Diabetic Foot Infection Presenting Systemic Inflammatory Response Syndrome: A Unique Disorder of Systemic Reaction from Infection of the Most Distal Body


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and DFI Treatments
2.2. DFI and Wound Scoring
2.3. Data Collection
2.4. Prognosis Analysis: LEAs and in-Hospital Mortality
2.5. Statistics
3. Results
3.1. The Characteristics of Patients DFI Presenting SIRS
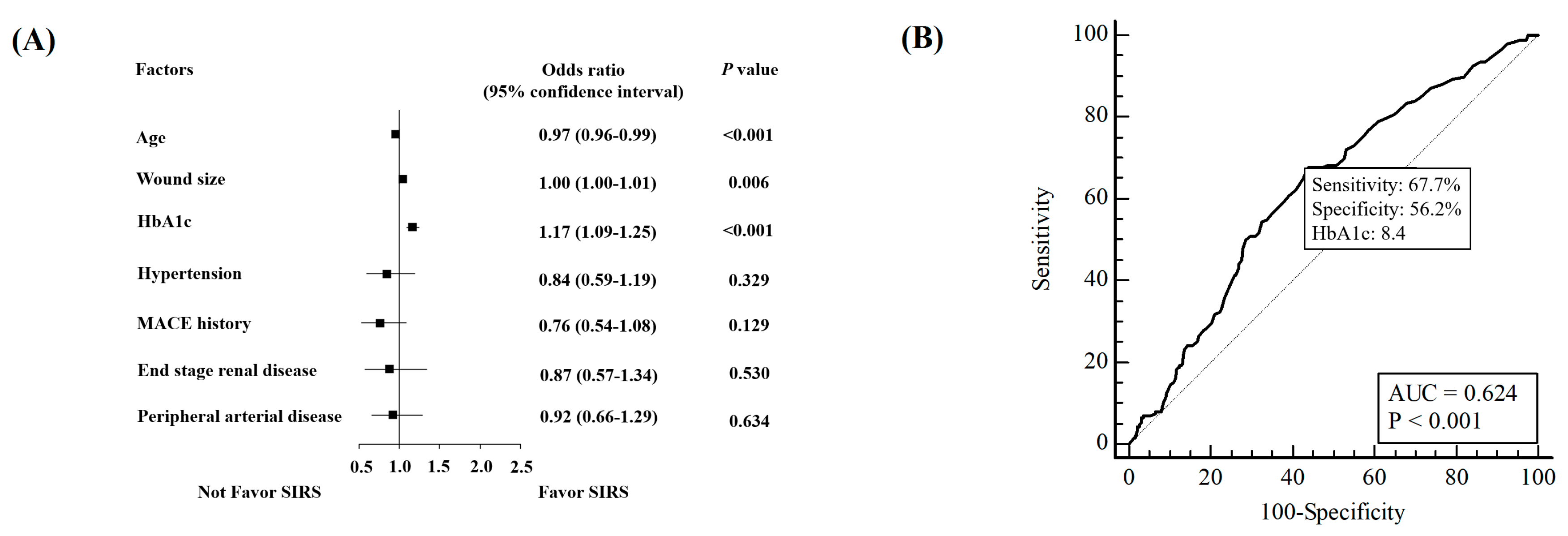
3.2. Factors Prone to Have SIRS Presentation
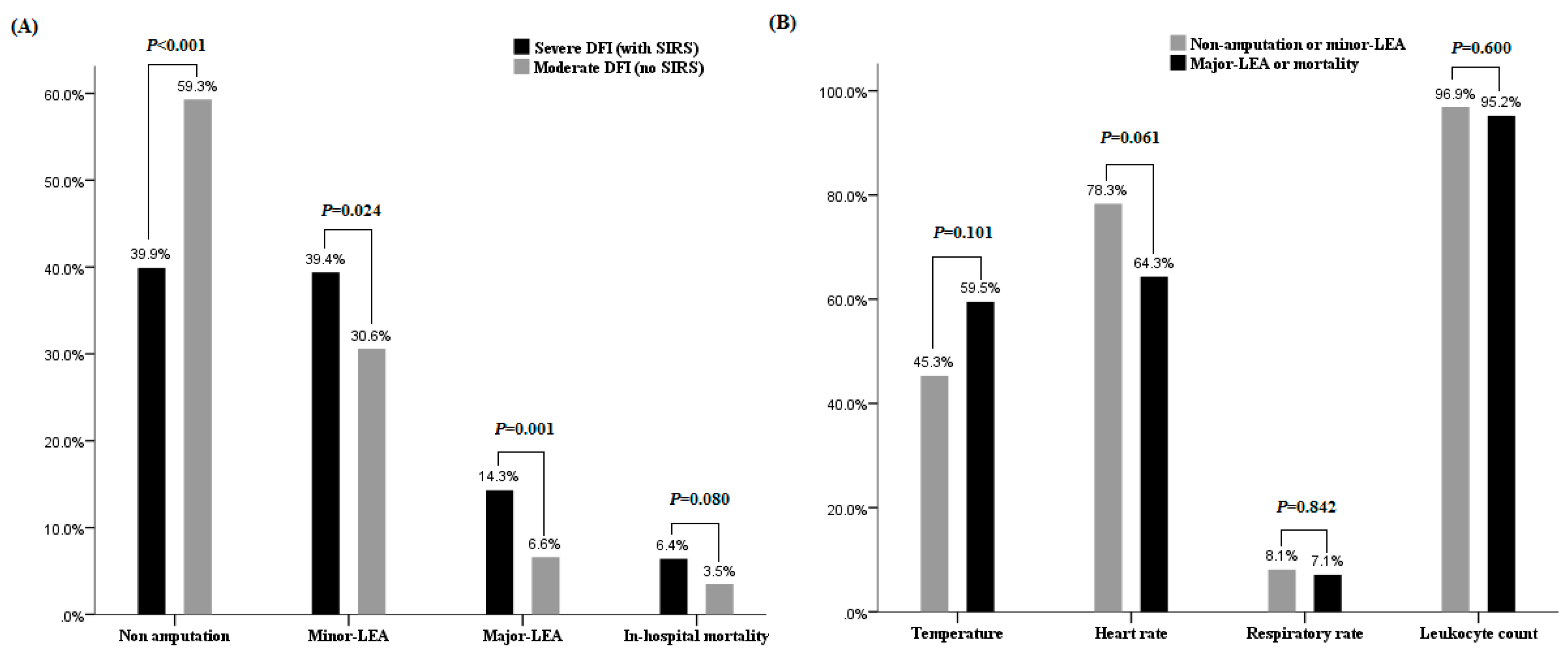
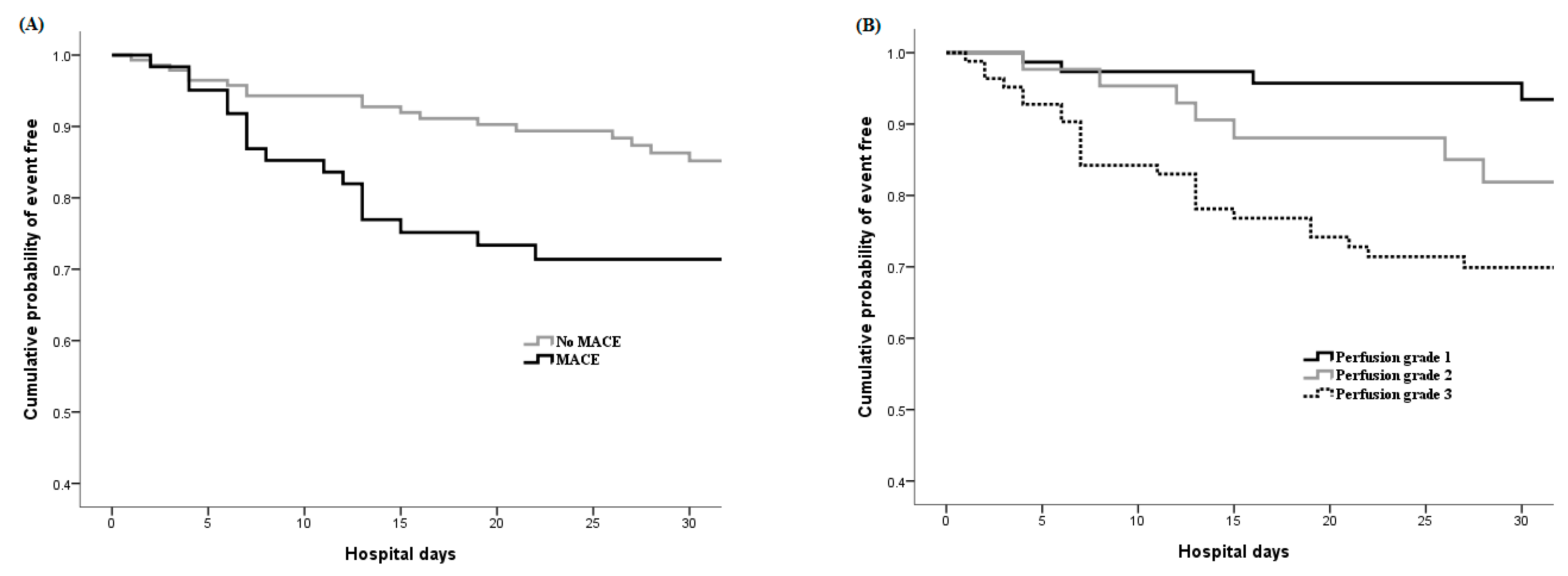
3.3. Prognosis and Prognostic Factors Analysis in Patients Presenting SIRS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lipsky, B.A. Medical treatment of diabetic foot infections. Clin. Infect. Dis. 2004, 39 (Suppl. 2), S104–S114. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Lipsky, B.A. Diabetic foot infections: Stepwise medical and surgical management. Int. Wound J. 2004, 1, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Lynar, S.A.; Robinson, C.H.; Boutlis, C.S.; Commons, R.J. Risk factors for mortality in patients with diabetic foot infections: A prospective cohort study. Intern. Med. J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Ndosi, M.; Wright-Hughes, A.; Brown, S.; Backhouse, M.; Lipsky, B.A.; Bhogal, M.; Reynolds, C.; Vowden, P.; Jude, E.B.; Nixon, J.; et al. Prognosis of the infected diabetic foot ulcer: A 12-month prospective observational study. Diabet. Med. 2018, 35, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J.M.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017; Centers for Disease Control and Prevention, U.S. Department of Health and Human Services: Atlanta, GA, USA, 2017. [Google Scholar]
