
Robotic vs. Laparoscopic Adrenalectomy for Pheochromocytoma—A Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
1. Introduction
2. Material and Methods
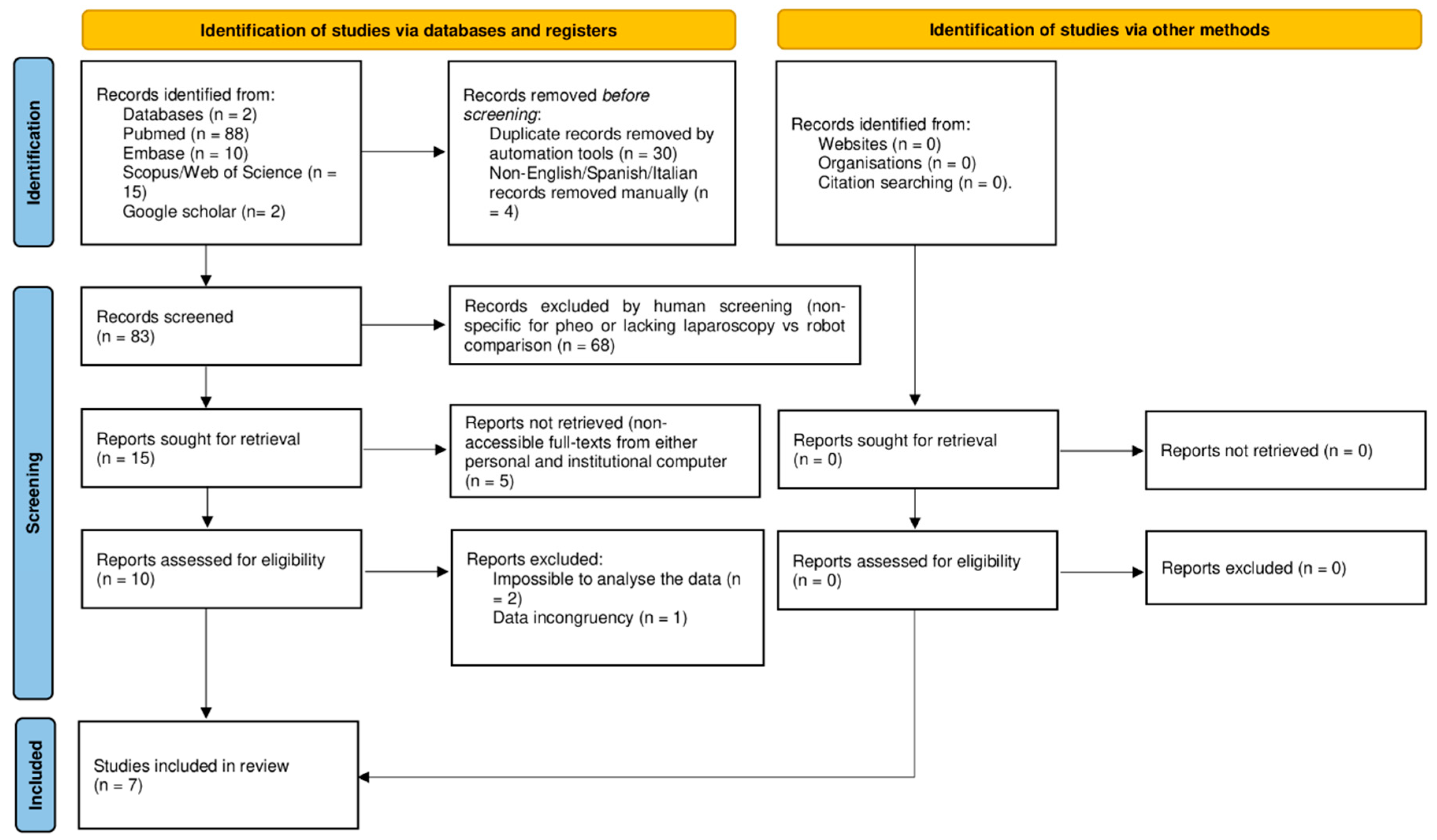
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Risk of Bias Assessment of Included Articles
2.5. Study Design
2.6. Statistical Analysis
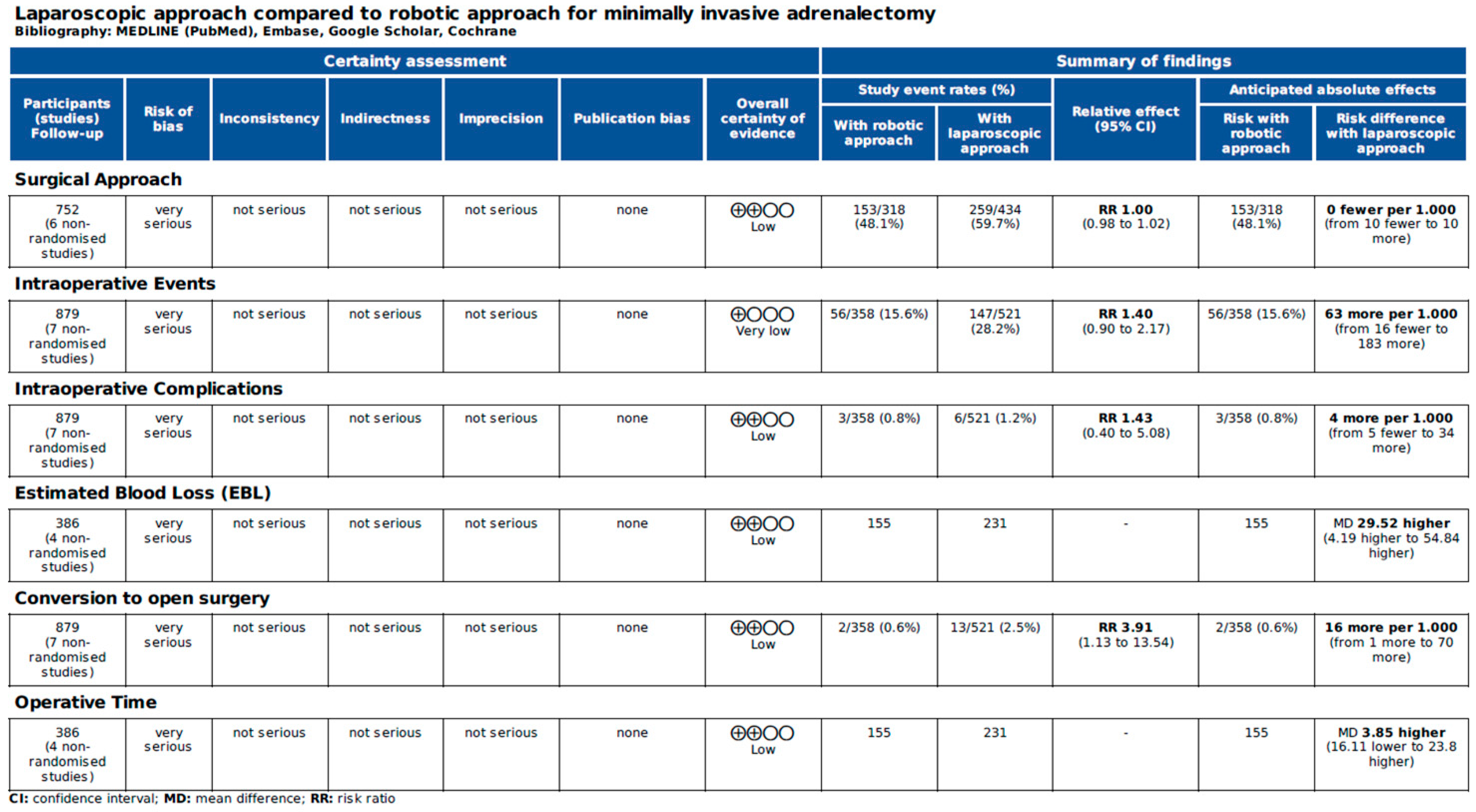
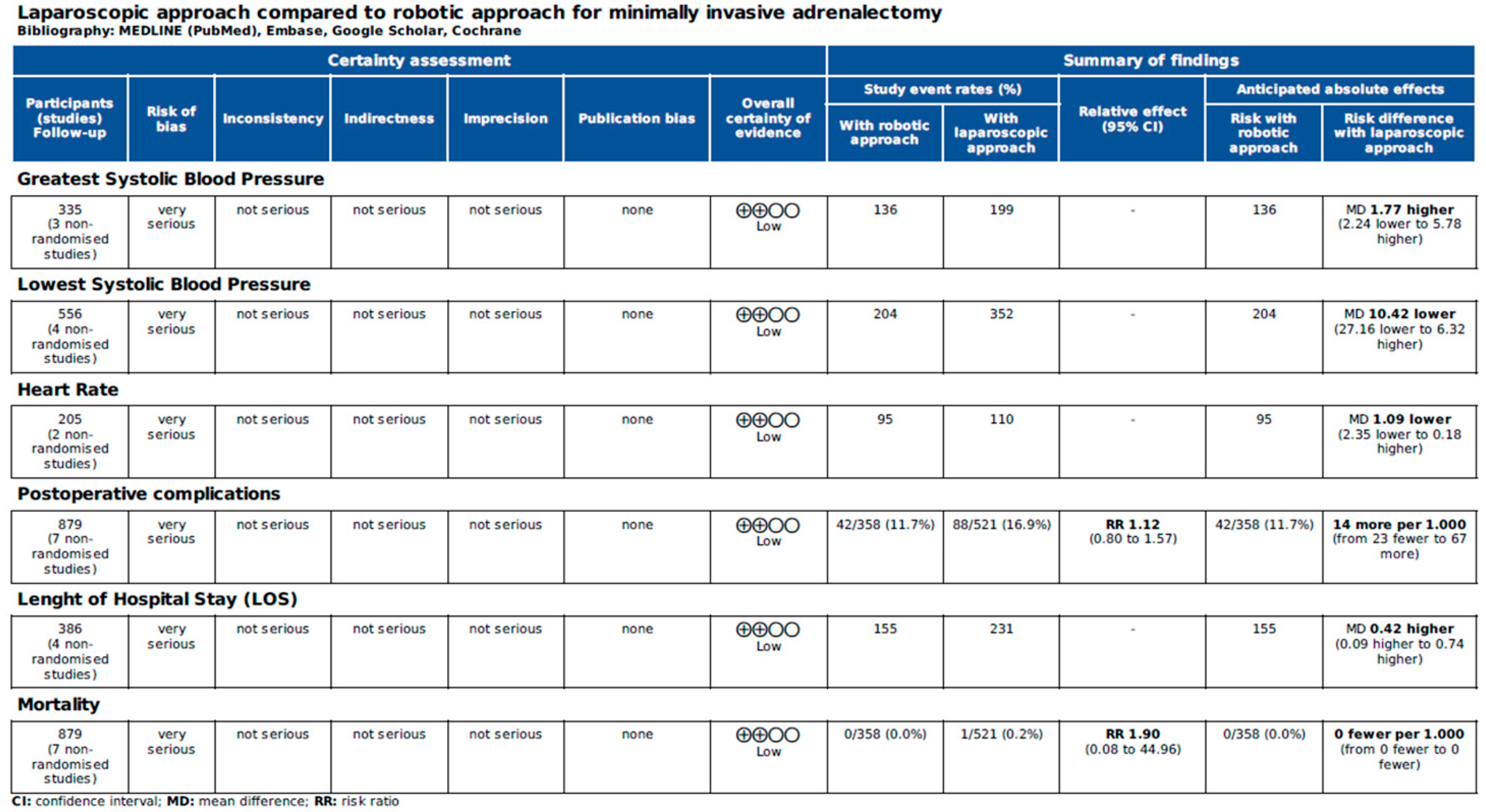
2.7. Grading the Quality of Evidence
3. Results
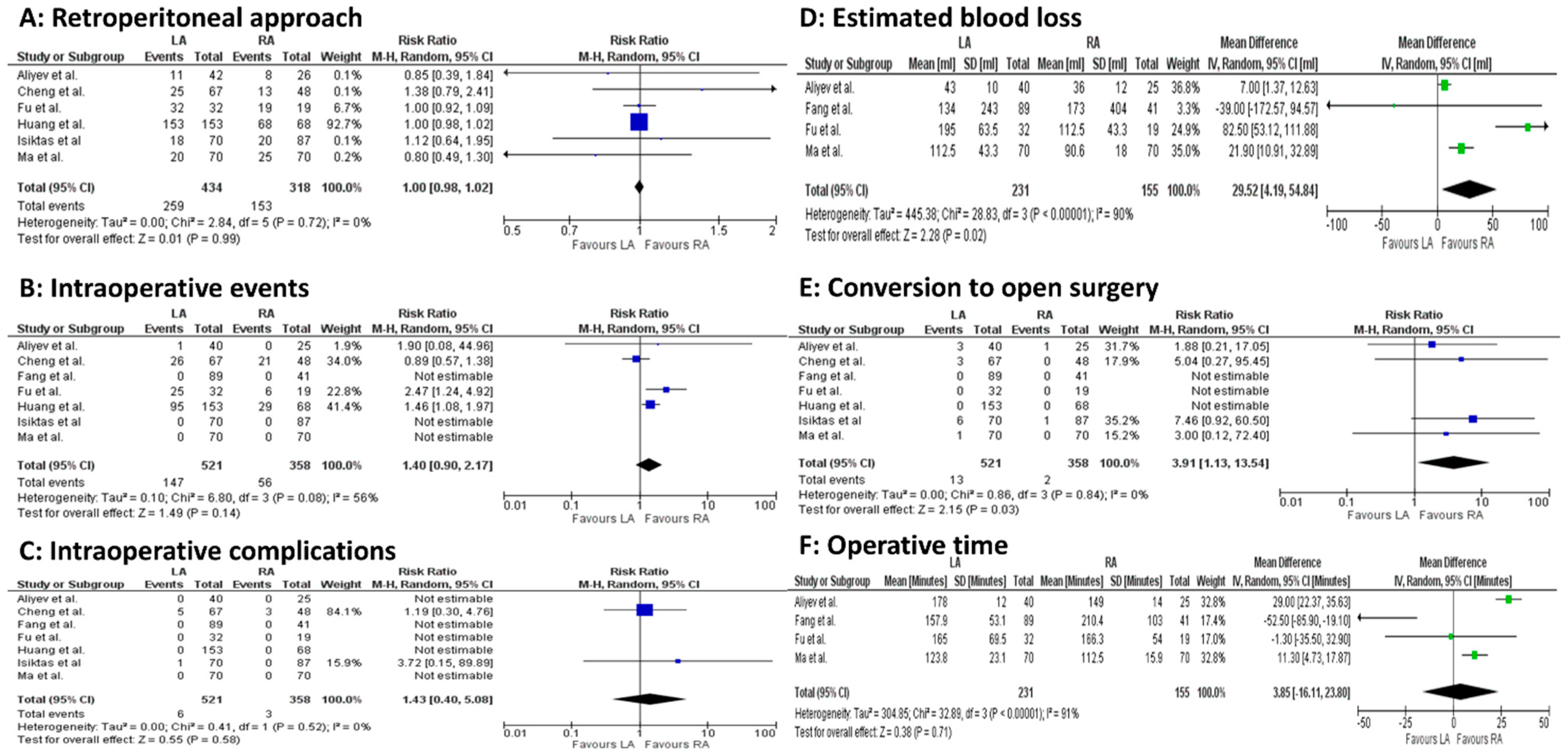
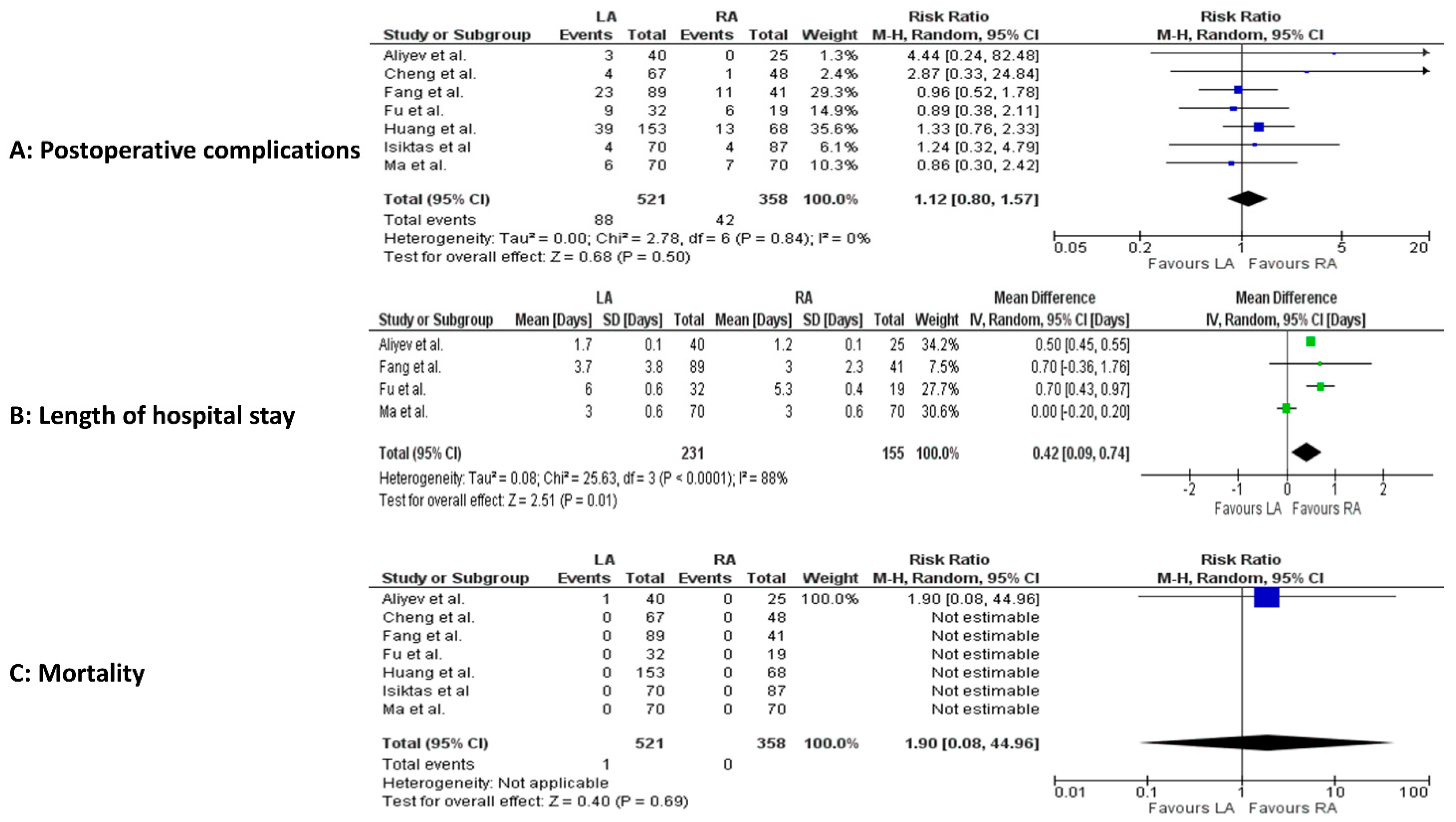
Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Omura, M.; Saito, J.; Yamaguchi, K.; Kakuta, Y.; Nishikawa, T. Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens. Res. 2004, 27, 193–202. [Google Scholar] [CrossRef]
- Zelinka, T.; Eisenhofer, G.; Pacak, K. Pheochromocytoma as a catecholamine producing tumor: Implications for clinical practice. Stress 2007, 10, 195–203. [Google Scholar] [CrossRef]
- Patel, D.; Phay, J.E.; Yen, T.W.F.; Dickson, P.V.; Wang, T.S.; Garcia, R.; Yang, A.D.; Solórzano, C.C.; Kim, L.T. Update on Pheochromocytoma and Paraganglioma from the SSO Endocrine/Head and Neck Disease-Site Work Group. Part 1 of 2: Advances in Pathogenesis and Diagnosis of Pheochromocytoma and Paraganglioma. Ann. Surg. Oncol. 2020, 27, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- De Crea, C.; Pennestri, F.; Voloudakis, N.; Sessa, L.; Procopio, P.F.; Gallucci, P.; Bellantone, R.; Raffaelli, M. Robot-assisted vs laparoscopic lateral transabdominal adrenalectomy: A propensity score matching analysis. Surg. Endosc. 2022, 36, 8619–8629. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Nissen, N.N.; Bannykh, S.I. Cardiac complications as initial manifestation of pheochromocytoma: Frequency, outcome, and predictors. Endocr. Pract. 2012, 18, 483–492. [Google Scholar] [CrossRef]
- Bihain, F.; Klein, M.; Nomine-Criqui, C.; Brunaud, L. Robotic adrenalectomy in patients with pheochromocytoma: A systematic review. Gland Surg. 2020, 9, 844–848. [Google Scholar] [CrossRef]
- Li, J.; Wang, Y.; Chang, X.; Han, Z. Laparoscopic adrenalectomy (LA) vs open adrenalectomy (OA) for pheochromocytoma (PHEO): A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2020, 46, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.Q.; Wang, S.Y.; Chen, Q.; Liu, Y.T.; Li, Z.L.; Sun, T. Laparoscopic versus open surgery for pheochromocytoma: A meta-analysis. BMC Surg. 2020, 20, 167. [Google Scholar] [CrossRef]
