Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Walk and Meditation Protocol
2.3. Assessment of Cognition
2.4. Additional Assessments
2.5. Statistical Analysis
3. Results
3.1. Manipulation Check
3.2. Main Outcomes
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Lambourne, K.; Tomporowski, P. The effect of exercise-induced arousal on cognitive task performance: A meta-regression analysis. Brain Res. 2010, 1341, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Herod, S.M.; Cardinal, B.J.; Noakes, T.D. Physical activity and the brain: A review of this dynamic, bi-directional relationship. Brain Res. 2013, 1539, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Piepmeier, A.T.; Etnier, J.L. Brain-derived neurotrophic factor (BDNF) as a potential mechanism of the effects of acute exercise on cognitive performance. J. Sport Health Sci. 2015, 4, 14–23. [Google Scholar] [CrossRef]
- Kempermann, G.; Fabel, K.; Ehninger, D.; Babu, H.; Leal-Galicia, P.; Garthe, A.; Wolf, S.A. Why and how physical activity promotes experience-induced brain plasticity. Front Neurosci. 2010, 4, 189. [Google Scholar] [CrossRef] [PubMed]
- Ying, S.W.; Futter, M.; Rosenblum, K.; Webber, M.J.; Hunt, S.P.; Bliss, T.V.; Bramham, C.R. Brain-derived neurotrophic factor induces long-term potentiation in intact adult hippocampus: Requirement for ERK activation coupled to CREB and upregulation of Arc synthesis. J. Neurosci. 2002, 22, 1532–1540. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, A.; Calati, R.; Serretti, A. Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clin. Psychol. Rev. 2011, 31, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, F.; Johnson, S.K.; Diamond, B.J.; David, Z.; Goolkasian, P. Mindfulness meditation improves cognition: Evidence of brief mental training. Conscious Cogn. 2010, 19, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Holzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Shors, T.J.; Olson, R.L.; Bates, M.E.; Selby, E.A.; Alderman, B.L. Mental and Physical (MAP) Training: A neurogenesis-inspired intervention that enhances health in humans. Neurobiol. Learn. Mem. 2014, 115, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Alderman, B.L.; Olson, R.L.; Brush, C.J.; Shors, T.J. MAP training: Combining meditation and aerobic exercise reduces depression and rumination while enhancing synchronized brain activity. Transl. Psychiatry 2016, 6, e726. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Lutz, A.; Slagter, H.A.; Dunne, J.D.; Davidson, R.J. Attention regulation and monitoring in meditation. Trends Cogn. Sci. 2008, 12, 163–169. [Google Scholar] [CrossRef] [PubMed]
- MCMorris, T. Exercise and cognitive functions: A neuroendocrinological explanation. In Exercise and Cognitive Function; McMorris, T., Tomporowski, P.D., Audiffren, M., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 41–68. [Google Scholar]