- Hicks, C.W.; Selvarajah, S.; Mathioudakis, N.; Sherman, R.E.; Hines, K.F.; Black, J.H., 3rd; Abularrage, C.J. Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs. Ann. Vasc. Surg. 2016, 33, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Y.; Lin, K.D.; Jiang, Y.D.; Chang, C.H.; Chung, C.H.; Chuang, L.M.; Tai, T.Y.; Ho, L.T.; Shin, S.J. Diabetes-related kidney, eye, and foot disease in Taiwan: An analysis of the nationwide data for 2000–2009. J. Formos. Med. Assoc. 2012, 111, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C. Diabetic foot ulcer classification system for research purposes: A progress report on criteria for including patients in research studies. Diabetes Metab. Res. Rev. 2004, 20 (Suppl. 1), S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2012, 54, e132–e173. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, L.U.; Pires, E.M.C.; Vieira, J.M., Jr.; Azevedo, L.C.P. Systemic inflammatory response syndrome criteria and the prediction of hospital mortality in critically ill patients: A retrospective cohort study. Rev. Bras. Ter. Intensiv. 2017, 29, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Wukich, D.K.; Hobizal, K.B.; Raspovic, K.M.; Rosario, B.L. SIRS is valid in discriminating between severe and moderate diabetic foot infections. Diabetes Care 2013, 36, 3706–3711. [Google Scholar] [CrossRef] [PubMed]
- Eneroth, M.; Apelqvist, J.; Stenstrom, A. Clinical characteristics and outcome in 223 diabetic patients with deep foot infections. Foot Ankle Int. 1997, 18, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.H.; Tsai, J.S.; Huang, C.H.; Lin, C.H.; Yang, H.M.; Chan, Y.S.; Hsieh, S.H.; Hsu, B.R.; Huang, Y.Y. Risk factors for lower extremity amputation in diabetic foot disease categorized by Wagner classification. Diabetes Res. Clin. Pract. 2012, 95, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.Y.; Chu, S.Y.; Wen, Y.W.; Hsu, L.A.; Chen, C.C.; Peng, S.H.; Huang, C.H.; Sun, J.H.; Huang, Y.Y. The value of Doppler waveform analysis in predicting major lower extremity amputation among dialysis patients treated for diabetic foot ulcers. Diabetes Res. Clin. Pract. 2013, 100, 181–188. [Google Scholar] [CrossRef]
