
Treatment of Established Status Epilepticus


Abstract
:1. Introduction
2. Causes of Ongoing Status Epilepticus
3. Pharmacologic Treatment
3.1. Phenytoin/Fosphenytoin
3.2. Valproic Acid
3.3. Phenobarbital
3.4. Levetiracetam
3.5. Lacosamide
4. Future Directions
5. Conclusions
Conflicts of Interest
References
- Shorvon, S.D. Status Epilepticus: Its Clinical Features and Treatment in Children and Adults; Cambridge University Press: Cambridge, UK, 1994; p. 27. [Google Scholar]
- Jallon, P. Mortality in patients with epilepsy. Curr. Opin. Neurol. 2004, 17, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Logroscino, G.; Hesdorffer, D.C.; Cascino, G.; Hauser, W.A.; Coeytaux, A.; Galobardes, B.; Morabia, A.; Jallon, P. Mortality after a first episode of status epilepticus in the United States and Europe. Epilepsia 1997, 46, 46–48. [Google Scholar] [CrossRef] [PubMed]
- Trinka, E.; Cock, H.; Rossetti, A.; Scheffer, I.; Shinnar, S.; Shorvon, S.; Lowenstein, D. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia 2015, 56, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Abend, N.S.; Bearden, D.; Helbig, I.; McGuire, J.; Narula, S.; Panzer, J.A.; Topjian, A.; Dlugos, D.J. Status Epilepticus and Refractory Status Epilepticus Management. Semin. Pediatr. Neurol. 2014, 21, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Riviello, J.J.; Ashwal, S.; Hirtz, D.; Glauser, T.; Ballaban-Gil, K.; Kelley, K.; Morton, L.D.; Phillips, S.; Sloan, E.; Shinnar, S. Practice Parameter: Diagnostic assessment of the child with status epilepticus (an evidence-based review). Neurology 2006, 67, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.B.; Gao, R.; Su, Y.Y.; Zhao, J.W.; Zhang, Y.Z.; Wang, L.; Ren, Y.; Fan, C.Q. Valproate versus diazepam for generalized convulsive status epilepticus: A pilot study. Eur. J. Neurol. 2011, 18, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Löscher, W. Molecular mechanisms of drug resistance in status epilepticus. Epilepsia 2009, 50 (Suppl. 8), 19–21. [Google Scholar] [CrossRef] [PubMed]
- Betjemann, J.P.; Lowenstein, D.H. Status Epilepticus in adults. Lancet Neurol. 2015, 14, 615–624. [Google Scholar] [CrossRef]
- Meierkord, H.; Boon, P.; Engelsen, B.; Göcke, K.; Tinuper, P.; Holtkamp, M. EFNS guideline on the management of status epilepticus in adults. Eur. J. Neurol. 2010, 17, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Brophy, G.M.; Bell, R.; Classen, J.; Alldredge, B.; Bleck, T.P.; Glauser, T.; LaRoche, S.M.; Riviello, J.J., Jr.; Shutter, L.; Sperline, M.R.; et al. Guidelines for the Evaluation and Management of Status Epilepticus. Neurocritical Care Society Status Epilepticus Guideline Wiriting Committee. Neurocrit. Care 2012, 17, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Glauser, T.; Shinnar, S.; Gloss, D.; Alldredge, B.; Ayra, R.; Bainbridge, J.; Bare, M.; Bleck, T.; Dodson, E.; Garrity, L.; et al. Evidence-Based Guidline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016, 16, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Trinka, E.; Höfler, J.; Laitinger, M.; Brigo, F. Pharmacotherapy for Status Epilepticus. Drugs 2015, 75, 1499–1521. [Google Scholar] [CrossRef] [PubMed]
- Ogutu, B.R.; Newton, C.R.; Muchohi, S.N.; Otieno, G.O.; Edwards, G.; Watkins, W.M.; Kokwaro, G.O. Pharmacokinetics and clinical effects of phenytoin and fosphenytoin in children with severe malaria and status epilepticus. J. Clin. Pharmacol. 2003, 56, 112–119. [Google Scholar] [CrossRef]
- Treiman, D.M.; Meyers, P.D.; Walton, N.Y.; Collins, J.F.; Colling, C.; Rowan, R.; Handforth, A.; Faught, E.; Calabrese, V.P.; Uthman, B.M.; et al. A comparison of four treatments for generalized convulsive status epilepticus. N. Engl. J. Med. 1998, 339, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Brevoord, J.C.; Joosten, K.F.; Arts, W.F.; van Rooij, R.W.; de Hoog, M. Status Epilepticus: Clinical Analysis of a Treatment Protocol Based on Midazolam and Phenytoin. J. Clin. Neurol. 2005, 20, 476–481. [Google Scholar]