- Hopthrow, T.; Hooper, N.; Mahmood, L.; Meier, B.P.; Weger, U. Mindfulness reduces the correspondence bias. Q. J. Exp. Psychol. 2017, 70, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Maruff, P.; Thomas, E.; Cysique, L.; Brew, B.; Collie, A.; Snyder, P.; Pietrzak, R.H. Validity of the CogState brief battery: Relationship to standardized tests and sensitivity to cognitive impairment in mild traumatic brain injury, schizophrenia, and AIDS dementia complex. Arch. Clin. Neuropsychol. 2009, 24, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Fratti, S.; Bowden, S.C.; Cook, M.J. Reliability and validity of the CogState computerized battery in patients with seizure disorders and healthy young adults: Comparison with standard neuropsychological tests. Clin. Neuropsychol. 2017, 31, 569–586. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cubillo, I.; Perianez, J.A.; Adrover-Roig, D.; Rodríguez-Sánchez, J.M.; Ríos-Lago, M.; Tirapu, J.; Barceló, F. Construct validity of the Trail Making Test: Role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J. Int. Neuropsychol. Soc. 2009, 15, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Potvin, S.; Charbonneau, G.; Juster, R.P.; Purdon, S.; Tourjman, S.V. Self-evaluation and objective assessment of cognition in major depression and attention deficit disorder: Implications for clinical practice. Compr. Psychiatry 2016, 70, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Shaw, S.; Oei, T.P.; Sawang, S. Psychometric validation of the Dysexecutive Questionnaire (DEX). Psychol. Assess. 2015, 27, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Walach, H.; Buchheld, N.; Buttenmuller, V.; Kleinknecth, N.; Schmidt, S. Measuring mindfulness- the Freiburg Mindfulness Inventory (FMI). Personal. Individ. Differ. 2006, 40, 1543–1555. [Google Scholar] [CrossRef]
- Johnson, D.C.; Polusny, M.A.; Erbes, C.R.; King, D.; King, L.; Litz, B.T.; Schnurr, P.P.; Friedman, M.; Pietrzak, R.H.; Southwick, S.M. Development and initial validation of the Response to Stressful Experiences Scale. Mil. Med. 2011, 176, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Marciniak, R.; Sheardova, K.; Cermakova, P.; Hudecek, D.; Sumec, R.; Hort, J. Effect of meditation on cognitive functions in context of aging and neurodegenerative diseases. Front. Behav. Neurosci. 2014, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Jindal, V.; Gupta, S.; Das, R. Molecular mechanisms of meditation. Mol. Neurobiol. 2013, 48, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Crush, E.A.; Loprinzi, P.D. Dose-Response Effects of Exercise Duration and Recovery on Cognitive Functioning. Percept. Mot Skills 2017, 124, 1164–1193. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Frith, E.; Edwards, M.K.; Sng, E.; Ashpole, N. The effects of exercise on memory function among young- to middle-age adults: Systematic review and recommendations for future research. Am. J. Health Promot. 2017, 32, 691–704. [Google Scholar] [CrossRef] [PubMed]