- Mihai, I.; Boicean, A.; Teodoru, C.A.; Grigore, N.; Iancu, G.M.; Dura, H.; Bratu, D.G.; Roman, M.D.; Mohor, C.I.; Todor, S.B.; et al. Laparoscopic Adrenalectomy: Tailoring Approaches for the Optimal Resection of Adrenal Tumors. Diagnostics 2023, 13, 3351. [Google Scholar] [CrossRef]
- Inaishi, T.; Kikumori, T.; Takeuchi, D.; Ishihara, H.; Miyajima, N.; Shibata, M.; Takano, Y.; Nakanishi, K.; Noda, S.; Kodera, Y. Obesity Does Not Affect Peri- and Postoperative Outcomes of Transabdominal Laparoscopic Adrenalectomy. Nagoya J. Med. Sci. 2018, 80, 21. [Google Scholar]
- Wang, L.; Zeng, W.; Wu, Y.; Gong, Z. Comparison of clinical efficacy and safety between robotic-assisted and laparoscopic adrenalectomy for pheochromocytoma: A systematic review and meta-analysis. J. Robot. Surg. 2024, 18, 115. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Li, J.; Peng, L.; Yang, X.; Xu, Y.; Li, X.; Li, Y.; Zhang, Z.; Wu, J. Comparison of Perioperative Outcomes of Robotic-Assisted vs Laparoscopic Adrenalectomy for Pheochromocytoma: A Meta-Analysis. Front. Oncol. 2021, 11, 724287. [Google Scholar] [CrossRef] [PubMed]
- Sforza, S.; Minervini, A.; Tellini, R.; Ji, C.; Bergamini, C.; Giordano, A.; Lu, Q.; Chen, W.; Zhang, F.; Ji, H.; et al. Perioperative outcomes of robotic and laparoscopic adrenalectomy: A large international multicenter experience. Surg. Endosc. 2021, 35, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Lee, K.Y.; Kim, J.K.; Yoon, D.S. The first laparoscopic resection of extra-adrenal pheochromocytoma using the da Vinci robotic system. J. Laparoendosc. Adv. Surg. Tech. A 2009, 19, 63–65. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 1 March 2025).
- Goossen, K.; Tenckhoff, S.; Probst, P.; Grummich, K.; Mihaljevic, A.L.; Büchler, M.W.; Diener, M.K. Optimal literature search for systematic reviews in surgery. Langenbecks Arch. Surg. 2018, 403, 119–129. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45 Pt A, 139–145. [Google Scholar] [CrossRef]
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University and Evidence Prime. 2024. Available online: https://gradepro.org (accessed on 1 March 2025).