- Yasiry, Z.; Shorvon, S. The relative effectiveness of five antiepileptic drugs in treatment of benzodiazepine-resistant convulsive status epilepticus: A meta-analysis of published studies. Seizure 2014, 23, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Wasim, M.; Husain, A. Non-Convulsive Seizure Control in the Intensive Care Unit. Curr. Treat. Options Neurol. 2015, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gilad, R.; Izkovitz, N.; Dabby, R.; Rapoport, A.; Sadeh, M.; Weller, B.; Lampl, Y. Treatment of status epilepticus and acute repetitive seizures with i.v. valproic acid vs. phenytoin. Acta Neurol. Scand. 2008, 118, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Misra, U.K.; Kalita, J.; Patel, R. Sodium valproate vs. phenytoin in status epilepticus: A pilot study. Neurology 2006, 67, 340–342. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Kumar, N.; Chandra, R.; Gupta, G.; Antony, A.R.; Garg, N. Randomized study of intravenous valproate and phenytoin in status epilepticus. Seizure 2007, 16, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Malamiri, R.A.; Ghaempanah, M.; Khosroshahi, N.; Nikkhah, A.; Banarian, B.; Ashrafi, M.R. Efficacy and safety of intravenous sodium valproate versus phenobarbital in controlling convulsive status epilepticus and acute prolonged convulsive seizures in children: A randomized trial. Eur. J. Paediatr. Neurol. 2012, 16, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Du, C.; Wang, X. Levetiracetam for the treatment of status epilepticus. Expert Rev. Neurother. 2015, 15, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Knake, S.; Gruener, J.; Hattemer, K.; Klein, K.M.; Bauer, S.; Oertel, W.H.; Hamer, H.M.; Rosenow, F. Intraveous levetiracetam in the treatment of benzodiazepine refractory status epilepticus. J. Neurol. Neurosurg. Psychiatry 2008, 79, 588–589. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, V.; Januel, J.; Burnand, B.; Rossetti, A.O. Second-line status epilepticus treatment: Comparison of phenytoin, valproate and levetiracetam. Epilepsia 2011, 52, 1292–1296. [Google Scholar] [CrossRef] [PubMed]
- Höfler, J.; Trinka, E. Lacosamide as a new treatment option in status epilepticus. Epilepsia 2013, 54, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Husain, A. Lacosamide in status epilepticus: Update on the TRENdS study. Epilepsy Behav. 2015, 49, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Cock, H. Established Status Epilepticus Treatment Trial (ESETT). Epilepsia 2011, 52, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Bleck, T.; Cock, H.; Chamberlain, J.; Cloyd, J.; Connor, J.; Elm, J.; Jones, E.; Lowenstain, D.; Shinnar, S.; Silbergleit, R.; et al. The Established Status Epilepticus Trial 2013. Epilepsia 2013, 54, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Kapur, J. Established Status Epilepticus Treatment Trial (ESETT). NIH Research Portfolio Online Reporting Tools (RePORT). Project Number: 1U01NS088034-01. Available online: https://projectreporter.nih.gov/project_info_description.cfm?projectnumber=1U01NS088034-01 (accessed on 21 April 2016).
- A Pragmatic Randomized Controlled Trial of Intravenous Levetiracetam versus Interavenous Phenytoin in Terminating Acute, Prolonged Tonic Clonic Seizures Including Convulsive Status Epilepticus in Children, the EcLiPSE Study: Emergency Treatment with Levetiracetam or Phenytoin in Status Epilepticus. National Institute for Health Research (NHS). NIHR HTA Reference Number: 12/127/134. Available online: http://www.nets.nihr.ac.uk/projects/hta/12127134 (accessed on 21 April 2016).
- Emergency Treatment with Levetiracetam or Phenytoin in Status Epilepticus in Children (EcLiPSE)—An Open Label Randomized Controlled Trial. National Institute for Health Research (NHS). NIHR HTA Reference number: 12/127/134. Available online: http://www.nets.nihr.ac.uk/__data/assets/pdf_file/0014/123350/PRO-12-127-134.pdf (accessed on 21 April 2016).

