The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of Patients at Referral
3.2. Prevalence of Comorbidities in Stage 3–5 CKD Patients
3.3. Factors Associated with Multimorbidity
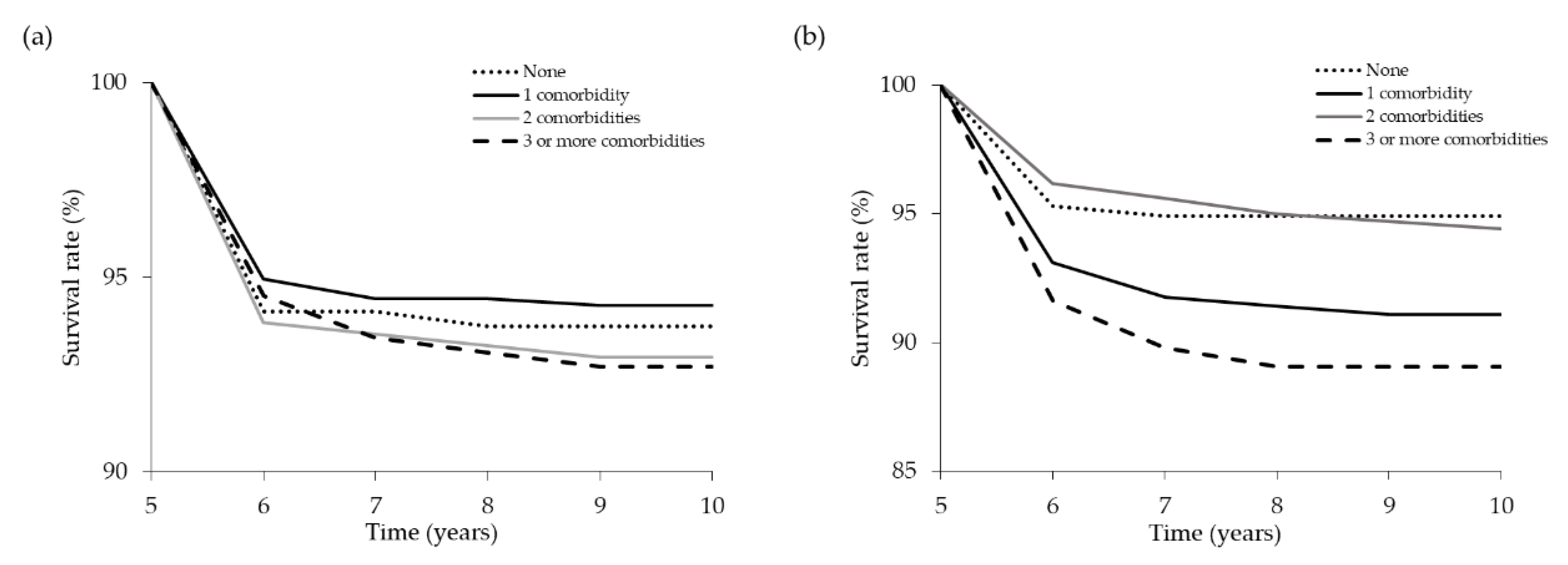
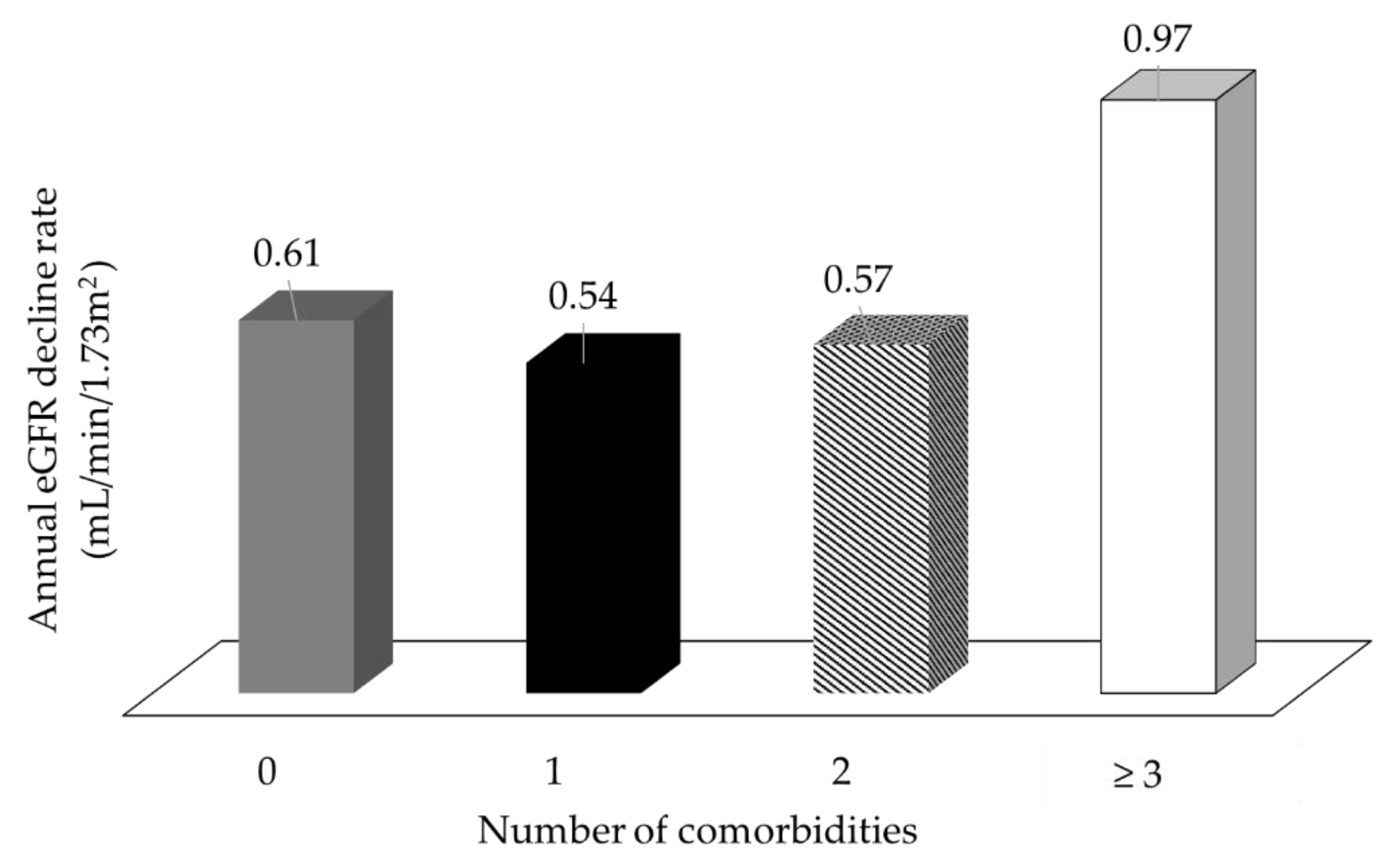
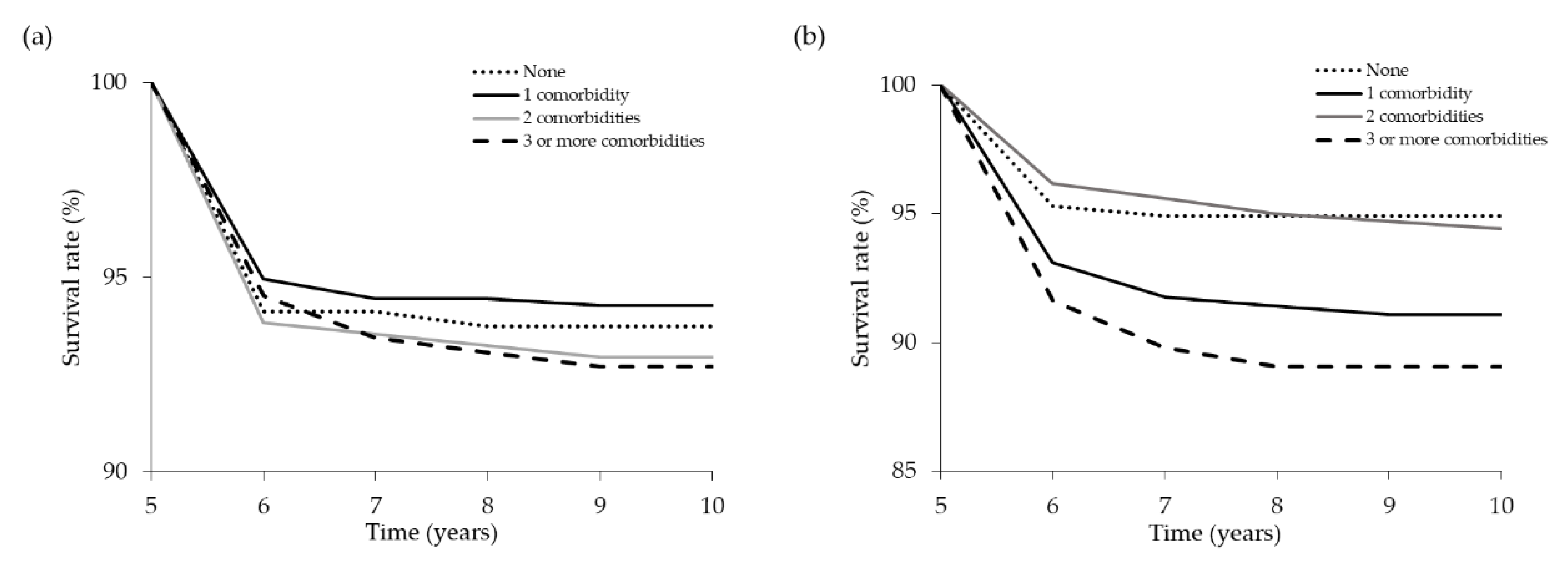
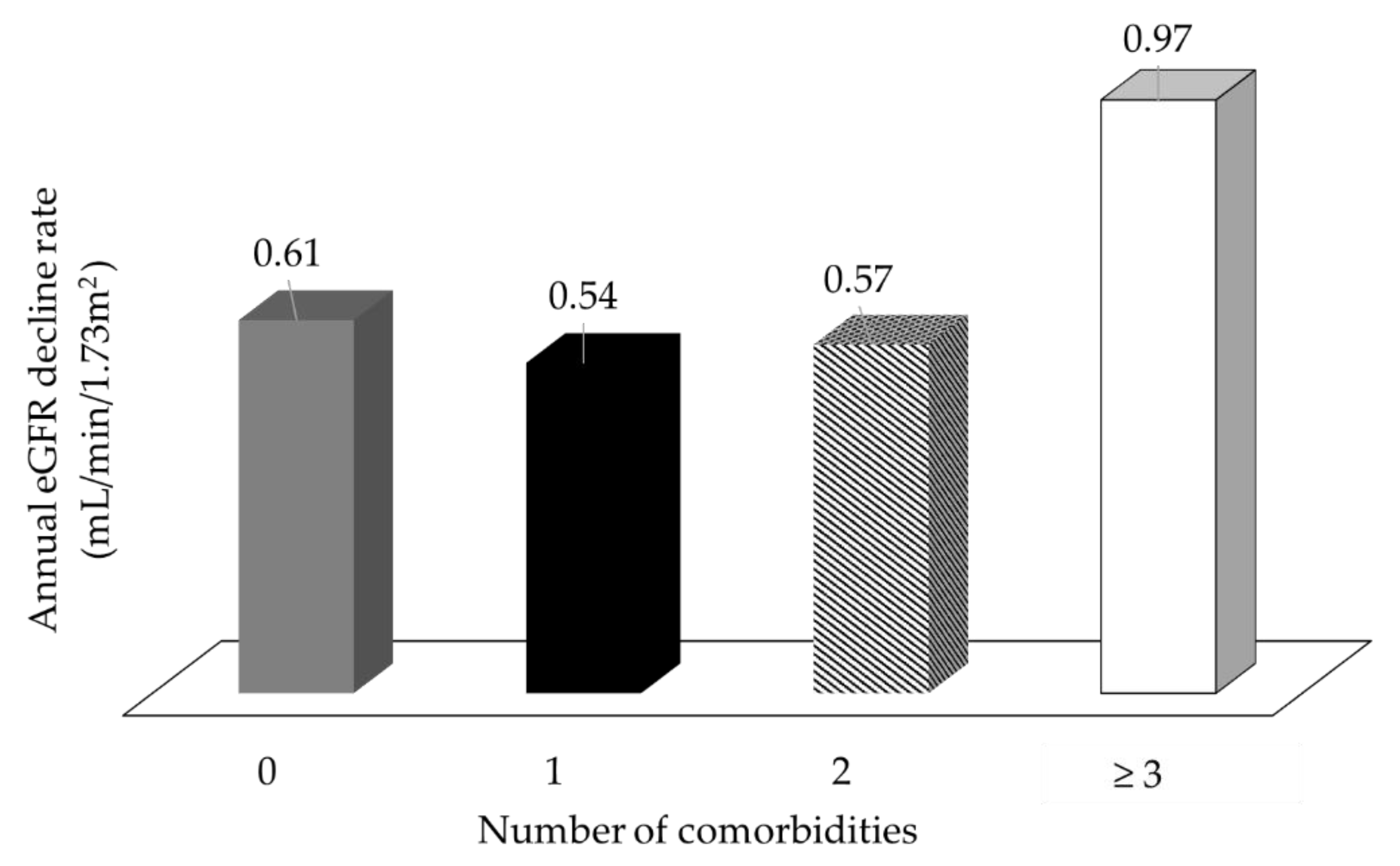
3.4. Number of Comorbidities Predicts Poor Renal Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- De Nicola, L.; Minutolo, R. Worldwide growing epidemic of ckd: Fact or fiction? Kidney Int. 2016, 90, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.J.; Li, S.; Gilbertson, D.T.; Liu, J.; Chen, S.C.; Herzog, C.A. Chronic kidney disease and cardiovascular disease in the Medicare population: Management of comorbidities in kidney disease in the 21st century: Anemia and bone disease. Kidney Int. Suppl. 2003, 243, 24–31. [Google Scholar] [CrossRef]
- Foley, R.N.; Murray, A.M.; Li, S.; Herzog, C.A.; McBean, A.M.; Eggers, P.W.; Collins, A.J. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the united states medicare population, 1998 to 1999. J. Am. Soc. Nephrol. 2005, 16, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Keith, D.S.; Nichols, G.A.; Gullion, C.M.; Brown, J.B.; Smith, D.H. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern. Med. 2004, 164, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Massy, Z.; Argiles, A.; Spasovski, G.; Verbeke, F.; Lameire, N.; European Uremic Toxin Work Group. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol. Dial. Transplant. 2005, 20, 1048–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef]
