1. Introduction
Sarcopenia is a skeletal muscle disorder characterized by the progressive loss of muscle mass, strength, and function [
1,
2]. The European Working Group on Sarcopenia in Older People (EWGSOP2) has established a diagnostic algorithm that includes the assessment of muscle strength, mass, and quality [
3]. Classified as a disease in the ICD-10-CM [
4], sarcopenia is common among older adults due to the progressive decline in skeletal muscle tissue beginning around the age of 40, increasing the risk of frailty and functional dependence [
5,
6].
Sarcopenia is associated with multiple comorbidities, including cancer [
7], obesity [
8,
9], and renal and cardiovascular diseases [
10]. Its prevalence is difficult to determine due to the wide range of diagnostic methods—such as the SARC-F questionnaire, BIA, MRI, CT, and DEXA [
1]—which differ in accessibility, accuracy, and clinical utility [
11,
12]. Early detection of sarcopenia in emergency settings may offer a window of opportunity to initiate timely interventions, particularly in frail or comorbid patients [
13].
Cardiovascular diseases such as heart failure and peripheral arterial disease may contribute to sarcopenia due to factors like oxidative stress and malnutrition [
14]. Likewise, cardiac surgery can lead to muscle mass loss due to immobilization [
10]. In respiratory conditions such as chronic obstructive pulmonary disease (COPD), dyspnea and chronic inflammation worsen sarcopenia [
15]. There is also evidence of higher sarcopenia prevalence in patients with malignant digestive diseases [
16] and in oncology patients with cachexia, a metabolic syndrome involving loss of muscle mass and body weight [
17,
18].
Trauma is also associated with sarcopenia, as appropriate nutritional support can reduce rehabilitation time in cases such as hip fractures [
18]. Among metabolic disorders, type 2 diabetes mellitus (T2DM) contributes to sarcopenia through insulin resistance and lipid-induced muscle dysfunction [
19].
Given the clinical relevance of this condition, the present study aimed to evaluate the relationship between sarcopenia and various pathologies in patients admitted to the emergency department, to identify which diseases are associated with higher sarcopenia indices, and to determine the related in-hospital complications.
We hypothesized that lower rectus femoris muscle thickness, indicative of sarcopenia, would be associated with a higher prevalence of comorbidities and increased risk of in-hospital complications among emergency department patients.
2. Materials and Methods
2.1. Study Design
This was an observational, prospective, and cross-sectional study conducted at the Infanta Cristina University Hospital in Parla (Madrid, Spain). Sarcopenia was assessed by ultrasound, performed under the supervision of a liaison nurse, in all patients who presented to the emergency department. The results were compared across the different diagnosed pathologies.
This study was approved by the Ethics and Research Committee of the Puerta de Hierro University Hospital (ACT 245.23, 24 November 2023).
The reporting of this observational study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
2.2. Study Population
The nutritional ultrasound program for the diagnosis of sarcopenia was implemented at the hospital in 2021. All patients presenting to the emergency department were evaluated using ultrasound, except for those who did not meet the inclusion criteria. All eligible patients who met the inclusion criteria were included and completed the full study protocol without loss to follow-up.
2.2.1. Inclusion Criteria
The study included all patients aged 18 years or older who presented to the Emergency Department of Infanta Cristina University Hospital between January and May 2023. To be eligible, patients had to be in stable clinical condition, allowing for ultrasound evaluation during their emergency department stay—either during prolonged observation or prior to hospital admission. Additionally, patients were required to have sufficient cognitive capacity to understand the information provided about the procedure and to give verbal consent for the assessment.
2.2.2. Exclusion Criteria
Patients were excluded from the study if, at the time of evaluation, they were in cardiac arrest (resuscitation bay), exhibited hemodynamic instability that precluded immediate ultrasound assessment, presented with an acute psychiatric condition that impaired cooperation, or had clinical presentations classified as high-resolution cases, where the short duration of stay in the emergency department did not allow for completion of the sarcopenia measurement protocol.
