
A Step-By-Step Guide for Robotic Blumgart Pancreaticojejunostomy

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
- The jejunal stump is marked with a simple stitch of 3/0 polydioxanone monofilament (see 00:20 in Supplementary Video S1).
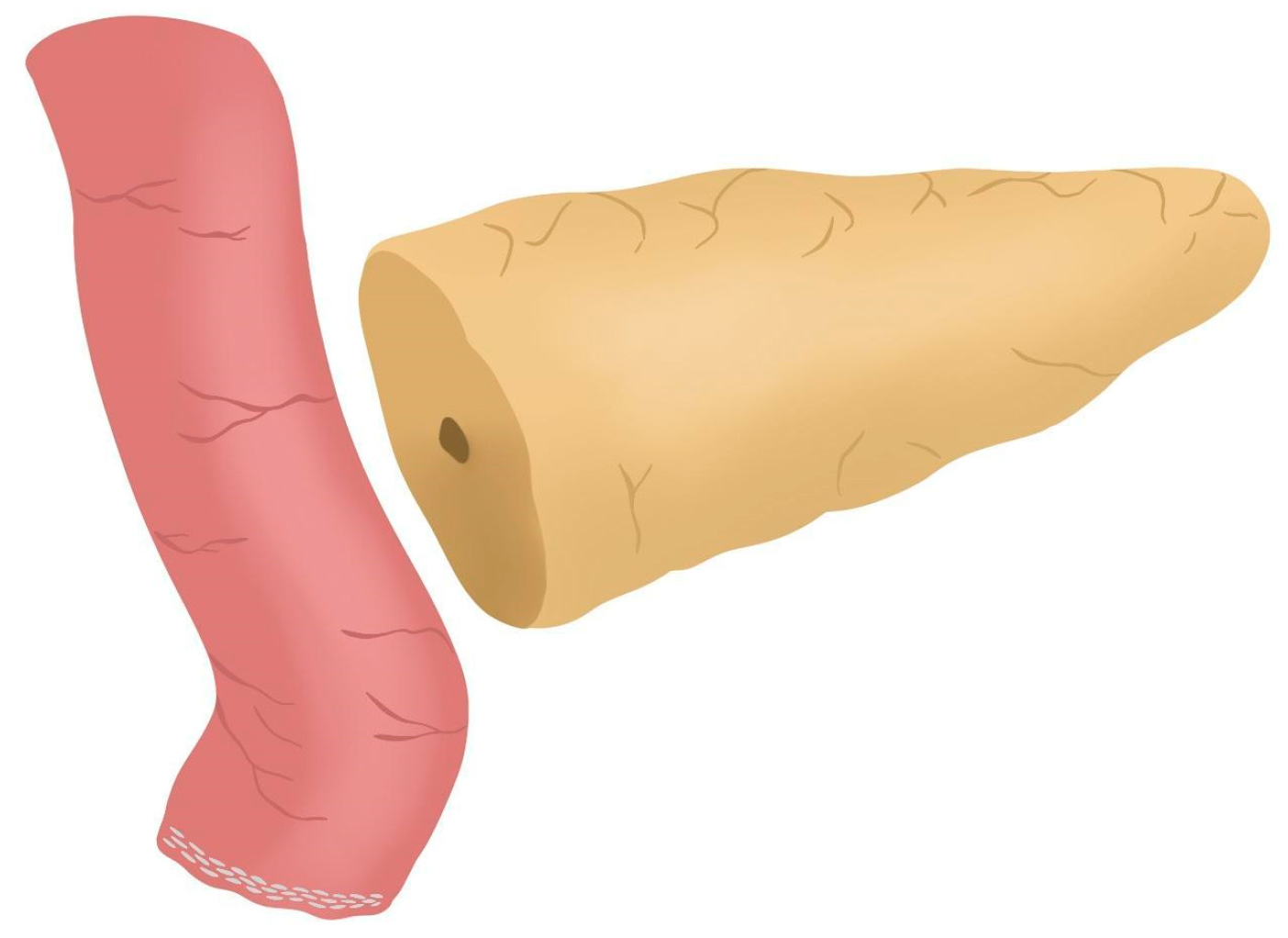
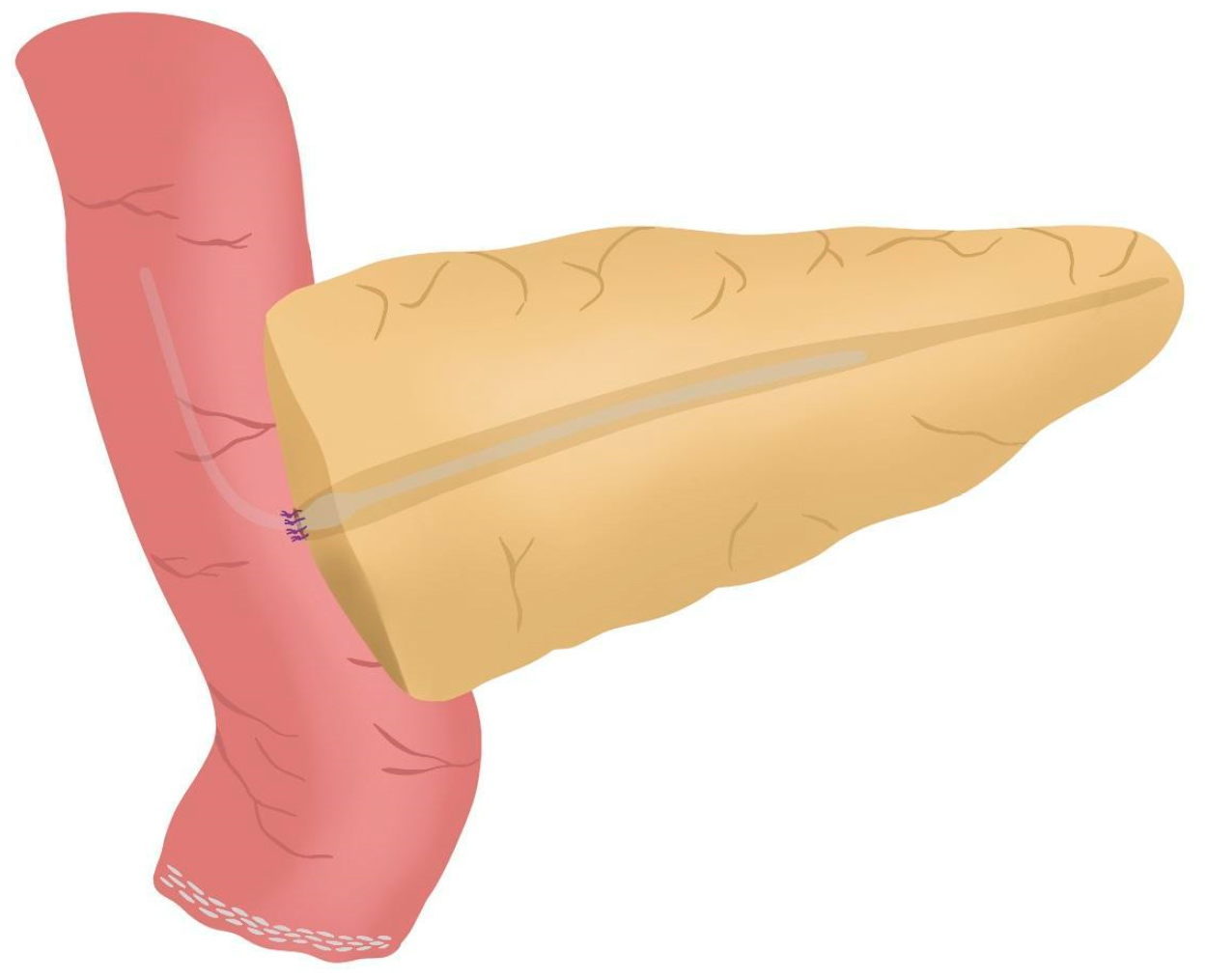
- The marked biliopancreatic limb is uncrossed through the duodenal tunnel and placed facing the pancreatic stump (Figure 2) (see 00:33 in Supplementary Video S1).
- The length of the pancreatic duct drainage is tested. We use a multi-perforated 1–2 mm polyvinyl chloride pancreatic drainage, depending on the diameter of the pancreatic duct. It must fill the whole length of the remaining pancreatic duct (see 00:43 in Supplementary Video S1).
