
Clinical Application of rhBMP-2 and Three-Dimensinal Preformed Titanium Mesh with Allograft and Xenograft for Peri-Implant Horizontal and Vertical Bone Augmentation–A Narrative Review with Technical Report


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
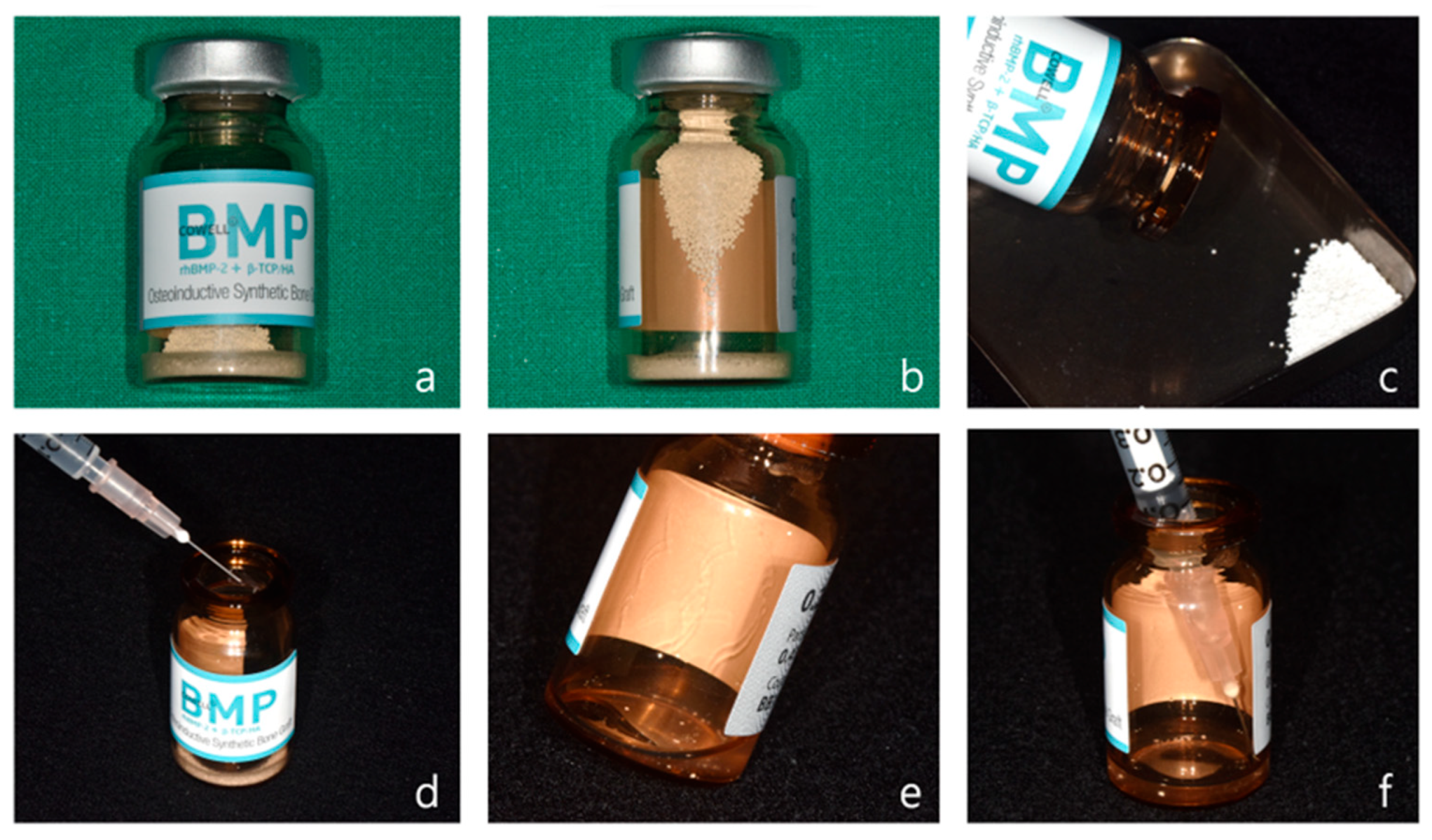
2.1. Preparation of Bone Graft Material with rhBMP-2
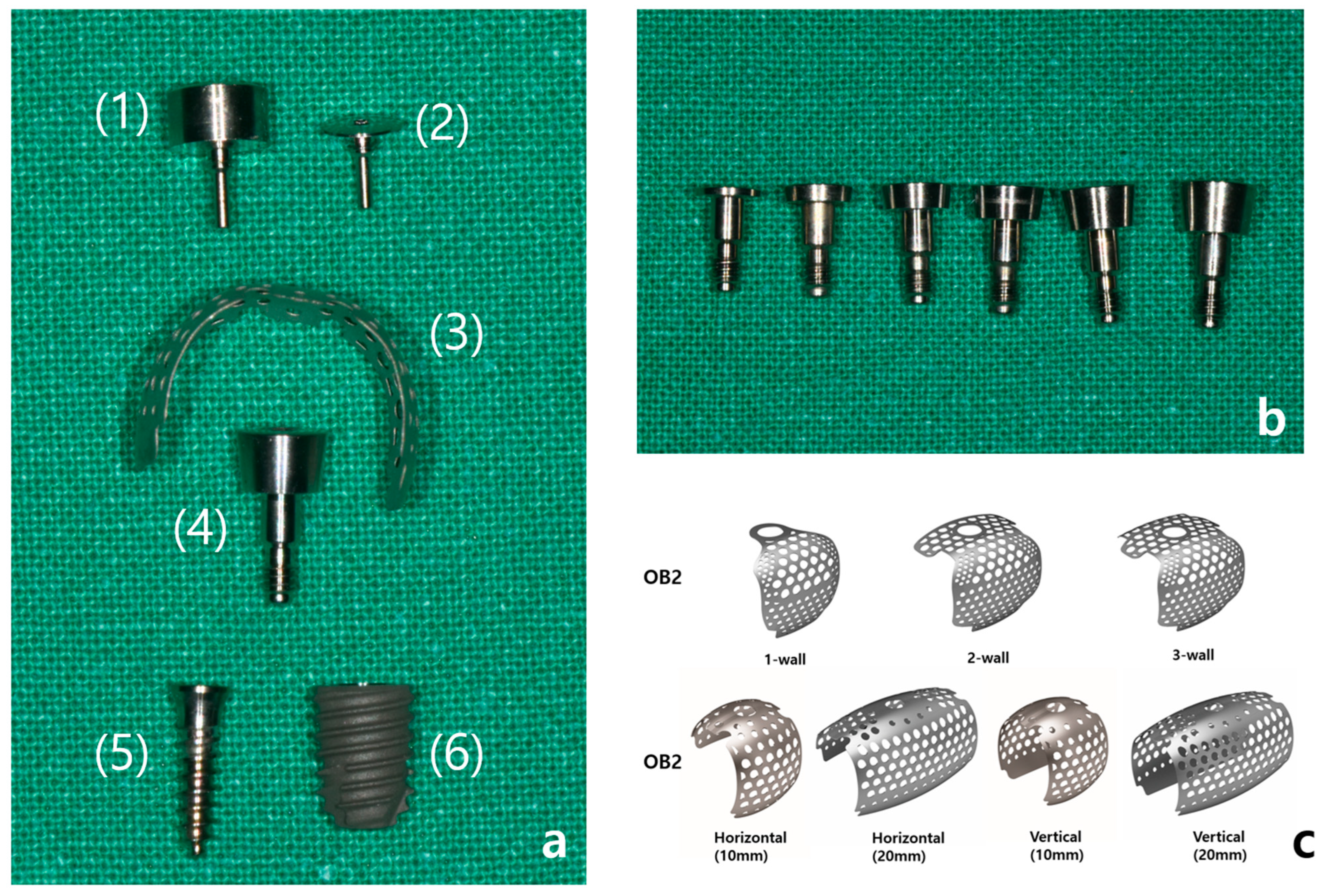
2.2. Preparation of 3-Dimensional Preformed Titanium Mesh
3. Results
- -
- Clinical efficacy: the combination of rhBMP-2 and a 3D-preformed titanium mesh (3D-PFTM) proved effective for reconstructing severely resorbed alveolar bone;
- -
- Osteoinductive potential: rhBMP-2 demonstrated strong osteoinductive activity, even in patients with compromised bone regenerative capacity;
- -
- Structural stability: the use of 3D-PFTM, particularly the OssBuilder system, provided reliable structural support for bone regeneration;
- -
- Implant success: the combined approach resulted in stable bone regeneration and long-term implant success;
- -
- Therapeutic value: the so called BOXAM (BMP-2, Oss-builder, xenograft, allograft, maintenance) technique appears to be a promising and reproducible strategy in dental and maxillofacial surgery.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
References
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543. [Google Scholar] [CrossRef]
- Hallman, M.; Thor, A. Bone substitutes and growth factors as an alternative/complement to autogenous bone for grafting in implant dentistry. Periodontol. 2000 2008, 47, 172–192. [Google Scholar] [CrossRef]
- Triplett, R.G.; Nevins, M.; Marx, R.E.; Spagnoli, D.B.; Oates, T.W.; Moy, P.K.; Boyne, P.J. Pivotal, randomized, parallel evaluation of recombinant human bone morphogenetic protein-2/absorbable collagen sponge and autogenous bone graft for maxillary sinus floor augmentation. J. Oral Maxillofac. Surg. 2009, 67, 1947–1960. [Google Scholar] [CrossRef]
- Rickert, D.; Slater, J.J.; Meijer, H.J.; Vissink, A.; Raghoebar, G.M. Maxillary sinus lift with solely autogenous bone compared to a combination of autogenous bone and growth factors or (solely) bone substitutes. A systematic review. Int. J. Oral Maxillofac. Surg. 2012, 41, 160–167. [Google Scholar] [CrossRef]
- Janjua, O.S.; Qureshi, S.M.; Shaikh, M.S.; Alnazzawi, A.; Rodriguez-Lozano, F.J.; Pecci-Lloret, M.P.; Zafar, M.S. Autogenous Tooth Bone Grafts for Repair and Regeneration of Maxillofacial Defects: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 3690. [Google Scholar] [CrossRef]
