

Admission Red Blood Cell Distribution Width and Mean Platelet Volume as Predictors of Mortality in the Pediatric Intensive Care Unit: A Five-Year Single-Center Retrospective Study
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
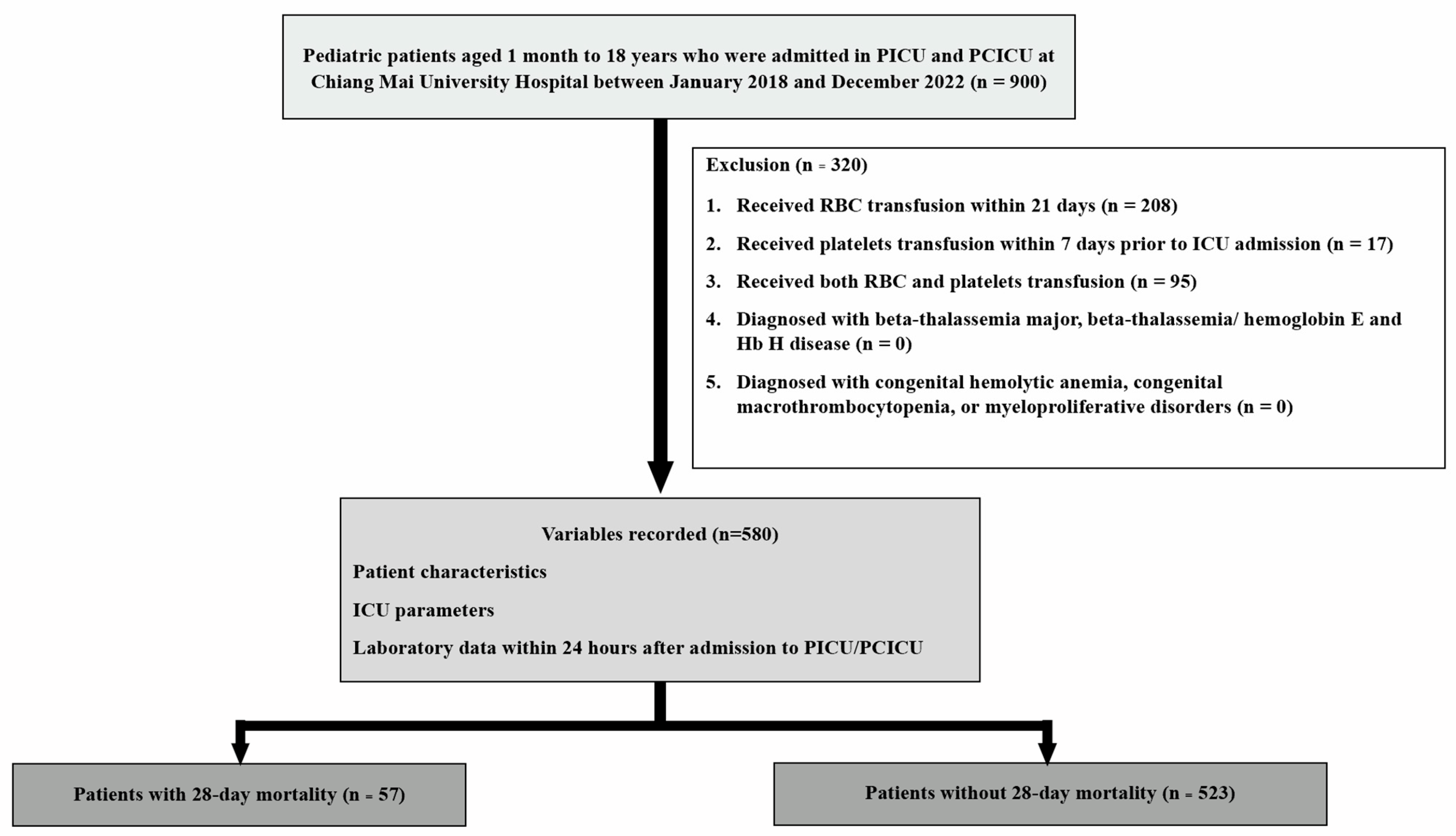
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Collection
2.4. Outcome
2.5. Study Size Estimation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| aRR | Adjusted relative risk |
| AuROC | Area under the receiver operating characteristic |
| BMI | Body mass index |
| BUN | Blood urea nitrogen |
| CBC | Complete blood count |
| CRP | C-reactive protein |
| CRRT | Continuous renal replacement therapy |
| DAGs | Directed acyclic graphs |
| ESR | Erythrocyte sedimentation rate |
| fL | flamtoliter |
| HR | Hazard ratio |
| ICU | Intensive care unit |
| IQR | Interquartile range |
| LOS | Length of stay |
| MCV | Mean corpuscular volume |
| MOD | Multi-organ dysfunction |
| MPV | Mean platelet volume |
| MV | Mechanical ventilation |
| NPV | Negative predictive value |
| PCR | Polymerase chain reaction |
| PCT | Platelet-crit |
| PDW | Platelet distribution width |
| PELOD-2 | Pediatric Logistic Organ Dysfunction-2 |
| PICU | Pediatric intensive care unit |
| PIM-2 | Pediatric Index of Mortality 2 |
| PPV | Positive predictive value |
| RBC | Red blood cell |
| RDW | Red blood cell distribution width |
| ROC | Receiver operating characteristic |
| RR | Relative risk |
| SD | Standard deviation |
| TNF-α | Tumor necrosis factor-α |
| WBC | White blood cell |
References
- Sachdev, A.; Simalti, A.; Kumar, A.; Gupta, N.; Gupta, D.; Chugh, P. Outcome Prediction Value of Red Cell Distribution Width in Critically-ill Children. Indian Pediatr. 2018, 55, 414–416. [Google Scholar] [CrossRef]
- Kim, D.H.; Ha, E.J.; Park, S.J.; Jhang, W.K. Evaluation of the usefulness of red blood cell distribution width in critically ill pediatric patients. Medicine 2020, 99, e22075. [Google Scholar] [CrossRef]