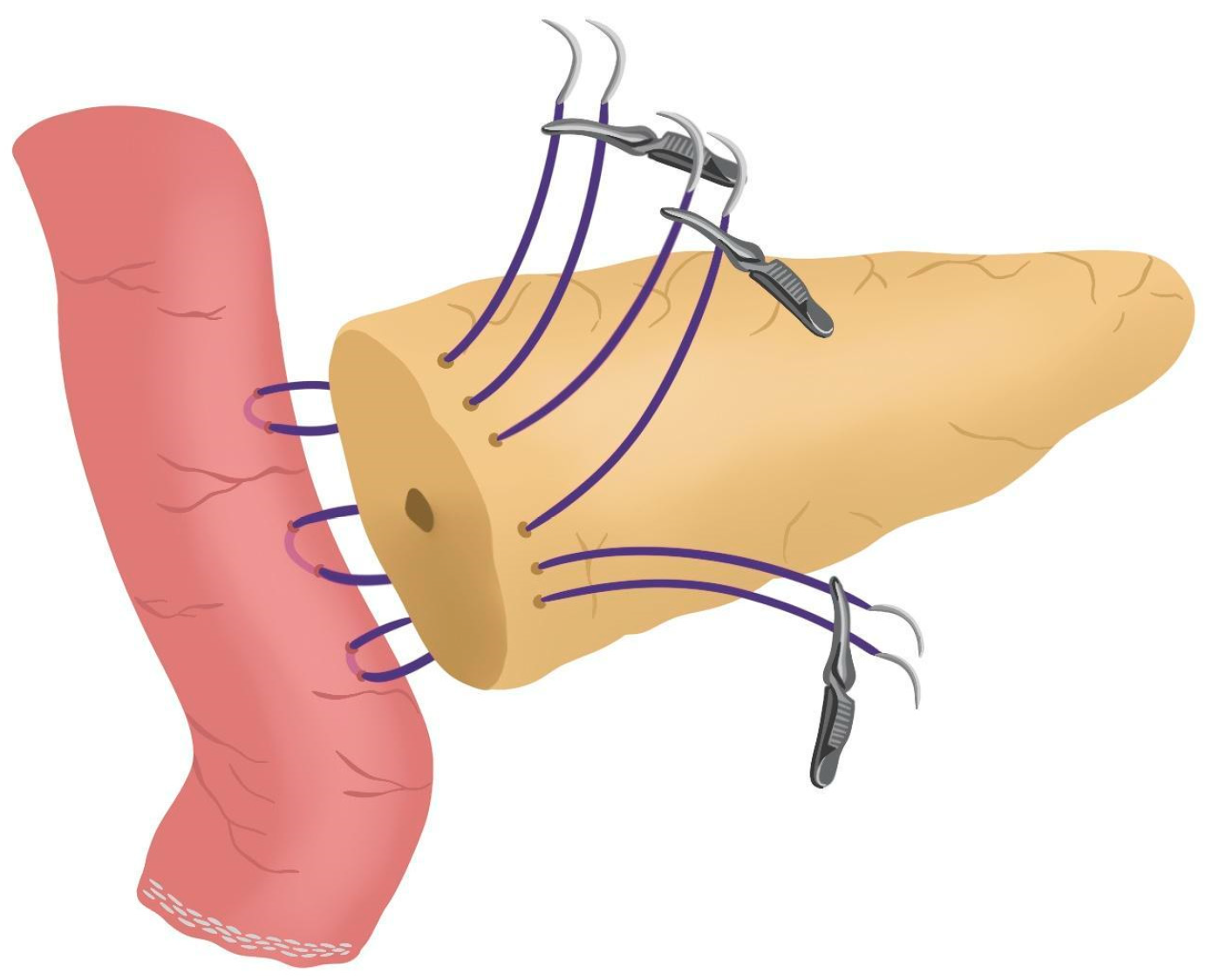
- Posterior Blumgart stitches with a double-needle 3/0 polydioxanone monofilament are performed. We usually perform 3 Blumgart stitches, but it can vary depending on the size of the pancreas. The first of them (the lower one) is performed below the pancreatic duct; the second one (the central one) is usually performed surrounding the pancreatic duct (one stitch below and the other over the pancreatic duct, without damaging it); and the third one (the upper one) over the pancreatic duct. The needle is inserted through the full thickness of the pancreatic stump with each stitch, starting from the anterior face and exiting through the posterior face. After that, the same needle is stitched on the posterior wall of the jejunal serosa in a longitudinal direction. Finally, the entire thickness of the pancreatic stump is pierced again from its posterior to its anterior face, in an upper position. Each Blumgart stitch is marked with a bulldog clamp and the needles are stuck in an orderly manner in a wrapped gauze (Figure 3) (see 00:52 in Supplementary Video S1).