- Filho, S.A.R.; Francischone, C.E.; de Oliveira, J.C.; Ribeiro, L.Z.; Prado, F.Z.X.; Sotto-Maior, B.S. Bone augmentation of the atrophic anterior maxilla for dental implants using rhBMP-2 and titanium mesh: Histological and tomographic analysis. Int. J. Oral Maxillofac. Surg. 2015, 44, 1492–1498. [Google Scholar] [CrossRef]
- de Freitas, R.M.; Spin-Neto, R.; Junior, E.M.; Pereira, L.A.V.D.; Wikesjö, U.M.E.; Susin, C. Alveolar ridge and maxillary sinus augmentation using rhBMP-2: A systematic review. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. S1), e192–e201. [Google Scholar] [CrossRef]
- Miyazawa, K.; Shinozaki, M.; Hara, T.; Furuya, T.; Miyazono, K. Two Major Smad Pathways in TGF-β Superfamily Signalling. Genes. Cells 2002, 7, 1191–1204. [Google Scholar] [CrossRef]
- Urist, M.R. Bone: Formation by autoinduction. Science 1965, 150, 893–899. [Google Scholar] [CrossRef]
- Wozney, J.M.; Rosen, V.; Celeste, A.J.; Mitsock, L.M.; Whitters, M.J.; Kriz, R.W.; Hewick, R.M.; Wang, E.A. Novel regulators of bone formation: Molecular clones and activities. Science 1988, 242, 1528–1534. [Google Scholar] [CrossRef]
- Gomez-Puerto, M.C.; Iyengar, P.V.; de Vinuesa, A.G.; Ten Dijke, P.; Sanchez-Duffhues, G. Bone Morphogenetic Protein Receptor Signal Transduction in Human Disease. J. Pathol. 2019, 247, 9–20. [Google Scholar] [CrossRef]
- Wang, E.A.; Rosen, V.; D’Alessandro, J.S.; Bauduy, M.; Cordes, P.; Harada, T.; Israel, D.I.; Hewick, R.M.; Kerns, K.M.; LaPan, P. Recombinant human bone morphogenetic protein induces bone formation. Proc. Natl. Acad. Sci. USA 1990, 87, 2220–2224. [Google Scholar] [CrossRef]
- Galimberti, F.; Lubelski, D.; Healy, A.T.; Wang, T.; Abdullah, K.G.; Nowacki, A.S.; Benzel, E.C.; Mroz, T.E. A Systematic Review of Lumbar Fusion Rates With and Without the Use of rhBMP-2. Spine 2015, 40, 1132–1139. [Google Scholar] [CrossRef]
- Xie, Y.; Li, S.; Zhang, T.; Wang, C.; Cai, X. Titanium mesh for bone augmentation in oral implantology: Current application and progress. Int. J. Oral Sci. 2020, 12, 37. [Google Scholar] [CrossRef]
- Lee, K.A.; Kim, M.-S.; Lee, J.-S.; Jung, U.-W.; Kim, C.-S.; Cho, K.-S.; Chai, J.-K.; Choi, S.-H. Ridge Augmentation Using Titanium Mesh in Severe Alveolar Bone Resorption: A Case Report. Implantology 2013, 17, 12–22. [Google Scholar]
- Jovanovic, S.A.; Schenk, R.K.; Orsini, M.; Kenney, E.B. Supracrestal bone formation around dental implants: An experimental dog study. Int. J. Oral Maxillofac. Implant. 1995, 10, 23–31. [Google Scholar]
