
Antiplatelet Treatment Strategy in MINOCA Patients: Predictors of Decision Making in Clinical Practice and Prognostic Implications

 ,
,  , , , , , , ,
, , , , , , , 
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Aim and Design
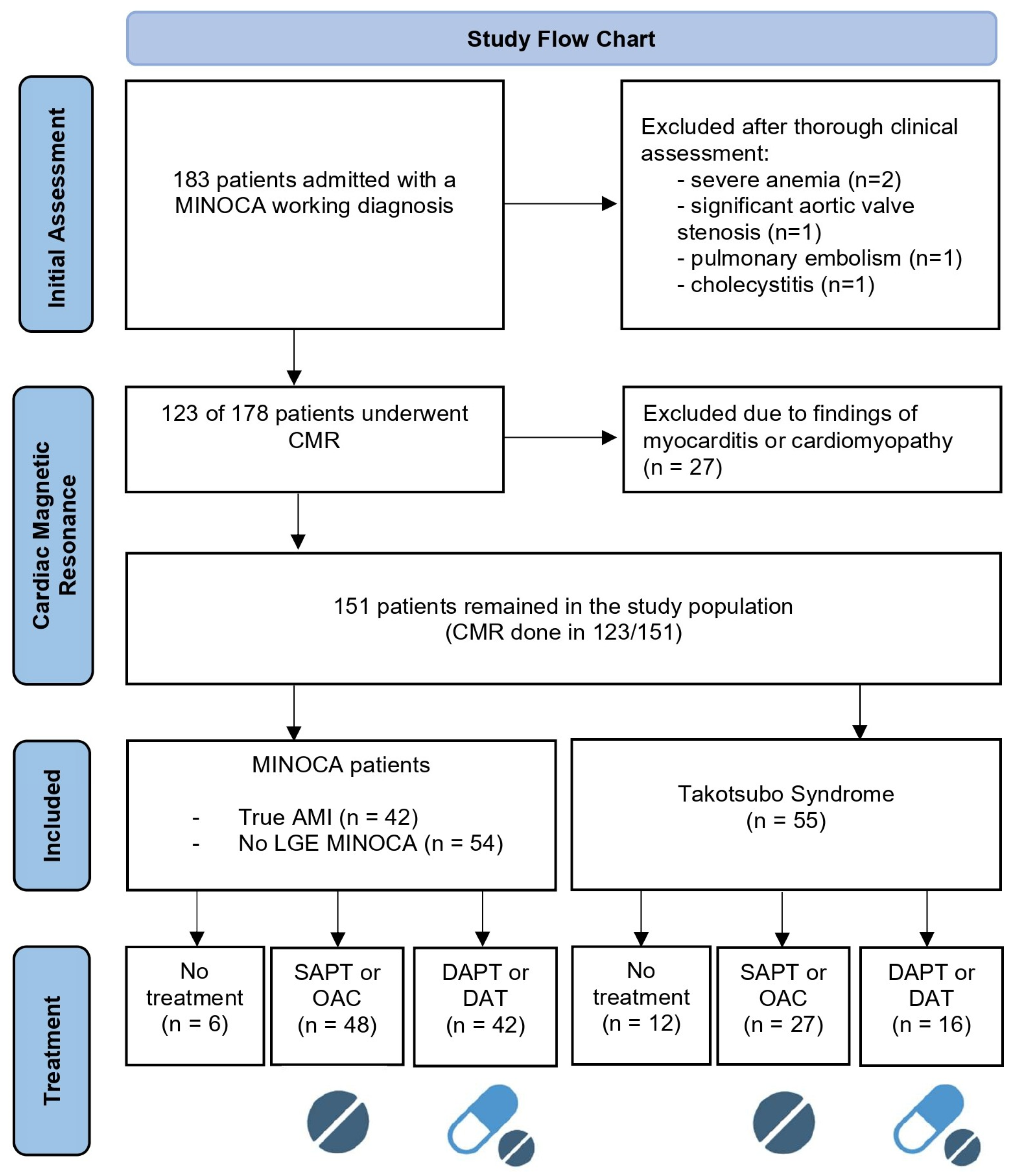
2.2. Study Population
2.3. Ethics
2.4. Study Protocol
2.4.1. Baseline Data Collection
- No antithrombotic therapy.