- Prior to enterotomy, both side corner stitches of the duct-to-jejunal anastomosis are performed with a 5/0 polydioxanone monofilament and marked with Hem-o-locks® (Figure 4) (see 01:36 in Supplementary Video S1).
- Enterotomy in the antimesenteric side of the biliopancreatic limb is performed (see 02:10 in Supplementary Video S1).
- Posterior wall stitches of the duct-to-mucosa anastomosis PJ are performed with 5/0 polydioxanone monofilament. They are marked with metallic clips to distinguish them from the corner stitches (marked with Hem-o-locks®) and subsequently tied when all the stitches have been performed (Figure 5) (see 02:16 in Supplementary Video S1).
- The pancreatic duct drainage is definitively placed into the pancreatic duct and biliopancreatic limb. The central stitch of the posterior wall of the duct-to-mucosa anastomosis is tied fixing the pancreatic duct drainage (Figure 6). This pancreatic duct drainage stent has an olive that acts as a stopper, preventing migration and ensuring it remains in the desired position for at least one month (see 03:24 in Supplementary Video S1). In patients with soft pancreatic texture and/or a small pancreatic duct (≤3 mm), we employ an externalized pancreatic duct drainage by Witzel technique to minimize the risk of POPF.
- Afterwards, the anterior wall stitches are performed with 5/0 polydioxanone monofilament, marked with metallic clips and subsequently tied, completing the duct-to-mucosa anastomosis (Figure 7) (see 04:02 in Supplementary Video S1).
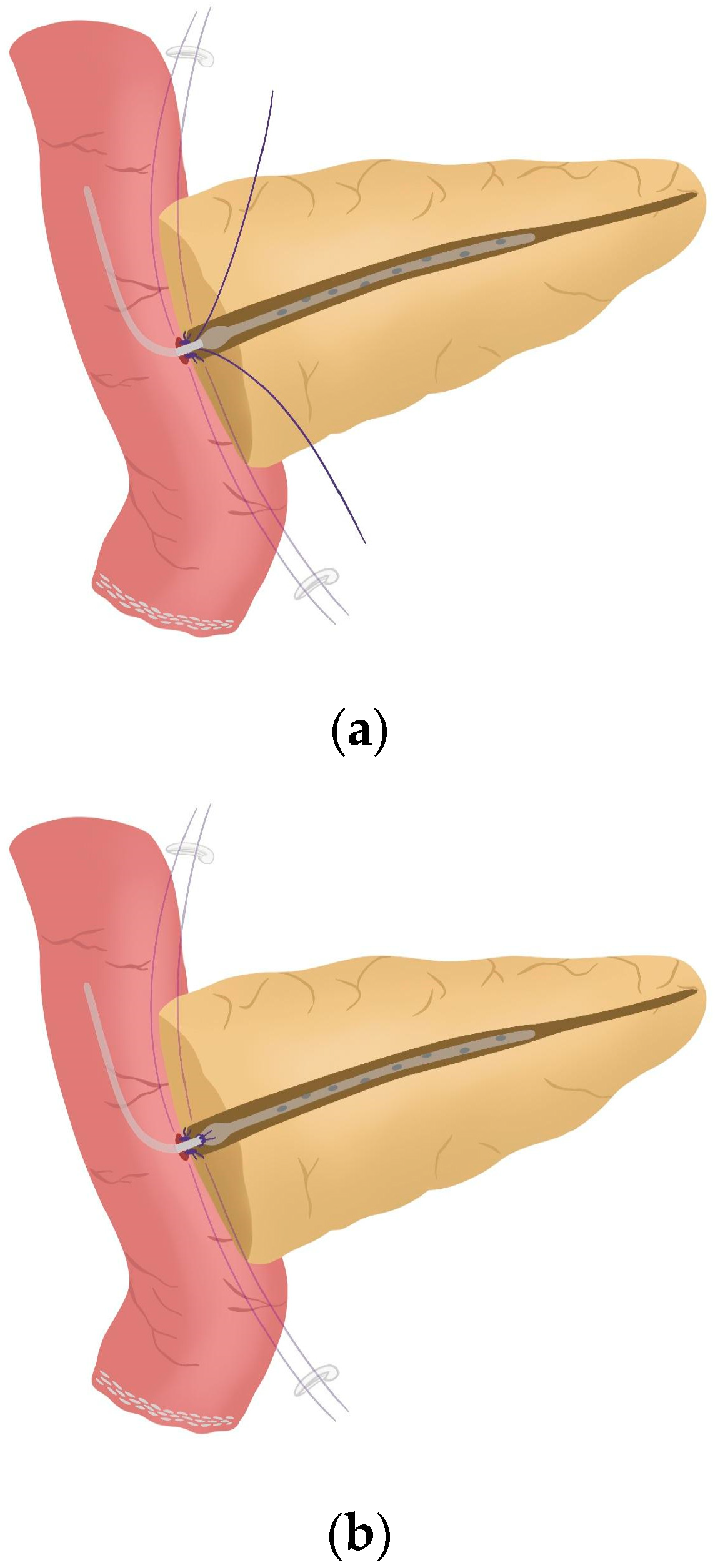
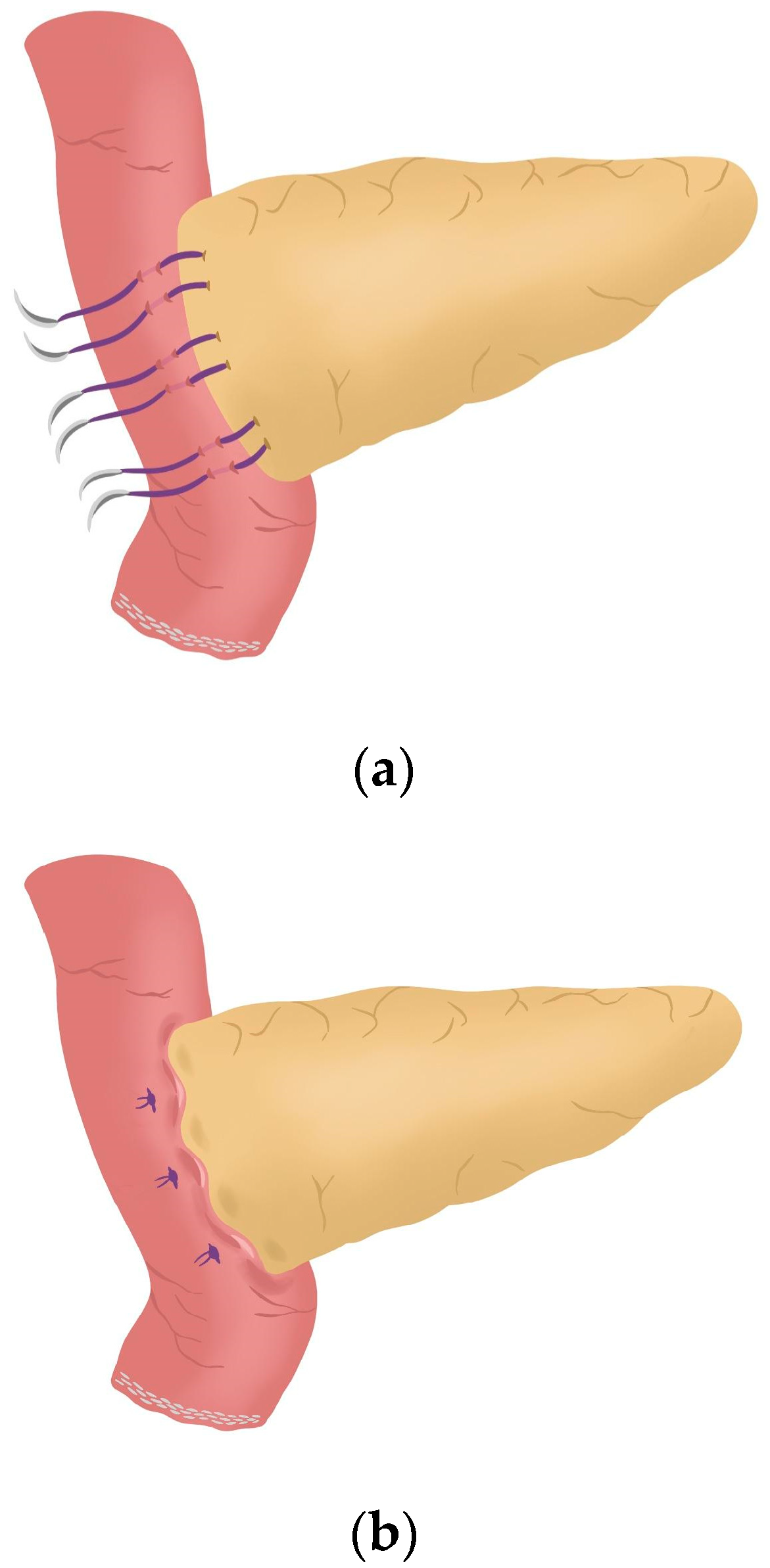
- Completion of Blumgart anastomosis: Finally, bulldog clamps are removed, and each needle of each double-needle 3/0 polydioxanone monofilament is stitched on the anterior wall of the jejunal serosa in a transverse direction and an orderly way (Figure 8a). Each of the three stitches are tied so that the pancreatic stump keeps invaginated against the jejunal serosa (Figure 8b) (see 04:39 in Supplementary Video S1).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PD | Pancreaticoduodenectomy |
| RPD | Robotic pancreaticoduodenectomy |
| OPD | Open pancreaticoduodenectomy |
| PJ | Pancreaticojejunostomy |
