

Clinical Variability of Pediatric MERS: Insights from a Retrospective Observational Study

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Preexisting Illness
3.2. Prodromal Symptoms
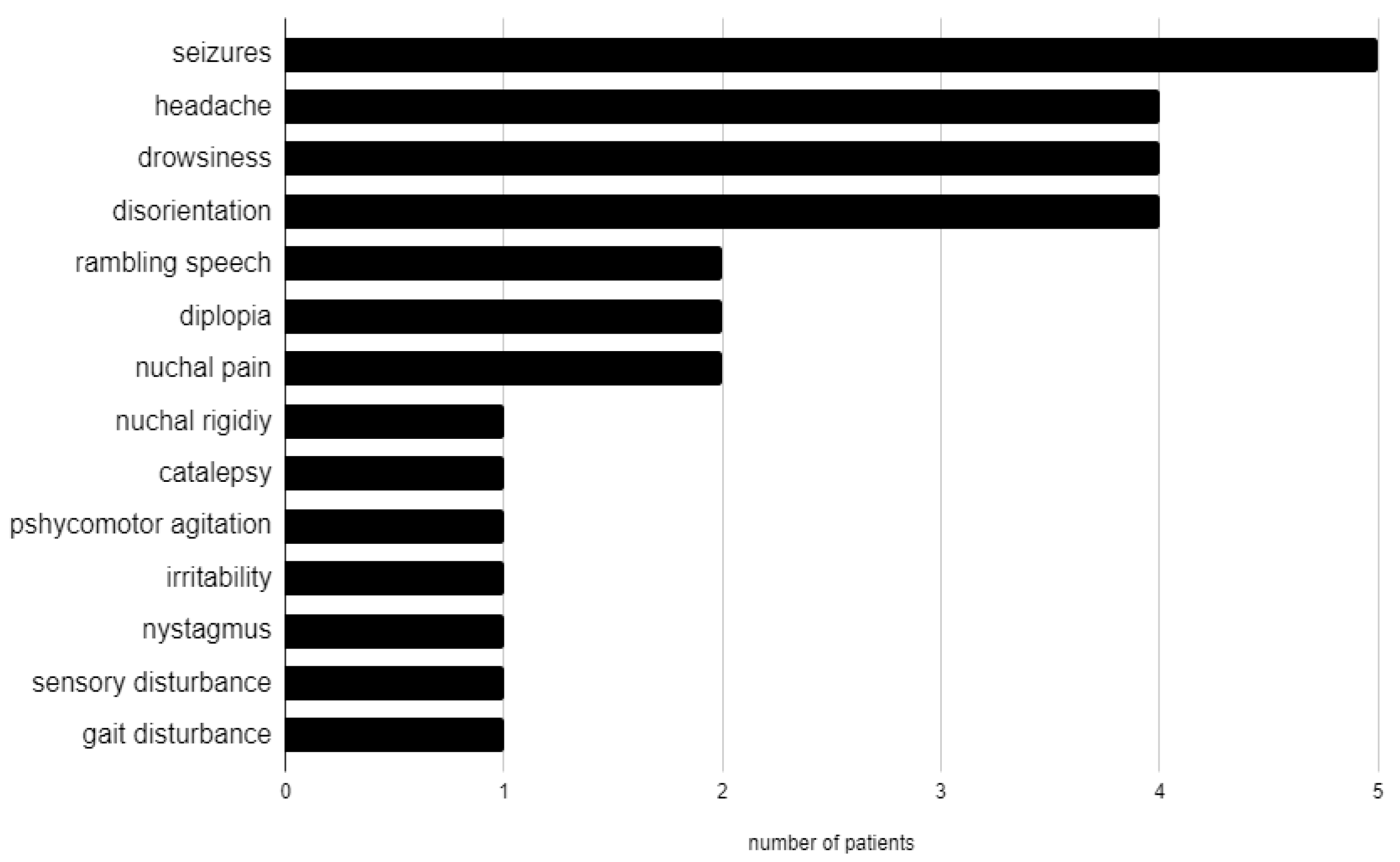
3.3. Neurological Manifestations
3.4. Putative Etiology
3.5. Instrumental Examination
3.6. Treatment and Outcome
4. Discussion
Limitations of the Present Study and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MERS | Mild encephalitis/encephalopathy with reversible splenial lesion |
| MRI | Magnetic Resonance Imaging |
| RESLES | Reversible splenial lesion syndrome |
| CLOCCs | cytotoxic lesions of the corpus callosum |
| SCC | splenium of the corpus callosum |
| DWI | diffusion-weighted imaging |
| ADC | apparent diffusion coefficient |
| FLAIR | fluid-attenuated inversion recovery |
| IVIg | intravenous immunoglobulin |
| MIS-C | Multisystem Inflammatory Syndrome in Children |
| HHV-6 | Human Herpesvirus 6 |
| CSF | cerebrospinal fluid |
| pNf-H | phosphorylated neurofilament heavy chain |
| sMRI | spectroscopic MRI |
References
- Tada, H.; Takanashi, J.; Barkovich, A.J.; Oba, H.; Maeda, M.; Tsukahara, H.; Suzuki, M.; Yamamoto, T.; Shimono, T.; Ichiyama, T.; et al. Clinically Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion. Neurology 2004, 63, 1854–1858. [Google Scholar] [CrossRef]
- Garcia-Monco, J.C.; Cortina, I.E.; Ferreira, E.; Martínez, A.; Ruiz, L.; Cabrera, A.; Beldarrain, M.G. Reversible Splenial Lesion Syndrome (RESLES): What’s in a Name? J. Neuroimaging 2011, 21, e1–e14. [Google Scholar] [CrossRef] [PubMed]
- Aksu Uzunhan, T.; Maraş Genç, H.; Kutlubay, B.; Kalın, S.; Bektaş, G.; Yapıcı, Ö.; Çıracı, S.; Sözen, H.G.; Şevketoğlu, E.; Palabıyık, F.; et al. Cytotoxic Lesions of the Corpus Callosum in Children: Etiology, Clinical and Radiological Features, and Prognosis. Brain Dev. 2021, 43, 919–930. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, M.; Tanabe, T.; Shimakawa, S.; Nakamura, M.; Murata, S.; Shabana, K.; Shinohara, J.; Odanaka, Y.; Matsumura, H.; Maki, K.; et al. Clinico-Radiological Spectrum of Reversible Splenial Lesions in Children. Brain Dev. 2014, 36, 330–336. [Google Scholar] [CrossRef]
- Xue, J.; Zhang, Y.; Kang, J.; Duan, C.; Yi, Z.; Yang, C.; Li, F.; Liu, K.; Song, Z. A Cohort Study of Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion in Children. Brain Behav. 2021, 11, e2306. [Google Scholar] [CrossRef]
- Gómez Iglesias, P.; López Valdés, E.; Vega Bayoll, M.; Gómez Ruíz, M.N. Mild Encephalitis/Encephalopathy with Reversible Splenial Lesion: A Little-Known Entity with Favourable Prognosis. Neurol. Engl. Ed. 2020, 35, 581–583. [Google Scholar] [CrossRef]
