Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries


 , , , and
, , , and 
Abstract
1. Introduction
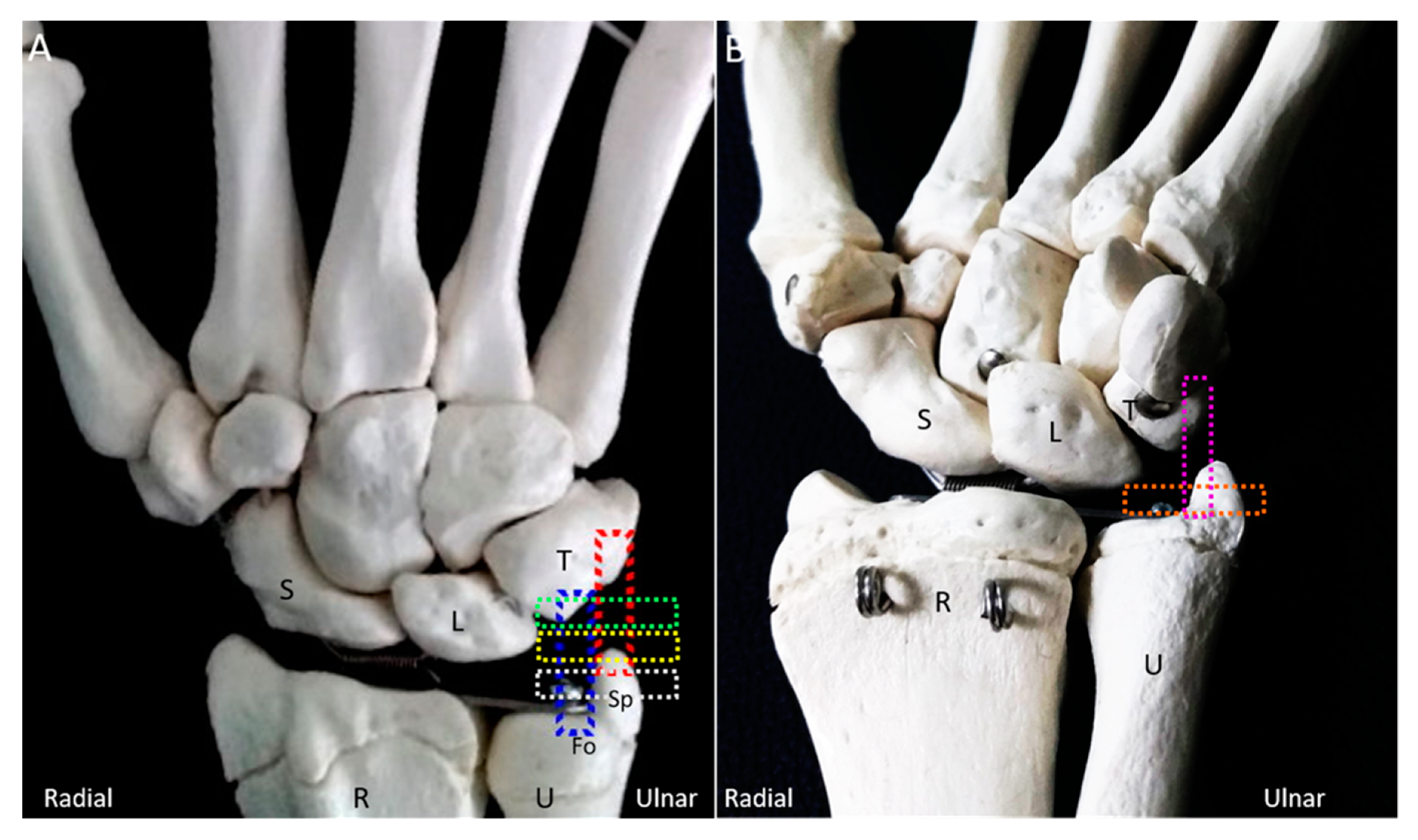
2. Anatomy
3. Mechanism of Injury
4. Physical Examination
5. Imaging (Other than US)
6. US Imaging
6.1. Scanning Protocol
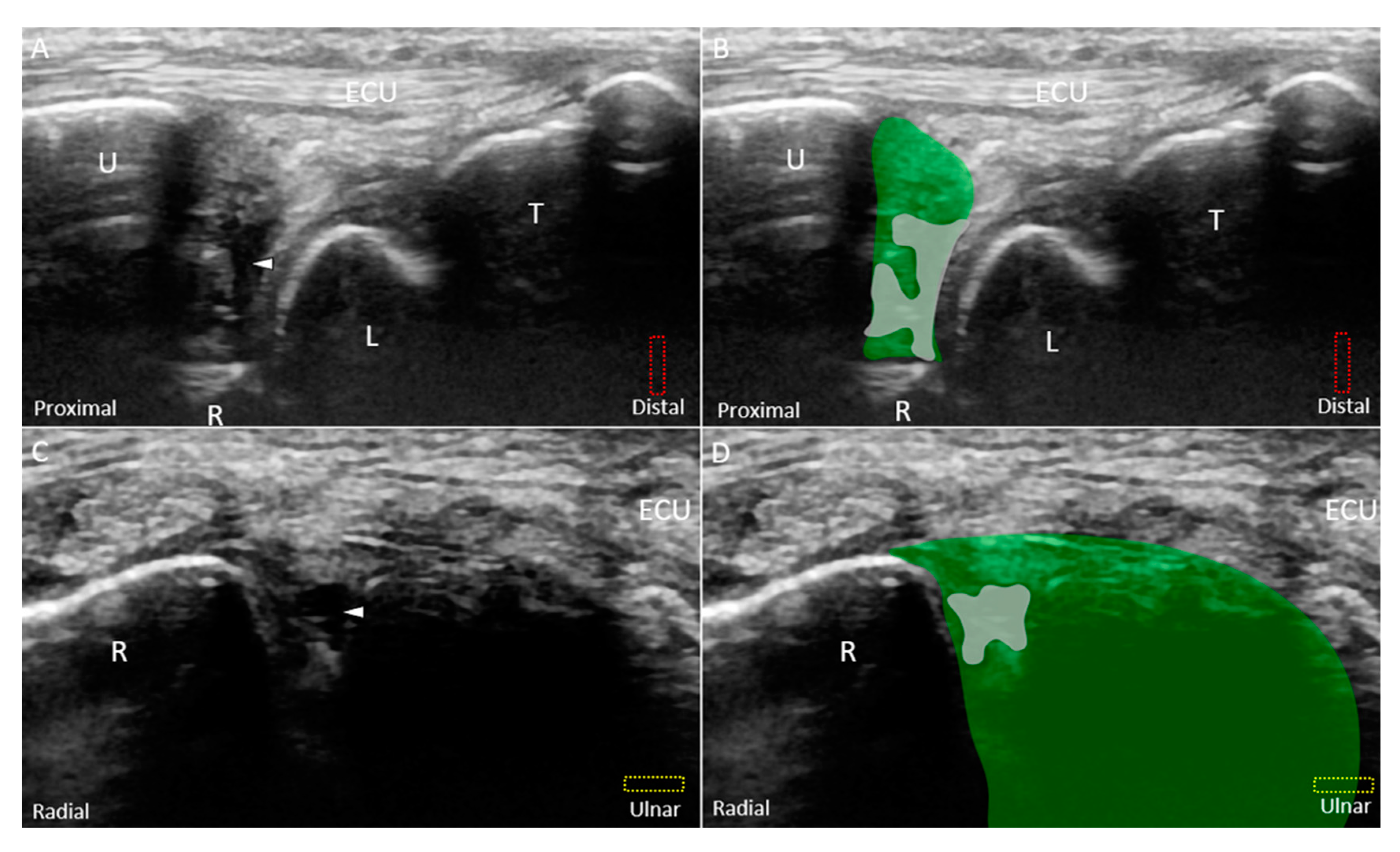
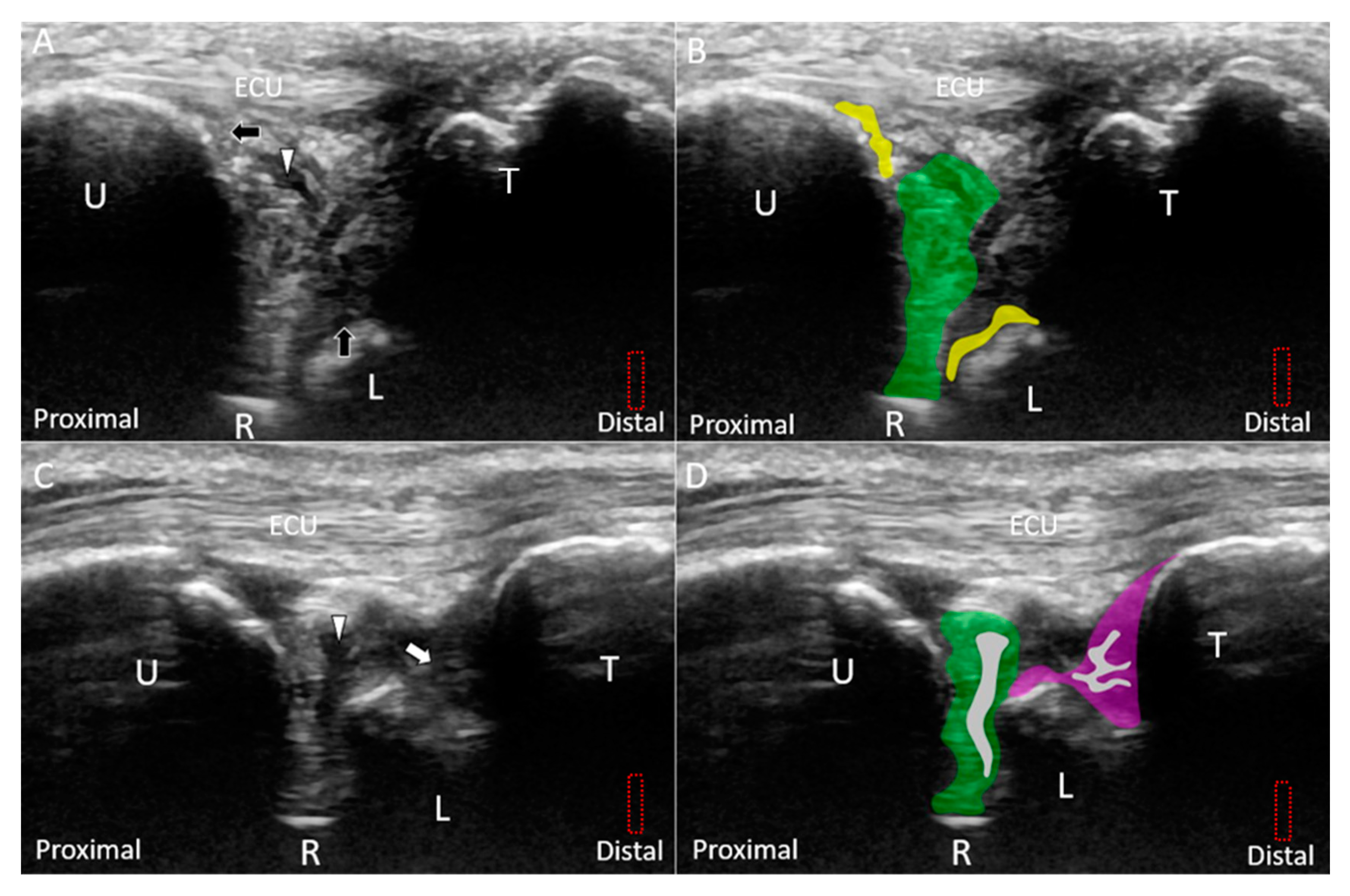
6.1.1. Long-Axis View
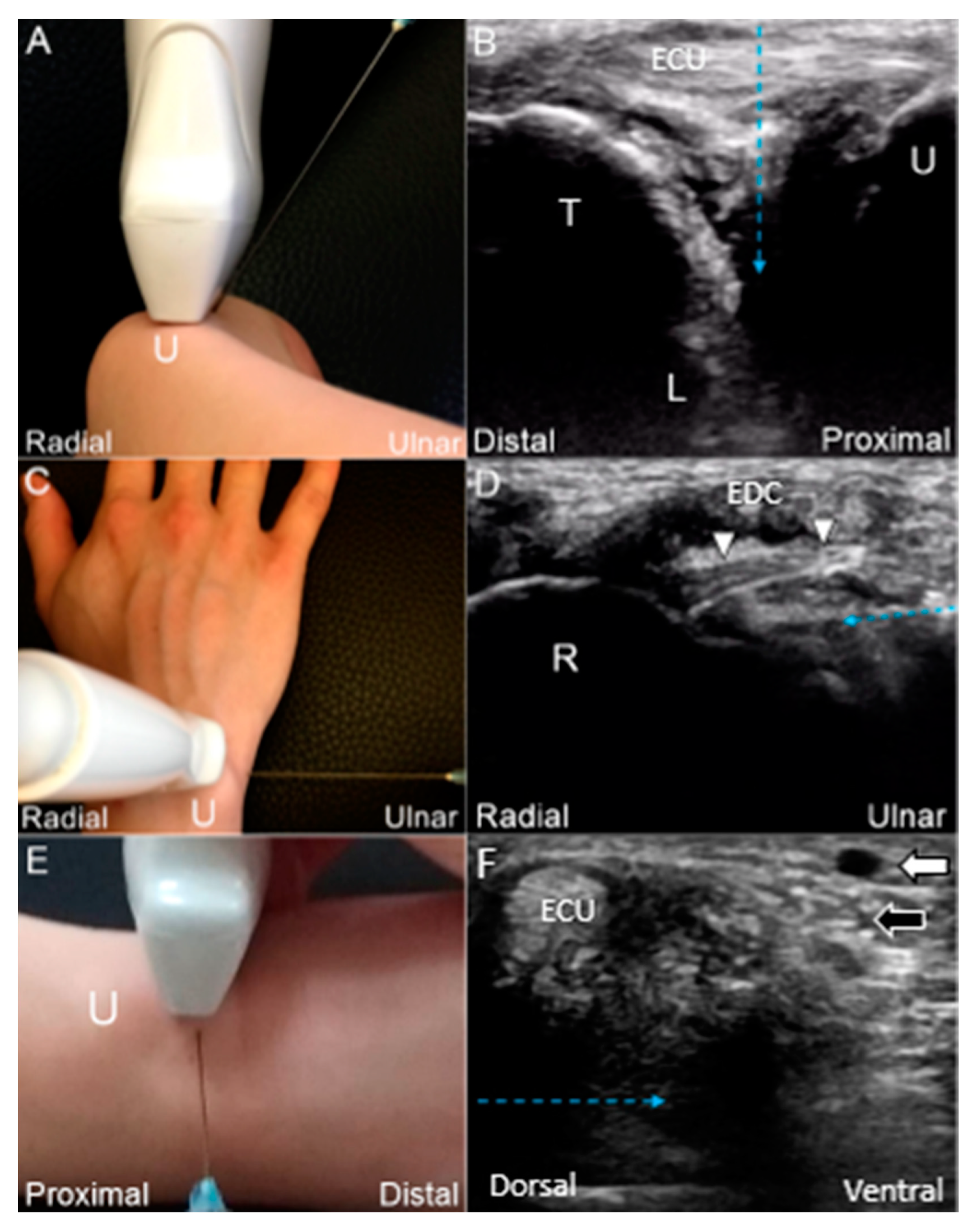
6.1.2. Short-Axis View
7. Pathologies—Classification
8. Treatment
8.1. General Principles
8.2. US-Guided Injection
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Palmer, A.K. Triangular fibrocartilage complex lesions: A classification. J. Hand Surg. 1989, 14, 594–606. [Google Scholar] [CrossRef]
- Pesquer, L.; Scepi, M.; Bihan, M.; Vialle, R.; Richer, J.P.; Roumy, J.; Tasu, J.P. Normal ultrasound anatomy of the triangular fibrocartilage of the wrist: A study on cadavers and on healthy subjects. J. Clin. Ultrasound 2009, 37, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-Y.; Chang, K.-V.; Özçakar, L. Dynamic and Doppler Ultrasound Imaging for the Diagnosis of Triangular Fibrocartilage Complex Injury and Ulnocarpal Wrist Instability. Am. J. Phys. Med. Rehabil. 2016, 95, e111–e112. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, H.; Burns, J.E. Magnetic resonance imaging of triangular fibrocartilage. J. Magn. Reson. Imaging 2012, 35, 764–778. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.J.; Wang, M.T.; Chang, K.V.; Liang, H.W. Ultrasonographic images of the hand in a case with early eosinophilic fasciitis. J. Med. Ultrason. 2018, 45, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-V.; Wu, W.