- Cai, N.; Chen, Z.Q.; Tao, M.; Fan, W.T.; Liao, W. Mean platelet volume and red blood cell distribution width is associated with prognosis in premature neonates with sepsis. Open Med. 2021, 16, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Dubey, A.; Kumar, S.; Acharya, S.; Wanjari, A.K.; Bawankule, S.; Agrawal, S.; Shukla, A. Impact of Red Cell and Platelet Distribution Width in Patients of Medical Intensive Care Unit. J. Lab. Physicians 2021, 13, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Bulut, O.; Akcakaya, A.; Bulut, N.; Ovali, F. Elevated Red Cell Distribution Width as a Useful Marker in Neonatal Sepsis. J. Pediatr. Hematol./Oncol. 2021, 43, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Liberski, P.S.; Szewczyk, M.; Krzych, Ł.J. Haemogram-Derived Indices for Screening and Prognostication in Critically Ill Septic Shock Patients: A Case-Control Study. Diagnostics 2020, 10, 638. [Google Scholar] [CrossRef]
- Rajagopal, P.; Ramamoorthy, S.; Jeslin, A.G. Utility of Haemogram Parameters in Mortality Risk Prediction of Critically ill Patients. J. Evol. Med. Dent. Sci. 2018, 7, 1024–1030. [Google Scholar] [CrossRef]
- Mangalesh, S.; Dudani, S.; Malik, A. Platelet Indices and Their Kinetics Predict Mortality in Patients of Sepsis. Indian J. Hematol. Blood Transfus. Off. J. Indian Soc. Hematol. Blood Transfus. 2021, 37, 600–608. [Google Scholar] [CrossRef]
- Weiss, G.; Goodnough, L.T. Anemia of chronic disease. N. Engl. J. Med. 2005, 352, 1011–1023. [Google Scholar] [CrossRef]
- Jo, Y.H.; Kim, K.; Lee, J.H.; Kang, C.; Kim, T.; Park, H.M.; Kang, K.W.; Kim, J.; Rhee, J.E. Red cell distribution width is a prognostic factor in severe sepsis and septic shock. Am. J. Emerg. Med. 2013, 31, 545–548. [Google Scholar] [CrossRef]
- Bazick, H.S.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Christopher, K.B. Red cell distribution width and all-cause mortality in critically ill patients. Crit. Care Med. 2011, 39, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Ku, N.S.; Kim, H.W.; Oh, H.J.; Kim, Y.C.; Kim, M.H.; Song, J.E.; Oh, D.H.; Ahn, J.Y.; Kim, S.B.; Jeong, S.J.; et al. Red blood cell distribution width is an independent predictor of mortality in patients with gram-negative bacteremia. Shock 2012, 38, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Said, A.S.; Spinella, P.C.; Hartman, M.E.; Steffen, K.M.; Jackups, R.; Holubkov, R.; Wallendorf, M.; Doctor, A. RBC Distribution Width: Biomarker for Red Cell Dysfunction and Critical Illness Outcome? Pediatr. Crit. Care Med. 2017, 18, 134–142. [Google Scholar] [CrossRef]