- Ka, A.; Britton, P.; Troedson, C.; Webster, R.; Procopis, P.; Ging, J.; Chua, Y.W.; Buckmaster, A.; Wood, N.; Jones, C.; et al. Mild Encephalopathy with Reversible Splenial Lesion: An Important Differential of Encephalitis. Eur. J. Paediatr. Neurol. 2015, 19, 377–382. [Google Scholar] [CrossRef]
- Takanashi, J.; Tada, H.; Maeda, M.; Suzuki, M.; Terada, H.; Barkovich, A.J. Encephalopathy with a Reversible Splenial Lesion Is Associated with Hyponatremia. Brain Dev. 2009, 31, 217–220. [Google Scholar] [CrossRef]
- Gallucci, M.; Limbucci, N.; Paonessa, A.; Caranci, F. Reversible Focal Splenial Lesions. Neuroradiology 2007, 49, 541–544. [Google Scholar] [CrossRef]
- Marsala, S.Z.; Antichi, E.; Pistacchi, M.; Gioulis, M.; Candeago, R.M.; Montemurro, R.T.; Gentile, M.; D’Andrea, P.; Ferracci, F. Mild Encephalitis with a Reversible Splenial Lesion: A Clinical Benign Condition, Often Underrecognized—Clinical Case and Literature Review. J. Neurosci. Rural Pract. 2017, 8, 281–283. [Google Scholar] [CrossRef]
- Ueda, N.; Minami, S.; Akimoto, M. Mycoplasma Pneumoniae-Associated Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion: Report of Two Pediatric Cases and a Comprehensive Literature Review. BMC Infect. Dis. 2016, 16, 671. [Google Scholar] [CrossRef] [PubMed]
- Takanashi, J.; Imamura, A.; Hayakawa, F.; Terada, H. Differences in the Time Course of Splenial and White Matter Lesions in Clinically Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion (MERS). J. Neurol. Sci. 2010, 292, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Fang, Q.; Chen, L.; Chen, Q.; Lin, Z.; Yang, F. Clinically Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion of Corpus Callosum in Chinese Children. Brain Dev. 2017, 39, 321–326. [Google Scholar] [CrossRef]
- Nakata, T.; Natsume, J.; Yamamoto, H.; Ito, Y.; Suzuki, T.; Kawaguchi, M.; Shiraki, A.; Kumai, S.; Sawamura, F.; Suzui, R.; et al. Underlying Disorders in Children with Infection-Related Acute Encephalopathy. Pediatr. Neurol. 2024, 155, 126–132. [Google Scholar] [CrossRef]
- Chen, W.-X.; Liu, H.-S.; Yang, S.-D.; Zeng, S.-H.; Gao, Y.-Y.; Du, Z.-H.; Li, X.-J.; Lin, H.-S.; Liang, H.-C.; Mai, J.-N. Reversible Splenial Lesion Syndrome in Children: Retrospective Study and Summary of Case Series. Brain Dev. 2016, 38, 915–927. [Google Scholar] [CrossRef]
