the forearm in children: A study of surgical procedures. J. Bone Jt. Surg. Br. 2006, 88, 255–260. [Google Scholar] [CrossRef]
- Rodgers, W.B.; Hall, J.E. One-bone forearm as a salvage procedure for recalcitrant forearm deformity in hereditary multiple exostoses. J. Pediatr. Orthop. 1993, 13, 587–591. [Google Scholar] [CrossRef]
- Kelly, J.P.; James, M.A. Radiographic Outcomes of Hemiepiphyseal Stapling for Distal Radius Deformity Due to Multiple Hereditary Exostoses. J. Pediatr. Orthop. 2016, 36, 42–47. [Google Scholar] [CrossRef]
- El-Sobky, T.A.; Samir, S.; Atiyya, A.N.; Mahmoud, S.; Aly, A.S.; Soliman, R. Current paediatric orthopaedic practice in hereditary multiple osteochondromas of the forearm: A systematic review. SICOT J. 2018, 4, 10. [Google Scholar] [CrossRef]
- Masada, K.; Tsuyuguchi, Y.; Kawai, H.; Kawabata, H.; Noguchi, K.; Ono, K. Operations for forearm deformity caused by multiple osteochondromas. J. Bone Jt. Surg. Br. 1989, 71, 24–29. [Google Scholar] [CrossRef]
- Nimityongskul, P.; Anderson, L.D.; Sri, P. Plastic deformation of the forearm: A review and case reports. J. Trauma 1991, 31, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Tarmuzi, N.A.; Abdullah, S.; Osman, Z.; Das, S. Paediatric forearm fractures: Functional outcome of conservative treatment. Bratisl. Lek. Listy 2009, 110, 563–568. [Google Scholar] [PubMed]