- Buser, D.; Dula, K.; Belser, U.C.; Hirt, H.P.; Berthold, H. Localized ridge augmentation using guided bone regeneration. II. Surgical procedure in the mandible. Int. J. Periodontics Restor. Dent. 1995, 15, 10–29. [Google Scholar]
- Miyamoto, I.; Funaki, K.; Yamauchi, K.; Kodama, T.; Takahashi, T. Alveolar ridge reconstruction with titanium mesh and autogenous particulate bone graft: Computed tomography-based evaluations of augmented bone quality and quantity. Clin. Implant Dent. Relat. Res. 2012, 14, 304–311. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Ramieri, G.; Bunino, M.; Berrone, S. Autogenous bone graft alone or associated with titanium mesh for vertical alveolar ridge augmentation: A controlled clinical trial. Clin. Oral Implant. Res. 2007, 18, 286–294. [Google Scholar] [CrossRef]
- Urban, I.; Montero, E.; Sanz-Sánchez, I.; Palombo, D.; Monje, A.; Tommasato, G.; Chiapasco, M. Minimal invasiveness in vertical ridge augmentation. Periodontol. 2000 2023, 91, 126–144. [Google Scholar] [CrossRef]
- Lee, S.H.; Moon, J.H.; Jeong, C.M.; Bae, E.B.; Park, C.E.; Jeon, G.R.; Lee, J.J.; Jeon, Y.C.; Huh, J.B. The mechanical properties and biometrical effect of 3D preformed titanium membrane for guided bone regeneration on alveolar bone defect. BioMed Res. Int. 2017, 2017, 7102123. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.-O.; Oh, J.-S.; Yu, S.-J.; Kim, B.-O.; Lee, W.-P. Retrospective Analysis of the Effect of Three-Dimensional Preformed Titanium Mesh on Peri-Implant Non-Contained Horizontal Defects in 100 Consecutive Cases. Appl. Sci. 2021, 11, 872. [Google Scholar] [CrossRef]
- Trento, G.S.; Carvalho, P.H.A.; Macedo, D.V.; Gabrielli, M.A.C.; Monnazzi, M.S.; Pereira-Filho, V.A. Titanium mesh associated with rhBMP-2 in alveolar ridge reconstruction. Int. J. Oral Maxillofac. Surg. 2019, 48, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.A. Vertical and Horizontal Ridge Augmentation: New Perspectives, 1st ed.; Quintessence Publishing: Berlin, Germany, 2017; pp. 117–146. [Google Scholar]
- Urban, I.A.; Montero, E.; Amerio, E.; Palombo, D.; Monje, A. Techniques on vertical ridge augmentation: Indications and effectiveness. Periodontol. 2000 2023, 93, 153–182. [Google Scholar] [CrossRef]
- Cucchi, A.; Vignudelli, E.; Franceschi, D.; Randellini, E.; Lizio, G.; Fiorino, A.; Corinaldesi, G. Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial. Clin. Oral Implant. Res. 2021, 32, 1411–1424. [Google Scholar] [CrossRef]