2.3. Sample Size
Assuming a 15% loss rate, a 95% confidence level, a 3% margin of error, and a 5% estimated proportion, an appropriate sample size of 150 participants was calculated.
2.4. Studied Variables
The following sociodemographic and clinical variables were collected: sex (male, female), age, nutritional ultrasound measurements of the rectus femoris (Y-axis, X-axis, and cross-sectional area), antidiabetic medication (metformin, sulfonylureas, sodium–glucose co-transporter 2 (iSGLT2) inhibitors, thiazolidinediones, dipeptidyl peptidase-4 (iDPP-4) inhibitors, insulin, glucagon-like peptide-1 (GLP-1Ra) receptor agonists, and their respective combinations), reason for admission or observation (cardiovascular, respiratory, endocrine-metabolic, digestive, oncological, neurological, orthopedic, urological, hematological), and personal medical history (yes/no) of cardiovascular disease, digestive disease, respiratory disease, urological disease, hematological disease, neurological disease, diabetes mellitus, and active cancer.
The clinical outcomes assessed included the following: hospital admission (yes/no), C-reactive protein (CRP), lymphocyte count, total protein, albumin, development of complications (yes/no), type of complication (infectious, respiratory, cardiovascular), and in-hospital mortality (yes/no).
Complications were defined as new events during hospitalization, including respiratory infections, cardiovascular events (e.g., arrhythmias, acute coronary syndromes), and other nosocomial infections, as documented in the electronic medical records.
2.5. Intervention
All patients included in the study underwent a nutritional ultrasound assessment aimed at estimating their degree of sarcopenia. Prior to the procedure, each patient’s capacity to understand the purpose, implications, and rationale for their inclusion in the program was evaluated to ensure adequate informed cooperation.
The ultrasound examination was performed during the emergency department stay, either when the patient required prolonged observation or had a pending hospital admission. At the same time, relevant clinical data were collected, including the reason for admission, personal medical history, and current medications.
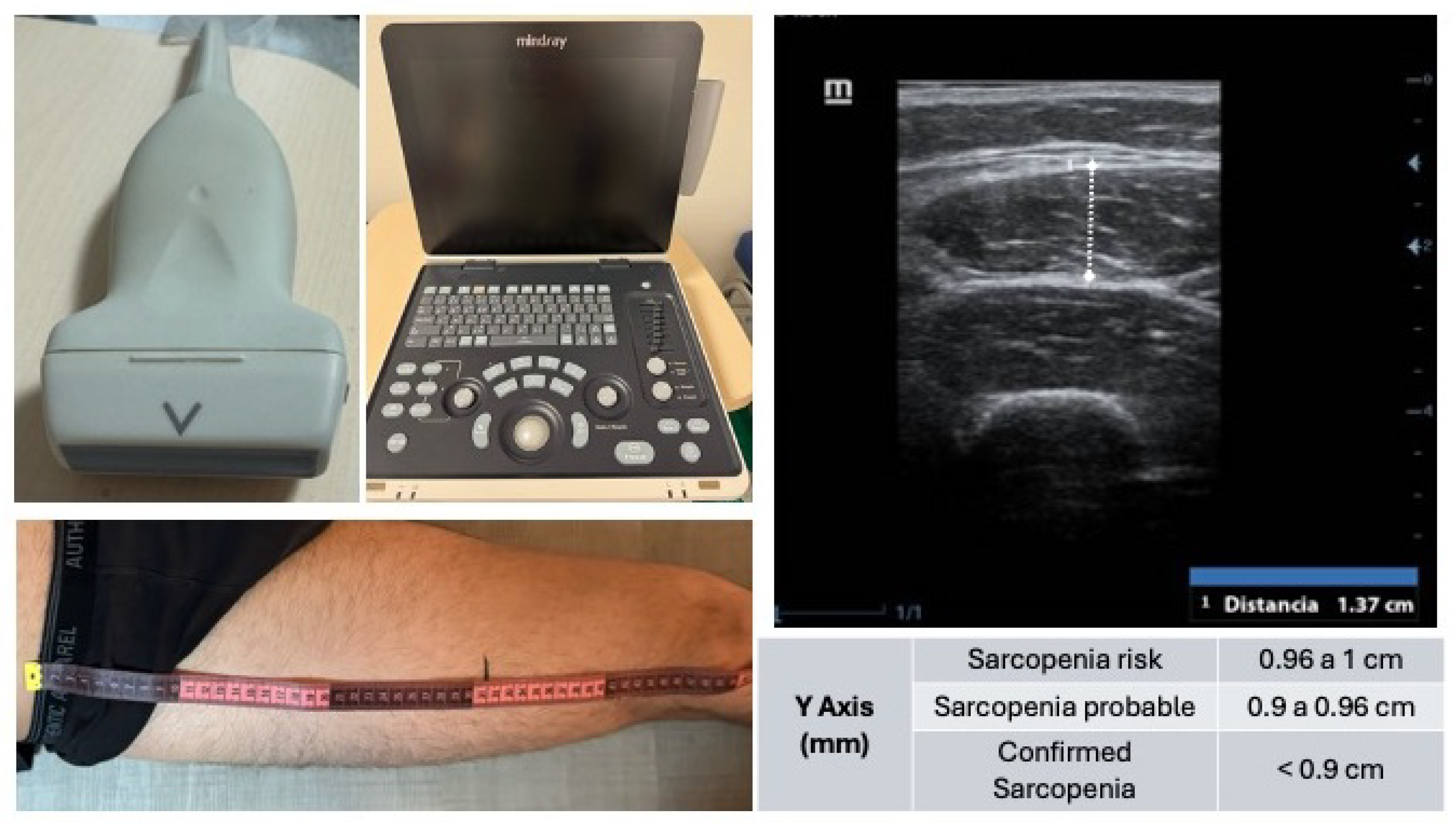