- Single antiplatelet therapy (SAPT) or oral anticoagulants (OACs): use of single antiplatelet therapy (aspirin) or ONLY an anticoagulant (usually in the context of atrial fibrillation).
- Dual antiplatelet therapy (DAPT), or a combination of one antiplatelet with one anticoagulant—dual antithrombotic therapy (DAT), or a combination of two antiplatelets with one anticoagulant—triple antithrombotic therapy (TAT). In the present study, there were no patients receiving TAT.
2.4.2. Follow-Up Period
2.4.3. Endpoint Definition
- Hospitalization for new ACS (NSTEMI/STEMI/Unstable Angina) or need for revascularization.
- Hospitalization for heart failure.
- Hospitalization for stroke (confirmed by imaging).
- Hospitalization for clinically significant arrhythmia (including atrial fibrillation, ventricular tachycardia/need for implantable defibrillator, or conduction disturbance requiring pacemaker implantation).
- Cardiovascular and all cause death.
- Composite outcome of cardiovascular morbidity and/or mortality.
2.5. Statistics
3. Results
3.1. Patient Characteristics
3.2. Antithrombotic Treatment Strategy
3.2.1. Predictors for Decision Making
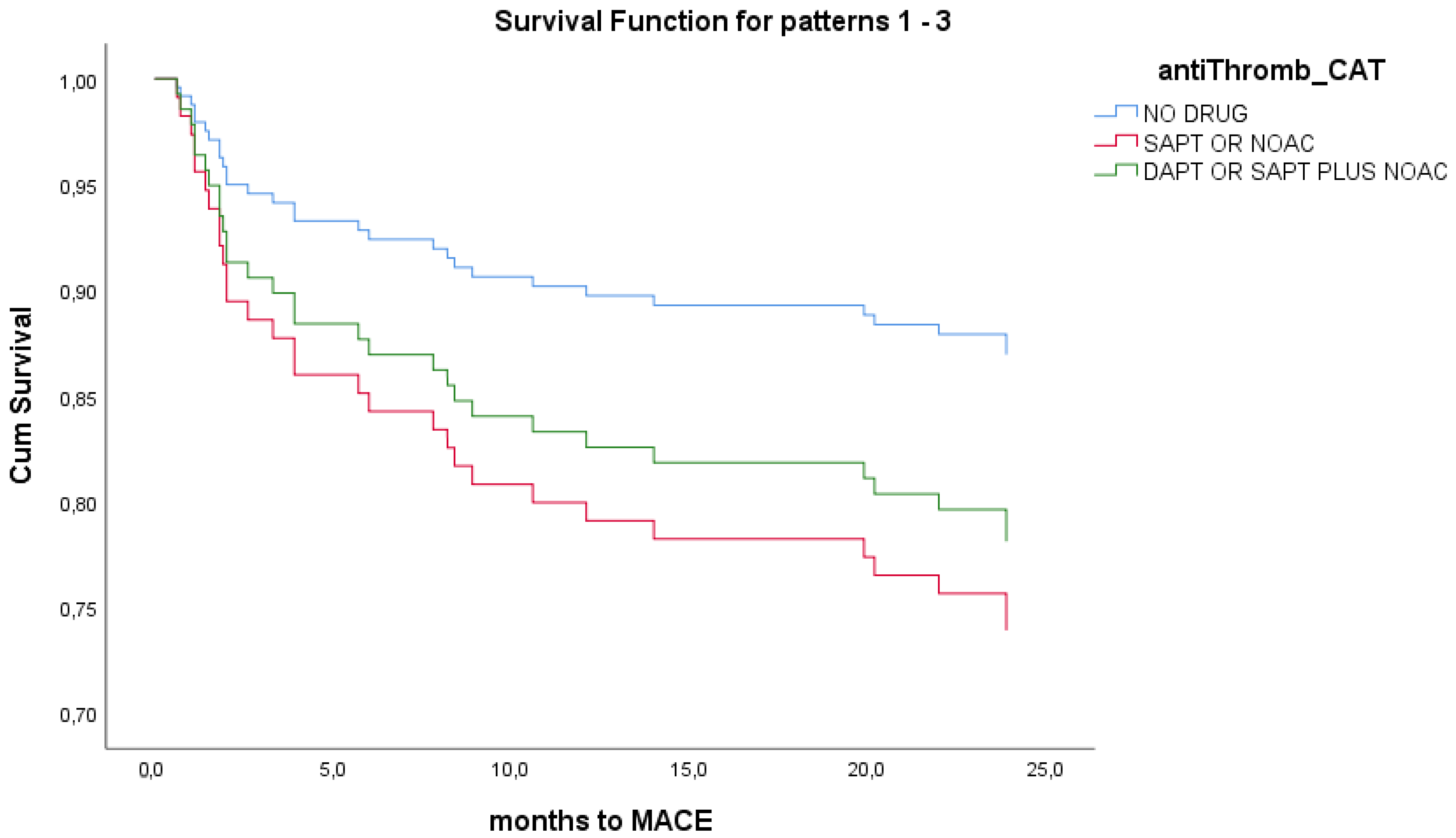
3.2.2. Prognostic Significance Analysis for Antithrombotic Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MINOCA | Myocardial Infarction with Non-Obstructive Coronary Arteries |
| CMR | Cardiac Magnetic Resonance |
| LGE | Late Gadolinium Enhancement |
| AMI | Acute Myocardial Infarction |
| TTS | Takotsubo Syndrome |
| DAPT | Dual Antiplatelet Therapy |
| DAT | Dual Antithrombotic Therapy |
| SAPT | Single Antiplatelet Therapy |
| OAC | Oral Anticoagulant |
| ACS | Acute Coronary Syndrome |
| RCT | Randomized Clinical Trial |
| CAD | Coronary Artery Disease |
| SCAD | Spontaneous Coronary Artery Dissection |
| OCT | Optical Coherence Tomography |
| IVUS | Intravascular Ultrasound |
| CCU | Coronary Care Unit |
| CRF | Case Report Form |
| eGFR | Estimated Glomerular Filtration Rate |
| CRP | C-Reactive Protein |
| MACEs | Major Adverse Cardiovascular Events |
| NSTEMI | Non-ST Elevation Myocardial Infarction |
| STEMI | ST Elevation Myocardial Infarction |
| UA | Unstable Angina |
| ICD | Implantable Cardioverter Defibrillator |
| HF | Heart Failure |
| AF | Atrial Fibrillation |
| BMI | Body Mass Index |
| HTN | Hypertension |
| DM | Diabetes Mellitus |
| CKD | Chronic Kidney Disease |
| NT-proBNP | N-terminal pro b-type Natriuretic Peptide |