| PG | Pancreaticogastrostomy |
| POPF | Postoperative pancreatic fistula |
| CR-POPF | Clinically relevant postoperative pancreatic fistula |
| BA | Blumgart anastomosis |
| CWA | Cattell–Warren anastomosis |
References
- Damoli, I.; Butturini, G.; Ramera, M.; Paiella, S.; Marchegiani, G.; Bassi, C. Minimally invasive pancreatic surgery—A review. Videosurg. Other Miniinvasive Tech. 2015, 10, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Abu Hilal, M.; Besselink, M.G.; Hackert, T.; Palanivelu, C.; Zhao, Y.; He, J.; Boggi, U.; Jang, J.Y.; Panaro, F.; et al. International consensus guidelines on robotic pancreatic surgery in 2023. Hepatobiliary Surg. Nutr. 2024, 13, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Aiolfi, A.; Lombardo, F.; Bonitta, G.; Danelli, P.; Bona, D. Systematic review and updated network meta-analysis comparing open, laparoscopic, and robotic pancreaticoduodenectomy. Updates Surg. 2021, 73, 909–922. [Google Scholar] [CrossRef]
- Zhao, W.; Liu, C.; Li, S.; Geng, D.; Feng, Y.; Sun, M. Safety and efficacy for robot-assisted versus open pancreaticoduodenectomy and distal pancreatectomy: A systematic review and meta-analysis. Surg. Oncol. 2018, 27, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Kone, L.B.; Maker, V.K.; Banulescu, M.; Maker, A.V. A propensity score analysis of over 12,000 pancreaticojejunal anastomoses after pancreaticoduodenectomy: Does technique impact the clinically relevant fistula rate? HPB 2020, 22, 1394–1401. [Google Scholar] [CrossRef]
- McMillan, M.T.; Malleo, G.; Bassi, C.; Sprys, M.H.; Vollmer, C.M., Jr. Defining the practice of pancreatoduodenectomy around the world. HPB 2015, 17, 1145–1154. [Google Scholar] [CrossRef]
- Barreto, S.G.; Shukla, P.J. Different types of pancreatico-enteric anastomosis. Transl. Gastroenterol. Hepatol. 2017, 2, 89. [Google Scholar] [CrossRef]
- Cheng, Y.; Briarava, M.; Lai, M.; Wang, X.; Tu, B.; Cheng, N.; Gong, J.; Yuan, Y.; Pilati, P.; Mocellin, S. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction for the prevention of postoperative pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2017, 9, CD012257. [Google Scholar] [CrossRef]