- Aliyev, S.; Karabulut, K.; Agcaoglu, O.; Wolf, K.; Mitchell, J.; Siperstein, A.; Berber, E. Robotic versus laparoscopic adrenalectomy for pheochromocytoma. Ann. Surg. Oncol. 2013, 20, 4190–4194. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Mao, Y.; Zhuo, R.; Dai, J.; Fang, C.; Wang, C.; Zhao, J.; He, W.; Zhu, Y.; Xu, D.; et al. Surgical outcomes of a randomized controlled trial compared robotic versus laparoscopic adrenalectomy for pheochromocytoma. Eur. J. Surg. Oncol. 2020, 46 Pt A, 1843–1847. [Google Scholar] [CrossRef]
- Fu, S.Q.; Zhuang, C.S.; Yang, X.R.; Xie, W.J.; Gong, B.B.; Liu, Y.F.; Liu, J.; Sun, T.; Ma, M. Comparison of robot-assisted retroperitoneal laparoscopic adrenalectomy versus retroperitoneal laparoscopic adrenalectomy for large pheochromocytoma: A single-centre retrospective study. BMC Surg. 2020, 20, 227. [Google Scholar] [CrossRef] [PubMed]
- Fang, A.M.; Rosen, J.; Saidian, A.; Bae, S.; Tanno, F.Y.; Chambo, J.L.; Bloom, J.; Gordetsky, J.; Srougi, V.; Phillips, J.; et al. Perioperative outcomes of laparoscopic, robotic, and open approaches to pheochromocytoma. J. Robot. Surg. 2020, 14, 849–854. [Google Scholar] [CrossRef]
- Isiktas, G.; Nazli Avci, S.; Ergun, O.; Krishnamurthy, V.; Jin, J.; Siperstein, A.; Berber, E. Laparoscopic versus robotic adrenalectomy in pheochromocytoma patients. J. Surg. Oncol. 2022, 126, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Zhu, Y. Comparison of Perioperative Outcomes Between Laparoscopic and Robot-Assisted Adrenalectomy for Large Pheochromocytoma (≥5 cm): A Retrospective Study. Cancer Manag. Res. 2023, 15, 1207–1216. [Google Scholar] [CrossRef]
- Huang, H.; Sun, T.; Liu, Z. Robot-assisted versus laparoscopic pheochromocytoma resection and construction of a nomogram to predict perioperative hemodynamic instability. Eur. J. Surg. Oncol. 2024, 50, 107986. [Google Scholar] [CrossRef]
- Giordano, A.; Alemanno, G.; Bergamini, C.; Valeri, A.; Prosperi, P. Laparoscopic adrenalectomy for giant adrenal tumours: Technical considerations and surgical outcome. J. Minimal Access Surg. 2021, 17, 76–80. [Google Scholar] [CrossRef]
- Öz, B.; Cücük, Ö.; Gök, M.; Akcan, A.; Sözüer, E. Laparoscopic transperitoneal adrenalectomy for adrenal tumours of 6 cm or greater: A single-centre experience. J. Minimal Access Surg. 2024, 20, 47–54. [Google Scholar] [CrossRef]
