
The RESCUE Technique: A Mnemonic Acronym to Enhance Outcomes in Nail Fixation of Extracapsular Hip Fractures

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
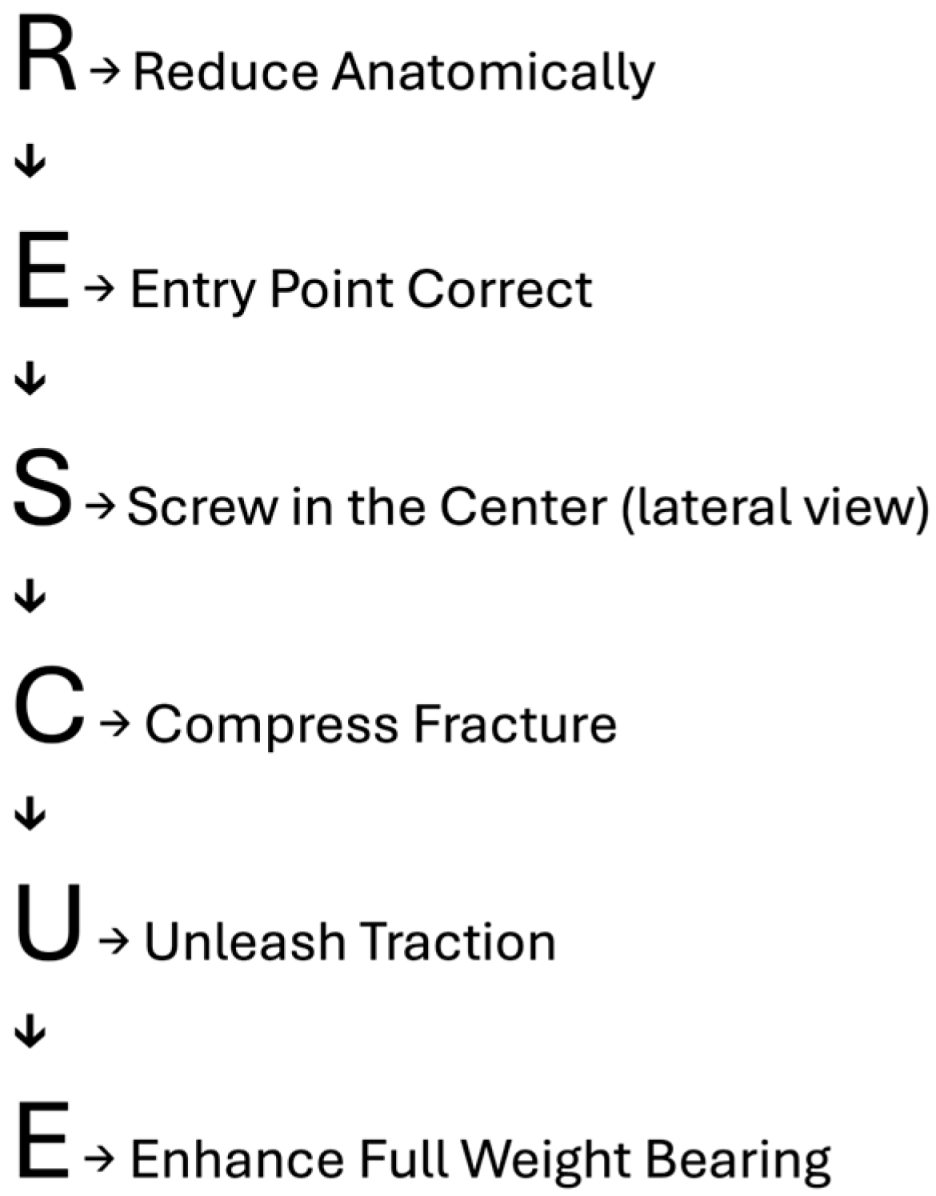
2. Introduction of the RESCUE Technique
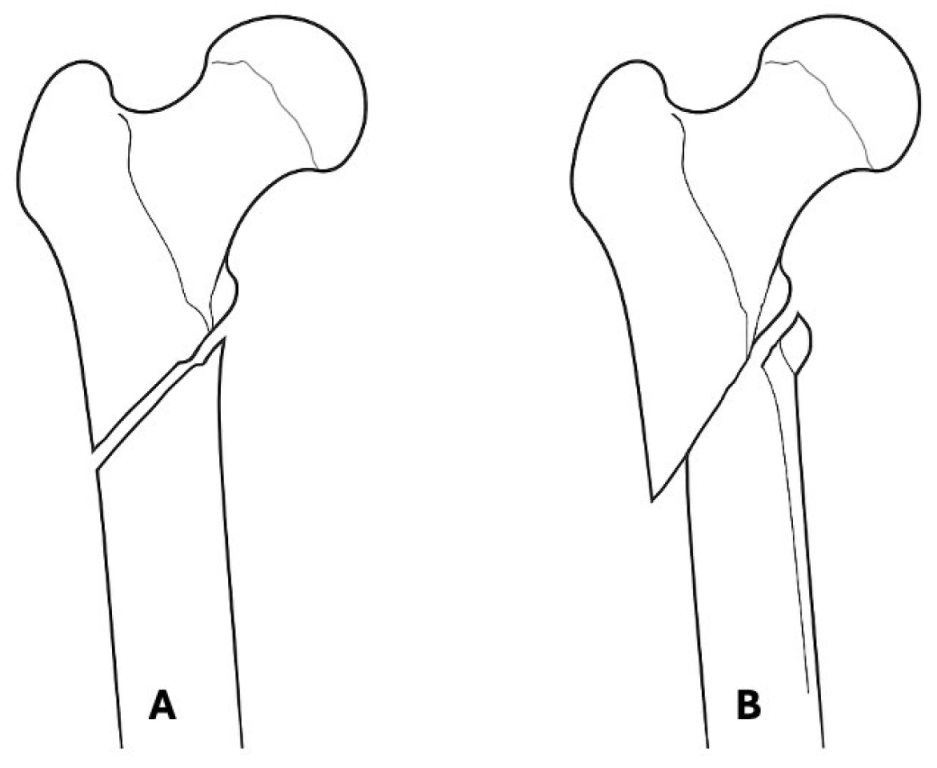
2.1. R—Reduce Anatomically
2.2. E—Entry Point Correct
2.3. S—Screw in Center (Lateral View)
2.4. C—Compress Fracture
2.5. U—Unleash Traction
2.6. E—Enhance Full-Weight Bearing
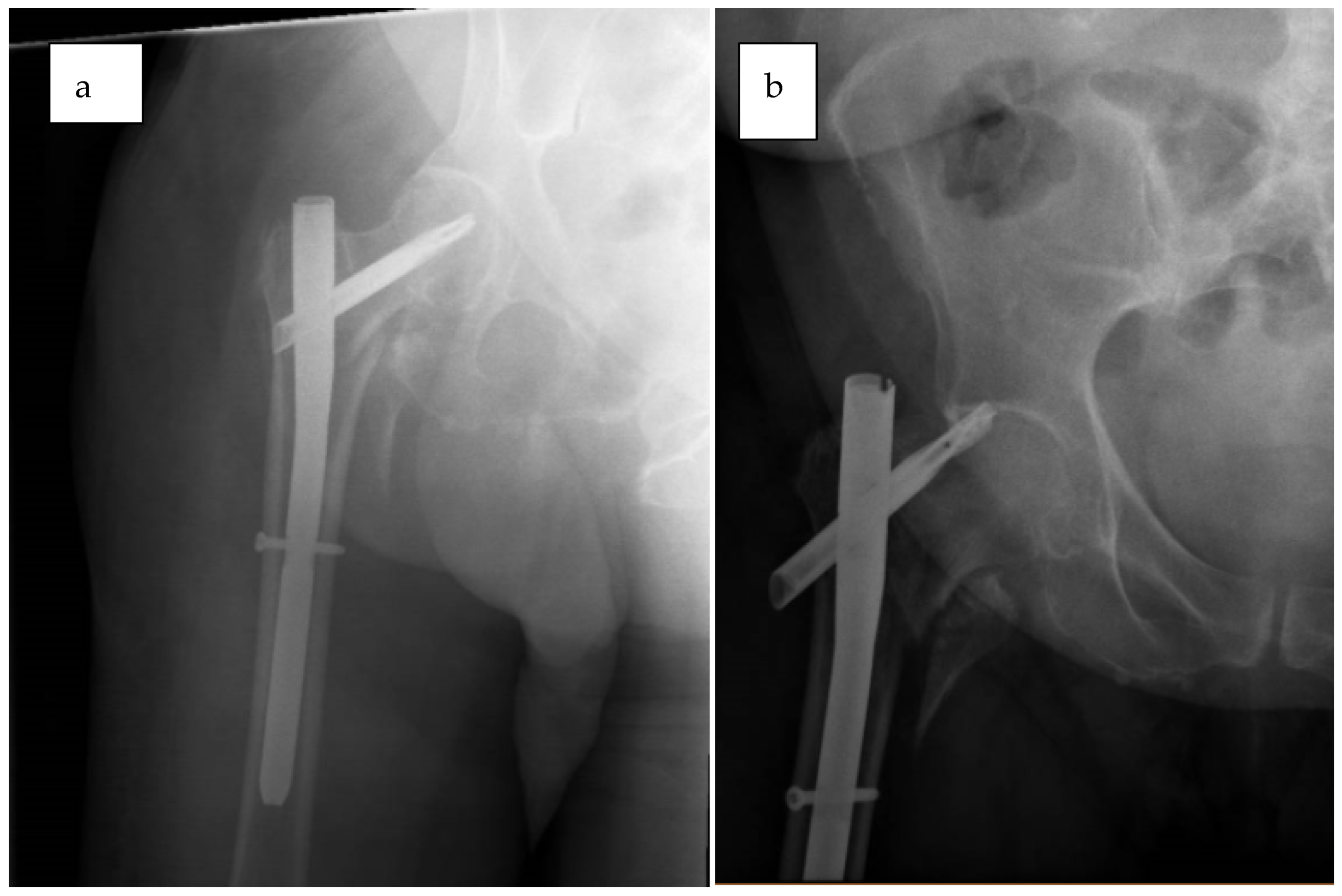
2.7. Case Examples
2.7.1. Case 1—Failure to Reduce Anatomically
2.7.2. Case 2—Unable to Unleash Traction
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamanaka, T.; Matsumura, T.; Ae, R.; Takeshita, K. AO/OTA 31A3 fractures and postoperative complications in older patients. J. Orthop. Sci. 2024, 29, 1073–1077. [Google Scholar] [CrossRef]
- Valen, A.K.; Viberg, B.; Gundtoft, P.H.; Wæver, D.; Thorninger, R. Mortality in patients with trochanteric hip fractures (AO/OTA 31-A) treated with sliding hip screw versus intramedullary nail: A retrospective national registry study of 9547 patients from the Danish Fracture Database. Injury 2023, 54, 1721–1726. [Google Scholar] [CrossRef]
- Haidukewych, G.J. Intertrochanteric Fractures: Ten Tips to Improve Results. J. Bone Joint Surg. Am. 2009, 91, 712–719. [Google Scholar]
- Ito, K.; Hungerbühler, R.; Wahl, D.; Grass, R. Improved intramedullary nail interlocking in osteoporotic bone. J. Orthop. Trauma 2001, 15, 192–196. [Google Scholar] [CrossRef]
- Zhou, X.; Shen, X. A Comparative Study of Hip Arthroplasty and Closed Reduction Proximal Femur Nail in the Treatment of Elderly Patients with Hip Fractures. Front. Surg. 2022, 9, 904928. [Google Scholar] [CrossRef]