- Yang, S.H.; Dou, K.F.; Sharma, N.; Song, W.J. The methods of reconstruction of pancreatic digestive continuity after pancreaticoduodenectomy: A meta-analysis of randomized controlled trials. World J. Surg. 2011, 35, 2290–2297. [Google Scholar] [CrossRef]
- Blumgart, L.H.; Fong, Y. Surgery of the Liver and Biliary Tract, 3rd ed.; Blumgart, L.H., Fong, Y., Eds.; Saunders: Philadelphia, PA, USA, 2000; pp. 1073–1089. [Google Scholar]
- Lee, Y.N.; Kim, W.Y. Comparison of Blumgart versus conventional duct-to-mucosa anastomosis for pancreaticojejunostomy after pancreaticoduodenectomy. Ann. Hepato-Biliary-Pancreat. Surg. 2018, 22, 253–260. [Google Scholar] [CrossRef]
- Ricci, C.; Ingaldi, C.; Alberici, L.; Pagano, N.; Mosconi, C.; Marasco, G.; Minni, F.; Casadei, R. Blumgart Anastomosis After Pancreaticoduodenectomy. A Comprehensive Systematic Review, Meta-Analysis, and Meta-Regression. World J. Surg. 2021, 45, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hua, R. The optimal choice for pancreatic anastomosis after pancreaticoduodenectomy. Minerva Surg. 2022, 77, 65–71. [Google Scholar] [CrossRef]
- Perivoliotis, K.; Sioka, E.; Tatsioni, A.; Stefanidis, I.; Zintzaras, E.; Zacharoulis, D. Pancreatogastrostomy versus Pancreatojejunostomy: An Up-to-Date Meta-Analysis of RCTs. Int. J. Surg. Oncol. 2017, 2017, 7526494. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.; Elewa, A.; Elsherbiny, M.; Tourkey, M.; Emechap, E.N.; Chikukuza, S.; Salman, A. Postoperative pancreatic fistula after pancreaticogastrostomy versus pancreatojejunostomy after pancreatic resection, a comparative systematic review and meta-analysis. World J. Surg. 2024, 48, 1467–1480. [Google Scholar] [CrossRef] [PubMed]
- Keck, T.; Wellner, U.F.; Bahra, M.; Klein, F.; Sick, O.; Niedergethmann, M.; Wilhelm, T.J.; Farkas, S.A.; Börner, T.; Bruns, C.; et al. Pancreatogastrostomy Versus Pancreatojejunostomy for RECOnstruction After PANCreatoduodenectomy (RECOPANC, DRKS 00000767): Perioperative and Long-term Results of a Multicenter Randomized Controlled Trial. Ann. Surg. 2016, 263, 440–449. [Google Scholar] [CrossRef]
- Olakowski, M.; Grudzińska, E.; Mrowiec, S. Pancreaticojejunostomy—A review of modern techniques. Langenbeck’s Arch. Surg. 2020, 405, 13–22. [Google Scholar] [CrossRef]