- Schepens, T.; De Dooy, J.J.; Verbrugghe, W.; Jorens, P.G. Red cell distribution width (RDW) as a biomarker for respiratory failure in a pediatric ICU. J. Inflamm. 2017, 14, 12. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, S.J.; Lee, M.J.; Kwon, Y.E.; Kim, Y.L.; Park, K.S.; Ryu, H.J.; Park, J.T.; Han, S.H.; Yoo, T.H.; et al. An increase in mean platelet volume from baseline is associated with mortality in patients with severe sepsis or septic shock. PLoS ONE 2015, 10, e0119437. [Google Scholar] [CrossRef]
- Briggs, C. Quality counts: New parameters in blood cell counting. Int. J. Lab. Hematol. 2009, 31, 277–297. [Google Scholar] [CrossRef]
- Leader, A.; Pereg, D.; Lishner, M. Are platelet volume indices of clinical use? A multidisciplinary review. Ann. Med. 2012, 44, 805–816. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mikhailidis, D.P.; Kitas, G.D. Mean platelet volume: A link between thrombosis and inflammation? Curr. Pharm. Des. 2011, 17, 47–58. [Google Scholar] [CrossRef]
- Lippi, G.; Targher, G.; Montagnana, M.; Salvagno, G.L.; Zoppini, G.; Guidi, G.C. Relation Between Red Blood Cell Distribution Width and Inflammatory Biomarkers in a Large Cohort of Unselected Outpatients. Arch. Pathol. Lab. Med. 2009, 133, 628–632. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Sanchis-Gomar, F.; Picanza, A.; Lippi, G. Red blood cell distribution width: A simple parameter with multiple clinical applications. Crit. Rev. Clin. Lab. Sci. 2015, 52, 86–105. [Google Scholar] [CrossRef]
- Seo, I.-H.; Lee, Y.-J. Usefulness of Complete Blood Count (CBC) to Assess Cardiovascular and Metabolic Diseases in Clinical Settings: A Comprehensive Literature Review. Biomedicines 2022, 10, 2697. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Zhai, Y.; Song, W.; Zhu, T.; Xu, Z.; Jiang, L.; Li, L.; Liu, D.; Wu, Q. Association between complete blood count-derived inflammatory markers and the risk of frailty and mortality in middle-aged and older adults. Front. Public Health 2024, 12, 1427546. [Google Scholar] [CrossRef] [PubMed]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- Safdar, S.A.; Modi, T.; Sriramulu, L.D.; Shaaban, H.; Sison, R.; Modi, V.; Adelman, M.; Guron, G. The Role of Red Cell Distribution Width as a Predictor of Mortality for Critically Ill Patients in an Inner-city Hospital. J. Nat. Sci. Biol. Med. 2017, 8, 154–158. [Google Scholar] [CrossRef]