- Qing, Y.; Xiong, W.; Da-xiang, H.; Juan, Z.; Fei, W.; Yong-qiang, Y. Statistical Analysis of the Apparent Diffusion Coefficient in Patients with Clinically Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion Indicates That the Pathology Extends Well beyond the Visible Lesions. Magn. Reson. Med. Sci. 2020, 19, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, M.; Abe, S.; Ikeno, M.; Shima, T.; Shimizu, T.; Okumura, A. A Nationwide Survey of Adenovirus-Associated Encephalitis/Encephalopathy in Japan. Brain Dev. 2024, 46, 10–17. [Google Scholar] [CrossRef]
- Hirayama, Y.; Saito, Y.; Maegaki, Y. “Symptomatic” Infection-Associated Acute Encephalopathy in Children with Underlying Neurological Disorders. Brain Dev. 2017, 39, 243–247. [Google Scholar] [CrossRef]
- Tsubouchi, Y.; Itamura, S.; Saito, Y.; Yamashita, E.; Shinohara, Y.; Okazaki, T.; Ohno, K.; Nishimura, Y.; Oguri, M.; Maegaki, Y. Use of High b Value Diffusion-Weighted Magnetic Resonance Imaging in Acute Encephalopathy/Encephalitis During Childhood. Brain Dev. 2018, 40, 116–125. [Google Scholar] [CrossRef]
- Mizuguchi, M.; Ichiyama, T.; Imataka, G.; Okumura, A.; Goto, T.; Sakuma, H.; Takanashi, J.; Murayama, K.; Yamagata, T.; Yamanouchi, H.; et al. Guidelines for the Diagnosis and Treatment of Acute Encephalopathy in Childhood. Brain Dev. 2021, 43, 2–31. [Google Scholar] [CrossRef]
- Chen, H.; Yu, X.; Chen, Y.; Wu, H.; Wu, Z.; Zhong, J.; Tang, Z. Reversible Splenial Lesion Syndrome in Children: A Retrospective Study of 130 Cases. Front. Neurol. 2023, 14, 1241549. [Google Scholar] [CrossRef] [PubMed]
- Vanderschueren, G.; Schotsmans, K.; Maréchal, E.; Crols, R. Mild Encephalitis with Reversible Splenial (MERS) Lesion Syndrome Due to Influenza B Virus. Pract. Neurol. 2018, 18, 391–392. [Google Scholar] [CrossRef]
- Feraco, P.; Porretti, G.; Marchiò, G.; Bellizzi, M.; Recla, M. Mild Encephalitis/Encephalopathy with Reversible Splenial Lesion (MERS) Due to Cytomegalovirus: Case Report and Review of the Literature. Neuropediatrics 2018, 49, 068–071. [Google Scholar] [CrossRef]
- Bektaş, G.; Akçay, N.; Boydağ, K.; Şevketoğlu, E. Reversible Splenial Lesion Syndrome Associated with SARS-CoV-2 Infection in Two Children. Brain Dev. 2021, 43, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Britton, P.N.; Dale, R.C.; Blyth, C.C.; Macartney, K.; Crawford, N.W.; Marshall, H.; Clark, J.E.; Elliott, E.J.; Webster, R.I.; Cheng, A.C.; et al. Influenza-Associated Encephalitis/Encephalopathy Identified by the Australian Childhood Encephalitis Study 2013–2015. Pediatr. Infect. Dis. J. 2017, 36, 1021–1026. [Google Scholar] [CrossRef]