- Hung, S.Y.; Huang, Y.Y.; Hsu, L.A.; Chen, C.C.; Yang, H.M.; Sun, J.H.; Lin, C.W.; Wang, C.C. Treatment for diabetic foot ulcers complicated by major cardiac events. Can. J. Diabetes 2015, 39, 183–187. [Google Scholar] [CrossRef]
- Lin, C.W.; Hsu, B.R.; Tsai, J.S.; Yang, H.M.; Lin, J.R.; Lin, C.H.; Huang, C.H.; Hung, S.Y.; Huang, Y.Y. Effect of limb preservation status and body mass index on the survival of patients with limb-threatening diabetic foot ulcers. J. Diabetes Complicat. 2017, 31, 180–185. [Google Scholar] [CrossRef][Green Version]
- Uccioli, L.; Meloni, M.; Izzo, V.; Giurato, L.; Merolla, S.; Gandini, R. Critical limb ischemia: Current challenges and future prospects. Vasc. Health Risk Manag. 2018, 14, 63–74. [Google Scholar] [CrossRef]
- Dinarello, C.A.; Gelfand, J.A.; Wolff, S.M. Anticytokine strategies in the treatment of the systemic inflammatory response syndrome. JAMA 1993, 269, 1829–1835. [Google Scholar] [CrossRef]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef] [PubMed]
- Fry, D.E.; Marek, J.M.; Langsfeld, M. Infection in the ischemic lower extremity. Surg. Clin. N. Am. 1998, 78, 465–479. [Google Scholar] [CrossRef]
- Pugin, J. How tissue injury alarms the immune system and causes a systemic inflammatory response syndrome. Ann. Intensiv. Care 2012, 2, 27. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.I.; Erqou, S.; Lima, T.A.; Robinson, A.H. Association between glycated haemoglobin and the risk of lower extremity amputation in patients with diabetes mellitus-review and meta-analysis. Diabetologia 2010, 53, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Katzmarzyk, P.T.; Horswell, R.; Wang, Y.; Johnson, J.; Heymsfield, S.B.; Cefalu, W.T.; Ryan, D.H.; Hu, G. HbA1c and lower-extremity amputation risk in low-income patients with diabetes. Diabetes Care 2013, 36, 3591–3598. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.Y.; Liu, Y.K.; Chen, H.L.; Yang, H.L.; Liu, F. HbA1c and Lower Extremity Amputation Risk in Patients With Diabetes: A Meta-Analysis. Int. J. Low. Extrem. Wounds 2015, 14, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.W.; Hsu, L.A.; Chen, C.C.; Yeh, J.T.; Sun, J.H.; Lin, C.H.; Chen, S.T.; Hsu, B.R.; Huang, Y.Y. C-reactive protein as an outcome predictor for percutaneous transluminal angioplasty in diabetic patients with peripheral arterial disease and infected foot ulcers. Diabetes Res. Clin. Pract. 2010, 90, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Bellomo, R. Stress hyperglycemia: An essential survival response! Crit. Care 2013, 17, 305. [Google Scholar] [CrossRef] [PubMed]
- McCowen, K.C.; Malhotra, A.; Bistrian, B.R. Stress-induced hyperglycemia. Crit. Care Clin. 2001, 17, 107–124. [Google Scholar] [CrossRef]
- Gyurko, R.; Siqueira, C.C.; Caldon, N.; Gao, L.; Kantarci, A.; Van Dyke, T.E. Chronic Hyperglycemia Predisposes to Exaggerated Inflammatory Response and Leukocyte Dysfunction in Akita Mice. J. Immunol. 2006, 177, 7250–7256. [Google Scholar] [CrossRef]
- Tuladhar, E.T.; Sharma, V.K.; Sigdel, M.; Shrestha, L. Type 2 diabetes mellitus with early phase acute inflammation protein and A1c. J. Pathol. Nepal 2012, 2, 211–214. [Google Scholar] [CrossRef]
- Morbach, S.; Furchert, H.; Groblinghoff, U.; Hoffmeier, H.; Kersten, K.; Klauke, G.T.; Klemp, U.; Roden, T.; Icks, A.; Haastert, B.; et al. Long-term prognosis of diabetic foot patients and their limbs: Amputation and death over the course of a decade. Diabetes Care 2012, 35, 2021–2027. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Y.; Lin, C.W.; Yang, H.M.; Hung, S.Y.; Chen, I.W. Survival and associated risk factors in patients with diabetes and amputations caused by infectious foot gangrene. J. Foot Ankle Res. 2018, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care 2003, 26, 3333–3341. [Google Scholar] [CrossRef] [PubMed]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e686–e725. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | DFI Presenting SIRS (N = 203) | Grade 3 DFI (N = 519) | p Value | ||
|---|---|---|---|---|---|
| Age (years) | 60.3 | [52.5; 67.9] | 66.0 | [56.6; 76.3] | <0.001 * |