- Ghimire, R.; Shakya, Y.M.; Shrestha, T.M.; Neupane, R.P. The utility of red cell distribution width to predict mortality of septic patients in a tertiary hospital of Nepal. BMC Emerg. Med. 2020, 20, 43. [Google Scholar] [CrossRef]
- Ramby, A.L.; Goodman, D.M.; Wald, E.L.; Weiss, S.L. Red Blood Cell Distribution Width as a Pragmatic Marker for Outcome in Pediatric Critical Illness. PLoS ONE 2015, 10, e0129258. [Google Scholar] [CrossRef]
- Go, H.; Ohto, H.; Nollet, K.E.; Takano, S.; Kashiwabara, N.; Chishiki, M.; Maeda, H.; Imamura, T.; Kawasaki, Y.; Momoi, N.; et al. Using Platelet Parameters to Anticipate Morbidity and Mortality Among Preterm Neonates: A Retrospective Study. Front. Pediatr. 2020, 8, 90. [Google Scholar] [CrossRef]
- Taha, R.S.; Afandy, M.E.; Elbadawi, A.H.; Abd El Ghafar, M.S. Platelet indices in critically ill septic patients as a predictor of mortality. Egypt. J. Anaesth. 2023, 39, 56–62. [Google Scholar] [CrossRef]
- Brown, M.; Nassoiy, S.; Plackett, T.; Luchette, F.; Posluszny, J., Jr. Red blood cell distribution width and outcome in trauma patients. J. Osteopath. Med. 2021, 121, 221–228. [Google Scholar] [CrossRef]
- Li, S.; Zhang, W.; Liang, X. Red blood cell distribution width and mortality risk in critically ill cardiovascular patients. Heliyon 2023, 9, e22225. [Google Scholar] [CrossRef]
- Wang, H.; Huang, J.; Liao, W.; Xu, J.; He, Z.; Liu, Y.; He, Z.; Chen, C. Prognostic Value of the Red Cell Distribution Width in Patients with Sepsis-Induced Acute Respiratory Distress Syndrome: A Retrospective Cohort Study. Dis. Markers 2021, 2021, 5543822. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.M.; Mahadevan, L. Physiological and pathological population dynamics of circulating human red blood cells. Proc. Natl. Acad. Sci. USA 2010, 107, 20587–20592. [Google Scholar] [CrossRef] [PubMed]
- Scharte, M.; Fink, M.P. Red blood cell physiology in critical illness. Crit. Care Med. 2003, 31, S651–S657. [Google Scholar] [CrossRef]
- Pierce, C.N.; Larson, D.F. Inflammatory cytokine inhibition of erythropoiesis in patients implanted with a mechanical circulatory assist device. Perfusion 2005, 20, 83–90. [Google Scholar] [CrossRef]
- Ghaffari, S. Oxidative Stress in the Regulation of Normal and Neoplastic Hematopoiesis. Antioxid. Redox Signal. 2008, 10, 1923–1940. [Google Scholar] [CrossRef]