- Fogel, G.R.; McElfresh, E.C.; Peterson, H.A.; Wicklund, P.T. Management of deformities of the forearm in multiple hereditary osteochondromas. J. Bone Jt. Surg. Am. 1984, 66, 670–680. [Google Scholar] [CrossRef]
- Tang, Z.W.; Cao, Y.L.; Liu, T.; Chen, T.; Zhang, X.S. Management of forearm deformities with ulnar shortening more than 15 mm caused by hereditary multiple osteochondromas. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Vogt, B.; Tretow, H.L.; Daniilidis, K.; Wacker, S.; Buller, T.C.; Henrichs, M.P.; Roedl, R.W.; Schiedel, F. Reconstruction of forearm deformity by distraction osteogenesis in children with relative shortening of the ulna due to multiple cartilaginous exostosis. J. Pediatr. Orthop. 2011, 31, 393–401. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Barbato, A.; Caldarini, C.; Biancardi, E.; Facchini, R.M. Gradual ulnar lengthening in children with multiple exostoses and radial head dislocation: Results at skeletal maturity. J. Child. Orthop. 2016, 10, 127–133. [Google Scholar] [CrossRef]
- Abe, M.; Shirai, H.; Okamoto, M.; Onomura, T. Lengthening of the forearm by callus distraction. J. Hand Surg. Br. 1996, 21, 151–163. [Google Scholar] [CrossRef]