- Ramly, E.P.; Alfonso, A.R.; Kantar, R.S.; Wang, M.M.B.; Siso, J.R.D.; Ibrahim, A.M.; Coelho, P.G.D.; Flores, R.L. Safety and Efficacy of Recombinant Human Bone Morphogenetic Protein-2 (rhBMP-2) in Craniofacial Surgery. Plast. Reconstr. Surg. Glob. Open. 2019, 7, e2347. [Google Scholar] [CrossRef]
- Hong, S.J.; Kim, C.S.; Han, D.K.; Cho, I.H.; Jung, U.W.; Choi, S.H.; Kim, C.K.; Cho, K.S. The effect of a fibrin-fbronectin/β-tricalcium phosphate/ recombinant human bone morphogenetic protein-2 system on bone formation in rat calvarial defects. Biomaterials 2006, 27, 3810–3816. [Google Scholar] [CrossRef]
- Sheikh, Z.; Javaid, M.A.; Hamdan, N.; Hashmi, R. Bone Regeneration Using Bone Morphogenetic Proteins and Various Biomaterial Carriers. Materials 2015, 8, 1778–1816. [Google Scholar] [CrossRef]
- Seo, J.I.; Lim, J.H.; Jo, W.M.; Lee, J.K.; Song, S.I. Effects of rhBMP-2 with various carriers on maxillofacial bone regeneration through computed tomography evaluation. Maxillofac. Plast. Reconstr. Surg. 2023, 45, 40. [Google Scholar] [CrossRef]
- Park, J.-C.; Bae, E.-B.; Kim, S.-E.; Kim, S.-Y.; Choi, K.-H.; Choi, J.-W.; Bae, J.-H.; Ryu, J.-J.; Huh, J.-B. Effects of BMP-2 Delivery in Calcium Phosphate Bone Graft Materials with Different Compositions on Bone Regeneration. Materials 2016, 9, 954. [Google Scholar] [CrossRef]
- Um, I.-W.; Ku, J.-K.; Kim, Y.-K.; Lee, B.-K.; Leem, D.-H. Histological Review of Demineralized Dentin Matrix as a Carrier of rhBMP-2. Tissue Eng. Part B Rev. 2020, 26, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.M. Bone augmentation of the atrophic posterior mandible for dental implants using rhBMP-2 and titanium mesh: Clinical technique and early results. Int. J. Periodontics Restor. Dent. 2011, 31, 581–589. [Google Scholar]
- Kloss, F.R.; Kämmerer, P.W.; Kloss-Brandstätter, A. First Clinical Case Report of a Xenograft–Allograft Combination for Alveolar Ridge Augmentation Using a Bovine Bone Substitute Material with Hyaluronate (Cerabone® Plus) Combined with Allogeneic Bone Granules (Maxgraft®). J. Clin. Med. 2023, 12, 6214. [Google Scholar] [CrossRef]
- Sohn, H.S.; Oh, J.K. Review of bone graft and bone substitutes with an emphasis on fracture surgeries. Biomater. Res. 2019, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Menchini-Fabris, G.B.; Cosola, S.; Toti, P.; Hwang, M.H.; Crespi, R.; Covani, U. Immediate Implant and Customized Healing Abutment for a Periodontally Compromised Socket: 1-Year Follow-Up Retrospective Evaluation. J. Clin. Med. 2023, 12, 2783. [Google Scholar] [CrossRef]
