
Impact of Acute Kidney Injury on Mortality Outcomes in Patients Hospitalized for COPD Exacerbation: A National Inpatient Sample Analysis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographical Data
3.1.1. Baseline Demographics
3.1.2. Mortality and Inpatient Complication Demographics
3.1.3. Comorbidity Distribution
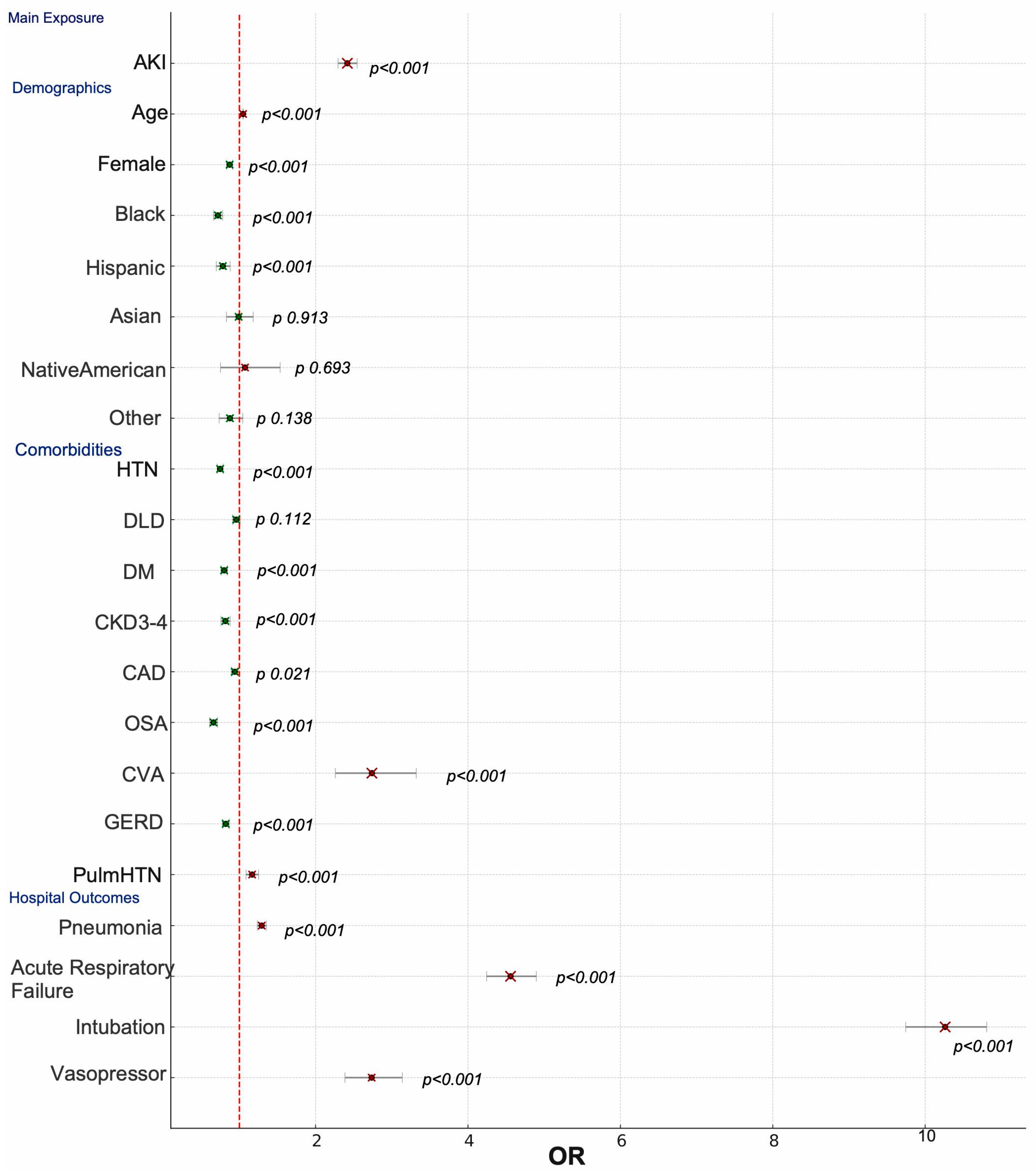
3.2. Multivariate Analysis Data
3.2.1. Demographic Risk Factors and Mortality
3.2.2. Hospital Complications and Mortality
3.2.3. Comorbidities and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AKI | Acute Kidney Injury |
| COPD | Chronic Obstructive Pulmonary Disease |
| COPDe | COPD Exacerbation |
| NIS | National Inpatient Sample |
| HCUP | Healthcare Cost and Utilization Project |
| LOS | Length of Stay |
| HTN | Hypertension |
| DLD | Dyslipidemia |
| DM | Diabetes Mellitus |
| CKD3–4 | Chronic Kidney Disease Stage 3 to 4 |
| CAD | Coronary Artery Disease |
| OSA | Obstructive Sleep Apnea |
| CVD | Cerebrovascular Disease |
| GERD | Gastroesophageal Reflux Disease |
| Pulm HTN | Pulmonary Hypertension |
| OR | Odds Ratio |
| CI | Confidence Interval |
| ESKD | End-Stage Kidney Disease |
| RRT | Renal Replacement Therapy |
| UTI | Urinary Tract Infection |
| KDIGO | Kidney Disease Improving Global Outcomes |
References
- Rodriguez-Roisin, R. Toward a consensus definition for COPD exacerbations. Chest 2000, 117, 398S–401S. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.cdc.gov/nchs/fastats/copd.htm (accessed on 26 February 2025).