- Halloran, C.M.; Neoptolemos, J.P.; Jackson, R.; Platt, K.; Psarelli, E.E.; Reddy, S.; Gomez, D.; O’Reilly, D.A.; Smith, A.; Pausch, T.M.; et al. A Multicenter, Randomized, Double-Blinded, Clinical Trial Comparing Cattell-Warren and Blumgart Anastomoses Following Partial Pancreatoduodenectomy: PANasta Trial. Ann. Surg. Open 2022, 3, e198. [Google Scholar] [CrossRef]
- Hai, H.; Li, Z.; Zhang, Z.; Cheng, Y.; Liu, Z.; Gong, J.; Deng, Y. Duct-to-mucosa versus other types of pancreaticojejunostomy for the prevention of postoperative pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2022, 3, CD013462. [Google Scholar] [CrossRef]
- Pedrazzoli, S. Pancreatoduodenectomy (PD) and postoperative pancreatic fistula (POPF): A systematic review and analysis of the POPF-related mortality rate in 60,739 patients retrieved from the English literature published between 1990 and 2015. Medicine 2017, 96, e6858. [Google Scholar] [CrossRef]
- Hirashita, T.; Iwashita, Y.; Fujinaga, A.; Nakanuma, H.; Tada, K.; Masuda, T.; Endo, Y.; Ohta, M.; Inomata, M. Short internal pancreatic stent reduces pancreatic fistula in pancreatoduodenectomy. Langenbecks Arch. Surg. 2021, 406, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Shrikhande, S.V.; Sivasanker, M.; Vollmer, C.M.; Friess, H.; Besselink, M.G.; Fingerhut, A.; Yeo, C.J.; Fernandez-delCastillo, C.; Dervenis, C.; Halloran, C.; et al. International Study Group of Pancreatic Surgery (ISGPS) Pancreatic anastomosis after pancreatoduodenectomy: A position statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2017, 161, 1221–1234. [Google Scholar] [CrossRef] [PubMed]
- Andrianello, S.; Marchegiani, G.; Malleo, G.; Masini, G.; Balduzzi, A.; Paiella, S.; Esposito, A.; Landoni, L.; Casetti, L.; Tuveri, M.; et al. Pancreaticojejunostomy With Externalized Stent vs. Pancreaticogastrostomy With Externalized Stent for Patients With High-Risk Pancreatic Anastomosis: A Single-Center, Phase 3, Randomized Clinical Trial. JAMA Surg. 2020, 155, 313–321. [Google Scholar] [CrossRef] [PubMed]
- McMillan, M.T.; Ecker, B.L.; Behrman, S.W.; Callery, M.P.; Christein, J.D.; Drebin, J.A.; Fraker, D.L.; Kent, T.S.; Lee, M.K.; Roses, R.E.; et al. Externalized Stents for Pancreatoduodenectomy Provide Value Only in High-Risk Scenarios. J. Gastrointest. Surg. 2016, 20, 2052–2062. [Google Scholar] [CrossRef]