The muscle ultrasound was conducted using a Mindray Z50® ultrasound system, Nanshan, Shenzhen, China equipped with a linear transducer, optimized for high-resolution imaging of superficial skeletal muscle tissue. The patient was placed in a supine position with the lower limbs relaxed to minimize muscle tension.
The anatomical reference points for the measurement were the anterior superior iliac spine (ASIS) and the superior border of the patella. The total distance between these landmarks was measured, and the probe was positioned at the junction of the distal third of this segment, a location providing optimal visualization of the rectus femoris muscle (
Figure 1).
After applying conductive gel to the skin, the transducer was placed perpendicularly to the muscle fibers in the transverse (short-axis) plane. Great care was taken to avoid any probe angulation, as oblique positioning can lead to erroneous measurements. Once the muscle architecture was clearly identified—typically including the skin, subcutaneous tissue, vastus lateralis, rectus femoris, and femoral bone interface—the image was frozen, and the anteroposterior thickness of the rectus femoris (Y-axis) was measured, along with other optional parameters (X-axis, cross-sectional area).
Following the ultrasound assessment, relevant laboratory values (e.g., C-reactive protein, lymphocyte count, total protein, and albumin levels) were recorded from the electronic health records. Additionally, at one month post-admission, a retrospective review of the patient’s clinical course was conducted to identify any in-hospital complications (e.g., infections, cardiovascular, or respiratory events) and to register mortality (exitus) where applicable.
2.6. Statistical Analysis
Statistical analysis was performed using SPSS software (version 29; IBM, Armonk, NY, USA). Descriptive statistics were calculated for all variables. Categorical variables were presented as frequencies and percentages, and continuous variables were expressed as means and standard deviations.
To assess the independent association between rectus femoris muscle thickness and the development of in-hospital complications, a multivariate logistic regression model was constructed. The model included the Y-axis muscle measurement as the primary predictor and adjusted for potential confounders, including age, sex, and the presence of cardiovascular, digestive, neurological, hematological, and respiratory comorbidities. Statistical significance was set at p < 0.05.