- Press, V.G.; Myers, L.C.; Feemster, L.C. Preventing COPD readmissions under the Hospital Readmissions Reduction Program: How far have we come? Chest 2021, 159, 996–1006. [Google Scholar] [CrossRef]
- Goyal, A.; Daneshpajouhnejad, P.; Hashmi, M.F.; Bashir, K. Acute Kidney Injury. [Updated 25 November 2023]; In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441896/ (accessed on 8 January 2025).
- Fabbian, F.; De Giorgi, A.; Manfredini, F.; Lamberti, N.; Forcellini, S.; Storari, A.; Gallerani, M.; Caramori, G.; Manfredini, R. Impact of renal dysfunction on in-hospital mortality of patients with severe chronic obstructive pulmonary disease: A single-center Italian study. Int. Urol. Nephrol. 2016, 48, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Rifkin, D.E.; Blantz, R.C. Chronic kidney disease: An inherent risk factor for acute kidney injury? Clin. J. Am. Soc. Nephrol. 2010, 5, 1690–1695. [Google Scholar] [CrossRef]
- Wan, X.; Chen, D.; Tan, Y.; Ma, M.; Zhang, F.; Liu, Z.; Chen, Y.; Shao, W.; Cao, C. Incidence, risk factors, and prognostic implications of acute kidney injury in patients with acute exacerbation of COPD. Int. J. Chron. Obstr. Pulm. Dis. 2020, 15, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Jiang, L.; Li, J.; Tan, Y.; Ma, M.; Cao, C.; Zhao, J.; Wan, X. Interaction of acute respiratory failure and acute kidney injury on in-hospital mortality of patients with acute exacerbation COPD. Int. J. Chron. Obstr. Pulm. Dis. 2021, 16, 3309–3316. [Google Scholar] [CrossRef] [PubMed]
- Barakat, M.F.; McDonald, H.I.; Collier, T.J.; Smeeth, L.; Nitsch, D.; Quint, J.K. Acute kidney injury in stable COPD and at exacerbation. Int. J. Chron. Obstr. Pulm. Dis. 2015, 10, 2067–2077. [Google Scholar] [CrossRef]
- Grams, M.E.; Matsushita, K.; Sang, Y.; Estrella, M.M.; Foster, M.C.; Tin, A.; Kao, W.L.; Coresh, J. Explaining the racial difference in AKI incidence. J. Am. Soc. Nephrol. 2014, 25, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Kwok, W.C.; Tam, T.C.; Ho, J.C.; Lam, D.C.; Ip, M.S.; Yap, D.Y. Hospitalized acute exacerbation in chronic obstructive pulmonary disease—Impact on long-term renal outcomes. Respir. Res. 2024, 25, 36. [Google Scholar] [CrossRef] [PubMed]
- Hsu, R.K.; Hsu, C.Y. The role of acute kidney injury in chronic kidney disease. Semin. Nephrol. 2016, 36, 283–292. [Google Scholar] [CrossRef]
- Marcy, F.; Goettfried, K.; Enghard, P.; Piper, S.K.; Kunz, J.V.; Schroeder, T. Impact of AKI on metabolic compensation for respiratory acidosis in ICU patients with AECOPD. J. Crit. Care 2024, 83, 154846. [Google Scholar] [CrossRef]
- Zhang, D. Correlation analysis of early renal injury in elderly patients with acute exacerbations of chronic obstructive pulmonary disease. Int. J. Chron. Obstr. Pulm. Dis. 2022, 17, 2109–2115. [Google Scholar] [CrossRef]
- Liu, Z.; Ma, Z.; Ding, C. Association between COPD and CKD: A systematic review and meta-analysis. Front. Public Health 2024, 12, 1494291. [Google Scholar] [CrossRef] [PubMed]
- Faubel, S.; Edelstein, C.L. Mechanisms and mediators of lung injury after acute kidney injury. Nat. Rev. Nephrol. 2016, 12, 48–60. [Google Scholar] [CrossRef]
- Legrand, M.; Rossignol, P. Cardiovascular consequences of acute kidney injury. N. Engl. J. Med. 2020, 382, 2238–2247. [Google Scholar] [CrossRef]
- Vieira, J.M., Jr.; Castro, I.; Curvello-Neto, A.; Demarzo, S.; Caruso, P.; Pastore, L., Jr.; Imanishe, M.H.; Abdulkader, R.C.; Deheinzelin, D. Effect of acute kidney injury on weaning from mechanical ventilation in critically ill patients. Crit. Care Med. 2007, 35, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Modi, K.; Padala, S.A.; Gupta, M. Contrast-Induced Nephropathy. [Updated 4 January 2025]; In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK448066/ (accessed on 20 January 2025).