-T.; Han, D.-S.; Özçakar, L. Static and dynamic shoulder imaging to predict initial effectiveness and recurrence after ultrasound-guided subacromial corticosteroid injections. Arch. Phys. Med. Rehabil. 2017, 98, 1984–1994. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.-T.; Chang, K.-V.; Mezian, K.; Naňka, O.; Lin, C.-P.; Özçakar, L. Basis of shoulder nerve entrapment syndrome: An ultrasonographic study exploring factors influencing cross-sectional area of the suprascapular nerve. Front. Neurol. 2018, 9, 902. [Google Scholar] [CrossRef] [PubMed]
- Özçakar, L.; Kara, M.; Chang, K.; Ulaşlı, A.; Hung, C.; Tekin, L.; Wu, C.; Tok, F.; Hsiao, M.; Akkaya, N. EURO-MUSCULUS/USPRM Basic Scanning Protocols for wrist and hand. Eur. J. Phys. Rehabil. Med. 2015, 51, 479–484. [Google Scholar]
- Wu, C.-H.; Chang, K.-V.; Özçakar, L.; Hsiao, M.-Y.; Hung, C.-Y.; Shyu, S.-G.; Wang, T.-G.; Chen, W.-S. Sonographic tracking of the upper limb peripheral nerves: A pictorial essay and video demonstration. Am. J. Phys. Med. Rehabil. 2015, 94, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Milz, S.; Sicking, B.; Sprecher, C.; Putz, R.; Benjamin, M. An immunohistochemical study of the triangular fibrocartilage complex of the wrist: Regional variations in cartilage phenotype. J. Anat. 2007, 211, 1–7. [Google Scholar] [CrossRef]
- Berger, R.A. The anatomy of the ligaments of the wrist and distal radioulnar joints. Clin. Orthop. Relat. Res. 2001, 383, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Haugstvedt, J.-R.; Berger, R.A.; Nakamura, T.; Neale, P.; Berglund, L.; An, K.