- Gagner, M.; Lacroix, A.; Bolté, E. Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N. Engl. J. Med. 1992, 327, 1033. [Google Scholar] [CrossRef]
- Giordano, A.; Feroci, F.; Podda, M.; Botteri, E.; Ortenzi, M.; Montori, G.; Guerrieri, M.; Vettoretto, N.; Agresta, F.; Bergamini, C. Minimally invasive versus open adrenalectomy for adrenocortical carcinoma: The keys surgical factors influencing the outcomes-a collective overview. Langenbecks Arch. Surg. 2023, 408, 256. [Google Scholar] [CrossRef]
- Ortenzi, M.; Balla, A.; Ghiselli, R.; Vergari, R.; Silecchia, G.; Guerrieri, E.; Maria Paganini, A.; Guerrieri, M. Minimally invasive approach to the adrenal gland in obese patients with Cushing’s syndrome. Minim. Invasive Ther. Allied Technol. 2019, 28, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Verhoeff, K.; Parente, A.; Wang, Y.; Wang, N.; Wang, Z.; Śledziński, M.; Hellmann, A.; Raffaelli, M.; Pennestrì, F.; Sywak, M.; et al. Outcomes for Patients with Obesity Undergoing Adrenalectomy for Pheochromocytoma: An International Multicenter Analysis. Ann. Surg. Oncol. 2025, 32, 1709–1720. [Google Scholar] [CrossRef]
- Du, L.; Yang, Z.; Qi, J.; Wang, Y. Robotic adrenalectomy versus laparoscopic adrenalectomy for pheochromocytoma: A systematic review and meta-analysis. Wideochir. Inne Tech. Maloinwazyjne 2022, 17, 1–8. [Google Scholar] [CrossRef]
- Balla, A.; Corallino, D.; Ortenzi, M.; Palmieri, L.; Meoli, F.; Guerrieri, M.; Paganini, A.M. Cancer risk in adrenalectomy: Are adrenal lesions equal or more than 4 cm a contraindication for laparoscopy? Surg. Endosc. 2022, 36, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Alzelfawi, L.; Almajed, E.; Alhindawi, Z.; AlDosari, L.; Alhumaidan, A.; Alharthi, B. Feasibility of laparoscopic adrenalectomy in adrenal masses greater than 5 centimeters: A systematic review and meta-analysis. Gland Surg. 2024, 13, 952–968. [Google Scholar] [CrossRef]
- Alberici, L.; Paganini, A.M.; Ricci, C.; Balla, A.; Ballarini, Z.; Ortenzi, M.; Casole, G.; Quaresima, S.; Di Dalmazi, G.; Ursi, P.; et al. Development and validation of a preoperative “difficulty score” for laparoscopic transabdominal adrenalectomy: A multicenter retrospective study. Surg. Endosc. 2022, 36, 3549–3557. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Hu, K.; Qing, J.; Chen, J.; Li, C.; Zhou, Y. Hyper-realistic rendering-assisted laparoscopic adrenalectomy for giant adrenal tumors: A pilot study. World J. Urol. 2024, 42, 550. [Google Scholar] [CrossRef]