- Tajarernmuang, P.; Phrommintikul, A.; Limsukon, A.; Pothirat, C.; Chittawatanarat, K. The Role of Mean Platelet Volume as a Predictor of Mortality in Critically Ill Patients: A Systematic Review and Meta-Analysis. Crit. Care Res. Pract. 2016, 2016, 4370834. [Google Scholar] [CrossRef]
- Vardon-Bounes, F.; Gratacap, M.P.; Groyer, S.; Ruiz, S.; Georges, B.; Seguin, T.; Garcia, C.; Payrastre, B.; Conil, J.M.; Minville, V. Kinetics of mean platelet volume predicts mortality in patients with septic shock. PLoS ONE 2019, 14, e0223553. [Google Scholar] [CrossRef]
- İşgüder, R.; Ceylan, G.; Ağın, H.; Nacaroğlu, H.T.; Korkmaz, H.A.; Devrim, İ.; Vergin, C. Increased mean platelet volume in children with sepsis as a predictor of mortality. Turk. J. Pediatr. 2016, 58, 503–511. [Google Scholar] [CrossRef]
- Zhang, S.; Cui, Y.L.; Diao, M.Y.; Chen, D.C.; Lin, Z.F. Use of Platelet Indices for Determining Illness Severity and Predicting Prognosis in Critically Ill Patients. Chin. Med. J. 2015, 128, 2012–2018. [Google Scholar] [CrossRef]
- Ye, S.; Zhang, Y.; Zhang, C.; Xu, D. Are platelet volume indices related to mortality in hospitalized children on mechanical ventilation? J. Int. Med. Res. 2018, 46, 1197–1208. [Google Scholar] [CrossRef]
- Mohsen, L.; Akmal, D.M.; Ghonaim, E.K.E.; Riad, N.M. Role of mean platelet volume and ischemia modified albumin in evaluation of oxidative stress and its association with postnatal complications in infants of diabetic mothers. J. Matern. Fetal Neonatal Med. 2018, 31, 1819–1823. [Google Scholar] [CrossRef] [PubMed]
- Yazici, S.; Yazici, M.; Erer, B.; Erer, B.; Calik, Y.; Ozhan, H.; Ataoglu, S. The platelet indices in patients with rheumatoid arthritis: Mean platelet volume reflects disease activity. Platelets 2010, 21, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Huczek, Z.; Kochman, J.; Filipiak, K.J.; Horszczaruk, G.J.; Grabowski, M.; Piatkowski, R.; Wilczynska, J.; Zielinski, A.; Meier, B.; Opolski, G. Mean platelet volume on admission predicts impaired reperfusion and long-term mortality in acute myocardial infarction treated with primary percutaneous coronary intervention. J. Am. Coll. Cardiol. 2005, 46, 284–290. [Google Scholar] [CrossRef]
- Hu, Z.D.; Lippi, G.; Montagnana, M. Diagnostic and prognostic value of red blood cell distribution width in sepsis: A narrative review. Clin. Biochem. 2020, 77, 1–6. [Google Scholar] [CrossRef]