- Cosola, S.; Di Dino, B.; Traini, T.; Kim, Y.S.; Park, Y.M.; Marconcini, S.; Covani, U.; Vinci, R. Radiographic and Histomorphologic Evaluation of the Maxillary Bone after Crestal Mini Sinus Lift Using Absorbable Collagen—Retrospective Evaluation. Dent. J. 2022, 10, 58. [Google Scholar] [CrossRef]
- Ahamed, S.K.; Menchini-Fabris, G.B.; Alqarni, A.; Alarabi, S.M.; Alharbi, A.A.; Alshamrani, A.; Covani, U.; Cosola, S. Insights into the Current Management Techniques for Peri-Implant Gaps: A Systematic Review. J. Clin. Med. 2025, 14, 3351. [Google Scholar] [CrossRef]
- Bostrom, M.P.G.; Seigerman, D.A. The Clinical Use of Allografts, Demineralized Bone Matrices, Synthetic Bone Graft Substitutes and Osteoinductive Growth Factors: A Survey Study. HSS J. 2005, 1, 9–18. [Google Scholar] [CrossRef]
- Kloss, F.R.; Offermanns, V.; Kloss-Brandstätter, A. Comparison of allogeneic and autogenous bone grafts for augmentation of alveolar ridge defects—A 12-month retrospective radiographic evaluation. Clin. Oral Implant. Res. 2018, 29, 1163–1175. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Deluiz, D.; Tinoco, E.M.B. Horizontal Alveolar Ridge Augmentation with Allogeneic Bone Block Graft Compared with Autogenous Bone Block Graft: A Systematic Review. J. Oral Maxillofac. Res. 2020, 11, e1. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Zahedpasha, A.; Ghassemi, A.; Bijani, A.; Haghanifar, S.; Majidi, M.S.; Ghorbani, Z.M. Comparison of Bone Formation After Sinus Membrane Lifting without Graft or Using Bone Substitute “Histologic and Radiographic Evaluation”. J. Oral Maxillofac. Surg. 2021, 79, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.-K.; Song, J.-M.; Kim, I.-R.; Park, B.-S.; Kim, C.-H.; Cheong, I.-K.; Shin, S.-H. Effect of recombinant human bone morphogenetic protein-2 on bisphosphonate-treated osteoblasts. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Min, S.-H.; Kang, N.-E.; Song, S.-I.; Lee, J.-K. Regenerative effect of recombinant human bone morphogenetic protein-2/absorbable collagen sponge (rhBMP-2/ACS) after sequestrectomy of medication-related osteonecrosis of the jaw (MRONJ). J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 191–196. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, K.J.; Kim, B.J.; Kim, C.H.; Kim, J.H. Immediate reconstruction of mandibular defect after treatment of medication-related osteonecrosis of the jaw (MRONJ) with rhBMP-2/ACS and miniplate: Review of 3 cases. Int. J. Surg. Case Rep. 2020, 66, 25–29. [Google Scholar] [CrossRef]