- Agarwal, N.; Feng, T.; Maclullich, A.; Duckworth, A.; Clement, N. Early mobilisation after hip fracture surgery is associated with improved patient outcomes: A systematic review and meta-analysis. Musculoskelet. Care 2024, 22, e1863. [Google Scholar] [CrossRef]
- Al-Dahan, T.; Murhekar, S.; Patel, N. Treatment Outcomes of Dynamic Hip Screws Versus Short Intramedullary Nails for Extra-capsular Fragility Hip Fractures and Their Coding Audit. Cureus 2024, 16, e68617. [Google Scholar] [CrossRef]
- Lewis, S.R.; Macey, R.; Gill, J.R.; Parker, M.J.; Griffin, X.L. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database Syst. Rev. 2022, 1, CD000093. [Google Scholar] [CrossRef]
- Queally, J.M.; Harris, E.; Handoll, H.H.G.; Parker, M.J. Intramedullary nails for extracapsular hip fractures in adults. Cochrane Database Syst. Rev. 2014, 2014, CD004961. [Google Scholar] [CrossRef]
- Liu, W.; Zhou, D.; Liu, F.; Weaver, M.J.; Vrahas, M.S. Mechanical complications of intertrochanteric hip fractures treated with trochanteric femoral nails. J. Trauma Acute Care Surg. 2013, 75, 304–310. [Google Scholar] [CrossRef]
- Li, J.; Zhang, L.; Zhang, H.; Yin, P.; Lei, M.; Wang, G.; Wang, S.; Tang, P. Effect of reduction quality on post-operative outcomes in 31-A2 intertrochanteric fractures following intramedullary fixation: A retrospective study based on computerised tomography findings. Int. Orthop. 2018, 43, 1951. [Google Scholar] [CrossRef] [PubMed]
- Bojan, A.J.; Beimel, C.; Taglang, G.; Collin, D.; Ekholm, C.; Jönsson, A. Critical factors in cut-out complication after Gamma Nail treatment of proximal femoral fractures. BMC Musculoskel. Disord. 2013, 14, 1. [Google Scholar] [CrossRef]
- Chang, S.M.; Zhang, Y.Q.; Ma, Z.; Li, Q.; Dargel, J.; Eysel, P. Fracture reduction with positive medial cortical support: A key element in stability reconstruction for the unstable pertrochanteric hip fractures. Arch. Orthop. Trauma Surg. 2015, 135, 811. [Google Scholar] [CrossRef]