| LVEF | Left Ventricular Ejection Fraction |
| FFR | Fractional Flow Reserve |
| PCI | Percutaneous Coronary Intervention |
| DCB | Drug-Coated Balloon |
| BRS | Bioresorbable Scaffold |
| INOCA | Ischemia with Non-Obstructive Coronary Arteries |
References
- Pasupathy, S.; Tavella, R.; McRae, S.; Beltrame, J.F. Myocardial Infarction with Non-obstructive Coronary Arteries—Diagnosis and Management. Eur. Cardiol. Rev. 2015, 10, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients with Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.P.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur. Heart J. 2017, 38, 143–153. [Google Scholar] [CrossRef]
- Ceasovschih, A.; Mantzouranis, E.; Dimitriadis, K.; Sorodoc, V.; Vlachakis, P.K.; Karanikola, A.E.; Theofilis, P.; Koutsopoulos, G.; Drogkaris, S.; Andrikou, I.; et al. Coronary artery thromboembolism as a cause of myocardial infarction with non-obstructive coronary arteries (MINOCA). Hell. J. Cardiol. 2024, 79, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Citro, R.; Okura, H.; Ghadri, J.R.; Izumi, C.; Meimoun, P.; Izumo, M.; Dawson, D.; Kaji, S.; Eitel, I.; Kagiyama, N.; et al. Multimodality imaging in takotsubo syndrome: A joint consensus document of the European Association of Cardiovascular Imaging (EACVI) and the Japanese Society of Echocardiography (JSE). Eur. Heart J.-Cardiovasc. Imaging 2020, 21, 1184–1207. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; Servi, S.D.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, J.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Vlachakis, P.K.; Varlamos, C.; Benetou, D.R.; Kanakakis, I.; Alexopoulos, D. Periprocedural Antithrombotic Treatment in Complex Percutaneous Coronary Intervention. J. Cardiovasc. Pharmacol. 2022, 79, 407–419. [Google Scholar] [CrossRef]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjöld, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients with Myocardial Infarction with Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Galli, M.; Capodanno, D.; Brugaletta, S.; Angiolillo, D.J. The Role of Antiplatelet Therapy in Patients with MINOCA. Front. Cardiovasc. Med. 2022, 8, 821297. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management. Eur. Heart J. 2018, 39, 2047–2062. [Google Scholar] [CrossRef] [PubMed]
- Leontsinis, I.; Mantzouranis, E.; Sakalidis, A.; Ntalakouras, I.; Dri, I.; Soulaidopoulos, S.; Vlachakis, P.K.; Palkopoulou, M.; Fragoulis, C.; Kasiakogias, A.; et al. Recent Advancements and Persistent Challenges in the Management of Patients with Takotsubo Syndrome. Int. J. Clin. Med. Educ. Res. 2025, 4, 1–11. [Google Scholar] [CrossRef]
