
The Effectiveness of Sacubitril/Valsartan in Systemic Sclerosis Patients with Heart Failure: A Retrospective Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Cohort Selection and Characteristics
3.2. Demographics and Baseline Clinical Characteristics
3.3. Functional, Laboratory, and Hemodynamic Outcomes
3.4. Subgroup Comparison by SSc Phenotype
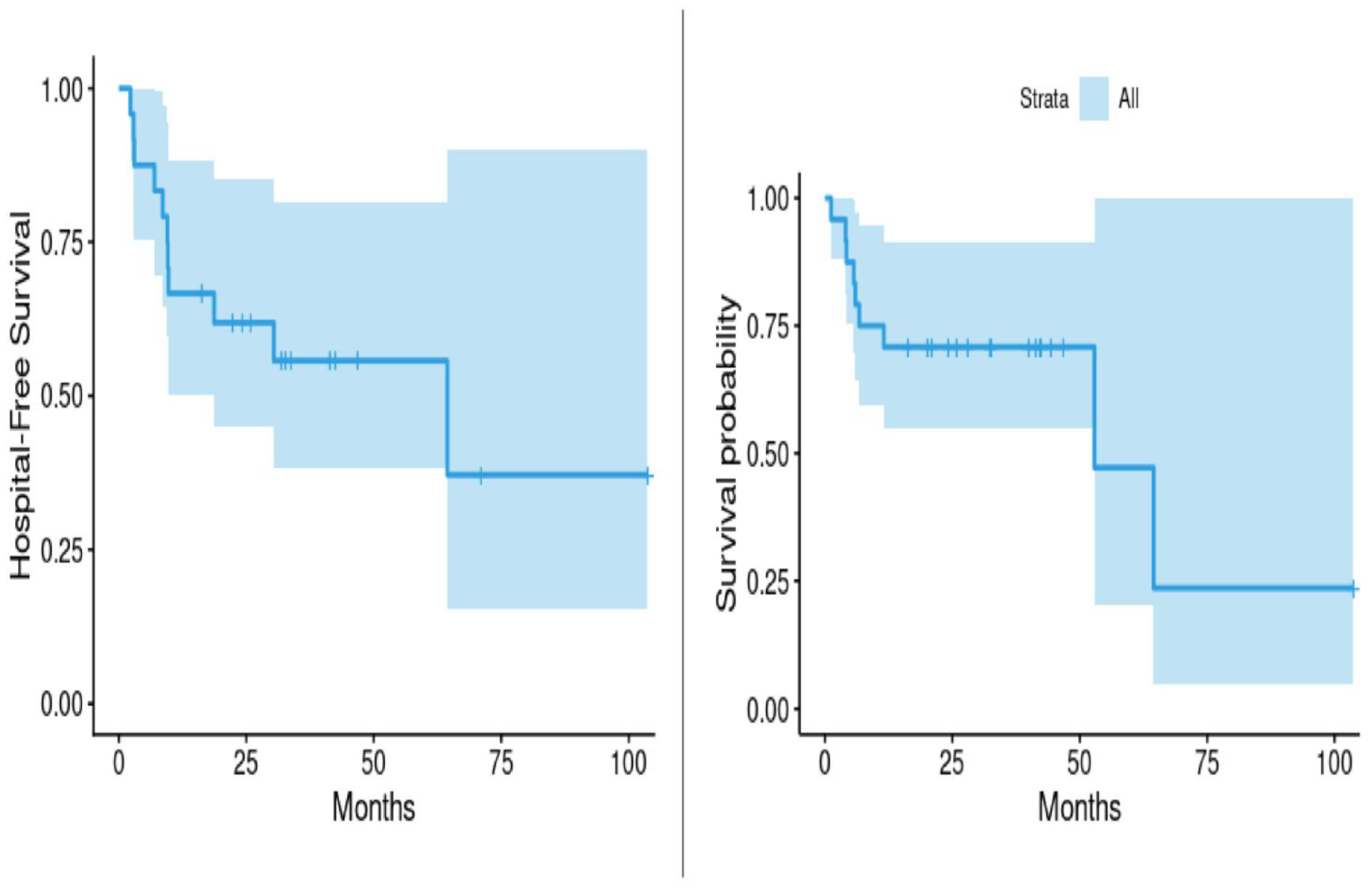
3.5. Survival Time and Hospitalization
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SSc | Systemic Sclerosis |
| SV | Sacubitril/Valsartan |
| HFrEF | Heart Failure with Reduced Ejection Fraction |
| CMR | Cardiac Magnetic Resonance Imaging |
| ARNI | Angiotensin Receptor–Neprilysin Inhibitor |
| NT-proBNP | N-Terminal Pro-B-Type Natriuretic Peptide |
| LVEF | Left Ventricular Ejection Fraction |
| NYHA | New York Heart Association |
| REDCap | Research Electronic Data Capture |
| ICD | International Classification of Diseases |
| ACR/EULAR | American College of Rheumatology/European Alliance of Associations for Rheumatology |
| SD | Standard Deviation |
| HFpEF | Heart Failure with Preserved Ejection Fraction |
| RVSP | Right Ventricular Systolic Pressure |
| LA | Left Atrium |
| RA | Right Atrium |
| LVESV | Left Ventricular End-Systolic Volume |
| LVESD | Left Ventricular End-Systolic Dimension |
| LVEDV | Left Ventricular End-Diastolic Volume |
| LVEDD | Left Ventricular End-Diastolic Dimension |
| TAPSE | Tricuspid Annular Plane Systolic Excursion |
| LVOT | Left Ventricular Outflow Tract |
| mPAP | Mean Pulmonary Arterial Pressure |
| FDA | Food and Drug Administration |
| GDMT | Guideline-Directed Medical Therapy |
| SRC | Scleroderma Renal Crisis |
| RP | Raynaud’s Phenomenon |
| PAH | Pulmonary Arterial Hypertension |
| CI | Confidence Interval |
| pg/mL | Picograms per Milliliter |
| mg/dL | Milligrams per Deciliter |
| L/min | Liters per Minute |
| mL/m2 | Milliliters per Square Meter |
| mmHg | Millimeters of Mercury |
References
- Jerjen, R.; Nikpour, M.; Krieg, T.; Denton, C.P.; Saracino, A.M. Systemic sclerosis in adults. Part I: Clinical features and pathogenesis. J. Am. Acad. Dermatol. 2022, 87, 937–954. [Google Scholar] [CrossRef] [PubMed]
- Fairley, J.L.; Ross, L.; Nikpour, M. Heart involvement in systemic sclerosis: Emerging concepts. Curr. Opin. Rheumatol. 2024, 36, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Nadel, A.; Nadel, M.; Taborska, N.; Stępień, B.; Gajdecki, J.; Brzezińska, O.; Opinc-Rosiak, A.; Makowska, J.; Lewandowska-Polak, A. Heart involvement in patients with systemic sclerosis—What have we learned about it in the last 5 years. Rheumatol. Int. 2024, 44, 1823–1836. [Google Scholar] [CrossRef] [PubMed]