-N. Relative contributions of the ulnar attachments of the triangular fibrocartilage complex to the dynamic stability of the distal radioulnar joint. J. Hand Surg. 2006, 31, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.-J.; Kim, J.-P.; Yang, H.-M.; Lee, E.-Y.; Go, J.-H.; Heo, K. Topographical anatomy of the distal ulna attachment of the radioulnar ligament. J. Hand Surg. 2017, 42, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.-L.; Li, W.-T.; Bai, R.-J.; Wang, N.-L.; Qian, Z.-H.; Ye, W.; Yin, Y.-M. High-resolution 3T magnetic resonance imaging of the triangular fibrocartilage complex in Chinese wrists: Correlation with cross-sectional anatomy. Chin. Med. J. 2017, 130, 817. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, W.B. Stability of the distal radioulna joint: Biomechanics, pathophysiology, physical diagnosis, and restoration of function what we have learned in 25 years. J. Hand Surg. 2007, 32, 1086–1106. [Google Scholar] [CrossRef] [PubMed]
- Moritomo, H.; Murase, T.; Arimitsu, S.; Oka, K.; Yoshikawa, H.; Sugamoto, K. Change in the length of the ulnocarpal ligaments during radiocarpal motion: Possible impact on triangular fibrocartilage complex foveal tears. J. Hand Surg. 2008, 33, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Taljanovic, M.S.; Goldberg, M.R.; Sheppard, J.E.; Rogers, L.F. US of the intrinsic and extrinsic wrist ligaments and triangular fibrocartilage complex—Normal anatomy and imaging technique. Radiographics 2011, 31, 79–80. [Google Scholar] [CrossRef]
- Watanabe, A.; Souza, F.; Vezeridis, P.S.; Blazar, P.; Yoshioka, H. Ulnar-sided wrist pain. II. Clinical imaging and treatment. Skelet. Radiol. 2010, 39, 837–857. [Google Scholar] [CrossRef]