- Ham, J.; Flipsen, M.; Koolen, M.; van der Zwan, A.; Mader, K. Multiple osteochondromas (MO) in the forearm: A 12-year single-centre experience. Strateg. Trauma Limb Reconstr. 2016, 11, 169–175. [Google Scholar] [CrossRef]
- Pritchett, J.W. Lengthening the ulna in patients with hereditary multiple exostoses. J. Bone Jt. Surg. Br. 1986, 68, 561–565. [Google Scholar] [CrossRef]
- Jo, A.R.; Jung, S.T.; Kim, M.S.; Oh, C.S.; Min, B.J. An Evaluation of Forearm Deformities in Hereditary Multiple Exostoses: Factors Associated with Radial Head Dislocation and Comprehensive Classification. J. Hand Surg. Am. 2017, 42, 292.e1–292.e8. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.P.; Hansen, M.O. Function of the upper extremities in hereditary multiple exostoses. J. Bone Jt. Surg. Am. 1996, 78, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Refsland, S.; Kozin, S.H.; Zlotolow, D.A. Ulnar Distraction Osteogenesis in the Treatment of Forearm Deformities in Children with Multiple Hereditary Exostoses. J. Hand Surg. Am. 2016, 41, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, H.; Tsuchiya, H.; Sakurakichi, K.; Yamashiro, T.; Watanabe, K.; Tomita, K. Correction and lengthening for deformities of the forearm in multiple cartilaginous exostoses. J. Orthop. Sci. 2006, 11, 459–466. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cho, Y.J.; Jung, S.T. Gradual lengthening of the ulna in patients with multiple hereditary exostoses with a dislocated radial head. Yonsei Med. J. 2014, 55, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Morrey, B.F.; Askew, L.J.; Chao, E.Y. A biomechanical study of normal functional elbow motion. J. Bone Jt. Surg. Am. 1981, 63, 872–877. [Google Scholar] [CrossRef]
- Demir, B.; Gursu, S.; Ozturk, K.; Yildirim, T.; Konya, M.N.; Er, T. Single-stage treatment of complete dislocation of radial head and forearm deformity using distraction osteogenesis in paediatric patients having multiple cartilaginous exostosis. Arch. Orthop. Trauma Surg. 2011, 131, 1195–1201. [Google Scholar] [CrossRef]
- Tonogai, I.; Takahashi, M.; Tsutsui, T.; Goto, T.; Hamada, D.; Suzue, N.; Matsuura, T.; Yasui, N.; Sairyo, K. Forearm lengthening by distraction osteogenesis: A report on 5 limbs in 3 cases. J. Med. Investig. 2015, 62, 219–222. [Google Scholar] [CrossRef][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Senior Group (n = 6) with Radial Correction | The Junior Group (n = 8) without Radial Correction | p Value | |
|---|---|---|---|
| Age (year) | 16.7 ± 4.4 | 8.1 ± 2.5 | <0.01 |
| Gender (Female/Male) | 1/5 | 4/4 | 0.30 |
| Side (Right/Left) | 5/1 | 5/3 | 0.58 |