- Moysidou, G.-S.; Dara, A.; Arvanitaki, A.; Skalkou, A.; Pagkopoulou, E.; Daoussis, D.; Kitas, G.D.; Dimitroulas, T. Understanding and managing cardiac involvement in systemic sclerosis. Expert Rev. Clin. Immunol. 2023, 19, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Guédon, A.F.; Carrat, F.; Mouthon, L.; Launay, D.; Chaigne, B.; Pugnet, G.; Lega, J.-C.; Hot, A.; Cottin, V.; Agard, C. Heart and systemic sclerosis—Findings from a national cohort study. Rheumatology 2024, 63, 3380–3389. [Google Scholar] [CrossRef] [PubMed]
- Asano, Y.; Jinnin, M.; Kawaguchi, Y.; Kuwana, M.; Goto, D.; Sato, S.; Takehara, K.; Hatano, M.; Fujimoto, M.; Mugii, N. Diagnostic criteria, severity classification and guidelines of systemic sclerosis. J. Dermatol. 2018, 45, 633–691. [Google Scholar] [CrossRef] [PubMed]
- Chhikara, S.; Kanda, A.; Ogugua, F.M.; Rouf, R.; Nouraee, C.; Bawaskar, P.; Molitor, J.A.; Shenoy, C. The primary cardiomyopathy of systemic sclerosis on cardiovascular magnetic resonance imaging. Eur. Heart J.-Cardiovasc. Imaging 2023, 24, 1661–1671. [Google Scholar] [CrossRef] [PubMed]
- Györfi, A.H.; Filla, T.; Polzin, A.; Tascilar, K.; Buch, M.; Tröbs, M.; Matei, A.E.; Airo, P.; Balbir-Gurman, A.; Kuwert, F. Evaluation of systemic sclerosis primary heart involvement and chronic heart failure in the European scleroderma trials and research cohort. J. Am. Heart Assoc. 2025, 14, e036730. [Google Scholar] [CrossRef] [PubMed]
- Gotschy, A.; Jordan, S.; Stoeck, C.T.; von Deuster, C.; Peer, T.; Gastl, M.; Vishnevskiy, V.; Wissmann, L.; Dobrota, R.; Mihai, C. Diffuse myocardial fibrosis precedes subclinical functional myocardial impairment and provides prognostic information in systemic sclerosis. Eur. Heart J.-Cardiovasc. Imaging 2023, 24, 373–382. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.J.; Yang, C.G.; Qiao, W.B.; Liu, Y.C.; Liu, S.Y.; Dong, G.J. Sacubitril/valsartan attenuates myocardial inflammation, hypertrophy, and fibrosis in rats with heart failure with preserved ejection fraction. Eur. J. Pharmacol. 2023, 961, 176170. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, H.E.; Askar, M.E.; Shaheen, M.A.; Baraka, N.M.; Mahmoud, Y.K. Sacubitril/valsartan alleviates sunitinib-induced cardiac fibrosis and oxidative stress via improving TXNIP/TRX system and downregulation of NF-ĸB/Wnt/β-catenin/SOX9 signaling. Int. Immunopharmacol. 