- Kataoka, T.; Moritomo, H.; Omokawa, S.; Iida, A.; Murase, T.; Sugamoto, K. Ulnar variance: Its relationship to ulnar foveal morphology and forearm kinematics. J. Hand Surg. 2012, 37, 729–735. [Google Scholar] [CrossRef]
- Palmer, A.K.; Werner, F.W.; Glisson, R.R.; Murphy, D.J. Partial excision of the triangular fibrocartilage complex. J. Hand Surg. 1988, 13, 391–394. [Google Scholar] [CrossRef]
- Tay, S.C.; Tomita, K.; Berger, R.A. The “ulnar fovea sign” for defining ulnar wrist pain: An analysis of sensitivity and specificity. J. Hand Surg. 2007, 32, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, R.; Horii, E.; Imaeda, T.; Nakao, E.; Kato, H.; Watanabe, K. The ulnocarpal stress test in the diagnosis of ulnar-sided wrist pain. J. Hand Surg. 1997, 22, 719–723. [Google Scholar] [CrossRef]
- Berger, R.A.; Dobyns, J.H. Physical examination and provocative maneuvers of the wrist. In Imaging of the Hand; Saunders: Philadelphia, PA, USA, 1996. [Google Scholar]
- Moriya, T.; Aoki, M.; Iba, K.; Ozasa, Y.; Wada, T.; Yamashita, T. Effect of triangular ligament tears on distal radioulnar joint instability and evaluation of three clinical tests: A biomechanical study. J. Hand Surg. (Eur. Vol.) 2009, 34, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.C.; Zimmerman, N.B.; Travis, M.T. Wrist arthrography versus arthroscopy: A comparative study of 150 cases. J. Hand Surg. 1996, 21, 591–594. [Google Scholar] [CrossRef]