- Shasho, M.; Al-Jawad, M.; Kudsi, M.A.; Khaiata, H.; Aswad, A.; Iskandar, Y. The effect of nonanatomic positive medial cortical support on the reduction stability of unstable pertrochanteric proximal femur fractures: A cohort study. Medicine 2025, 104, e42498. [Google Scholar] [CrossRef] [PubMed]
- Horoz, L.; Kilic, A.I.; Kircil, C.; Cakmak, M.F. Flexible reamer use to overcome entry point errors in proximal femoral nail application in severe obese intertrochanteric fracture patients. BMC Musculoskel. Disord. 2024, 25, 810. [Google Scholar] [CrossRef]
- Aygün, Ü.; Şenocak, E.; Aksay, M.F.; Çiçek, A.C.; Halaç, O.; Toy, S. An overview of patients with intertrochanteric femoral fractures treated with proximal femoral nail fixation using important criteria. BMC Musculoskel. Disord. 2024, 25, 1051. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertner, M.R.; Curtin, S.L.; Lindskog, D.M.; Keggi, J.M. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J. Bone Jt. Surg. Am. 1995, 77, 1058–1064. [Google Scholar] [CrossRef]
- Yang, Y.F.; Huang, J.W.; Gao, X.S. CalTAD is the Key Evaluation Tool for Measurement of Cephalic Fixation Position for Predicting Cut-Out in Geriatric Intertrochanteric Fracture Patients with Internal Fixations after Achieving Acceptable Reduction. Geriatr. Orthop. Surg. Rehabil. 2022, 13, 21514593221083820. [Google Scholar] [CrossRef]
- Caruso, G.; Corradi, N.; Caldaria, A.; Bottin, D.; Re, D.L.; Lorusso, V.; Morotti, C.; Valpiani, G.; Massari, L. New tip-apex distance and calcar-referenced tip-apex distance cut-offs may be the best predictors for cut-out risk after intramedullary fixation of proximal femur fractures. Sci. Rep. 2022, 12, 357. [Google Scholar] [CrossRef]