- Nagaraju, N.; Varma, A.; Taksande, A.; Meshram, R.J. Bone Marrow Changes in Septic Shock: A Comprehensive Review. Cureus 2023, 15, e42517. [Google Scholar] [CrossRef]
- Gallagher, P.G. Anemia in the pediatric patient. Blood 2022, 140, 571–593. [Google Scholar] [CrossRef]
- Sun, H.; Weaver, C.M. Decreased Iron Intake Parallels Rising Iron Deficiency Anemia and Related Mortality Rates in the US Population. J. Nutr. 2021, 151, 1947–1955. [Google Scholar] [CrossRef]
- Scott, S.P.; Chen-Edinboro, L.P.; Caulfield, L.E.; Murray-Kolb, L.E. The impact of anemia on child mortality: An updated review. Nutrients 2014, 6, 5915–5932. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 580) | Non-Survivors (n= 57) | Survivors (n= 523) | p-Value |
|---|---|---|---|---|
| Age (years) | 5.9 (4.7, 10.4) | 5.8 (4.7, 8.8) | 6 (4.8, 10.4) | 0.689 |
| Male, n (%) | 321 (55.3) | 38 (66.7) | 283 (54.1) | 0.070 |
| Body mass index (kg/m2) | 15.2 (13.5, 17.4) | 15.1 (12.9, 17.8) | 15.2 (13.6, 17.4) | 0.614 |
| Comorbidities | ||||
| Seizure/epilepsy, n (%) | 49 (8.4) | 5 (8.7) | 44 (8.4) | 0.926 |
| Chronic lung disease, n (%) | 43 (7.4) | 8 (14.0) | 35 (6.7) | 0.045 |
| Cardiac arrythmia, n (%) | 27 (4.6) | 3 (5.3) | 24 (4.6) | 0.819 |
| Asthma, n (%) | 12 (2.1) | 0 (0) | 12 (2.3) | 0.248 |
| Neuromuscular disease, n (%) | 1 (0.2) | 0 (0) | 1 (0.2) | 0.741 |
| Solid tumor, n (%) | 22 (3.8) | 0 (0) | 22 (4.2) | 0.114 |
| Systemic lupus erythematosus, n (%) | 10 (1.7) | 2 (3.5) | 8 (1.5) | 0.276 |
| Reason for intensive care unit admission | ||||
| Respiratory failure and acute respiratory distress syndrome, n (%) | 418 (72.1) | 51 (89.5) | 367 (70.2) | 0.002 |
| Congestive heart failure, n (%) | 130 (22.4) | 20 (35.1) | 110 (21.0) | 0.016 |
| Sepsis/Septic shock, n (%) | 99 (17.1) | 15 (26.3) | 84 (16.1) | 0.051 |
| Post-operative care, n (%) | 113 (19.5) | 7 (12.3) | 106 (20.3) | 0.148 |
| Neurologic condition/alteration of consciousness, n (%) | 27 (4.6) | 3 (5.3) | 24 (4.6) | 0.819 |
| Others, n (%) | 62 (10.7) | 7 (12.3) | 55 (10.5) | 0.682 |
| Illness severity | ||||
| Multi-organ failure, n (%) | 259 (44.6) | 46 (80.7) | 213 (40.7) | <0.001 |
| Pediatric Index of Mortality 2 score | 2.9 (1.0, 6.6) | 4.1 (1.5, 9.2) | 2.8 (1.0, 6.3) | 0.021 |
| Management | ||||