- Frith, E.; Sng, E.; Loprinzi, P.D. Randomized controlled trial evaluating the temporal effects of high-intensity exercise on learning, short-term and long-term memory, and prospective memory. Eur. J. Neurosci. 2017, 46, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Edwards, M.K.; Frith, E. Potential avenues for exercise to activate episodic memory-related pathways: A narrative review. Eur. J. Neurosci. 2017, 46, 2067–2077. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Frith, E. A brief primer on the mediational role of BDNF in the exercise-memory link. Clin. Physiol. Funct. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Gur, R.M.; David, Z.; Currier, E. One session mindfulness meditation: A randomized controlled study of effects on cognition and mood. Mindfulness 2015, 6, 88–98. [Google Scholar] [CrossRef]
- Schmolesky, M.T.; Webb, D.L.; Hansen, R.A. The effects of aerobic exercise intensity and duration on levels of brain-derived neurotrophic factor in healthy men. J. Sports Sci. Med. 2013, 12, 502–511. [Google Scholar] [PubMed]
- Jaffery, A.; Edwards, M.K.; Loprinzi, P.D. The Effects of Acute Exercise on Cognitive Function: Solomon Experimental Design. J. Prim. Prev. 2018, 39, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.K.; Loprinzi, P.D. Effects of a Sedentary Behavior-Inducing Randomized Controlled Intervention on Depression and Mood Profile in Active Young Adults. Mayo Clin. Proc. 2016, 91, 984–998. [Google Scholar] [CrossRef] [PubMed]
- Ebben, W.; Brudzynski, L. Motivations and barriers to exercise among college students. J. Physiol. Online 2008, 11, 1–11. [Google Scholar]

{kind=link}
| Group | ||||
|---|---|---|---|---|
| Variable | Walking + Meditation (n = 22) | Meditation + Walking (n = 22) | Control (n = 22) | P-Value Ψ |
| Age, mean years | 21.2 (2.3) | 20.7 (1.7) | 20.9 (2.5) | 0.11 |
| Gender, % male | 27.3 | 22.7 | 36.4 | 0.85 |
| Race, % | 0.57 | |||
| Mexican American | 0 | 0 | 4.5 | |
| Other Hispanic | 0 | 4.5 | 0 | |
| Non-Hispanic White | 77.3 | 59.1 | 77.3 | |
| Non-Hispanic Black | 13.6 | 13.6 | 9.1 | |
| Other | 9.1 | 22.7 | 9.1 | |
| BMI, mean kg/m2 | 23.1 (4.1) | 24.4 (4.2) | 24.6 (4.5) | 0.64 |
| MVPA, mean min | 268.6 (213.4) | 287.4 (137.5) | 328.5 (416.3) | 0.79 |
| Previous meditation experience, % | 63.6 | 50.0 | 59.1 | 0.38 |
| Currently meditating, % | 36.4 | 62.5 | 50.0 | 0.86 |
| Last meal, mean h | 3.8 (3.1) | 4.4 (4.7) | 4.0 (3.7) | 0.82 |
| Dysexecutive function, mean score | 44.9 (12.6) | 42.5 (12.3) | 47.8 (14.9) | 0.64 |
| Emotion regulation, mean score | 72.7 (18.2) | 73.7 (18.8) | 72.6 (19.8) | 0.83 |
| Mindfulness, mean score | 39.2 (5.3) | 38.9 (5.3) | 39.5 (7.2) | 0.40 |
| Stress responses, mean score | 67.1 (11.4) | 68.2 (10.0) | 66.0 (11.2) | 0.68 |
| Heart Rate, mean | ||||
| Resting | 74.4 (10.7) | 70.1 (11.0) | 67.9 (12.6) | 0.15 |
| 5 min exercise | 111.7 (18.1) | 104.4 (22.8) | N/A | 0.49 |
| 9 min exercise | 113.1 (17.2) | 108.8 (22.7) | N/A | 0.60 |
| 5 min meditation | 68.7 (11.6) | 63.1 (9.5) | N/A | 0.32 |
| 9 min meditation | 66.8 (10.4) | 61.5 (9.8) | N/A | 0.36 |