| Male gender | 125 | (61.6%) | 319 | (61.5%) | 0.978 |
| Diabetes duration (years) | 12.0 | [5.0; 20.0] | 15.0 | [7.0; 20.0] | 0.040 * |
| Smoker | 88 | (43.3%) | 204 | (39.3%) | 0.320 |
| Hypertension | 136 | (67.0%) | 367 | (70.7%) | 0.329 |
| MACE a History | 61 | (30.0%) | 187 | (36.0%) | 0.128 |
| Retinopathy | 115 | (56.7%) | 299 | (57.6%) | 0.815 |
| Renal status | 0.563 | ||||
| eGFR ≥60 | 84 | (41.4%) | 226 | (43.5%) | |
| eGFR <60 | 84 | (41.4%) | 193 | (37.2%) | |
| Dialysis | 35 | (17.2%) | 100 | (19.3%) | |
| HbA1c (%) | 9.6 | [7.6; 11.3] | 8.1 | [6.8; 10.16] | <0.001 * |
| Perfusion score | 0.192 | ||||
| Grade 1 | 77 | (37.9%) | 187 | (36.0%) | |
| Grade 2 | 31 | (15.3%) | 110 | (21.2%) | |
| Grade 3 | 95 | (46.8%) | 222 | (42.8%) | |
| Extent size (cm2) | 15.0 | [6.0; 45.0] | 9.0 | [4.0; 25.5] | <0.001 * |
| Depth/tissue loss score | 0.175 | ||||
| Grade 1 | 9 | (4.4%) | 43 | (8.3%) | |
| Grade 2 | 47 | (23.2%) | 124 | (23.9%) | |
| Grade 3 | 147 | (72.4%) | 352 | (67.8%) | |
| Sensation | 0.156 | ||||
| Grade 1 | 100 | (49.3%) | 285 | (55.1%) | |
| Grade 2 | 103 | (50.7%) | 232 | (44.9%) | |
| Osteomyelitis | 82 | (40.4%) | 202 | (38.9%) | 0.716 |
| Days before visit | 15.5 | [9.0; 44.25] | 23.5 | [9.0; 60.0] | 0.066 |
| Hospital stay (days) | 39.0 | [24.0; 57.0] | 26.0 | [15.0; 40.0] | <0.001 * |
| Characteristic | Non-Amputation or Minor LEA a (n = 161) | Major LEA or Death b (n = 42) | p Value | Odds Ratio c (95% CI) | p Value | ||
|---|---|---|---|---|---|---|---|
| Age (years) | 60.0 | [50.3; 67.6] | 62.2 | [57.8; 73.3] | 0.053 | ||
| MACE history | 39 | (24.2%) | 22 | (52.4%) | <0.001 * | 2.41* (1.06–5.47) | 0.036 * |
| Retinopathy | 84 | (52.2%) | 31 | (73.8%) | 0.012 * | 1.89 (0.81–4.41) | 0.141 |
| Renal status | <0.001 * | ||||||
| eGFR ≥60 | 70 | (43.5%) | 14 | (33.3%) | 1 | ||
| eGFR <60 | 74 | (46.0%) | 10 | (23.8%) | 0.46 (0.17–1.24) | 0.124 | |
| Dialysis | 17 | (10.6%) | 18 | (42.9%) | 2.38 (0.88–6.47) | 0.089 | |