- Urban, I.A.; Nagursky, H.; Lozada, J.L.; Nagy, K. Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: A prospective case series in 25 patients. Int. J. Periodontics Restor. Dent. 2013, 33, 299–307. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and Options Using Resorbable versus Nonresorbable Membranes for Successful Guided Bone Regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar]
- Carbonell, J.M.; Martín, I.S.; Santos, A.; Pujol, A.; Sanz-Moliner, J.D.; Nart, J. High-Density Polytetrafluoroethylene Membranes in Guided Bone and Tissue Regeneration Procedures: A Literature Review. Int. J. Oral Maxillofac. Surg. 2014, 43, 75–84. [Google Scholar] [CrossRef]
- Ronda, M.; Rebaudi, A.; Torelli, L.; Stacchi, C. Expanded vs. Dense Polytetrafluoroethylene Membranes in Vertical Ridge Augmentation around Dental Implants: A Prospective Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2014, 25, 859–866. [Google Scholar] [CrossRef]
- Cucchi, A.; Ghensi, P. Vertical Guided Bone Regeneration Using Titanium-Reinforced d-PTFE Membrane and Prehydrated Corticocancellous Bone Graft. Open Dent. J. 2014, 8, 194–200. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, Z.; Yun, J.; Liu, R.; Li, J.; Chen, Y.; Cai, H.; Jiang, H.B.; Lee, E.S.; Han, J.; et al. Effect of Different Membranes on Vertical Bone Regeneration: A Systematic Review and Network Meta-Analysis. BioMed Res. Int. 2022, 2022, 7742687. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Vignudelli, E.; Napolitano, A.; Marchetti, C.; Corinaldesi, G. Evaluation of Complication Rates and Vertical Bone Gain after Guided Bone Regeneration with Non-resorbable Membranes versus Titanium Meshes and Resorbable Membranes: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 821. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Chiono, V.; Tonda-Turo, C.; Ferreira, A.M.; Ciardelli, G. Polymeric Membranes for Guided Bone Regeneration. Biotechnol. J. 2011, 6, 1187–1197. [Google Scholar] [CrossRef]
- Rasia dal Polo, M.; Poli, P.P.; Rancitelli, D.; Beretta, M.; Maiorana, C. Alveolar Ridge Reconstruction with Titanium Meshes: A Systematic Review of the Literature. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e639. [Google Scholar] [CrossRef]