- Zanetti, M.; Saupe, N.; Nagy, L. Role of MR imaging in chronic wrist pain. Eur. Radiol. 2007, 17, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Bayoumy, M.A.; Elkady, H.A.; Said, H.G.; El-Sayed, A.; Saleh, W.R. Arthroscopic grading of common wrist disorders and its role in management. J. Orthop. 2015, 12, S244–S250. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Taljanovic, M.S.; Sheppard, J.E.; Jones, M.D.; Switlick, D.N.; Hunter, T.B.; Rogers, L.F. Sonography and sonoarthrography of the scapholunate and lunotriquetral ligaments and triangular fibrocartilage disk: Initial experience and correlation with arthrography and magnetic resonance arthrography. J. Ultrasound Med. 2008, 27, 179–191. [Google Scholar] [CrossRef] [PubMed]
- von Borstel, D.; Wang, M.; Small, K.; Nozaki, T.; Yoshioka, H. High-resolution 3T MR imaging of the triangular fibrocartilage complex. Magn. Reson. Med. Sci. 2016. [Google Scholar] [CrossRef]
- Nakamura, T.; Yabe, Y. Histological anatomy of the triangular fibrocartilage complex of the human wrist. Ann. Anat.-Anat. Anz. 2000, 182, 567–572. [Google Scholar] [CrossRef]
- Moritomo, H.; Arimitsu, S. Tenodesis of the Ulnotriquetrum Ligament to the Fovea for a Triangular Fibrocartilage Complex Tear. Tech. Hand Up. Extrem. Surg. 2018, 22, 141–145. [Google Scholar] [CrossRef]
- Palmer, A.K.; Werner, F.W. The triangular fibrocartilage complex of the wrist—Anatomy and function. J. Hand Surg. 1981, 6, 153–162. [Google Scholar] [CrossRef]
- McAdams, T.R.; Swan, J.; Yao, J. Arthroscopic treatment of triangular fibrocartilage wrist injuries in the athlete. Am. J. Sports Med. 2009, 37, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Atzei, A.; Luchetti, R. Foveal TFCC tear classification and treatment. Hand Clin. 2011, 27, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Ishii, S.; Palmer, A.K.; Werner, F.W.; Short, W.H.; Fortino, M.D. An anatomic study of the ligamentous structure of the triangular fibrocartilage complex. J. Hand Surg. 1998, 23, 977–985. [Google Scholar] [CrossRef]