- Donald, M.; Kahlon, B.K.; Beanlands, H.; Straus, S.; Ronksley, P.; Herrington, G.; Tong, A.; Grill, A.; Waldvogel, B.; Large, C.A.; et al. Self-management interventions for adults with chronic kidney disease: A scoping review. BMJ Open 2018, 8, e019814. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.E.; Levin, A.; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Fraser, S.D.; Taal, M.W. Multimorbidity in people with chronic kidney disease: Implications for outcomes and treatment. Curr. Opin. Nephrol. Hypertens 2016, 25, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Fraser, S.D.; Roderick, P.J.; May, C.R.; McIntyre, N.; McIntyre, C.; Fluck, R.J.; Shardlow, A.; Taal, M.W. The burden of comorbidity in people with chronic kidney disease stage 3: A cohort study. BMC Nephrol. 2015, 16, 193. [Google Scholar] [CrossRef] [PubMed]
- Titze, S.; Schmid, M.; Kottgen, A.; Busch, M.; Floege, J.; Wanner, C.; Kronenberg, F.; Eckardt, K.U.; Titze, S.; Prokosch, H.-U.; et al. Disease burden and risk profile in referred patients with moderate chronic kidney disease: Composition of the German Chronic Kidney Disease (GCKD) cohort. Nephrol. Dial. Transplant. 2015, 30, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Bowling, C.B.; Plantinga, L.; Phillips, L.S.; McClellan, W.; Echt, K.; Chumbler, N.; McGwin, G.; Vandenberg, A.; Allman, R.M.; Johnson, T.M., II. Association of multimorbidity with mortality and healthcare utilization in chronic kidney disease. J. Am. Geriatr. Soc. 2017, 65, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Beddhu, S.; Bruns, F.J.; Saul, M.; Seddon, P.; Zeidel, M.L. A simple comorbidity scale predicts clinical outcomes and costs in dialysis patients. Am. J. Med. 2000, 108, 609–613. [Google Scholar] [CrossRef]
- Hemmelgarn, B.R.; Manns, B.J.; Quan, H.; Ghali, W.A. Adapting the charlson comorbidity index for use in patients with ESRD. Am. J. Kidney Dis. 2003, 42, 125–132. [Google Scholar] [CrossRef]
- Park, J.Y.; Kim, M.H.; Han, S.S.; Cho, H.; Kim, H.; Ryu, D.R.; Kim, H.; Lee, H.; Lee, J.P.; Lim, C.S.; et al. Recalibration and validation of the charlson comorbidity index in Korean incident hemodialysis patients. PLoS ONE 2015, 10, e0127240. [Google Scholar] [CrossRef] [PubMed]