- Petfield, J.L.; Visscher, L.E.; Gueorguiev, B.; Stoffel, K.; Pape, H.-C. Tips and tricks to avoid implant failure in proximal femur fractures treated with cephalomedullary nails: A review of the literature. OTA Int. 2022, 5, e191. [Google Scholar] [CrossRef]
- Lin, D.; Zhu, F.; Chen, P.; Lin, C.; Chen, B.; Zheng, K.; Zheng, S.; Lin, F. Pre-sliding of the femoral neck system to prevent postoperative shortening of femoral neck fractures. Heliyon 2024, 10, e29187. [Google Scholar] [CrossRef] [PubMed]
- Nherera, L.; Trueman, P.; Horner, A.; Watson, T.; Johnstone, A.J. In reply to the letter to the editor regarding “Comparison of a twin interlocking derotation and compression screw cephalomedullary nail (InterTAN) with a single screw derotation cephalomedullary nail (proximal femoral nail antirotation): A systematic review and meta-analysis for intertrochanteric fractures”. J. Orthop. Surg. Res. 2022, 17, 354. [Google Scholar] [CrossRef] [PubMed]
- Lobo-Escolar, A.; Joven, E.; Iglesias, D.; Herrera, A. Predictive factors for cutting-out in femoral intramedullary nailing. Injury 2010, 41, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.M.; Hou, Z.Y.; Hu, S.J.; Du, S.-C. Intertrochanteric Femur Fracture Treatment in Asia: What We Know and What the World Can Learn. Orthop. Clin. N. Am. 2020, 51, 189–205. [Google Scholar] [CrossRef]
- Song, H.; Chang, S.M.; Hu, S.J.; Du, S.-C.; Xiong, W.-F. Calcar fracture gapping: A reliable predictor of anteromedial cortical support failure after cephalomedullary nailing for pertrochanteric femur fractures. BMC Musculoskel. Disord. 2022, 23, 175. [Google Scholar] [CrossRef]
- Shivashankar, B.; Keshkar, S. Intertrochanteric Fractures: Ten Commandments for How to Get Good Results with Proximal Femoral Nailing. Indian J. Orthop. 2021, 55, 521–524. [Google Scholar] [CrossRef]