- Gaillard, M.; Razafinimanana, M.; Challine, A.; Araujo, R.L.C.; Libé, R.; Sibony, M.; Barat, M.; Bertherat, J.; Dousset, B.; Fuks, D.; et al. Laparoscopic or Open Adrenalectomy for Stage I–II Adrenocortical Carcinoma: A Retrospective Study. J. Clin. Med. 2023, 12, 3698. [Google Scholar] [CrossRef]
- Paganini, A.M.; Balla, A.; Guerrieri, M.; Lezoche, G.; Campagnacci, R.; D’Ambrosio, G.; Quaresima, S.; Antonica, M.V.; Lezoche, E. Laparoscopic transperitoneal anterior adrenalectomy in pheochromocytoma: Experience in 62 patients. Surg. Endosc. 2014, 28, 2683–2689. [Google Scholar] [CrossRef]
- Chai, Y.J.; Yu, H.W.; Song, R.Y.; Kim, S.J.; Choi, J.Y.; Lee, K.E. Lateral transperitoneal adrenalectomy versus posterior retroperitoneoscopic adrenalectomy for benign adrenal gland disease: Randomized controlled trial at a single tertiary medical centre. Ann. Surg. 2019, 269, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Tai, Y.; Shang, J. Progress in treatment and follow-up of pheochromocytoma. Eur. J. Surg. Oncol. 2025, 51, 110144. [Google Scholar] [CrossRef] [PubMed]
- Habeeb, T.A.A.M.; Elias, A.A.; Adam, A.A.M.; Gadallah, M.A.; Ahmed, S.M.A.; Khyrallh, A.; Alsayed, M.H.; Awad, E.T.K.; Ibrahim, E.A.; Labib, M.F.; et al. Early readmission after adrenalectomy for pheochromocytoma. A retrospective study. Langenbecks Arch. Surg. 2025, 410, 154. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assessment of risk of bias based on Risk of Bias In Non-randomised Studies—of Interventions (ROBINS-I) | ||||||||
| Author, year, type of study | Bias due to confounding | Bias in selection of participants for the study | Bias in classification of interventions | Bias due to deviations from intended interventions | Bias due to missing data | Bias in measurement of outcomes | Bias in selection of reported result | Overall |
| Aliyev, 2013, retrospective [23] | Low | Serious | Low | Low | Low | Low | Low | Serious |
| Fu, 2020, retrospective [25] | Low | Serious | Low | Low | Low | Low | Low | Serious |
| Fang, 2020, retrospective [26] | Low | Serious | Moderate | Low | Moderate | Low | Moderate | Serious |
| Isiktas, 2022, retrospective [27] | Low | Serious | Low | Low | Low | Low | Moderate | Serious |