- Rattanasompattikul, M.; Feroze, U.; Molnar, M.Z.; Dukkipati, R.; Kovesdy, C.P.; Nissenson, A.R.; Norris, K.C.; Kopple, J.D.; Kalantar-Zadeh, K. Charlson comorbidity score is a strong predictor of mortality in hemodialysis patients. Int. Urol. Nephrol. 2012, 44, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.; He, X.; Liu, X.; Shabir, S.; Ball, S.; Cockwell, P.; Inston, N.; Little, M.A.; Johnston, A.; Borrows, R. Mortality prediction after kidney transplantation: Comparative clinical use of 7 comorbidity indices. Exp. Clin. Transplant. 2011, 9, 32–41. [Google Scholar] [PubMed]
- Tonelli, M.; Wiebe, N.; Guthrie, B.; James, M.T.; Quan, H.; Fortin, M.; Klarenbach, S.W.; Sargious, P.; Straus, S.; Lewanczuk, R.; et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int. 2015, 88, 859–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucsi, I.; Kovacs, A.Z.; Molnar, M.Z.; Novak, M. Co-morbidity and quality of life in chronic kidney disease patients. J. Nephrol. 2008, 21 (Suppl. 13), 84–91. [Google Scholar]
- Stevens, L.A.; Li, S.; Wang, C.; Huang, C.; Becker, B.N.; Bomback, A.S.; Brown, W.W.; Burrows, N.R.; Jurkovitz, C.T.; McFarlane, S.I.; et al. Prevalence of CKD and comorbid illness in elderly patients in the united states: Results from the Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2010, 55, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, K.; May, C.R.; Montori, V.M.; Mair, F.S. Understanding patients’ experiences of treatment burden in chronic heart failure using normalization process theory. Ann. Fam. Med. 2011, 9, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Gunn, J.M.; Ayton, D.R.; Densley, K.; Pallant, J.F.; Chondros, P.; Herrman, H.E.; Dowrick, C.F. The association between chronic illness, multimorbidity and depressive symptoms in an australian primary care cohort. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Kahn, L.S.; Vest, B.M.; Madurai, N.; Singh, R.; York, T.R.; Cipparone, C.W.; Reilly, S.; Malik, K.S.; Fox, C.H. Chronic kidney disease (CKD) treatment burden among low-income primary care patients. Chronic Illn. 2015, 11, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Mair, F.S.; May, C.R. Thinking about the burden of treatment. BMJ 2014, 349, 6680. [Google Scholar] [CrossRef] [PubMed]
- May, C.; Montori, V.M.; Mair, F.S. We need minimally disruptive medicine. BMJ 2009, 339, 2803. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Puth, M.T.; Weckbecker, K.; Schmid, M.; Munster, E. Prevalence of multimorbidity in germany: Impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health 2017, 17, 826. [Google Scholar] [CrossRef] [PubMed]
- Fortin, M.; Haggerty, J.; Almirall, J.; Bouhali, T.; Sasseville, M.; Lemieux, M. Lifestyle factors and multimorbidity: A cross sectional study. BMC Public Health 2014, 14, 686. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.R.; Yang, Y.; Wang, S.C.; Chiu, P.F.; Chou, W.Y.; Lin, C.Y.; Chang, J.M.; Chen, T.W.; Ferng, S.H.; Lin, C.L. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: A 3-year prospective cohort study. Nephrol. Dial. Transplant. 2013, 28, 671–682. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.W.; Wang, S.Y.; Hsu, K.H.; Lee, C.C.; Sun, C.Y.; Tsai, C.J.; Wu, M.S. Multidisciplinary predialysis education decreases the incidence of dialysis and reduces mortality--A controlled cohort study based on the nkf/doqi guidelines. Nephrol. Dial. Transplant. 2009, 24, 3426–3433. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lee, Y.-T.; Lee, W.-C.; Ng, H.-Y.; Wu, C.-H.; Lee, C.-T. Goal attainment and renal outcomes in patients enrolled in the chronic kidney disease care program in taiwan: A 3-year observational study. Int. J. Health Care Qual. Assur. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wallace, E.; Salisbury, C.; Guthrie, B.; Lewis, C.; Fahey, T.; Smith, S.M. Managing patients with multimorbidity in primary care. BMJ 2015, 350. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| CKD Stage | |||||
|---|---|---|---|---|---|
| Characteristic | Category | 3 | 4 | 5 | Total n = 1463 |
| Total n = 819 | Total n = 468 | Total n = 176 | |||
| n (%) | n (%) | n (%) | n (% of total) | ||
| Sex | Male | 555 (67.8) | 256 (54.7) | 78 (44.3) | 889 (60.8) |
| Female | 264 (32.2) | 212 (45.3) | 98 (55.7) | 574 (39.2) | |
| Age | mean(SD) | 71.5 (12.3) | 72.4 (12.2) | 70.8 (12.5) | 71.7 (12.3) |
| 18–64 | 207 (25.3) | 117 (25.0) | 54 (30.7) | 378 (25.8) | |
| 65+ | 612 (74.7) | 351 (75.0) | 122 (69.3) | 1085 (74.2) | |
| Education status | No formal or elementary school | 407 (49.7) | 279 (59.6) | 110 (62.5) | 796 (54.4) |
| High school | 280 (34.2) | 141 (30.1) | 55 (31.3) | 476 (32.5) | |
| College or higher | 132 (16.1) | 48 (10.3) | 11 (6.3) | 191 (13.1) | |
| Smoking | Current | 94 (11.5) | 41 (8.8) | 6 (3.4) | 141 (9.6) |
| Ex-smoker | 183 (22.3) | 85 (18.2) | 27 (15.3) | 295 (20.2) | |
| Never | 542 (66.2) | 342 (73.1) | 143 (81.3) | 1027 (70.2) | |
| Proteinuria | Current | 353 (43.1) | 202 (43.2) | 91 (51.7) | 646 (44.2) |
| No proteinuria | 466 (56.9) | 266 (56.8) | 85 (48.3) | 817 (55.8) | |
| Number of comorbidities | None | 145 (17.7) | 79 (16.9) | 31 (17.6) | 255 (17.4) |
| 1 | 332 (40.5) | 190 (40.6) | 72 (40.9) | 594 (40.6) | |
| 2 | 194 (23.7) | 104 (22.2) | 42 (23.9) | 340 (23.2) | |
| 3 or more | 148 (18.1) | 95 (20.3) | 31 (17.6) | 274 (18.7) | |
| Comorbidity | CKD Stage 3 Total n = 819 | CKD Stage 4 Total n = 468 | CKD Stage 5 Total n = 176 | Total | ||||
|---|---|---|---|---|---|---|---|---|
