
The Impact of Diabetes on Outcomes in Anterior Cervical Discectomy and Fusion (ACDF)
 ,
,
Abstract
1. Introduction
Research Questions
2. Methods
2.1. Dataset Acquisition
2.2. Study Period and Data Source
2.3. Patient Identification and Exclusions
2.4. Statistical Analyses and Propensity Score Matching
2.5. Comorbidity and Outcome Identification
2.6. Risk Ratio Analysis
2.7. Ethical Considerations
3. Results
3.1. Demographics and Insurance Characteristics
3.2. Comparative Analysis of Comorbidities in ACDF Patients with and Without Type II Diabetes
3.3. Propensity Score-Matched Analysis
3.4. Comparison of Hospitalization Outcomes in Propensity Score-Matched Single-Level ACDF Patients
3.5. Comparison of Select Postoperative Complications in Propensity Score-Matched Single-Level ACDF Patients
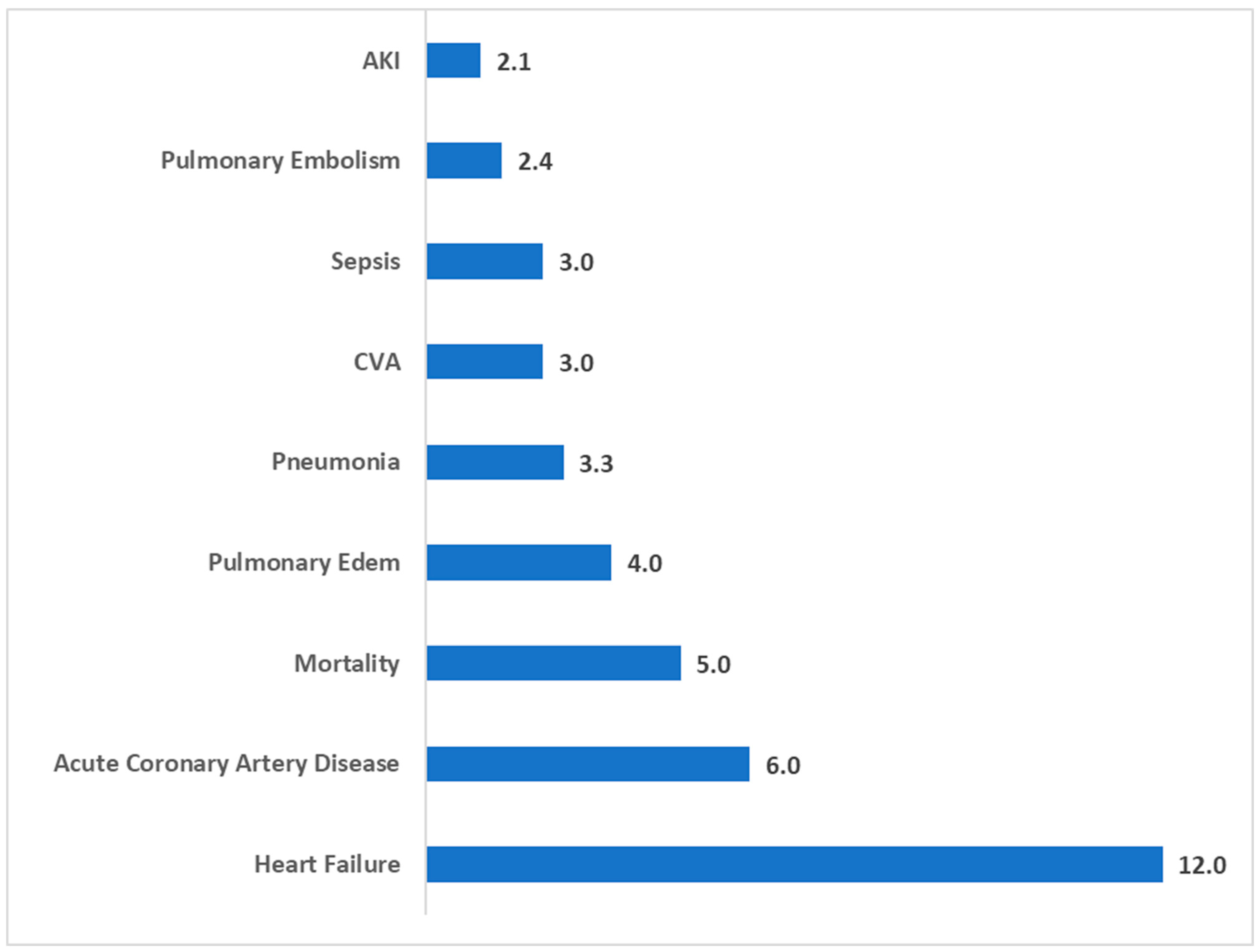
3.6. Elevated Risk Ratios for General Postoperative Complications in Single-Level ACDF Patients with Type II Diabetes
3.7. Elevated Risk Ratios for ACDF-Specific Complications in Single-Level ACDF Patients with Type II Diabetes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACDF | Anterior Cervical Discectomy and Fusion; |
| CI | Confidence Interval; |
| CSF | Cerebrospinal Fluid; |
| CVA | Cerebrovascular Accident; |
| DVT | Deep Vein Thrombosis; |
| HbA1c | Hemoglobin A1c; |
| HCUP | Healthcare Cost and Utilization Project; |
| HMO | Health Maintenance Organization; |
| ICD-10 | International Classification of Diseases, 10th Revision; |
| IDDM | Insulin-Dependent Diabetes Mellitus; |
| LOS | Length of Stay; |
| NIDDM | Non-Insulin Dependent Diabetes Mellitus; |
| NIS | Nationwide Inpatient Sample; |
| OGTT | Oral Glucose Tolerance Test; |
| PSM | Propensity Score Matching; |
| RR | Risk Ratio; |
| SPSS | Statistical Package for the Social Sciences; |
| T2DM | Type 2 Diabetes Mellitus; |
| UTI | Urinary Tract Infection; |
| WHO | World Health Organization. |
References
- Epstein, N.E. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg. Neurol. Int. 2019, 10, 100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Neifert, S.N.; Martini, M.L.; Yuk, F.; McNeill, I.T.; Caridi, J.M.; Steinberger, J.; Oermann, E.K. Predicting trends in cervical spinal surgery in the United States from 2020 to 2040. World Neurosurg. 2020, 141, e175–e181. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Cao, Q.; Wang, D.; Tan, R.; Shi, Y.; Chen, J.; Chen, R.; Tang, G.; Chen, L.; Mei, Z.; et al. The impact of diabetes on postoperative outcomes following spine surgery: A meta-analysis of 40 cohort studies with 2.9 million participants. Int. J. Surg. 2022, 104, 106789. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, T.; Bartlett, S.; Deshpande, N.; Hadi, M.; Reese, J.C.; Mansour, T.R.; Telemi, E.; Springer, K.; Schultz, L.; Nerenz, D.R.; et al. Association of prolonged symptom duration with poor outcomes in lumbar spine surgery: A Michigan Spine Surgery Improvement Collaborative study. J. Neurosurg. Spine 2023, 39, 452–461. [Google Scholar] [CrossRef]
- Gregg, E.W.; Buckley, J.; Ali, M.K.; Davies, J.; Flood, D.; Mehta, R.; Griffiths, B.; Lim, L.L.; Manne-Goehler, J.; Pearson-Stuttard, J.; et al. Improving health outcomes of people with diabetes: Target setting for the WHO Global Diabetes Compact. Lancet 2023, 401, 1302–1312. [Google Scholar] [CrossRef]
- Genuth, S.M.; Palmer, J.P.; Nathan, D.M. Classification and diagnosis of diabetes. In Diabetes in America; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2021. [Google Scholar] [PubMed]
- Michelot, M.; Lucke-Wold, B. Diabetes management in spinal surgery. J. Clin. Images Med. Case Rep. 2022, 3, 1906. [Google Scholar]
- Shuman, W.H.; Neifert, S.N.; Gal, J.S.; Snyder, D.J.; Deutsch, B.C.; Zimering, J.H.; Rothrock, R.J.; Caridi, J.M. The Impact of Diabetes on Outcomes and Health Care Costs Following Anterior Cervical Discectomy and Fusion. Glob. Spine J. 2020, 12, 780–786. [Google Scholar] [CrossRef]
- Shapiro, L.M.; Bolognesi, M.P.; Bozic, K.; Kamal, R.N. Preoperative Optimization for Orthopaedic Surgery: Steps to Reduce Complications. J. Am. Acad. Orthop. Surg. 2023, 31, e949–e960. [Google Scholar] [CrossRef]
- Karunarathna, I.; Kusumarathna, K.; Jayathilaka, P.; Rathnayake, B.; Gunathilake, S.; Senarathna, R.; Wijayawardana, K.; Priyalath, N.; Liyanapathirana, D.; Gunarathna, I.; et al. Comprehensive Management of Diabetes Mellitus in the Perioperative Setting: An Anesthesia Perspective. 2024. Available online: https://www.researchgate.net/publication/379809223_Comprehensive_Management_of_Diabetes_Mellitus_in_the_Perioperative_Setting_An_Anesthesia_Perspective (accessed on 25 April 2025).