- Zhan, H.; Zhang, H.; Bai, R.; Qian, Z.; Liu, Y.; Zhang, H.; Yin, Y. High-resolution 3-T MRI of the triangular fibrocartilage complex in the wrist: Injury pattern and MR features. Skelet. Radiol. 2017, 46, 1695–1706. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T. Anatomical reattachment of the TFCC to the ulnar fovea using an ECU half-slip. J. Wrist Surg. 2015, 4, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-V.; Mezian, K.; Naňka, O.; Wu, W.-T.; Lou, Y.-M.; Wang, J.-C.; Martinoli, C.; Özçakar, L. Ultrasound imaging for the cutaneous nerves of the extremities and relevant entrapment syndromes: From anatomy to clinical implications. J. Clin. Med. 2018, 7, 457. [Google Scholar] [CrossRef] [PubMed]
- Mikić, Z. The blood supply of the human distal radioulnar joint and the microvasculature of its articular disk. Clin. Orthop. Relat. Res. 1992, 275, 19–28. [Google Scholar] [CrossRef]
- Unglaub, F.; Kroeber, M.W.; Thomas, S.B.; Wolf, M.B.; Arkudas, A.; Dragu, A.; Horch, R.E. Incidence and distribution of blood vessels in punch biopsies of Palmer 1A disc lesions in the wrist. Arch. Orthop. Trauma Surg. 2009, 129, 631–634. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class 1 (Traumatic) |
|---|
| (A). Central tear of the articular disc |
| (B). Ulnar attachment tear of the articular disc |
| (C). Radial attachment tear of the articular disc |