- Minniti, A.; Caroprese, M.; Zarantonello, M.; De Santis, D.; Caliendo, G.; Gelpi, F. High-Density Dermal Matrix for Soft Tissue Augmentation Using a Matrix Tissue Graft Technique—A Comprehensive Multicenter Analysis of 20 Implants: A 1-Year Follow-Up Retrospective Study. J. Clin. Med. 2024, 13, 2954. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Menchini Fabris, G.B.; Lotti, J.; Palumbo, C.; Ferretti, M.; Castellani, R.; Lotti, T.; Zanotti, G.; Gelpi, F.; Covani, C.; et al. Bi-layered collagen nano-structured membrane prototype collagen matrix 10826® for soft tissue regeneration in rabbits: An in vivo ultra-structural study of the early healing phase. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. S2), 91–97. [Google Scholar]
- Nocini, P.F.; Menchini Fabris, G.B.; Gelpi, F.; Lotti, J.; Favero, V.; Zanotti, G.; Jurlaro, A.; Rosskopf, I.; Lotti, T.; Barone, A.; et al. Treatment of skin defects with growth factors and biodegradable collagen carrier: Histological evaluation in animal model. J. Biol. Regul. Homeost. Agents 2017, 31, 1–13. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.W.; Cosola, S.; Kim, Y.S.; Park, Y.M.; Covani, U.; Fabbri, A.; Menchini-Fabris, G.B. Clinical Application of rhBMP-2 and Three-Dimensinal Preformed Titanium Mesh with Allograft and Xenograft for Peri-Implant Horizontal and Vertical Bone Augmentation–A Narrative Review with Technical Report. J. Clin. Med. 2025, 14, 4788. https://doi.org/10.3390/jcm14134788
Kim YW, Cosola S, Kim YS, Park YM, Covani U, Fabbri A, Menchini-Fabris GB. Clinical Application of rhBMP-2 and Three-Dimensinal Preformed Titanium Mesh with Allograft and Xenograft for Peri-Implant Horizontal and Vertical Bone Augmentation–A Narrative Review with Technical Report. Journal of Clinical Medicine. 2025; 14(13):4788. https://doi.org/10.3390/jcm14134788
Chicago/Turabian StyleKim, Yeong Wook, Saverio Cosola, Young Sam Kim, Young Min Park, Ugo Covani, Aimone Fabbri, and Giovanni Battista Menchini-Fabris. 2025. "Clinical Application of rhBMP-2 and Three-Dimensinal Preformed Titanium Mesh with Allograft and Xenograft for Peri-Implant Horizontal and Vertical Bone Augmentation–A Narrative Review with Technical Report" Journal of Clinical Medicine 14, no. 13: 4788. https://doi.org/10.3390/jcm14134788
APA StyleKim, Y. W., Cosola, S., Kim, Y. S., Park, Y. M., Covani, U., Fabbri, A., & Menchini-Fabris, G. B. (2025). Clinical Application of rhBMP-2 and Three-Dimensinal Preformed Titanium Mesh with Allograft and Xenograft for Peri-Implant Horizontal and Vertical Bone Augmentation–A Narrative Review with Technical Report. Journal of Clinical Medicine, 14(13), 4788. https://doi.org/10.3390/jcm14134788