- Albeladi, F.I.; Salem, I.M.W.; Bugshan, S.A.; Alghamdi, A.A. Acute kidney injury as a risk factor for cerebrovascular disease outcome among patients presenting with stroke. Saudi J. Kidney Dis. Transpl. 2021, 32, 60–68. [Google Scholar] [CrossRef]
- Sirnes, P.A.; Tendera, M.; Vardas, P.; Widimsky, P. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2009, 30, 2493–2537. [Google Scholar] [CrossRef]
- Nickel, N.P.; O’leary, J.M.; Brittain, E.L.; Fessel, J.P.; Zamanian, R.T.; West, J.D.; Austin, E.D. Kidney dysfunction in patients with pulmonary arterial hypertension. Pulm. Circ. 2017, 7, 38–54. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xie, Z.; Xiong, S.; Xiong, W.; Zhong, T.; Su, Y. Acute kidney injury in hospitalized patients with nonexacerbated chronic obstructive pulmonary disease. BMC Pulm. Med. 2020, 20, 108. [Google Scholar] [CrossRef]
- Cardoso, R.; Graffunder, F.P.; Ternes, C.M.; Fernandes, A.; Rocha, A.V.; Fernandes, G.; Bhatt, D.L. SGLT2 inhibitors decrease cardiovascular death and heart failure hospitalizations in patients with heart failure: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100933. [Google Scholar] [CrossRef] [PubMed]
- Van Vark, L.C.; Bertrand, M.; Akkerhuis, K.M.; Brugts, J.J.; Fox, K.; Mourad, J.J.; Boersma, E. Angiotensin-converting enzyme inhibitors reduce mortality in hypertension: A meta-analysis. Eur. Heart J. 2012, 33, 2088–2097. [Google Scholar] [CrossRef]
- Kabarriti, R.; Brodin, N.P.; Maron, M.I.; Guha, C.; Kalnicki, S.; Garg, M.K.; Racine, A.D. Association of race and ethnicity with comorbidities and survival among patients with COVID-19. JAMA Netw. Open 2020, 3, e2019795. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable * | With AKI (n = 55,270) | Without AKI (n = 350,575) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 72.69 (±10.29) | 69.55 (±10.84) | 0.01 ** |
| LOS, mean (SD) | 6.12 (±5.40) | 4.58 (±3.98) | 0.015 *** |
| Female, n (%) | 24,306 (44.0%) | 190,102 (54.2%) | <0.001 **** |
| Race, n (%) | <0.001 **** | ||
| White | 41,523 (76.9%) | 275,654 (80.5%) | |
| Black | 7515 (13.9%) | 38,915 (11.4%) | |
| Hispanic | 2880 (5.3%) | 16,399 (4.8%) | |
| Asian | 897 (1.7%) | 4082 (1.2%) | |
| Native American | 232 (0.4%) | 1554 (0.5%) | |
| Other | 981 (1.8%) | 5894 (1.7%) | |
| Comorbidities, n (%) | |||
| HTN | 46,596 (84.3%) | 253,850 (72.4%) | <0.001 **** |
| DLD | 20,164 (36.5%) | 103,124 (29.4%) | <0.001 **** |
| DM | 22,274 (40.3%) | 100,466 (28.7%) | <0.001 **** |
| CKD3–4 | 17,129 (31.0%) | 24,920 (7.1%) | <0.001 **** |
| CAD | 19,329 (35.0%) | 97,045 (27.7%) | <0.001 **** |
| OSA | 9191 (16.6%) | 48,413 (13.8%) | <0.001 **** |
| CVD | 412 (0.7%) | 1314 (0.4%) | <0.001 **** |
| GERD | 14,965 (27.1%) | 100,214 (28.6%) | <0.001 **** |