| HbA1c (%) | 9.7 | [7.8; 11.4] | 9.25 | [7.23; 10.88] | 0.220 | ||
| Perfusion score | <0.001 * | ||||||
| Grade 1 | 72 | (44.7%) | 5 | (11.9%) | 1 | ||
| Grade 2 | 26 | (16.1%) | 5 | (11.9%) | 1.40 (0.32–6.24) | 0.658 | |
| Grade 3 | 63 | (39.1%) | 32 | (76.2%) | 3.37* (1.04–10.94) | 0.044 * | |
| Extent size (cm2) | 11.3 | [4.98; 35.0] | 44.5 | [20.75; 102.38] | <0.001 * | 1.003* (1.00–1.01) | 0.017 * |
| Depth/tissue loss | 0.038 | ||||||
| Grade 1 | 8 | (5.0%) | 1 | (2.4%) | 1 | ||
| Grade 2 | 43 | (26.7%) | 4 | (9.5%) | 0.95 (0.08–11.64) | 0.989 | |
| Grade 3 | 110 | (68.3%) | 37 | (88.1%) | 1.93 (0.20–18.58) | 0.568 | |
| Sensation | 0.135 | ||||||
| Grade 1 | 75 | (46.6%) | 25 | (59.5%) | |||
| Grade 2 | 86 | (53.4%) | 17 | (40.5%) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-W.; Hung, S.-Y.; Huang, C.-H.; Yeh, J.-T.; Huang, Y.-Y. Diabetic Foot Infection Presenting Systemic Inflammatory Response Syndrome: A Unique Disorder of Systemic Reaction from Infection of the Most Distal Body. J. Clin. Med. 2019, 8, 1538. https://doi.org/10.3390/jcm8101538
Lin C-W, Hung S-Y, Huang C-H, Yeh J-T, Huang Y-Y. Diabetic Foot Infection Presenting Systemic Inflammatory Response Syndrome: A Unique Disorder of Systemic Reaction from Infection of the Most Distal Body. Journal of Clinical Medicine. 2019; 8(10):1538. https://doi.org/10.3390/jcm8101538
Chicago/Turabian StyleLin, Cheng-Wei, Shih-Yuan Hung, Chung-Huei Huang, Jiun-Ting Yeh, and Yu-Yao Huang. 2019. "Diabetic Foot Infection Presenting Systemic Inflammatory Response Syndrome: A Unique Disorder of Systemic Reaction from Infection of the Most Distal Body" Journal of Clinical Medicine 8, no. 10: 1538. https://doi.org/10.3390/jcm8101538
APA StyleLin, C.-W., Hung, S.-Y., Huang, C.-H., Yeh, J.-T., & Huang, Y.-Y. (2019). Diabetic Foot Infection Presenting Systemic Inflammatory Response Syndrome: A Unique Disorder of Systemic Reaction from Infection of the Most Distal Body. Journal of Clinical Medicine, 8(10), 1538. https://doi.org/10.3390/jcm8101538