- Mereddy, P.; Kamath, S.; Ramakrishnan, M.; Malik, H.; Donnachie, N. The AO/ASIF proximal femoral nail antirotation (PFNA): A new design for the treatment of unstable proximal femoral fractures. Injury 2009, 40, 428–432. [Google Scholar] [CrossRef]
- Sircar, P.; Godkar, D.; Mahgerefteh, S.; Chambers, K.; Niranjan, S.; Cucco, R. Morbidity and mortality among patients with hip fractures surgically repaired within and after 48 hours. Am. J. Ther. 2007, 14, 508–513. [Google Scholar] [CrossRef]
- Li, N.; Cheng, K.Y.; Zhang, J.; Liu, G.; Zhou, L.; Zhu, S.-W.; Yang, M.-H.; Wu, X.-B.; Jiang, X.-Y. Immediate weight bearing as tolerated versus delayed weight bearing following intramedullary fixation for geriatric intertrochanteric fractures: A post hoc analysis. BMC Musculoskel. Disord. 2024, 25, 1041. [Google Scholar] [CrossRef]
- Yam, M.; Chawla, A.; Kwek, E. Rewriting the tip apex distance for the proximal femoral nail anti-rotation. Injury 2017, 48, 1843–1847. [Google Scholar] [CrossRef]
- Kashigar, A.; Vincent, A.; Gunton, M.J.; Backstein, D.; Safir, O.; Kuzyk, P.R.T. Predictors of failure for cephalomedullary nailing of proximal femoral fractures. Bone Joint J. 2014, 96-B, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, K.K.; Fang, C.K.; Chen, C.M.; Su, Y.-P.; Wu, H.-F.; Chiu, F.-Y. Risk factors in cutout of sliding hip screw in intertrochanteric fractures: An evaluation of 937 patients. Int. Orthop. 2010, 34, 1273–1276. [Google Scholar] [CrossRef] [PubMed]
- Güven, M.; Yavuz, U.; Kadioǧlu, B.; Akman, B.; Kilinçoğlu, V.; Unay, K.; Altintaş, F. Importance of screw position in intertrochanteric femoral fractures treated by dynamic hip screw. Orthop. Traumatol. Surg. Res. 2010, 96, 33–34. [Google Scholar] [CrossRef]