| Mechanical ventilation, n (%) | 432 (74.5) | 54 (94.7) | 378 (72.3) | <0.001 |
| Vasoactive drugs, n (%) | 217 (37.4) | 45 (78.9) | 172 (32.9) | <0.001 |
| Continuous renal replacement therapy, n (%) | 25 (4.3) | 7 (12.3) | 18 (3.4) | 0.002 |
| Laboratory Parameters | Total (n = 580) | Non-Survivors (n = 57) | Survivors (n = 523) | p-Value |
|---|---|---|---|---|
| Hemoglobin (g/dL) | 11.2 ± 2.8 | 11.2 ± 3.4 | 11.6 ± 2.7 | 0.862 |
| Hematocrit (%) | 34.1 ± 8.7 | 34.7 ± 11.1 | 33.9 ± 8.4 | 0.559 |
| White blood cell count (×103 cell/mm3) * | 12.0 (8.8, 16.6) | 12.1 (7.7, 19.5) | 12.0 (9.0, 16.5) | 0.994 |
| Absolute neutrophil count | 7883.8 (4776.6, 11,733.8) | 8020.2 (3689.6, 13,156.6) | 7882.5 (4833.2, 11,707.5) | 0.878 |
| Absolute lymphocyte count | 2590.9 (1551.4, 4187.5) | 2333.4 (1210.7, 3695.1) | 2592.8 (1580.6, 4218.4) | 0.265 |
| Platelet count (×103 cell/mm3) * | 285 (181, 400) | 196 (86, 340) | 292 (194, 408) | <0.001 |
| Red blood cell distribution width (%) | 15.7 ± 2.8 | 18.2 ± 3.6 | 15.5 ± 2.5 | <0.001 |
| Mean corpuscular volume (fL) | 78.2 ± 9.1 | 81.1 ± 7.9 | 77.9 ± 9.2 | 0.014 |
| Red blood cell count (×103 cell/mm3) | 4.4 ± 1.2 | 4.3 ± 1.4 | 4.4 ± 1.1 | 0.633 |
| Nucleated red blood cell (%) * | 0 (0, 0.1) | 0.1 (0, 1.7) | 0 (0, 0.1) | <0.001 |
| Mean platelet volume (fL) | 9.9 ±1.0 | 10.4 ± 1.2 | 9.8 ± 0.9 | <0.001 |
| Platelet distribution width (PDW) | 10.8 ± 2.4 | 12.5 ± 3.0 | 10.7 ± 2.2 | <0.001 |
| Erythrocyte sedimentation rate (mm/h) * | 24 (9, 41) | 33 (16, 53) | 24 (9, 39) | 0.297 |
| C-reactive protein (mg/L) * | 15.5 (4.6, 62.5) | 36.6 (7.9, 113) | 15.1 (4.2, 62.4) | 0.323 |
| Lactate (mmol/L) * | 2.2 (1.3, 3.7) | 3.4 (2.1, 4.5) | 2.1 (1.3, 3.4) | 0.004 |
| Procalcitonin (ng/mL) * | 0.8 (0.2, 5.9) | 1.3 (0.4, 18.0) | 0.7 (0.2, 4.9) | 0.087 |
| Blood urea nitrogen (mg/dL) * | 10 (6, 16) | 13 (7, 27) | 9 (6, 15) | 0.002 |
| Creatinine (mg/dL) * | 0.3 (0.2, 0.5) | 0.5 (0.3, 0.8) | 0.3 (0.2, 0.4) | <0.001 |
| Albumin (g/dL) | 3.6 ± 0.7 | 3.4 ± 0.7 | 3.6 ± 0.7 | 0.084 |
| Aspartate transaminase (U/L) * | 41 (28, 79) | 56.5 (36, 169) | 40 (27, 73.5) | <0.001 |
| Alanine transaminase (U/L) * | 23.5 (14, 46) | 31.5 (19, 86) | 23 (14, 43) | 0.010 |
| Total bilirubin (mg/dL) * | 0.4 (0.2, 0.9) | 0.7 (0.3, 1.9) | 0.4 (0.2, 0.8) | 0.023 |
| Direct bilirubin (mg/dL) * | 0.2 (0.1, 0.5) | 0.3 (0.1, 0.8) | 0.2 (0.1, 0.4) | 0.011 |