| (D). Horizontal tear of the articular disc |
| (E). Injury of the triangular fibrocartilage component other than the articular disc, i.e., meniscus homologue; radioulnar, lunotriquetral, and ulnar collateral ligaments; or extensor carpi ulnaris tendon subsheath |
| Class 2 (Degenerative) |
| (A). Articular disc wear |
| (B). Class 2A plus chondromalacia of the lunate or the ulna |
| (C). Class 2B plus articular disc rupture |
| (D). Class 2C plus lunotriquetral ligament rupture and cartilage abnormalities |
| (E). Class 2D plus ulnocarpal/radioulnar arthritis |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, W.-T.; Chang, K.-V.; Mezian, K.; Naňka, O.; Yang, Y.-C.; Hsu, Y.-C.; Hsu, P.-C.; Özçakar, L. Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries. J. Clin. Med. 2019, 8, 1540. https://doi.org/10.3390/jcm8101540
Wu W-T, Chang K-V, Mezian K, Naňka O, Yang Y-C, Hsu Y-C, Hsu P-C, Özçakar L. Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries. Journal of Clinical Medicine. 2019; 8(10):1540. https://doi.org/10.3390/jcm8101540
Chicago/Turabian StyleWu, Wei-Ting, Ke-Vin Chang, Kamal Mezian, Ondřej Naňka, Yi-Chiang Yang, Yu-Chun Hsu, Po-Cheng Hsu, and Levent Özçakar. 2019. "Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries" Journal of Clinical Medicine 8, no. 10: 1540. https://doi.org/10.3390/jcm8101540
APA StyleWu, W.-T., Chang, K.-V., Mezian, K., Naňka, O., Yang, Y.-C., Hsu, Y.-C., Hsu, P.-C., & Özçakar, L. (2019). Ulnar Wrist Pain Revisited: Ultrasound Diagnosis and Guided Injection for Triangular Fibrocartilage Complex Injuries. Journal of Clinical Medicine, 8(10), 1540. https://doi.org/10.3390/jcm8101540