- Talukder, N.T.; Feezel, A.; Lankford, J.E. Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion Associated with Systemic Mycoplasma Pneumoniae Infection in North America: A Case Report. J. Med. Case Rep. 2022, 16, 74. [Google Scholar] [CrossRef] [PubMed]
- Tuscano, A.; Zoppo, M.; Canavese, C.; Cogoni, M.; Scolfaro, C. Transient Blindness Associated with Mild Encephalitis/Encephalopathy with a Reversible Splenial Lesion (MERS): A Case Report and Review of Literature. Ital. J. Pediatr. 2020, 46, 152. [Google Scholar] [CrossRef]
- Le Soudéer, L.; Truong, J.; Le Gal, J.; Escoda, S. Shigella-Associated Mild Encephalitis with Reversible Splenial Lesion in Hospital Center Delafontaine, Saint-Denis, France: A Case Report. BMC Pediatr. 2022, 22, 421. [Google Scholar] [CrossRef]
- Varol, F.; Ergul, N.; Sahin, E.G.; Can, Y.Y.; Ergul, U.; Guven, S.; Cam, H. Can Plasma Exchange Therapy Be an Option for the Treatment of SARS-CoV-2 Related Splenial Lesion Syndrome: Two Cases from the Pediatric Intensive Care Unit. Transfus. Apher. Sci. 2022, 61, 103491. [Google Scholar] [CrossRef]
- Oger, V.; Bost, C.; Salah, L.; Yazbeck, E.; Maurey, H.; Bellesme, C.; Sevin, C.; Adamsbaum, C.; Chrétien, P.; Benaiteau, M.; et al. Mild Encephalitis/Encephalopathy with Reversible Splenial Lesion Syndrome: An Unusual Presentation of Anti-GFAP Astrocytopathy. Eur. J. Paediatr. Neurol. 2020, 26, 89–91. [Google Scholar] [CrossRef]
- Grosset, L.; Hosseini, H.; Bapst, B.; Hodel, J.; Cleret De Langavant, L.; Faugeras, F.; Bachoud-Lévi, A.-C.; Seddik, L. Mild Encephalopathy with reversible Splenial Lesion: Description of Nine Cases and Review of the Literature. Seizure 2021, 88, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Brar, J.S.S.; Gupta, S.; Mohideen, S.M.H.; Liauw, L.; Lath, N. The Pancreatic and Extrapancreatic Manifestations of IgG4-Related Disease. Diagn. Interv. Radiol. 2019, 24, 83–88. [Google Scholar] [CrossRef]
- Gupte, A.; Sriram, S.; Gunasekaran, V.; Chaudhari, K.; Kamat, D. The Triad of COVID-19 in Children: Acute COVID-19, Multisystem Inflammatory Syndrome, and Long COVID—Part II. Pediatr. Ann. 2025, 54, e40–e44. [Google Scholar] [CrossRef] [PubMed]
- Palabiyik, F.; Akcay, N.; Sevketoglu, E.; Hatipoglu, N.; Sari, E.E.; Inci, E. Imaging of Multisystem Inflammatory Disease in Children (MIS-C) Associated With COVID-19. Acad. Radiol. 2021, 28, 1200–1208. [Google Scholar] [CrossRef]