- Ferreira, V.M. CMR Should Be a Mandatory Test in the Contemporary Evaluation of “MINOCA”. JACC Cardiovasc. Imaging 2019, 12, 1983–1986. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.; Bisaccia, G.; Leo, I.; Williams, M.G.L.; Dastidar, A.; Strange, J.W.; Sammut, E.; Johnson, T.W.; Bucciarelli-Ducci, C. CMR reclassifies the majority of patients with suspected MINOCA and non MINOCA. Eur. Heart J.-Cardiovasc. Imaging 2023, 25, 8–15. [Google Scholar] [CrossRef]
- Reynolds, H.R. Searching for Underlying Causes of MINOCA with Multi-Modality Imaging. JACC Cardiovasc. Imaging 2020, 13, 2632–2634. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Maehara, A.; Kwong, R.Y.; Sedlak, T.; Saw, J.; Smilowitz, N.R.; Mahmud, E.; Wei, J.; Marzo, K.; Matsumura, M.; et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction with Nonobstructive Coronary Arteries in Women. Circulation 2021, 143, 624–640. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Cammann, V.L.; Jurisic, S.; Seifert, B.; Napp, L.C.; Diekmann, J.; Bataiosu, D.R.; D’Ascenzo, F.; Ding, K.J.; Sarcon, A.; et al. A novel clinical score (InterTAK Diagnostic Score) to differentiate takotsubo syndrome from acute coronary syndrome: Results from the International Takotsubo Registry. Eur. J. Heart Fail. 2017, 19, 1036–1042. [Google Scholar] [CrossRef]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, J.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sörensson, P.; Ekenbäck, C.; Lundin, M.; Agewall, S.; Bacsovics Brolin, E.; Caidahl, K.; Cederlund, K.; Collste, O.; Daniel, M.; Jensen, J.; et al. Early Comprehensive Cardiovascular Magnetic Resonance Imaging in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries. JACC Cardiovasc. Imaging 2021, 14, 1774–1783. [Google Scholar] [CrossRef]
- Park, S.J.; Ahn, J.M.; Kang, D.Y.; Yun, S.C.; Ahn, Y.K.; Kim, W.J.; Nam, C.W.; Jeong, J.O.; Chae, I.H.; Shiomi, H.; et al. Preventive percutaneous coronary intervention versus optimal medical therapy alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT): A multicentre, open-label, randomised controlled trial. Lancet 2024, 403, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Montone, R.A.; Cosentino, N.; Graziani, F.; Gorla, R.; Del Buono, M.G.; La Vecchia, G.; Rinaldi, R.; Marenzi, G.; Bartorelli, A.L.; Marco, F.D.; et al. Precision medicine versus standard of care for patients with myocardial infarction with non-obstructive coronary arteries (MINOCA): Rationale and design of the multicentre, randomised PROMISE trial. EuroIntervention 2022, 18, e933–e939. [Google Scholar] [CrossRef]