2024, 132, 111963. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, N.H.; Jalil, J.; Zainalabidin, S.; Saleh, M.S.; Asmadi, A.Y.; Kamisah, Y. Molecular mechanisms of sacubitril/valsartan in cardiac remodeling. Front. Pharmacol. 2022, 13, 892460. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Lai, J.; Zhou, J.; Hou, Y.; Xu, D.; Li, M.; Zeng, X. The clinical characteristics and outcomes of patients with systemic sclerosis with myocardial involvement. Orphanet J. Rare Dis. 2023, 18, 83. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M. Association of change in N-terminal pro–B-type natriuretic peptide following initiation of sacubitril-valsartan treatment with cardiac structure and function in patients with heart failure with reduced ejection fraction. Jama 2019, 322, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Menendez, J.T. The mechanism of action of LCZ696. Card. Fail. Rev. 2016, 2, 40. [Google Scholar] [CrossRef] [PubMed]
- Öz, T.K.; Abdelnabi, M.; Fiore, C.; Almaghraby, A.; Cihan, D.; Babazade, N.; Omar, B.; Dağdeviren, B. Assessment of sacubitril/valsartan effects on left ventricular dynamics using 3D echocardiography and 3D strain in heart failure with reduced ejection fraction patients. Minerva Cardiol. Angiol. 2021, 70, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Codina, P.; Domingo, M.; Barceló, E.; Gastelurrutia, P.; Casquete, D.; Vila, J.; Abdul-Jawad Altisent, O.; Spitaleri, G.; Cediel, G.; Santiago-Vacas, E. Sacubitril/valsartan affects pulmonary arterial pressure in heart failure with preserved ejection fraction and pulmonary hypertension. ESC Heart Fail. 2022, 9, 2170–2180. [Google Scholar] [CrossRef] [PubMed]
- Spannella, F.; Giulietti, F.; Filipponi, A.; Sarzani, R. Effect of sacubitril/valsartan on renal function: A systematic review and meta-analysis of randomized controlled trials. ESC Heart Fail. 2020, 7, 3487–3496. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Baseline Characteristics | All Patients (N = 24) | |||||
|---|---|---|---|---|---|---|
| Female Gender | 18 (75%) | |||||
| Age at diagnosis (y); mean (SD) | 53 (13) | |||||
| Disease duration prior to S/V use (y); mean (SD) | 6.8 (5.6) | |||||
| Scleroderma phenotype: | N = 23 | |||||
| 11 (45%) | |||||
| 9 (37%) | |||||
| 1 (4%) | |||||
| 2 (8%) | |||||
| Duration of SV use (months); mean (SD) | 20.6 (20) | |||||
| Indication for use: | ||||||
| 21 (87.5%) | |||||
| 3 (12.5%) | |||||
| Heart failure etiology | ||||||
| 3(12.5%) | |||||