| Cheng, 2023, retrospective [28] | Low | Serious | Low | Low | Low | Low | Moderate | Serious |
| Huang, 2024, retrospective [29] | Low | Serious | Low | Low | Low | Low | Moderate | Serious |
| Assessment of risk of bias based on Cochrane Risk of Bias 2.0 (RoB 2.0) tool for randomized trials | ||||||||
| Author, year, type of study | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported results | Overall | ||
| Ma, 2020, randomized control trial [24] | Low | Low | Moderate | Low | Moderate | Moderate | ||
| Author | Number of Patients | Sex Men:Women, n (%) | Mean Age ± Standard Deviation, Years | Mean Body Mass Index ± Standard Deviation, Kg/m2 | Lesion Side, Right:Left:Bilateral n (%) | Mean Lesion Size ± Standard Deviation, cm | American Society of Anesthesiologists Grade, n (%) |
|---|---|---|---|---|---|---|---|
| Aliyev et al. [23] | LA: 40 | 20 (50):20 (50) | 51.3 ± 2.5 | 28.7 ± 1.1 | 19 (47.5):19 (47.5):2 (5) | 4.4 ± 0.4 | n.r. |
| RA: 25 | 7 (28):18 (72) | 50.9 ± 3.4 | 27.6 ± 1.5 | 14 (56):10 (40):1 (4) | 5.5 ± 0.5 | n.r. | |
| Ma et al. [24] | LA: 70 | 39 (55.7):31 (44.3) | Median 50 (IQR 35–58) | Median 22.8 (IQR 20.8–25.1) | 36 (51.4):34 (48.6) | Median 4 (IQR 3–6) | II: 40 (57.1), III: 29 (41.4), IV: 1 (1.4) |
| RA: 70 | 37 (52.9):33 (47.1) | Median 44 (IQR 34.5–53.5) | Median 21.9 (IQR 19.6–23.9) | 32 (45.7):38 (54.3) | Median 4.6 (IQR 3.8–5.6) | II: 37 (52.9), III: 31 (44.3), IV: 2 (2.9) | |
| Fu et al. [25] | LA: 32 | 15 (46.9):17 (53.1) | 47.5 ± 14.5 | 25.8 ± 4.4 | 16 (50):16 (50) | Median 7.6 (IQR 6.6–9) | I–II: 7 (21.9), III–IV: 25 (78.1) |
| RA: 19 | 11 (57.9):8 (42.1) | 44 ± 9.1 | 26.6 ± 3.8 | 10 (52.6):9 (47.4) | Median 8 (IQR 6–9) | I–II: 1 (5.3), III–IV: 18 (94.7) | |
| Fang et al. [26] | LA: 89 | 38 (42.7):51 (57.3) | 46.2 ± 17.9 SEM | 24.5 ± 4.9 SEM | 48 (53.9):33 (37.1):8 (9) | 4.6 ± 2.5 SEM | n.r. |
| RA: 41 | 22 (53.7):19 (46.3) | 55.9 ± 15.4 SEM | 29.8 ± 6.5 SEM | 23 (56.1):18 (43.9) | 6.2 ± 8.4 SEM | n.r. | |
| Isiktas et al. [27] | LA: 70 | 35 (50):35 (50) | Median 51.6 (IQR 18.3) | Median 29.1 (IQR 10.4) | 32 (45.7):38 (54.3) | Median 4.1 (IQR 2.3) | n.r. |
| RA: 87 | 26 (29.9):61 (70.1) | Median 48.7 (IQR 28) | Median 28.6 (IQR 7.4) | 46 (52.9):41 (47.1) | Median 3.6 (IQR 2.5) | n.r. | |
| Cheng et al. [28] | LA: 67 | 31 (46.3):36 (53.7) | 45 (range 33–60) | 22.6 (range 20.9–25.4) | 32 (47.8):35 (52.2) | 6 (range 5.5–7) | I–II: 55 (82.1), III–IV: 12 (17.9) |