- Dimitriadis, K.; Pyrpyris, N.; Theofilis, P.; Mantzouranis, E.; Beneki, E.; Kostakis, P.; Koutsopoulos, G.; Aznaouridis, K.; Aggeli, K.; Tsioufis, K. Computed Tomography Angiography Identified High-Risk Coronary Plaques: From Diagnosis to Prognosis and Future Management. Diagnostics 2024, 14, 1671. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.B.; Liu, H.D.; Xing, J.H.; Chen, B.W.; Zhao, Y.Y.; Gu, H.P.; Tao, H.L. Safety and Efficacy of Drug-Coated Balloons in Patients with Acute Coronary Syndromes and Vulnerable Plaque. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296221130063. [Google Scholar] [CrossRef]
- Stone, G.W.; Biensock, S.W.; Neumann, F.J. Bioresorbable coronary scaffolds are ready for a comeback: Pros and cons. Eur Collab Work Group Interv Cardiol Eur Soc Cardiol. EuroIntervention 2023, 19, 199–202. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Total (n = 151) | TTS (n = 55) | MINOCA (n = 96) | p | |
|---|---|---|---|---|
| Demographics—History | ||||
| Age, years | 62 ± 12 | 68 ± 11 | 59 ± 11 | 0.065 |
| Female sex, n (%) | 107 (71) | 50 (91) | 57 (59) | <0.001 |
| BMI, kg/m2 | 27 ± 5 | 26 ± 4 | 28 ± 5 | NS |
| Smoking, n (%) | 94 (43.3) | 12 (21.8) | 32 (33) | 0.001 |
| HTN, n (%) | 84 (55.6) | 37 (67.3) | 47 (49) | <0.001 |
| DM, n (%) | 26 (17.2) | 8 (14.5) | 18 (19) | NS |
| Dyslipidemia, n (%) | 66 (43.7) | 28 (51) | 38 (39.5) | NS |
| CKD, n (%) | 17 (11.3) | 10 (18.2) | 7 (7.2) | <0.001 |
| CAD, n (%) | 8 (5.3) | 3 (5.5) | 5 (5.2) | NS |
| HF, n (%) | 1 (0.7) | 1 (1.8) | 0 | NS |
| AF, n (%) | 11 (7.3) | 8 (14.5) | 3 (3) | <0.001 |
| Family History of CAD, n (%) | 20 (13.2) | 10 (18.2) | 10 (10.4) | 0.012 |
| Pre-hospital Medication | ||||
| Antiplatelet agents, n (%) | 18 (11.9) | 6 (10.9) | 12 (12.5) | NS |
| OACs, n (%) | 11 (7.3) | 7 (12.7) | 4 (4) | <0.001 |
| Laboratory Values | ||||
| Entry hs-TnI, pg/mL | 392 (1–157,000) | 425 (3–10,956) | 290 (1–157,000) | NS |
| Peak hs-TnI, pg/mL | 715 (25–157,000) | 570 (30–10,956) | 786 (25–157,000) | 0.010 |
| NT pro BNP, pg/mL | 919 (50–11,693) | 2281 (50–11,693) | 255 (70–919) | 0.046 |
| Hemoglobin, g/dL | 13.4 ± 1.5 | 13.2 ± 1.3 | 13.6 ± 1.6 | NS |
| eGFR, mL/min/1.73 m2 | 80 ± 26 | 74 ± 27 | 86 ± 26 | 0.056 |