| n | Prevalence (%) | n | Prevalence (%) | n | Prevalence (%) | n | Prevalence (%) | |
| Hypertension | 547 | 66.8 | 307 | 65.6 | 117 | 66.5 | 971 | 66.4 |
| Diabetes | 265 | 32.4 | 164 | 35.0 | 57 | 32.4 | 486 | 33.2 |
| Hyperlipidemia | 101 | 12.3 | 52 | 11.1 | 14 | 8.0 | 167 | 11.4 |
| Cerebrovascular disease | 59 | 7.2 | 24 | 5.1 | 8 | 4.5 | 91 | 6.2 |
| Malignancy | 33 | 4.0 | 23 | 4.9 | 5 | 2.8 | 61 | 4.2 |
| Liver disease | 32 | 3.9 | 9 | 1.9 | 5 | 2.8 | 46 | 3.1 |
| Anaemia | 8 | 1.0 | 14 | 3.0 | 11 | 6.3 | 33 | 2.3 |
| Ischemic heart disease | 13 | 1.6 | 12 | 2.6 | 3 | 1.7 | 28 | 1.9 |
| Gout | 13 | 1.6 | 12 | 2.6 | 3 | 1.7 | 28 | 1.9 |
| Connective tissue disease | 6 | 0.7 | 4 | 0.9 | 2 | 1.1 | 12 | 0.8 |
| Congestive heart failure | 3 | 0.4 | 5 | 1.1 | 1 | 0.6 | 9 | 0.6 |
| Tuberculosis | 1 | 0.1 | 2 | 0.2 | 1 | 0.6 | 4 | 0.3 |
| Variable | Two or More Comorbidities (vs. One or Fewer) | ||||
|---|---|---|---|---|---|
| Univariate | Multivariable * | ||||
| OR (95 % CI) | p-Value | OR (95 % CI) | p-Value | ||
| Age (vs. 65+) | 1.560 (1.22–1.99) | <0.001 | 1.759 (1.34–2.30) | <0.001 | |
| Sex (male vs. female) | 0.944 (0.76–1.16) | 0.595 | 1.152 (0.88–1.49) | 0.289 | |
| Education status (vs. no formal or elementary school) | High school | 0.967 (0.76–1.21) | 0.774 | 1.089 (0.84–1.40) | 0.509 |
| College or higher | 0.825 (0.59–1.14) | 0.246 | 1.018 (0.71–1.45) | 0.923 | |
| Smoking (vs. non-smokers) | Current smoker | 1.616 (1.13–2.30) | 0.008 | 1.908 (1.29–2.81) | 0.001 |
| Ex-smoker | 1.202 (0.92–1.56) | 0.168 | 1.270 (0.94–1.71) | 0.118 | |
| eGFR at study entry (mL/min per 1.73 m2, continuous) | 0.999 (0.99–1.00) | 0.798 | 0.998 (0.99–1.00) | 0.639 | |
| Proteinuria (vs. no proteinuria) | 1.405 (1.14–1.73) | 0.001 | 1.492 (1.20–1.84) | <0.001 | |
| Variable | Model 1 (Univariate) | Model 2 (Sociodemographic and Clinical Variables) | |||
|---|---|---|---|---|---|