4. Discussion
This study describes the sarcopenia outcomes of patients who presented to the emergency department, as well as the prevalence of the condition according to different underlying diseases. Sarcopenia has often been reported as a comorbidity of cardiac conditions. A literature review identified sarcopenia as one of the most important factors contributing to impaired physical function and the progression of cardiovascular disease [
5]. In the present study, cardiovascular disease was the most frequent reason for emergency consultation (20.70%) and also the most common comorbidity, with 91 out of 150 patients having a history of cardiovascular disease.
Stroke ranked as the second leading cause of death in Spain during the first half of 2023, following ischemic heart disease [
20]. Sarcopenia has been linked to such conditions due to its role in capillary alterations in skeletal muscle tissue and its association with neuronal degeneration [
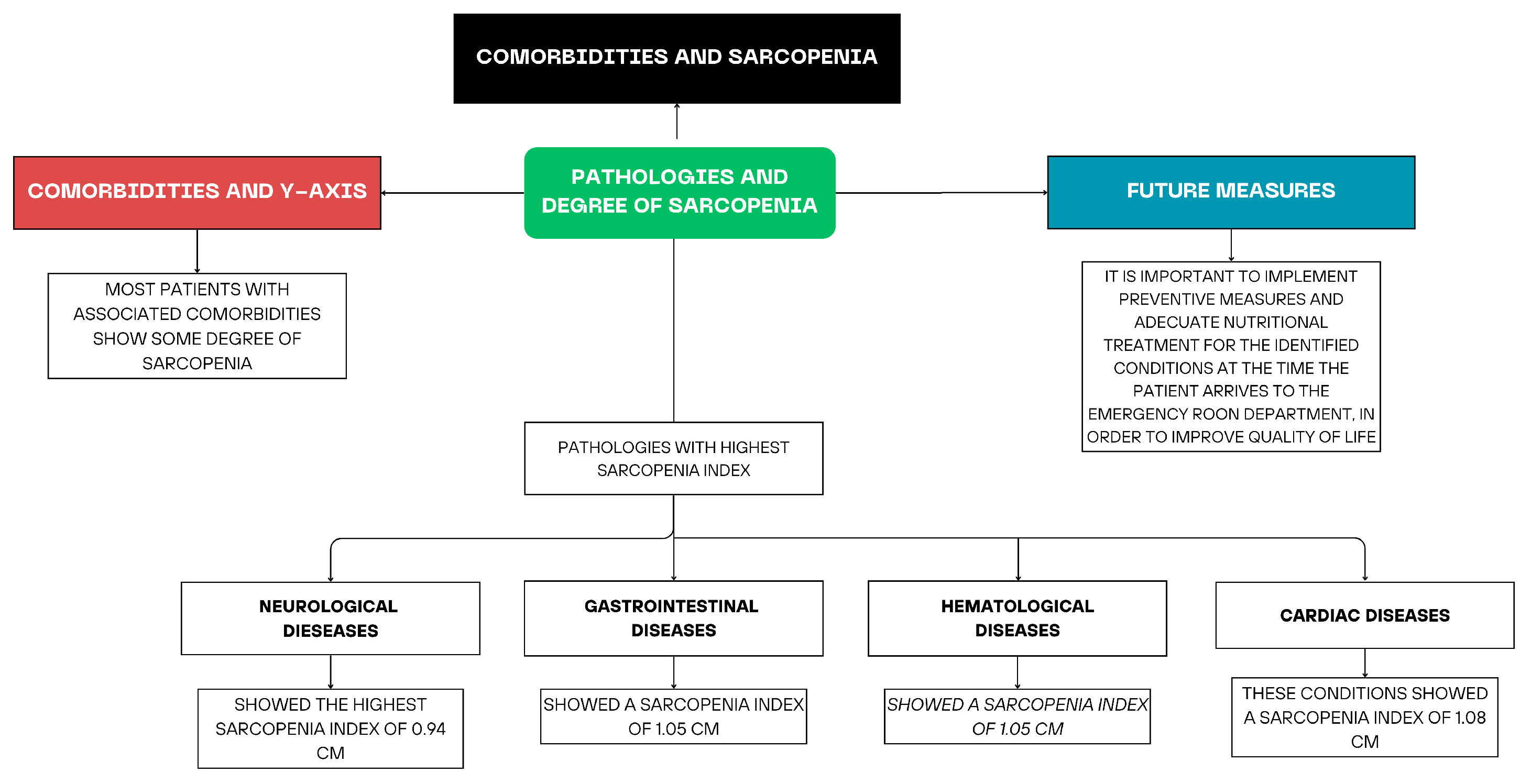
21]. In ischemic stroke, cerebral injury leads to synaptic remodeling, including alterations in motor neuron innervation, which increases the likelihood of developing sarcopenia. Among the 150 participants, neurological pathology showed the highest degree of sarcopenia, with a mean Y-axis measurement of 0.93 cm in the rectus femoris. However, this group was relatively small, as only 23 out of 150 patients presented with neurological symptoms. Most were ischemic stroke survivors with one or more cardiovascular risk factors, though other clinical conditions, such as epilepsy, were also represented.
A descriptive observational study of 303 patients with digestive diseases showed that 32.00% had a diagnosis of sarcopenia. Sarcopenia prevalence was reported as 22.20% in gastrointestinal disease, 36.60% in biliary–pancreatic disease, and 36.90% in hepatic disease [
16]. A literature review further concluded that early-onset Crohn’s disease and advanced-age ulcerative colitis were associated with a higher risk of sarcopenia due to the malabsorption and inflammation characteristic of these conditions [
22]. The present study supports this evidence, showing that patients with digestive diseases had the second-highest prevalence of sarcopenia, with a mean Y-axis measurement of 1.05 cm.