| 21(87.5%) | |||||
| S/V discontinued | 6 (25%) | |||||
| Reason for discontinuation: | N = 6 | |||||
| 4 (16%) | |||||
| 2 (8%) | |||||
| S/V dosage: | ||||||
| 17 (70.8%) | |||||
| 4 (16.7%) | |||||
| 3 (12.5%) | |||||
| Clinical, Lab, and Echocardiogram Data at Baseline and Follow-up | ||||||
| N | Baseline | Follow-up | Δ | 95% CI | p-value | |
| Systolic blood pressure (mmHg); mean (SD) | 22 | 128(20) | 114(18) | −14(13) | (−20.1, −8.4) | <0.001 |
| LVEF (%); mean (SD) | 19 | 40.3(12.8) | 47.7 (9.6) | 7.4 (11.9) | (1.7, 13.2) | 0.014 |
| RVSP (mmHg); mean (SD) | 11 | 41.2 (10.5) | 37.3 (9.8) | −3.9 (9.5) | (−10.2, 2.5) | 0.202 |
| NT-ProBNP; mean (SD) | 14 | 15,130.1 (23,394.3) | 5082.4 (9221.8) | −10,047.7 (17,001.6) | (−19,864.1, −231.3) | 0.046 |
| Creatinine (mg/dL); mean (SD) | 21 | 1.9 (3.6) | 1.3 (0.9) | 0.138 (0.306) | (−0.045, 0.260) | 0.057 |
| Clinical outcomes | ||||||
| Time to hospitalization (months); median | 64.4 | |||||
| Survival time (months); median | 52.9 | |||||
| N | Baseline | Follow-Up | Δ | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Clinical Parameters | ||||||
| Systolic Blood Pressure (mmHg); mean (SD) | 22 | 128 (20) | 114 (18) | −14 (13) | (−20.1, −8.4) | <0.001 |
| TTE Parameters | ||||||
| LVEF (%); mean (SD) | 19 | 40.3(12.8) | 47.7 (9.6) | 7.4 (11.9) | (1.7, 13.2) | 0.014 |
| LVESV (mL) | 8 | 83.8 (41.1) | 73.4 (41.1) | −10.4 (16.7) | (−24.3, 3.6) | 0.123 |
| LVESD (mm) | 13 | 39.5 (6.7) | 38 (7.2) | −1.5 (4.3) | (−4.1, 1.2) | 0.247 |
| LVEDV (mL) | 8 | 130.3 (50.9) | 124.5 (47.7) | −5.8 (29.9) | (−30.8, 19.3) | 0.604 |
| LVEDD (mm) | 16 | 50.4 (6.7) | 49.6 (6.4) | −0.8 (6) | (−3.9, 2.4) | 0.622 |
| LA Biplane Max Volume (mL) | 4 | 76.3 (19.8) | 70.3 (24.1) | −6 (8.1) | (−18.9, 6.9) | 0.234 |
| LA Biplane Volume Index; mean (mL/m2) | 6 | 37.4 (7.1) | 36 (9.6) | −1.4 (5.9) | (−7.6, 4.8) | 0.59 |
| RVSP (mmHg); mean (SD) | 11 | 41.2 (10.5) | 37.3 (9.8) | −3.9 (9.5) | (−10.2, 2.5) | 0.202 |
| RA Basal; mean (mm) | 5 | 41.4 (9.6) | 39.6 (10.9) | −1.8 (5.8) | (−9.0, 5.4) | 0.523 |
| RA Mid; mean (mm) | 4 | 28.8 (9.9) | 29.8 (13.5) | 1 (9.1) | (−13.5, 15.5) | 0.841 |
| RV Base-Apex Length (mm) | 2 | 72.5 (12) | 70.5 (12) | −2 (24) | (−218, 214) | 0.925 |
| TAPSE; mean (cm) | 6 | 1.9 (0.4) | 1.7 (0.5) | −0.2 (0.4) | (−0.6, 0.2) | 0.239 |
| Tricuspid Regurgitant Velocity; mean (m/s) | 6 | 2.8 (0.4) | 2.8 (0.5) | 0 (0.3) | (−0.3, 0.3) | 1.000 |
| LVOT Cardiac Output; mean (L/min) | 8 | 4 (1.3) | 4.5 (1.2) | 0.4 (1.6) | (−0.9, 1.8) | 0.477 |