- Mizuguchi, M.; Yamanouchi, H.; Ichiyama, T.; Shiomi, M. Acute Encephalopathy Associated with Influenza and Other Viral Infections. Acta Neurol. Scand. 2007, 115, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, S.; Matsushige, T.; Inoue, H.; Shirabe, K.; Fukano, R.; Ichiyama, T. Serum and Cerebrospinal Fluid Cytokine Profile of Patients with 2009 Pandemic H1N1 Influenza Virus-Associated Encephalopathy. Cytokine 2011, 54, 167–172. [Google Scholar] [CrossRef]
- Motobayashi, M.; Fukuyama, T.; Okuno-Yuguchi, J.; Tsukahara, K.; Nahaharu, S.; Hagimoto, R.; Kinoshita, T.; Nakazawa, Y.; Inaba, Y. Subclinical neuroaxonal damage in patients with clinically mild encephalitis/encephalopathy with a reversible splenial lesion. Pediatr. Neurol. 2017, 74, e3–e4. [Google Scholar] [CrossRef]
- Ueda, F.; Yoshie, Y.; Aburano, H.; Hashimoto, M.; Matsui, O.; Gabata, T. Splenial and white matter lesions showing transiently-reduced diffusion in mild encephalopathy monitored with MR spectroscopy and imaging. Magn. Reson. Med. Sci. 2014, 13, 271–275. [Google Scholar] [CrossRef]
- Lin, Y.; Yu, C. Reversible Focal Splenium Lesion–MRS Study of a Different Etiology. Acta Neurol. Taiwan 2009, 18, 203–206. [Google Scholar]
- Shimizu, H.; Kataoka, H.; Yagura, H.; Hirano, M.; Taoka, T.; Ueno, S. Extensive neuroimaging of a transient lesion in the splenium of the corpus callosum. Eur. J. Neurol. 2007, 14, e37–e39. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| N° | Age Onset (Y)/ Sex | Pre Existing Illness | Etiology | Prodromal Manifestations | Neurological Manifestation | Na (136–145 mEq/L) | CRP (<0.50 mg/dL) | WBC 103/L (4.00–13.50) | CSF Cell Count | Time to First MRI After the Onset (Days) | Lesion Type (1, 2) | EEG Findings | Treatment | Time to Follow-Up MRI (Days-Months) | Hospital Stay (Days) | Prognosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | 1 y/F | None | Rotavirus, hyponatremia | Vomiting, diarrhea, asthenia | Gait disturbance, seizure | 134 | 0.71 | 14.61 | Normal | 1 | 1 | Normal | Glucoelectrolytic rehydration | NE | 3 | CR |
| 2. | 4 m/F | Aortic coarctation, heart failure | Unknown | None, occasional finding | None | 133 | 0.12 | 8.67 | NE | 70 | 1 | NE | NE | 1 m | 15 | CR |
| 3. | 15 y/F | None | HHV-6; hyponatremia | Fever, vomiting | Headache and psychomotor agitation and drowsiness | 134 | 0.05 | 14.35 | Normal | 5 | 1 | Slow-wave abn with a bilateral fronto-central expression | Glucoelectrolytic rehydration, antibiotics, antivirals, oral NaCl and sodium bicarbonate | 22 d | 63 | CR |
| 4. | 2 y/F | None | Unknown | Lack of appetite and abdominal pain | Drowsiness, non-convulsive status epilepticus | 137 | Unknown | Unknown | Normal | 3 | 1 | Slow BA, slow sharp waves on the posterior leads with a prevalence on the right hemisphere | Antibiotics, corticosteroids, ASM | 7 d | 25 | Movement and speech difficulties |