- Turgut, A.; Kalenderer, Ö.; Karapınar, L.; Kumbaracı, M.; Akkan, H.A.; Ağuş, H. Which factor is most important for occurrence of cutout complications in patients treated with proximal femoral nail antirotation? Retrospective analysis of 298 patients. Arch. Orthop. Trauma Surg. 2016, 136, 623–630. [Google Scholar] [CrossRef]
- Zhang, G.; Li, J.; Li, J.; Zhou, X.; Xie, J.; Wang, A. Selective Laser Melting Molding of Individualized Femur Implant: Design, Process, Optimization. J. Bionic. Eng. 2021, 18, 128–137. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolaides, A.P.; Abesamis, J.B.; Hamed, A.; Sarofeen, S.; Vetharajan, N.; Sahemey, R.; Salar, O.; Konstantinou, P. The RESCUE Technique: A Mnemonic Acronym to Enhance Outcomes in Nail Fixation of Extracapsular Hip Fractures. J. Clin. Med. 2025, 14, 5419. https://doi.org/10.3390/jcm14155419
Nikolaides AP, Abesamis JB, Hamed A, Sarofeen S, Vetharajan N, Sahemey R, Salar O, Konstantinou P. The RESCUE Technique: A Mnemonic Acronym to Enhance Outcomes in Nail Fixation of Extracapsular Hip Fractures. Journal of Clinical Medicine. 2025; 14(15):5419. https://doi.org/10.3390/jcm14155419
Chicago/Turabian StyleNikolaides, Anastasios P., Julius Bryan Abesamis, Ahmed Hamed, Samer Sarofeen, Niraj Vetharajan, Rajpreet Sahemey, Omer Salar, and Panagiotis Konstantinou. 2025. "The RESCUE Technique: A Mnemonic Acronym to Enhance Outcomes in Nail Fixation of Extracapsular Hip Fractures" Journal of Clinical Medicine 14, no. 15: 5419. https://doi.org/10.3390/jcm14155419
APA StyleNikolaides, A. P., Abesamis, J. B., Hamed, A., Sarofeen, S., Vetharajan, N., Sahemey, R., Salar, O., & Konstantinou, P. (2025). The RESCUE Technique: A Mnemonic Acronym to Enhance Outcomes in Nail Fixation of Extracapsular Hip Fractures. Journal of Clinical Medicine, 14(15), 5419. https://doi.org/10.3390/jcm14155419