Regarding hematological conditions, a direct relationship was also observed with sarcopenia. A cross-sectional study indicated that low hematocrit, decreased hemoglobin levels—as in anemia—and increased IL-6 were associated with a greater likelihood of sarcopenia [
23]. Similarly, our findings placed hematological conditions as the third leading group in terms of sarcopenia prevalence, with a mean of 1.05 cm.
Finally, patients with respiratory conditions in this study exhibited the lowest degrees of sarcopenia, as there were no substantial numerical differences in Y-axis means between patients with or without a respiratory history. However, certain respiratory conditions, such as pneumonia, are associated with inflammation that promotes muscle atrophy via a pro-inflammatory cytokine cascade [
21]. It is noteworthy that the majority of complications observed after hospital admission in this study were infectious respiratory events, often requiring extended hospital stays and contributing to physical decline and muscle mass loss. Emerging literature has also highlighted the relevance of sarcopenia in infectious diseases such as COVID-19, where low muscle mass has been associated with worse outcomes [
24].
Despite the variation in the frequency of diagnoses and Y-axis measurements, most patients with any of the comorbidities listed above showed some degree of sarcopenia, with Y-axis means generally around 1.0–1.1 cm. The results of this study demonstrate that neurological pathology was associated with the lowest muscle thickness and highest sarcopenia index, with a mean of 0.93 cm, followed by digestive, hematological, and cardiac conditions with means of 1.05 cm, 1.05 cm, and 1.08 cm, respectively.
The multivariate analysis confirmed that reduced rectus femoris thickness, as a surrogate marker of sarcopenia, was independently associated with the development of in-hospital complications. This reinforces prior evidence suggesting that muscle mass serves as a marker of physiological reserve and vulnerability. Interestingly, none of the specific comorbidities reached significance in the adjusted model, which underscores the potential value of incorporating muscle ultrasound into routine risk stratification.
The marginal association between male sex and complications aligns with some literature suggesting sex-related differences in inflammatory and metabolic response. Further studies are needed to explore these gender-based variations (
Figure A1).


 ,
, 

{kind=link}
{kind=link}