| 5. | 6 y/M | None | Unknown | Fever | None | 138 | Unknown | Unknown | NE | Unknown | 1 | CT abn predominant on the right hemisphere | NE | NE | 16 | CR |
| 6. | 16 y/M | None | HHV-6 | Asthenia and low-grade fever | Headache, drowsiness and diplopia | 138 | 0.50 | 5.67 | Normal | 2 | 2 | Normal | Antibiotics, IVIg | 3 m | 16 | CR |
| 7. | 4 y/F | None | Unknown | Vomiting, dehydration | Seizure | 136 | 0.50 | 8.75 | Normal | 1 | 1 | Normal | Glucoelectrolytic rehydration, BDZ, ASM | 3 m | 4 | CR |
| 8. | 1 m/F | None | Haemophilus influenzae, hyponatremia | Vomiting, lack of appetite, weight loss | Drowsiness, irritability | 114 | 6.25 | 9.11 | NE | 4 | 1 | NE | Glucoelectrolytic rehydration, antibiotic | 1 m | 25 | CR |
| 9. | 14 y/M | None | Sepsis of suspected meningococcal origin, bacterial meningitis, hypertransaminasemia | Fever, petechiae | Headache, nuchal pain and rigidity | 136 | 28.9 | 20.5 | Normal | 1 | 1 | NE | Glucoelectrolytic rehydration, antibiotics, antivirals, corticosteroids | 3 d | 10 | CR |
| 10. | 5 y/F | None | Hyponatremia | Fever | Seizures | 134 | 18.52 | 12.17 | NE | 3 | 1 | Slow BA | Glucoelectrolytic rehydration, antivirals | NE | 7 | CR |
| 11. | 7 y/F | Coexisting Hemolytic-Uremic Syndrome | E. coli O26, hyponatremia | Diarrhea, fever | Disorientation, diplopia and bilateral nystagmus | 135 | 2.07 | 6.45 | NE | 0 | 1 | Slow BA and slow abn | Immunosuppressant | 2 m | 17 | CR |
| 12. | 14 y/F | Coexisting MIS-C and acute adrenal crisis | MIS-C, hyponatremia | Diarrhea, fever, vomiting, asthenia | Catalepsy | 126 | 37.49 | 14.690 | Normal | 2 | 1 | Diffuse slow abn predominant in the anterior regions | Glucoelectrolytic rehydration, corticosteroids, IVIg | 1 m | 16 | CR |
| 13. | 17 y/M | Sleep disorder, migraine | Unknown | None (occasional finding) | None | 136 | Unknown | Unknown | NE | Unknown | 1 | NE | NE | Unknown | Unknown | CR |
| 14. | 10 y/F | None | Unknown | Fever | Headache and nuchal pain | 136 | Unknwn | Unknown | Normal | Unknown | 1 | Unknown | NE | 1 m | Unknown | CR |
| 15. | 7 y/M | None | Parvovirus B19, hyponatremia | Fever, vomiting | Seizures | 132 | 8.03 | 17.98 | Normal | 1 | 1 | Sporadic slow waves in the left centro-parietal region | IVIg | 4 m | 4 | CR |
| 16. | 9 y/M | None | MIS-C, hyponatremia | Fever, vomiting, conjunctivitis and skin rash | Sensory disturbance | 126 | 16.62 | 5.06 | NE | 1 | 1 | Slow BA | IVIg, corticosteroids, immunosuppressant | NE | 19 | CR |