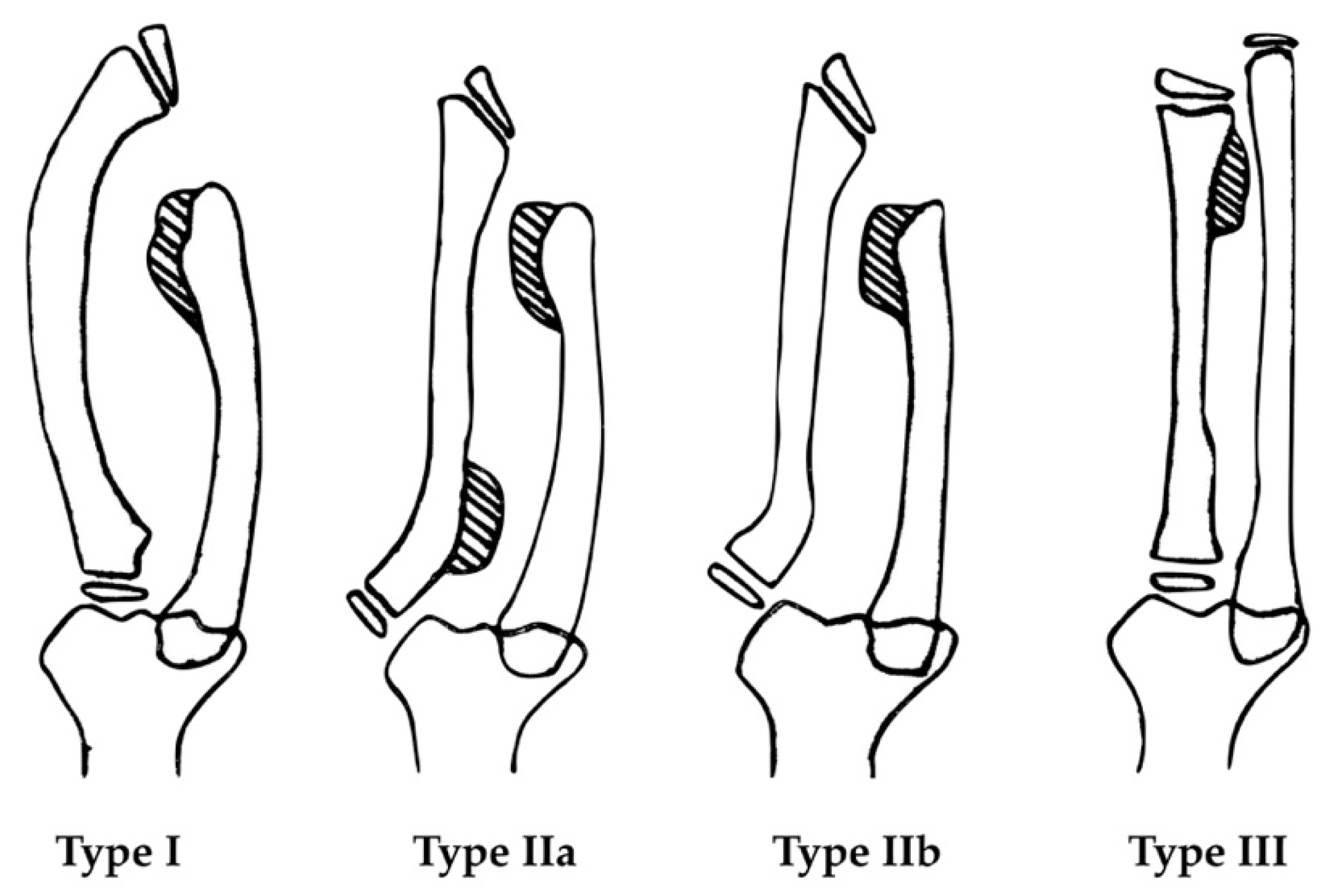
| Masada Classification | |||
| Type I | 4 | 7 | |
| Type IIa | 1 | 0 | |
| Type IIb | 1 | 1 | |
| Elongated length (mm) | 21.3 ± 5.8 | 22.5 ± 2.4 | 0.43 |
| EFT (day) | 204.3 ± 63.7 | 159.0 ± 38.8 | 0.14 |
| EFI (day/cm) | 104.9 ± 53.6 | 72.0 ± 20.0 | 0.20 |
| Follow-up (month) | 38.7 ± 22 | 51.4 ± 18.6 | 0.12 |
| The Senior Group (n = 6) | The Junior Group (n = 8) | p Value | |
|---|---|---|---|
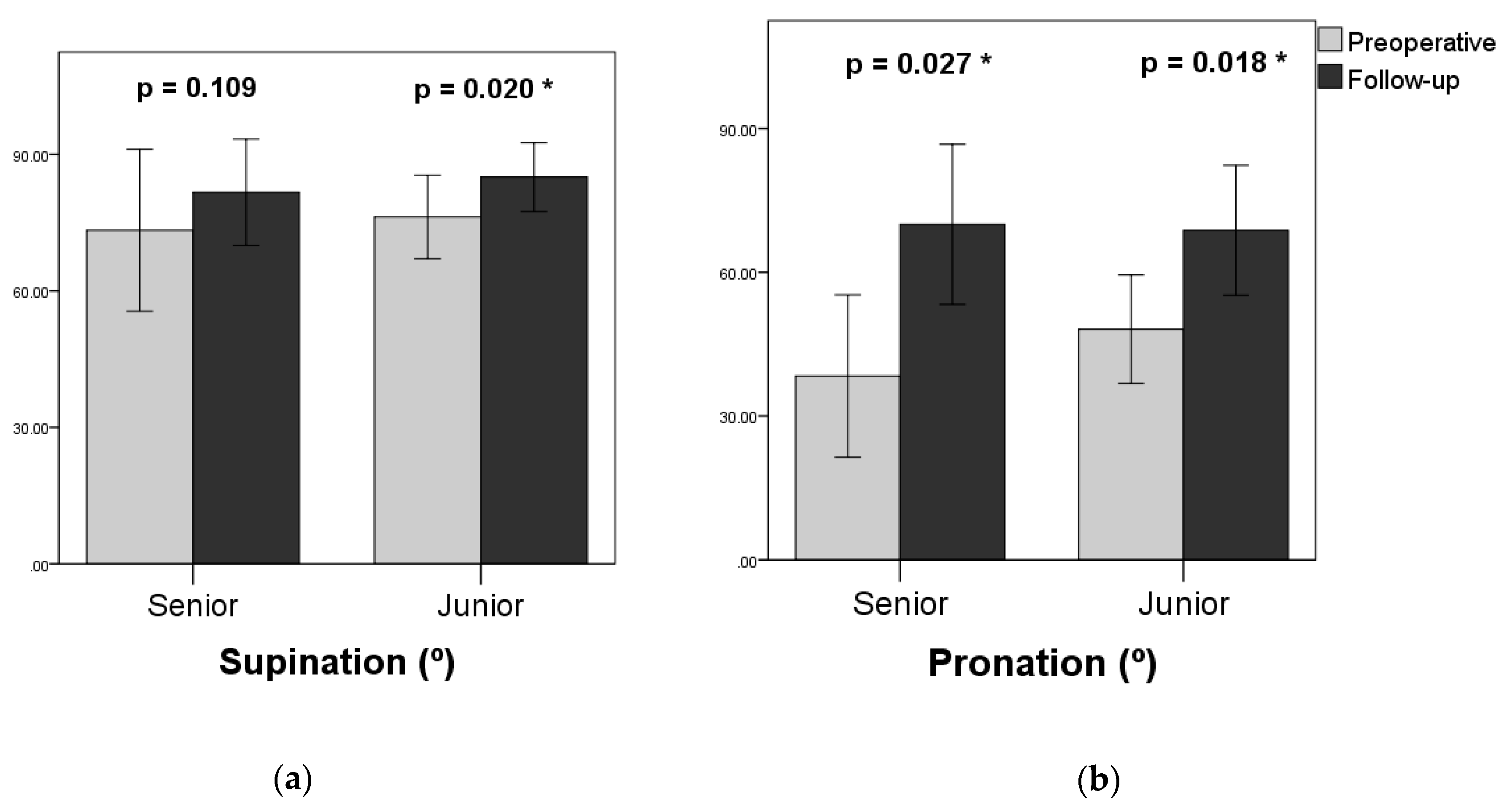
| Supination | |||
| Preoperative | 73.3° ± 16.2° | 76.3° ± 8.6° | 0.95 |
| Follow-up | 81.7° ± 10.7° | 85.0° ± 7.1° | 0.61 |
| Gained | 8.3° ± 11.1° | 8.8° ± 6.0° | 0.59 |
| Pronation | |||
| Preoperative | 38.3° ± 15.5° | 48.1° ± 10.6° | 0.29 |
| Follow-up | 70.0° ± 15.3° | 68.8° ± 12.7° | 0.89 |
| Gained | 31.7° ± 17.5° | 20.6° ± 14.2° | 0.30 |
| The Senior Group (n = 6) | The Junior Group (n = 8) | p Value | |
|---|---|---|---|
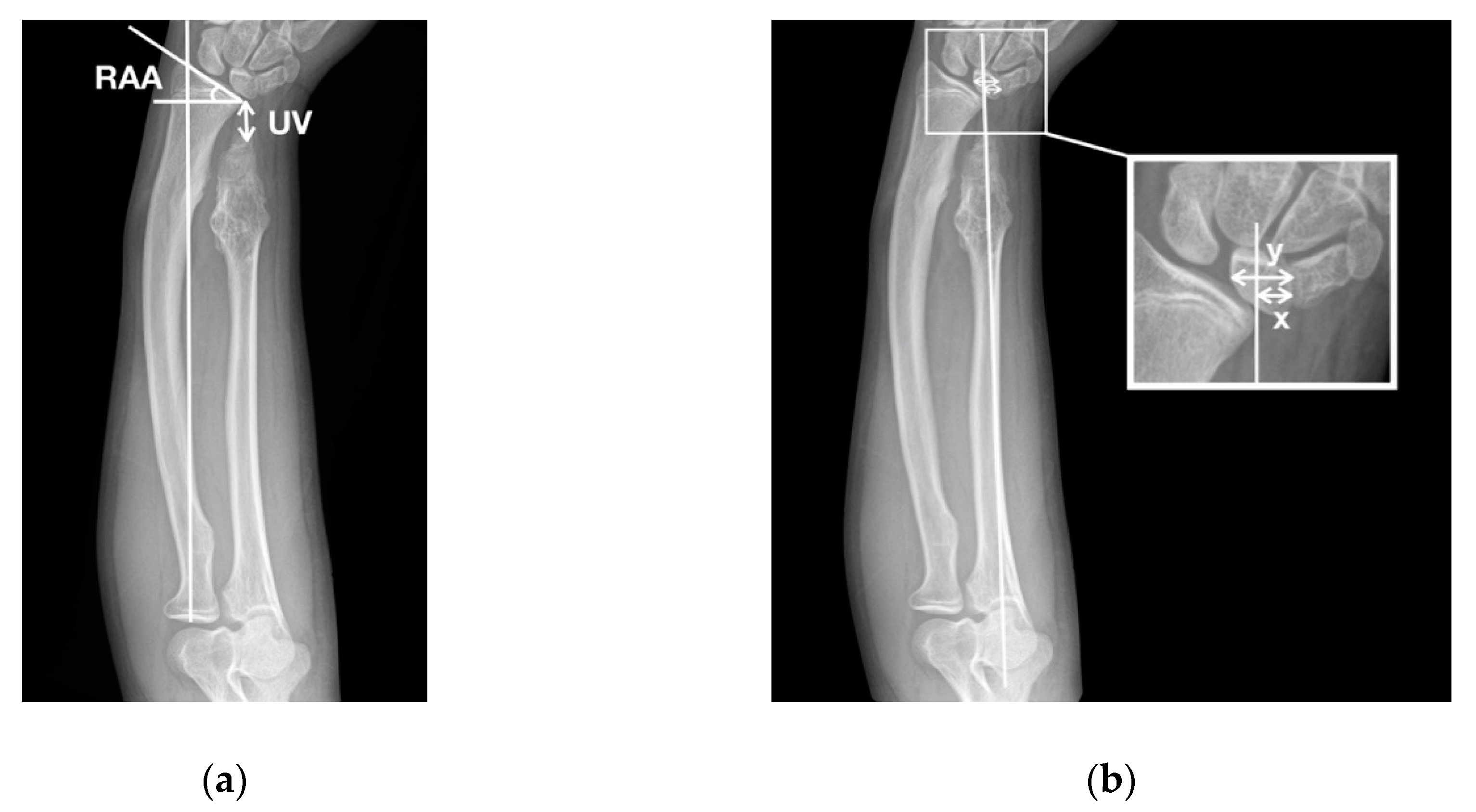
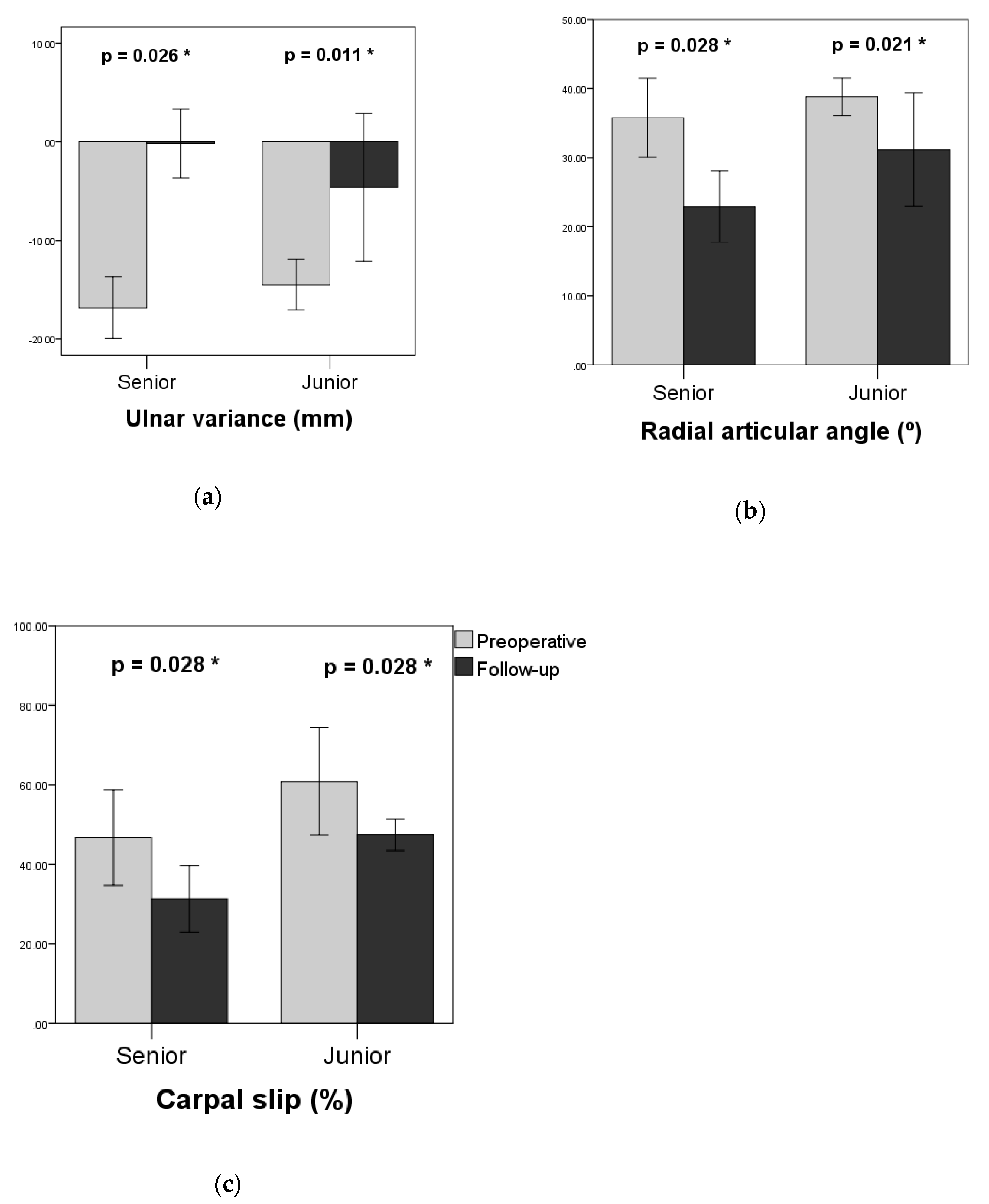
| UV (mm) | |||
| Preoperative | −16.8 ± 2.9 | −14.5 ± 2.4 | 0.11 |
| Follow-up | −0.2 ± 3.2 | −4.6 ± 7.0 | 0.32 |
| RAA (°) | |||
| Preoperative | 35.8 ± 5.2 | 38.8 ± 2.5 | 0.44 |
| Follow-up | 22.9 ± 4.7 | 31.2 ± 7.7 | 0.07 |
| CS (%) | |||
| Preoperative | 46.7 ± 11.0 | 60.8 ± 12.3 | 0.11 |