| 5 min control | N/A | N/A | 69.2 (14.5) | |
| 9 min control | N/A | N/A | 68.9 (14.8) | |
| 3 min post | 75.3 (12.5) | 71.5 (15.4) | 67.9 (14.1) | 0.46 |
| RPE, mean | 9.0 (2.4) | 9.5 (1.8) | N/A | 0.69 |
| Speed, mean km/h | 6.1 (2.4) | 5.6 (2.7) | N/A | 0.38 |
| Group | ||||
|---|---|---|---|---|
| Cognitive Function Parameter | Walk then Meditate | Meditate then Walk | Control | P-Value |
| Identification Task | 0.45 | |||
| Baseline | 0.7 (0.8) | 0.8 (2.1) | 0.5 (0.9) | |
| Post-Intervention | 1.0 (1.3) | 0.7 (0.9) | 3.1 (11.7) | |
| Set-Shifting Task | 0.29 | |||
| Baseline | 23.0 (14.2) | 26.0 (16.1) | 27.3 (15.1) | |
| Post-Intervention | 23.3 (16.8) | 24.7 (14.2) | 22.2 (16.1) | |
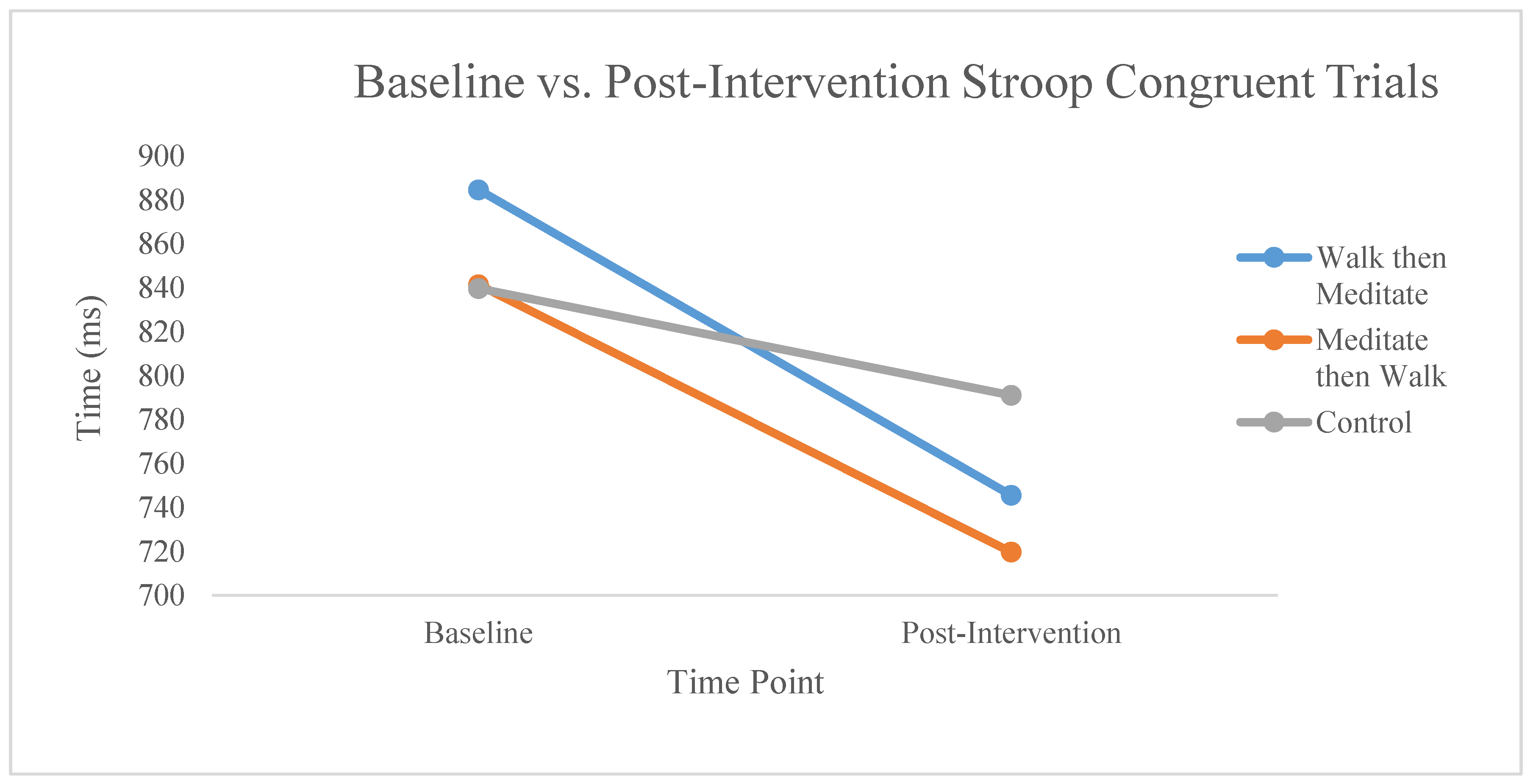
| Stroop Task (ms) | ||||
| Congruent Trials | 0.05 | |||
| Baseline | 884.6 (262.8) | 841.4 (181.6) | 839.7 (199.9) | |
| Post-Intervention | 745.5 (214.7) | 719.6 (126.6) | 791.0 (109.9) | |
| Incongruent Trials | 0.23 | |||
| Baseline | 1096.9 (409.1) | 1039.4 (218.1) | 1044.1 (203.4) | |
| Post-Intervention | 928.3 (235.5) | 917.9 (195.0) | 971.2 (169.9) | |
| Control Trials | 0.65 | |||
| Baseline | 891.8 (344.9) | 862.1 (256.6) | 829.3 (164.4) | |
| Post-Intervention | 776.6 (231.1) | 730.0 (135.5) | 749.2 (100.0) | |
| Subjective Cognition | ||||
| Attention | 0.75 | |||
| Baseline | 78.0 (20.0) | 76.8 (23.1) | 79.6 (18.5) | |
| Post-Intervention | 78.1 (18.0) | 80.2 (23.6) | 78.5 (19.6) | |
| Task-Switching | 0.09 | |||
| Baseline | 85.5 (13.8) | 77.5 (18.7) | 79.0 (20.9) | |
| Post-Intervention | 75.7 (21.3) | 82.3 (24.1) | 77.9 (19.4) | |
| Flexibility | 0.90 | |||
| Baseline | 61.4 (25.5) | 54.8 (25.4) | 53.5 (23.2) | |
| Post-Intervention | 57.1 (27.1) | 53.7 (26.0) | 49.3 (23.4) | |
| Inhibition | 0.57 | |||
| Baseline | 80.6 (22.0) | 79.3 (23.1) | 84.9 (18.6) | |
| Post-Intervention | 71.7 (28.7) | 61.2 (32.0) | 72.8 (27.4) | |
| Trail Making (s) | ||||
| Trail Making A | 0.50 | |||
| Baseline | 16.2 (4.1) | 17.0 (3.8) | 16.4 (4.0) | |
| Post-Intervention | 13.8 (3.0) | 13.8 (3.2) | 14.1 (2.9) | |
| Trail Making B | 0.53 | |||
| Baseline | 51.0 (37.3) | 38.2 (7.9) | 38.5 (25.0) | |
| Post-Intervention | 39.4 (16.5) | 34.1 (13.1) | 32.3 (11.2) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edwards, M.K.; Loprinzi, P.D. Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function. J. Clin. Med. 2018, 7, 125. https://doi.org/10.3390/jcm7060125
Edwards MK, Loprinzi PD. Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function. Journal of Clinical Medicine. 2018; 7(6):125. https://doi.org/10.3390/jcm7060125
Chicago/Turabian StyleEdwards, Meghan K., and Paul D. Loprinzi. 2018. "Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function" Journal of Clinical Medicine 7, no. 6: 125. https://doi.org/10.3390/jcm7060125
APA StyleEdwards, M. K., & Loprinzi, P. D. (2018). Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function. Journal of Clinical Medicine, 7(6), 125. https://doi.org/10.3390/jcm7060125