| Parameters | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Unadjusted RR (95% CI) | p-Value | Adjusted RR (95% CI) | p-Value | |
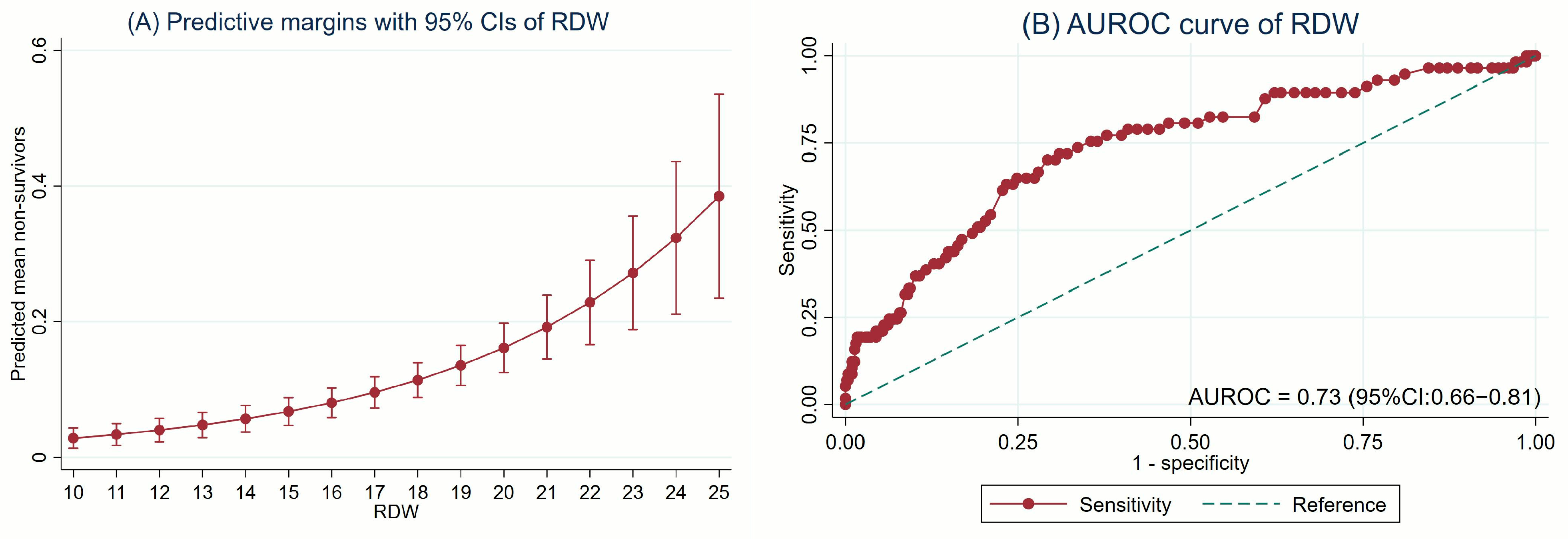
| RDW (%) | 1.25 (1.19–1.33) | <0.001 | 1.19 (1.13–1.25) | <0.001 |
| RDW ≥ 15% * | 3.82 (2.02–7.23) | <0.001 | 2.73 (1.45–5.13) | 0.002 |
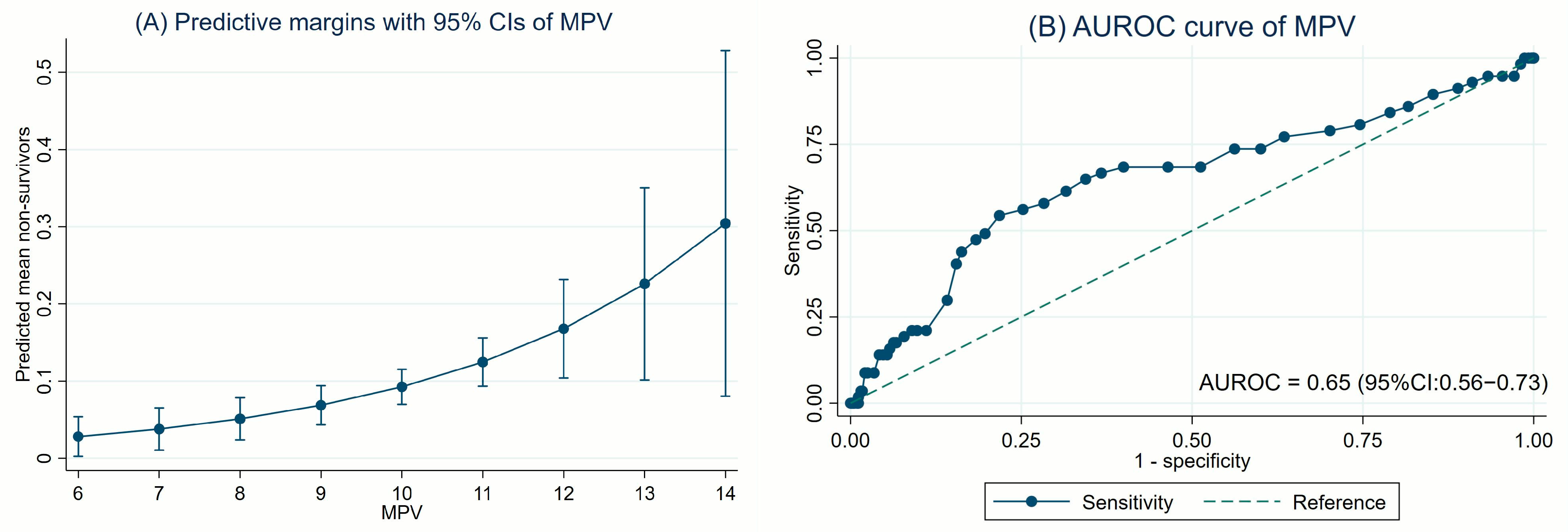
| MPV (fL) | 1.54 (1.25–1.89) | <0.001 | 1.34 (1.10–1.64) | 0.003 |
| MPV ≥ 10 fL * | 3.04 (1.79–5.15) | <0.001 | 2.38 (1.43–3.93) | 0.001 |
| Parameters | Non-Survivors (n = 57) | Survivors (n = 523) | Sensitivity | Specificity | PPV | NPV | AuROC |
|---|---|---|---|---|---|---|---|
| RDW ≥ 15% | 46 (80.7) | 257 (49.1) | 80.7% | 50.9% | 15.2% | 96.0% | 0.66 (0.60–0.71) |
| MPV ≥ 10 fL | 38 (66.7) | 192 (36.7) | 66.7% | 63.3% | 16.5% | 94.6% | 0.65 (0.58–0.71) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sunkonkit, K.; Chai-adisaksopha, C.; Natesirinilkul, R.; Phinyo, P.; Trongtrakul, K. Admission Red Blood Cell Distribution Width and Mean Platelet Volume as Predictors of Mortality in the Pediatric Intensive Care Unit: A Five-Year Single-Center Retrospective Study. J. Clin. Med. 2025, 14, 3839. https://doi.org/10.3390/jcm14113839
Sunkonkit K, Chai-adisaksopha C, Natesirinilkul R, Phinyo P, Trongtrakul K. Admission Red Blood Cell Distribution Width and Mean Platelet Volume as Predictors of Mortality in the Pediatric Intensive Care Unit: A Five-Year Single-Center Retrospective Study. Journal of Clinical Medicine. 2025; 14(11):3839. https://doi.org/10.3390/jcm14113839
Chicago/Turabian StyleSunkonkit, Kanokkarn, Chatree Chai-adisaksopha, Rungrote Natesirinilkul, Phichayut Phinyo, and Konlawij Trongtrakul. 2025. "Admission Red Blood Cell Distribution Width and Mean Platelet Volume as Predictors of Mortality in the Pediatric Intensive Care Unit: A Five-Year Single-Center Retrospective Study" Journal of Clinical Medicine 14, no. 11: 3839. https://doi.org/10.3390/jcm14113839
APA StyleSunkonkit, K., Chai-adisaksopha, C., Natesirinilkul, R., Phinyo, P., & Trongtrakul, K. (2025). Admission Red Blood Cell Distribution Width and Mean Platelet Volume as Predictors of Mortality in the Pediatric Intensive Care Unit: A Five-Year Single-Center Retrospective Study. Journal of Clinical Medicine, 14(11), 3839. https://doi.org/10.3390/jcm14113839