| Follow-up | 31.3 ± 7.6 | 47.4 ± 3.6 | 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-J.; Wu, K.-W.; Lee, C.-C.; Kuo, K.N.; Chang, J.-F.; Wang, T.-M. Less Is More: Ulnar Lengthening Alone without Radial Corrective Osteotomy in Forearm Deformity Secondary to Hereditary Multiple Exostoses. J. Clin. Med. 2019, 8, 1765. https://doi.org/10.3390/jcm8111765
Hsu P-J, Wu K-W, Lee C-C, Kuo KN, Chang J-F, Wang T-M. Less Is More: Ulnar Lengthening Alone without Radial Corrective Osteotomy in Forearm Deformity Secondary to Hereditary Multiple Exostoses. Journal of Clinical Medicine. 2019; 8(11):1765. https://doi.org/10.3390/jcm8111765
Chicago/Turabian StyleHsu, Po-Jen, Kuan-Wen Wu, Chia-Che Lee, Ken N. Kuo, Jia-Feng Chang, and Ting-Ming Wang. 2019. "Less Is More: Ulnar Lengthening Alone without Radial Corrective Osteotomy in Forearm Deformity Secondary to Hereditary Multiple Exostoses" Journal of Clinical Medicine 8, no. 11: 1765. https://doi.org/10.3390/jcm8111765
APA StyleHsu, P.-J., Wu, K.-W., Lee, C.-C., Kuo, K. N., Chang, J.-F., & Wang, T.-M. (2019). Less Is More: Ulnar Lengthening Alone without Radial Corrective Osteotomy in Forearm Deformity Secondary to Hereditary Multiple Exostoses. Journal of Clinical Medicine, 8(11), 1765. https://doi.org/10.3390/jcm8111765