- Goheer, H.E.; Samuel, L.T.; Flynn, A.J.; Hendrix, C.G.; Newcomb, A.H.; Carmouche, J.J. Insulin dependence negatively impacts outcomes in anterior cervical discectomy with fusions: A 10-year retrospective analysis. Spine J. Off. J. N. Am. Spine Soc. 2024, 24, 1851–1857. [Google Scholar] [CrossRef]
- Phan, K.; Kim, J.S.; Lee, N.; Kothari, P.; Cho, S.K. Impact of Insulin Dependence on Perioperative Outcomes Following Anterior Cervical Discectomy and Fusion. Spine 2017, 42, 456–464. [Google Scholar] [CrossRef]
- Mariscal, G.; Sasso, R.C.; O’Toole, J.E.; Chaput, C.D.; Steinmetz, M.P.; Arnold, P.M.; Witiw, C.D.; Jacobs, W.B.; Harrop, J.S. The economic burden of diabetes in spinal fusion surgery: A systematic review and meta-analysis. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2025, 34, 935–953. [Google Scholar] [CrossRef] [PubMed]
- Sayed, D.; Deer, T.R.; Hagedorn, J.M.; Sayed, A.; D’Souza, R.S.; Lam, C.M.; Khatri, N.; Hussaini, Z.; Pritzlaff, S.G.; Abdullah, N.M.; et al. A Systematic Guideline by the ASPN Workgroup on the Evidence, Education, and Treatment Algorithm for Painful Diabetic Neuropathy: SWEET. J. Pain Res. 2024, 17, 1461–1501. [Google Scholar] [CrossRef] [PubMed]
- Harrop, J.S.; Mohamed, B.; Bisson, E.F.; Dhall, S.; Dimar, J.; Mummaneni, P.V.; Wang, M.C.; Hoh, D.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines for Perioperative Spine: Preoperative Surgical Risk Assessment. Neurosurgery 2021, 89 (Suppl. S1), S9–S18. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, N.; Soliman, M.A.R.; Kuo, C.C.; Aguirre, A.O.; Quiceno, E.; Saleh, J.; Yeung, K.; Khan, A.; Hess, R.M.; Lim, J.; et al. The Effect of Diabetes on Complications after Spinal Fusion: A Systematic Review and Meta-Analysis. World Neurosurg. 2021, 185, e976–e994. [Google Scholar] [CrossRef]
- Cook, C.; Tackett, S.; Shah, A.; Pietrobon, R.; Browne, J.; Viens, N.; Richardson, W.; Isaacs, R. Diabetes and perioperative outcomes following cervical fusion in patients with myelopathy. Spine 2008, 33, E254–E260. [Google Scholar] [CrossRef]
- Cheng, S.W.; Wang, C.Y.; Chen, J.H.; Ko, Y. Healthcare costs and utilization of diabetes-related complications in Taiwan: A claims database analysis. Medicine 2018, 97, e11602. [Google Scholar] [CrossRef]
- American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef]
- Zhuo, X.; Zhang, P.; Kahn, H.S.; Bardenheier, B.H.; Li, R.; Gregg, E.W. Change in medical spending attributable to diabetes: National data from 1987 to 2011. Diabetes Care 2015, 38, 581–587. [Google Scholar] [CrossRef]
- Garg, R.; Schuman, B.; Bader, A.; Hurwitz, S.; Turchin, A.; Underwood, P.; Metzger, C.; Rein, R.; Lortie, M. Effect of Preoperative Diabetes Management on Glycemic Control and Clinical Outcomes After Elective Surgery. Ann. Surg. 2018, 267, 858–862. [Google Scholar] [CrossRef]
- Pai, S.L.; Haehn, D.A.; Pitruzzello, N.E.; Rao, S.N.; Meek, S.E.; Irizarry Alvarado, J.M. Reducing Infection Rates with Enhanced Preoperative Diabetes Mellitus Diagnosis and Optimization Processes. South. Med. J. 2023, 116, 215–219. [Google Scholar] [CrossRef]
- Tao, X.; Matur, A.V.; Palmisciano, P.; Conteh, F.S.; Onyewadume, L.; Duah, H.O.; Shukla, G.; Vorster, P.; Gupta, S.; Chilakapati, S.S.; et al. Preoperative HbA1c and Postoperative Outcomes in Spine Surgery: A Systematic Review and Meta-Analysis. Spine 2023, 48, 1155–1165. [Google Scholar] [CrossRef]