- Pessaux, P.; Sauvanet, A.; Mariette, C.; Paye, F.; Muscari, F.; Cunha, A.S.; Sastre, B.; Arnaud, J.P.; Fédération de Recherche en Chirurgie (French). External pancreatic duct stent decreases pancreatic fistula rate after pancreaticoduodenectomy: Prospective multicenter randomized trial. Ann. Surg. 2011, 253, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.E.; Shyr, B.U.; Chen, S.C.; Shyr, Y.M. Comparison between robotic and open pancreaticoduodenectomy with modified Blumgart pancreaticojejunostomy: A propensity score-matched study. Surgery 2018, 164, 1162–1167. [Google Scholar] [CrossRef]
- Uchida, Y.; Takahara, T.; Mizumoto, T.; Nishimura, A.; Mii, S.; Iwama, H.; Kojima, M.; Kato, Y.; Uyama, I.; Suda, K. Technical details of robotic pancreatojejunostomy using a modified Blumgart anastomosis: Thread manipulation using gauze and an assisted port. World J. Surg. 2024, 48, 1721–1729. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qian, S.; Carrillo-Peña, J.; Domínguez-Prieto, V.; Villarejo-Campos, P.; Jiménez-Fuertes, M.; Pastor-Riquelme, P.; Jiménez-Galanes, S. A Step-By-Step Guide for Robotic Blumgart Pancreaticojejunostomy. J. Clin. Med. 2025, 14, 4471. https://doi.org/10.3390/jcm14134471
Qian S, Carrillo-Peña J, Domínguez-Prieto V, Villarejo-Campos P, Jiménez-Fuertes M, Pastor-Riquelme P, Jiménez-Galanes S. A Step-By-Step Guide for Robotic Blumgart Pancreaticojejunostomy. Journal of Clinical Medicine. 2025; 14(13):4471. https://doi.org/10.3390/jcm14134471
Chicago/Turabian StyleQian, Siyuan, Jeison Carrillo-Peña, Víctor Domínguez-Prieto, Pedro Villarejo-Campos, Montiel Jiménez-Fuertes, Pablo Pastor-Riquelme, and Santos Jiménez-Galanes. 2025. "A Step-By-Step Guide for Robotic Blumgart Pancreaticojejunostomy" Journal of Clinical Medicine 14, no. 13: 4471. https://doi.org/10.3390/jcm14134471
APA StyleQian, S., Carrillo-Peña, J., Domínguez-Prieto, V., Villarejo-Campos, P., Jiménez-Fuertes, M., Pastor-Riquelme, P., & Jiménez-Galanes, S. (2025). A Step-By-Step Guide for Robotic Blumgart Pancreaticojejunostomy. Journal of Clinical Medicine, 14(13), 4471. https://doi.org/10.3390/jcm14134471