| Pulm HTN | 6143 (11.1%) | 28,861 (8.2%) | <0.001 **** |
| Hospital outcomes, n (%) | |||
| Pneumonia | 23,326 (42.2%) | 124,112 (35.4%) | <0.001 **** |
| Acute respiratory failure | 32,268 (58.4%) | 181,124 (51.7%) | <0.001 **** |
| Intubation | 5918 (10.7%) | 13,837 (3.9%) | <0.001 **** |
| Vasopressor support | 651 (1.2%) | 744 (0.2%) | <0.001 **** |
| Inpatient mortality | 3213 (5.8%) | 5728 (1.6%) | <0.001 **** |
| Variable * | OR | 95% CI (Lower) | 95% CI (Upper) | p-Value |
|---|---|---|---|---|
| AKI | 2.417 | 2.295 | 2.545 | <0.001 |
| Age | 1.049 | 1.046 | 1.051 | <0.001 |
| Female | 0.872 | 0.833 | 0.913 | <0.001 |
| Race (White = reference) | ||||
| Black | 0.718 | 0.66 | 0.781 | <0.001 |
| Hispanic | 0.783 | 0.697 | 0.879 | <0.001 |
| Asian | 0.99 | 0.83 | 1.181 | 0.913 |
| Native American | 1.074 | 0.752 | 1.535 | 0.693 |
| Other | 0.876 | 0.735 | 1.044 | 0.138 |
| Comorbidities | ||||
| HTN | 0.747 | 0.709 | 0.787 | <0.001 |
| DLD | 0.959 | 0.911 | 1.01 | 0.112 |
| DM | 0.8 | 0.758 | 0.844 | <0.001 |
| CKD3–4 | 0.816 | 0.758 | 0.879 | <0.001 |
| CAD | 0.94 | 0.893 | 0.991 | 0.021 |
| OSA | 0.66 | 0.61 | 0.714 | <0.001 |
| CVD | 2.739 | 2.259 | 3.321 | <0.001 |
| GERD | 0.821 | 0.778 | 0.867 | <0.001 |
| Pulm HTN | 1.167 | 1.088 | 1.252 | <0.001 |
| Hospital outcomes | ||||
| Pneumonia | 1.293 | 1.236 | 1.354 | <0.001 |
| Acute respiratory failure | 4.559 | 4.245 | 4.897 | <0.001 |
| Intubation | 10.262 | 9.744 | 10.808 | <0.001 |
| Vasopressor | 2.736 | 2.385 | 3.138 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morcos, Z.; Daniel, R.; Hassan, M.; Qandil, H.; Lahoud, C.; Wei, C.; El Sayegh, S. Impact of Acute Kidney Injury on Mortality Outcomes in Patients Hospitalized for COPD Exacerbation: A National Inpatient Sample Analysis. J. Clin. Med. 2025, 14, 5393. https://doi.org/10.3390/jcm14155393
Morcos Z, Daniel R, Hassan M, Qandil H, Lahoud C, Wei C, El Sayegh S. Impact of Acute Kidney Injury on Mortality Outcomes in Patients Hospitalized for COPD Exacerbation: A National Inpatient Sample Analysis. Journal of Clinical Medicine. 2025; 14(15):5393. https://doi.org/10.3390/jcm14155393
Chicago/Turabian StyleMorcos, Zeina, Rachel Daniel, Mazen Hassan, Hamza Qandil, Chloe Lahoud, Chapman Wei, and Suzanne El Sayegh. 2025. "Impact of Acute Kidney Injury on Mortality Outcomes in Patients Hospitalized for COPD Exacerbation: A National Inpatient Sample Analysis" Journal of Clinical Medicine 14, no. 15: 5393. https://doi.org/10.3390/jcm14155393
APA StyleMorcos, Z., Daniel, R., Hassan, M., Qandil, H., Lahoud, C., Wei, C., & El Sayegh, S. (2025). Impact of Acute Kidney Injury on Mortality Outcomes in Patients Hospitalized for COPD Exacerbation: A National Inpatient Sample Analysis. Journal of Clinical Medicine, 14(15), 5393. https://doi.org/10.3390/jcm14155393