| RA: 48 | 21 (43.8):27 (56.2) | 43.5 (range 32.5–58) | 23.1 (range 21.9–24.5) | 18 (37.5):30 (62.5) | 6 (range 5.5–7.3) | I–II: 44 (91.7), III–IV: 4 (8.3) | |
| Huang et al. [29] | LA: 153 | 72 (47.1):81 (52.9) | 47.2 ± 13.7 | 22.2 ± 3.6 | 82 (53.6):71 (46.4) | 4.5 ± 1.8 | I–II: 26 (17), III–IV: 127 (83) |
| RA: 68 | 31 (45.6):37 (54.4) | 46.4 ± 12.5 | 22 ± 2.6 | 36 (52.9):32 (47.1) | 5.6 ± 2 | I–II: 8 (11.8), III–IV: 60 (88.2) |
| Author | Number of Patients | Approach, n (%) | Intraoperative Events/Complications, n (%) | Mean EBL ± SD, ml | Mean SBP ± SD, mmHg. Greatest HR, n (%) | Conversion to Open Surgery, n (%) | Mean Operative Time ± SD, Minutes | Postoperative Complications, n (%) | Mean LOS ± SD, Days | Mortality, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Aliyev et al. [23] | LA: 40 a | Lateral transperitoneal: 31 (73.8) Posterior retroperitoneal: 11 (26.2) | Cardiac arrhythmia: 1 (2.5) | 43 ± 10 | Greatest: 173 ± 4 Lowest: 102 ± 2 HR: 92 ± 2 | Tumor bleeding: 1 (2.5) Accessory renal vein bleeding: 1 (2.5) Difficult dissection: 1 (2.5) | 178 ± 12 | Cardiac arrhythmia: 2 (5) Pleural effusion: 1 (2.5) | 1.7 ± 0.1 | Cardiac arrhythmia: 1 (2.5) |
| RA: 25 b | Lateral transperitoneal: 18 (69.2) Posterior retroperitoneal: 8 (30.8) | - | 36 ± 12 | Greatest: 174 ± 6 Lowest: 97 ± 3 HR: 92 ± 4 | Tumor adhesions: 1 (4) | 149 ± 14 | - | 1.2 ± 0.1 | - | |
| Ma et al. [24] | LA: 70 | Transperitoneal: 50 (71.4) Retroperitoneal: 20 (28.6) | - | Median 100 (IQR 50–200) | Greatest median: 140 (IQR 123–170) Lowest median: 80 (IQR 80–90) Median HR: 95 (IQR 85–105) | 1 (1.4) | Median 122.5 (IQR 85–165) | Pneumonia: 6 (8.6) Transfusion: 2 (2.9) | Median 3 (IQR 2–4) | - |
| RA: 70 | Transperitoneal: 45 (64.3) Retroperitoneal: 25 (35.7) | - | Median 100 (IQR 50–112.5) | Greatest median: 139 (IQR 125–155) Lowest median: 83 (IQR 80–95) Median HR: 95 (IQR 90–110) | - | Median 107.5 (IQR 90–145) | Pneumonia: 7 (10) Transfusion: 4 (5.7) | Median 3 (IQR 2–4) | - | |
| Fu et al. [25] | LA: 32 | Retroperitoneal | Transfusion: 7 (21.9) Hemodynamic instability: 18 (56.2) | Median 200 (IQR 80–300) | n.r. | - | 165 ± 69.5 | 9 (28.1) | Median 6 (IQR 5–7) | - |
| RA: 19 | Retroperitoneal | Transfusion: 1 (5.3) Hemodynamic instability: 5 (26.3) | Median 100 (IQR 50–200) | n.r. | - | 166.3 ± 54 | 6 (31.6) | Median 5 (IQR 5–6) | - | |