| LVOT Cardiac Index (L/min/m2) | 8 | 2.2 (0.7) | 2.4 (0.5) | 0.2 (0.7) | (−0.4, 0.8) | 0.435 |
| Stroke Volume (mL) | 9 | 57.2 (15) | 66.8 (20.2) | 9.6 (27.7) | (−11.8, 30.9) | 0.332 |
| Stroke Volume Index (mL/m2) | 9 | 32.7 (7.7) | 37.9 (9.9) | 5.2 (14.3) | (−5.7, 16.2) | 0.304 |
| Labs | ||||||
| NT-ProBNP; mean (SD) | 14 | 15,130.1 (23,394.3) | 5082.4 (9221.8) | −10,047.7 (17,001.6) | (−19,864.1, −231.3) | 0.046 |
| Creatinine (mg/dL); mean (SD) | 21 | 1.9 (3.6) | 1.3 (0.9) | 0.138 (0.306) | (−0.045, 0.260) | 0.057 |
| Clinical Outcomes | ||||||
| Time to Hospitalization (months); median | 64.4 | |||||
| Survival Time (months); median | 52.9 | |||||
| Diffuse Scleroderma (N = 9) | Limited Scleroderma (N = 11) | 95% CI | p-Value | |
|---|---|---|---|---|
| Female gender | 6 (66.7%) | 8 (72.7%) | 0.769 | |
| Age at diagnosis (y); mean (SD) | 52 (19.2) | 54.9 (10.9) | (−13.9, 19.7) | 0.680 |
| Duration of S/V use; mean (SD) | 14.3 (15.7) | 19.1 (16.6) | (−11.9, 21.5) | 0.549 |
| S/V discontinued | 2 (22.2%) | 4 (36.4%) | 0.492 | |
| Baseline LVEF (%); mean (SD) | (N = 8) | (N = 7) | ||
| 33 (9.2) | 45.4 (14.1) | (−1.4, 26.3) | 0.061 | |
| Follow-up LVEF (%); mean (SD) | (N = 8) | (N = 7) | ||
| 43.5 (9.6) | 51 (10.1) | (−3.5, 18.5) | 0.163 | |
| 5-year survival events (N) | (6) | (6) | ||
| 44.4% | 36.4% | 0.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eshak, N.; Abdelnabi, M.; Quillen, J.; Pham, M.; Hentz, J.; Nagaraja, V. The Effectiveness of Sacubitril/Valsartan in Systemic Sclerosis Patients with Heart Failure: A Retrospective Analysis. J. Clin. Med. 2025, 14, 4054. https://doi.org/10.3390/jcm14124054
Eshak N, Abdelnabi M, Quillen J, Pham M, Hentz J, Nagaraja V. The Effectiveness of Sacubitril/Valsartan in Systemic Sclerosis Patients with Heart Failure: A Retrospective Analysis. Journal of Clinical Medicine. 2025; 14(12):4054. https://doi.org/10.3390/jcm14124054
Chicago/Turabian StyleEshak, Nouran, Mahmoud Abdelnabi, Jaxon Quillen, Micheal Pham, Joseph Hentz, and Vivek Nagaraja. 2025. "The Effectiveness of Sacubitril/Valsartan in Systemic Sclerosis Patients with Heart Failure: A Retrospective Analysis" Journal of Clinical Medicine 14, no. 12: 4054. https://doi.org/10.3390/jcm14124054
APA StyleEshak, N., Abdelnabi, M., Quillen, J., Pham, M., Hentz, J., & Nagaraja, V. (2025). The Effectiveness of Sacubitril/Valsartan in Systemic Sclerosis Patients with Heart Failure: A Retrospective Analysis. Journal of Clinical Medicine, 14(12), 4054. https://doi.org/10.3390/jcm14124054