{kind=link}
| ILAE Definitions of Status Epilepticus | ||
| Time after which if seizures do not terminate patient is considered in status epilepticus (t1) | Time after which ongoing seizures have long term consequences (t2) | |
| Convulsive status epilepticus | 5 min | 30 min |
| Focal status epilepticus with impaired consciousness | 10 min | 60 min |
| Absence status epilepticus | 10–15 min | unknown |
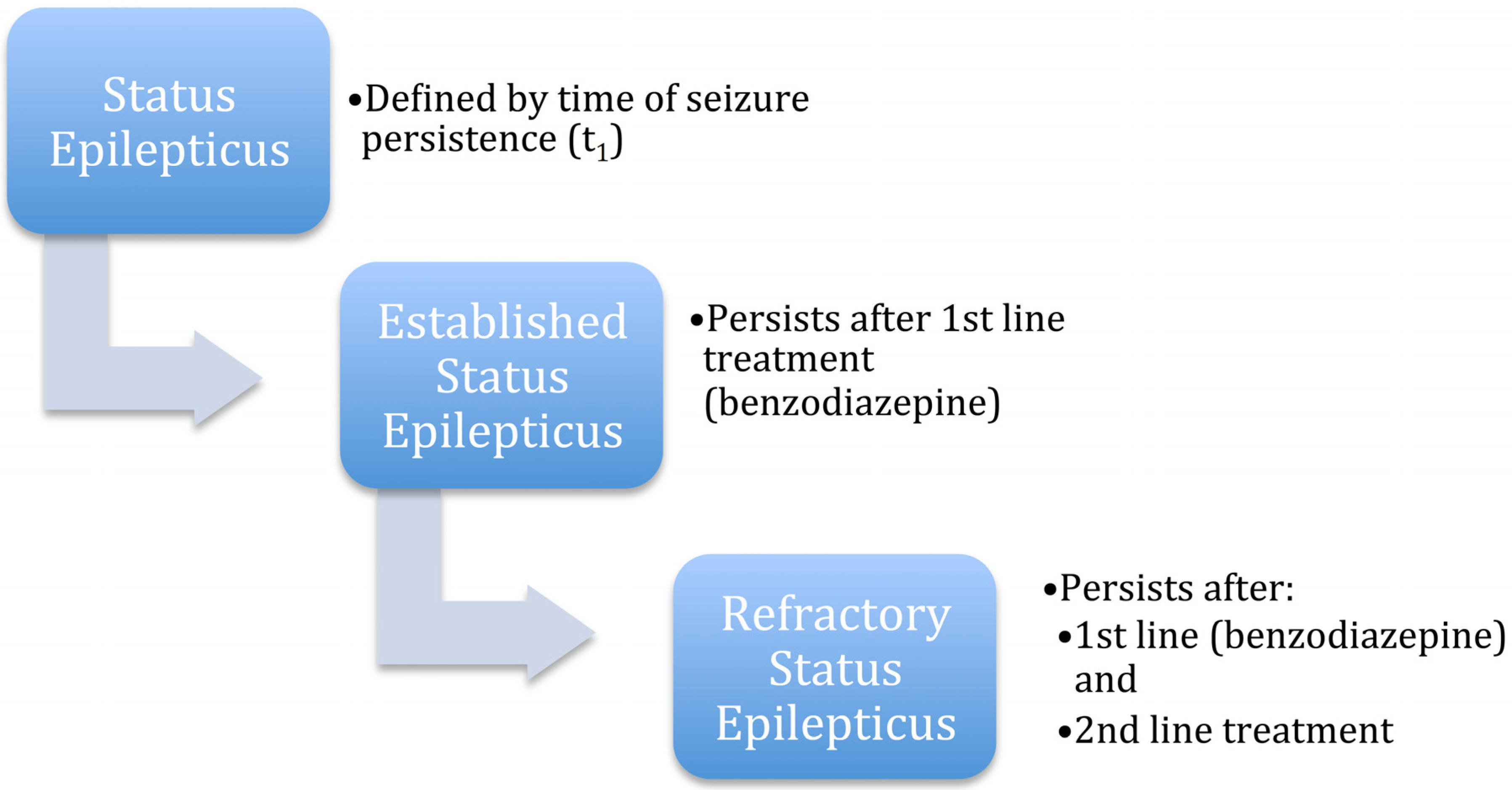
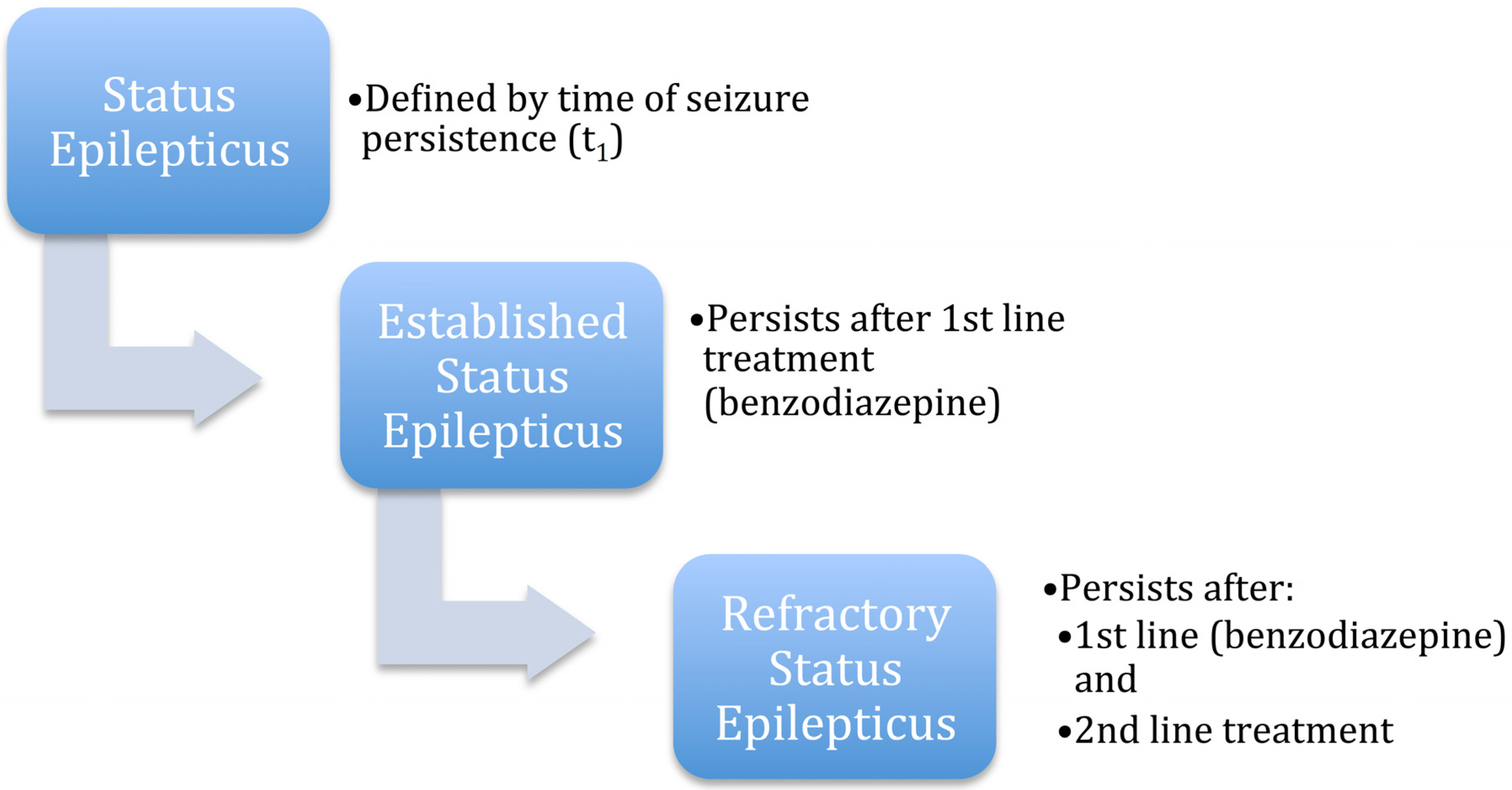
| Other Definitions of Status Epilepticus | ||
| Established statusepilepticus | Status epilepticus that persists after treatment with a benzodiazepine (1st line treatment) | |
| Refractory status epilepticus | Status epilepticus that persists after a 1st line agent (benzodiazepine) and 2nd lines | |
| agent (additional agent such as levetiracetam, phenytoin, valproic acid) have failed | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falco-Walter, J.J.; Bleck, T. Treatment of Established Status Epilepticus. J. Clin. Med. 2016, 5, 49. https://doi.org/10.3390/jcm5050049
Falco-Walter JJ, Bleck T. Treatment of Established Status Epilepticus. Journal of Clinical Medicine. 2016; 5(5):49. https://doi.org/10.3390/jcm5050049
Chicago/Turabian StyleFalco-Walter, Jessica J., and Thomas Bleck. 2016. "Treatment of Established Status Epilepticus" Journal of Clinical Medicine 5, no. 5: 49. https://doi.org/10.3390/jcm5050049
APA StyleFalco-Walter, J. J., & Bleck, T. (2016). Treatment of Established Status Epilepticus. Journal of Clinical Medicine, 5(5), 49. https://doi.org/10.3390/jcm5050049