- Guzman, J.Z.; Skovrlj, B.; Shin, J.; Hecht, A.C.; Qureshi, S.A.; Iatridis, J.C.; Cho, S.K. The impact of diabetes mellitus on patients undergoing degenerative cervical spine surgery. Spine 2014, 39, 1656–1665. [Google Scholar] [CrossRef]
- Roth, S.G.; Chanbour, H.; Gupta, R.; O’Brien, A.; Davidson, C.; Archer, K.R.; Pennings, J.S.; Devin, C.J.; Stephens, B.F.; Abtahi, A.M.; et al. Optimal hemoglobin A1C target in diabetics undergoing elective cervical spine surgery. Spine J. Off. J. N. Am. Spine Society 2022, 22, 1149–1159. [Google Scholar] [CrossRef]
- Maman, D.; Laver, L.; Becker, R.; Mahamid, A.; Berkovich, Y. Robotic-assisted total knee arthroplasty reduces postoperative complications and length of stay without increased cost compared to navigation-guided techniques: A national analysis. Knee Surg. Sports Traumatol. Arthrosc. 2024, 323, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Laver, L.; Becker, R.; Takrori, L.A.; Mahamid, A.; Finkel, B.; Gan-Or, H.; Yonai, Y.; Berkovich, Y. Trends and epidemiology in robotic-assisted total knee arthroplasty: Reduced complications and shorter hospital stays. Knee Surg. Sports Traumatol. Arthrosc. 2024, 32, 3281–3288. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Mahamid, A.; Yonai, Y.; Berkovich, Y. Comparing Complication Rates, Costs, and Length of Stay between Unicompartmental and Total Knee Arthroplasty: Insights from a Big Data Analysis Using the National Inpatient Sample Dataset. J. Clin. Med. 2024, 13, 3888. [Google Scholar] [CrossRef] [PubMed]
- Godshaw, B.M.; Ojard, C.A.; Adams, T.M.; Chimento, G.F.; Mohammed, A.; Waddell, B.S. Preoperative glycemic control predicts perioperative serum glucose levels in patients undergoing total joint arthroplasty. J. Arthroplast. 2018, 33, S76–S80. [Google Scholar] [CrossRef]
- Han, H.S.; Kang, S.B. Relations between long-term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin. Orthop. Surg. 2013, 5, 118–123. [Google Scholar] [CrossRef]
- KhKheir, M.M.; Tan, T.L.; Kheir, M.; Maltenfort, M.G.; Chen, A.F. Postoperative Blood Glucose Levels Predict Infection After Total Joint Arthroplasty. J. Bone Jt. Surg. 2018, 100, 1423–1431. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameter | No Type 2 Diabetes | Type 2 Diabetes | Significance |
|---|---|---|---|
| Total Surgeries | 69,325 | 16,260 | - |
| Average Age (y) | 54.5 | 60.3 | p < 0.001 |
| Female (%) | 52.8 | 47.0 | p < 0.001 |
| Primary expected payer—Medicare (%) | 30.6 | 47.8 | p < 0.001 |
| Primary expected payer—Medicaid (%) | 11 | 9.5 | |
| Primary expected payer—private including HMO (%) | 46.9 | 34 | |
| Primary expected payer—self-pay (%) | 1.3 | 1 | |
| Primary expected payer—no charge (%) | 0.1 | 0.1 | |
| Primary expected payer—other (%) | 10.1 | 7.6 |
| Parameter | No Type 2 Diabetes | Type 2 Diabetes | Significance |
|---|---|---|---|
| Hypertension (%) | 38.4 | 66.3 | p < 0.001 |
| Dyslipidemia (%) | 24.1 | 55.1 | p < 0.001 |
| Obstructive Sleep Apnea (%) | 7.6 | 17.9 | p < 0.001 |
| Chronic Anemia (%) | 2.1 | 3.2 | p < 0.001 |
| Alcohol Abuse (%) | 1.2 | 1.1 | p = 0.376 |
| Osteoporosis (%) | 2.2 | 2.8 | p < 0.001 |