| HR (95 % CI) | p-Value | HR (95 % CI) | p-Value | ||
| Number of comorbidities (vs none) | 1 | 1.708 (0.93–3.13) | 0.084 | 2.032 (1.10–3.74) | 0.023 |
| 2 | 1.023 (0.50–2.07) | 0.950 | 1.347 (0.65–2.75) | 0.415 | |
| 3 or more | 2.237 (1.16–4.29) | 0.015 | 2.971 (1.53–5.76) | 0.001 | |
| Age (vs. 65+) | 0.463 (0.30–0.69) | <0.001 | |||
| Sex (male vs. female) | 0.730 (0.46–1.13) | 0.162 | |||
| Education status (vs. no formal or low level of qualifications) | High school | 1.269 (0.83–1.93) | 0.266 | ||
| College or higher | 0.683 (0.34–1.36) | 0.282 | |||
| Smoking (vs. non-smokers) | Current smoker | 0.970 (0.47–1.97) | 0.933 | ||
| Ex-smoker | 1.049 (0.61–1.79) | 0.863 | |||
| eGFR at study entry (mL/min per 1.73 m2, continuous) | 0.932 (0.91–0.94) | <0.001 | |||
| Proteinuria (vs. no proteinuria) | 1.286 (0.88–1.87) | 0.191 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, W.-C.; Lee, Y.-T.; Li, L.-C.; Ng, H.-Y.; Kuo, W.-H.; Lin, P.-T.; Liao, Y.-C.; Chiou, T.T.-Y.; Lee, C.-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. https://doi.org/10.3390/jcm7120493
Lee W-C, Lee Y-T, Li L-C, Ng H-Y, Kuo W-H, Lin P-T, Liao Y-C, Chiou TT-Y, Lee C-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. Journal of Clinical Medicine. 2018; 7(12):493. https://doi.org/10.3390/jcm7120493
Chicago/Turabian StyleLee, Wen-Chin, Yueh-Ting Lee, Lung-Chih Li, Hwee-Yeong Ng, Wei-Hung Kuo, Pei-Ting Lin, Ying-Chun Liao, Terry Ting-Yu Chiou, and Chien-Te Lee. 2018. "The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease" Journal of Clinical Medicine 7, no. 12: 493. https://doi.org/10.3390/jcm7120493
APA StyleLee, W.-C., Lee, Y.-T., Li, L.-C., Ng, H.-Y., Kuo, W.-H., Lin, P.-T., Liao, Y.-C., Chiou, T. T.-Y., & Lee, C.-T. (2018). The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. Journal of Clinical Medicine, 7(12), 493. https://doi.org/10.3390/jcm7120493