| InterTAK Score | 48 ± 21 | 61 ± 18 | 39 ± 19 | <0.001 |
| LVEF (%) | 51 ± 11 | 44 ± 12 | 54 ± 9 | 0.002 |
| Coronary Findings | ||||
| Normal or atherosclerotic vessels, n (%) | 95 (63) | 41 (74.5) | 54 (56) | - |
| New stenosis < 50%, n (%) | 32 (21.2) | 11 (20) | 21 (22) | - |
| >50% in non-culprit vessel, n (%) | 4 (2.6) | 2 (3.6) | 2 (2) | - |
| Epicardial spasm, n (%) | 6 (4) | 0 | 6 (6.2) | - |
| Spontaneous coronary dissection, n (%) | 5 (3.3) | 0 | 5 (5.2) | - |
| Myocardial bridge, n (%) | 7 (4.6) | 1 (1.8) | 6 (6.2) | - |
| Predictors | OR | 95% CI | p | |
|---|---|---|---|---|
| CA findings | 0.334 | 0.307 | 0.813 | <0.001 |
| Age | −0.133 | −0.018 | −0.001 | 0.096 |
| ECG | 0.057 | −0.194 | 0.434 | NS |
| LVEF | −0.061 | −0.190 | 0.080 | ΝS |
| Prior OAC | −0.224 | −1.040 | −0.192 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantzouranis, E.; Leontsinis, I.; Vlachakis, P.K.; Mihas, C.; Iliakis, P.; Dri, E.; Sakalidis, A.; Soulaidopoulos, S.; Fragoulis, C.; Milkas, A.; et al. Antiplatelet Treatment Strategy in MINOCA Patients: Predictors of Decision Making in Clinical Practice and Prognostic Implications. J. Clin. Med. 2025, 14, 3984. https://doi.org/10.3390/jcm14113984
Mantzouranis E, Leontsinis I, Vlachakis PK, Mihas C, Iliakis P, Dri E, Sakalidis A, Soulaidopoulos S, Fragoulis C, Milkas A, et al. Antiplatelet Treatment Strategy in MINOCA Patients: Predictors of Decision Making in Clinical Practice and Prognostic Implications. Journal of Clinical Medicine. 2025; 14(11):3984. https://doi.org/10.3390/jcm14113984
Chicago/Turabian StyleMantzouranis, Emmanouil, Ioannis Leontsinis, Panayotis K. Vlachakis, Constantinos Mihas, Panagiotis Iliakis, Eirini Dri, Athanasios Sakalidis, Stergios Soulaidopoulos, Christos Fragoulis, Anastasios Milkas, and et al. 2025. "Antiplatelet Treatment Strategy in MINOCA Patients: Predictors of Decision Making in Clinical Practice and Prognostic Implications" Journal of Clinical Medicine 14, no. 11: 3984. https://doi.org/10.3390/jcm14113984
APA StyleMantzouranis, E., Leontsinis, I., Vlachakis, P. K., Mihas, C., Iliakis, P., Dri, E., Sakalidis, A., Soulaidopoulos, S., Fragoulis, C., Milkas, A., Tsiamis, E., Tsiachris, D., Dimitriadis, K., & Tsioufis, K. (2025). Antiplatelet Treatment Strategy in MINOCA Patients: Predictors of Decision Making in Clinical Practice and Prognostic Implications. Journal of Clinical Medicine, 14(11), 3984. https://doi.org/10.3390/jcm14113984