| Chronic Kidney Disease (%) | 2.4 | 9.6 | p < 0.001 |
| Congestive Heart Failure (%) | 0.6 | 2.2 | p < 0.001 |
| Liver Disease (%) | 0.9 | 1.9 | p < 0.001 |
| History of Myocardial Infarction (%) | 2.3 | 5.5 | p < 0.001 |
| History of Cerebrovascular Accident (%) | 3.2 | 6.9 | p < 0.001 |
| Chronic Lung Disease (%) | 7.2 | 11.2 | p < 0.001 |
| Obesity (%) | 15.6 | 30.9 | p < 0.001 |
| Fibromyalgia (%) | 3.8 | 4 | p = 0.177 |
| Parameter | No Type 2 Diabetes | Type 2 Diabetes | Significance |
|---|---|---|---|
| Total Surgeries (%) | 16,260 | 16,260 | - |
| Average Age (y) | 60.2 | 60.3 | 0.65 |
| Female (%) | 46.4 | 47.0 | p = 0.18 |
| Primary expected payer—Medicare (%) | 48 | 47.8 | p = 0.13 |
| Primary expected payer—Medicaid (%) | 8.7 | 9.5 | |
| Primary expected payer—private and HMO (%) | 35.2 | 34 | |
| Primary expected payer—self-pay (%) | 0.4 | 1 | |
| Primary expected payer—no charge (%) | 0.1 | 0.1 | |
| Primary expected payer—other (%) | 7.6 | 7.6 | |
| Hypertension (%) | 66.8 | 66.3 | p = 0.24 |
| Dyslipidemia (%) | 54.9 | 55.1 | p = 0.70 |
| Obstructive Sleep Apnea (%) | 17.1 | 17.9 | p = 0.24 |
| Chronic Anemia (%) | 2.9 | 3.2 | p = 0.43 |
| Alcohol Abuse (%) | 1.3 | 1.1 | p = 0.28 |
| Osteoporosis (%) | 2.8 | 2.8 | p = 0.87 |
| Chronic Kidney Disease (%) | 9 | 9.6 | p = 0.20 |
| Congestive Heart Failure (%) | 2 | 2.2 | p = 0.07 |
| Liver Disease (%) | 2.3 | 1.9 | p = 0.05 |
| History of Myocardial Infarction (%) | 5.6 | 5.5 | p = 0.63 |
| History of Cerebrovascular Accident (%) | 6.6 | 6.9 | p = 0.30 |
| Chronic Lung Disease (%) | 11.2 | 11.2 | p = 0.82 |
| Obesity (%) | 30.2 | 30.9 | p = 0.18 |
| Fibromyalgia (%) | 3.9 | 4 | p = 0.63 |
| No Type 2 Diabetes | Type 2 Diabetes | Significance | |
|---|---|---|---|
| Length of stay, mean, in days | 1.79 (Std. deviation 2.3) | 1.99 (Std. deviation 2.6) | p < 0.001 |
| Total charges, mean, in USD | 67,998 (Std. deviation 56191) | 71,884 (Std. deviation 55528) | p = 0.004 |
| Parameter | No Type 2 Diabetes | Type 2 Diabetes | Significance |
|---|---|---|---|
| DVT (%) | 0.1 | 0.1 | p = 0.157 |
| Blood Loss Anemia (%) | 20.1 | 20.5 | p = 0.357 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maman, D.; Mahamid, A.; Nisanov, G.; Fagbamila, O.; Sleiman, A.; Shpigelman, A.; Berkovich, Y. The Impact of Diabetes on Outcomes in Anterior Cervical Discectomy and Fusion (ACDF). J. Clin. Med. 2025, 14, 3039. https://doi.org/10.3390/jcm14093039
Maman D, Mahamid A, Nisanov G, Fagbamila O, Sleiman A, Shpigelman A, Berkovich Y. The Impact of Diabetes on Outcomes in Anterior Cervical Discectomy and Fusion (ACDF). Journal of Clinical Medicine. 2025; 14(9):3039. https://doi.org/10.3390/jcm14093039
Chicago/Turabian StyleMaman, David, Assil Mahamid, Gabriel Nisanov, Oluwaseun Fagbamila, Ali Sleiman, Arsen Shpigelman, and Yaron Berkovich. 2025. "The Impact of Diabetes on Outcomes in Anterior Cervical Discectomy and Fusion (ACDF)" Journal of Clinical Medicine 14, no. 9: 3039. https://doi.org/10.3390/jcm14093039
APA StyleMaman, D., Mahamid, A., Nisanov, G., Fagbamila, O., Sleiman, A., Shpigelman, A., & Berkovich, Y. (2025). The Impact of Diabetes on Outcomes in Anterior Cervical Discectomy and Fusion (ACDF). Journal of Clinical Medicine, 14(9), 3039. https://doi.org/10.3390/jcm14093039