| 17. | 8 y/M | None | Rotavirus, hyponatremia | Diarrhea, fever | Disorientation and poorly reactive | 130 | 0.88 | 12.6 | NE | 1 | 1 | Normal | Glucoelectrolytic rehydration | 3 m | Unknown | CR |
| 18. | 8 y/F | None | Rotavirus, hyponatremia | Diarrhea, fever, vomiting, lack of appetite, weight loss | Disorientation, rambling speech | 122 | 9.08 | 11.0 | NE | 1 | 1 | Slow abn on the frontotemporal regions bilaterally | Glucoelectrolytic rehydration | NE | Unknown | CR |
| 19. | 8 y/M | None | Rotavirus, hyponatremia | Diarrhea, fever, vomiting, lack of appetite | Disorientation, rambling speech | 127 | 7.52 | 8.4 | Normal | 1 | 1 | Normal | Glucoelectrolytic rehydration | 4 m | Unknown | CR |
| Pathogen Infection | Data n | % |
| Rotavirus | 4/10 | 40 |
| HHV-6 | 2/10 | 20 |
| Parvovirus B19 | 1/10 | 10 |
| E. coli | 1/10 | 10 |
| H. Influenzae | 1/10 | 10 |
| Meningococcus | 1/10 | 10 |
| Noninfectious causes | Data n | % |
| Hyponatriemia | 12/19 | 63 |
| MIS-C | 2/19 | 11 |
| Treatment | Data n | % | Posology |
|---|---|---|---|
| Glucoelectrolytic rehydration | 10/19 | 53 | Hollyday-Segar Formula |
| Antibiotics | 5/19 | 26 | Weight-based |
| IVIg | 4/19 | 21 | A single dose of 2 g/kg |
| Corticosteroids | 4/19 | 21 | Weight-based |
| Antiviral drugs | 3/19 | 16 | Weight-based |
| Immunosuppresant drugs | 2/19 | 11 | Weight-based |
| Antiepileptic medications | 2/19 | 11 | Weight-based |
| No treatment | 5/19 | 26 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeo, M.; Polselli, M.; Mantero, V.; Moavero, R.; Mazzone, L.; Valeriani, M. Clinical Variability of Pediatric MERS: Insights from a Retrospective Observational Study. J. Clin. Med. 2025, 14, 4169. https://doi.org/10.3390/jcm14124169
Romeo M, Polselli M, Mantero V, Moavero R, Mazzone L, Valeriani M. Clinical Variability of Pediatric MERS: Insights from a Retrospective Observational Study. Journal of Clinical Medicine. 2025; 14(12):4169. https://doi.org/10.3390/jcm14124169
Chicago/Turabian StyleRomeo, Mariaelena, Maria Polselli, Vittorio Mantero, Romina Moavero, Luigi Mazzone, and Massimiliano Valeriani. 2025. "Clinical Variability of Pediatric MERS: Insights from a Retrospective Observational Study" Journal of Clinical Medicine 14, no. 12: 4169. https://doi.org/10.3390/jcm14124169
APA StyleRomeo, M., Polselli, M., Mantero, V., Moavero, R., Mazzone, L., & Valeriani, M. (2025). Clinical Variability of Pediatric MERS: Insights from a Retrospective Observational Study. Journal of Clinical Medicine, 14(12), 4169. https://doi.org/10.3390/jcm14124169