| Fang et al. [26] | LA: 89 c | n.r. | - | 134 ± 243 SEM | Greatest: 175.3 ± 25.4 SEM Lowest: 86.1 ± 16.7 SEM | - | 157.9 ± 53.1 SEM | 23 (25.8) | 3.7 ± 3.8 SEM | - |
| RA: 41 | n.r. | - | 173 ± 404 SEM | Greatest: 169.8 ± 24.2 SEM Lowest: 78.8 ± 17.9 SEM | - | 210.4 ± 103 SEM | 11 (26.8) | 3 ± 2.3 SEM | - | |
| Isiktas et al. [27] | LA: 70 | Lateral transperitoneal: 52 (74.3) Posterior retroperitoneal: 18 (25.7) | Spleen bleeding requiring splenectomy: 1 (1.4) | Median 99.9 (IQR 65) | n.r. | Inadequate surgical field exposure: 2 (2.9) Spleen bleeding: 1 (1.4) Difficult dissection for adrenal mass: 3 (4.3) | Median 180.2 (IQR 22.6) | Renal failure 1 (1.4) Acute respiratory distress syndrome: 1 (1.4) Hyponatremia: 1 (1.4) Intra-abdominal abscess: 1 (1.4) | Median 2.2 (IQR 1) | - |
| RA: 87 | Lateral transperitoneal: 67 (77) Posterior retroperitoneal: 20 (23) | - | Median 36.3 (IQR 35) | n.r. | Inadequate surgical exposure: 1 (1.5) | Median 166.2 (IQR 60.5) | Urinary tract infection: 2 (2.3) Pneumonia: 1 (1.1) Volume overload: 1 (1.1) | Median 1.3 (IQR 0) | - | |
| Cheng et al. [28] | LA: 67 | Transperitoneal: 42 (62.7) Retroperitoneal: 25 (37.3) | Hypertensive crisis: 8 (11.9) Organ injury requiring suture: 2 (3) Cava injury requiring suture: 1 (1.5) Bleeding: 1 (1.5) Suspecting spleen rupture requiring open exploration: 1 (1.5) Transfusion: 18 (26.9) | 120 (range 100–200) | n.r. | 3 (4.5) | 220 (range 190–260) | Electrolyte imbalance: 1 (1.5) Fever: 1 (1.5) Pneumonia: 1 (1.5) Heart failure: 1 (1.5) Transfusion: 14 (20.9) | 13 (range 8–21) | - |
| RA: 48 | Transperitoneal: 35 (72.9) Retroperitoneal: 13 (27.1) | Ventricular fibrillation: 1 (2.1) Hypertensive crisis: 2 (4.2) Organ injury requiring suture: 1 (2.1) Bleeding: 1 (2.1) Diaphragmatic rupture requiring suture: 1 (2.1) Transfusion: 18 (37.5) | 50 (range 30–212.5) | n.r. | - | 190 (range 170–215) | Electrolyte imbalance: 1 (2.1) Transfusion: 13 (27.1) | 12.5 (range 8–18) | - | |
| Huang et al. [29] | LA: 153 | Retroperitoneal | Hemodynamic instability: 95 (62.1) | 100 (range 50–200) | Greatest: 160 (range 145.5–175.5) Lowest: 94.6 ± 12.3 | - | 145 (range 115–190) | 39 (25.5) | 6 (range 5–7) | - |
| RA: 68 | Retroperitoneal | Hemodynamic instability: 29 (42.6) | 100 (range 50–200) | Greatest: 161 (range 140.5–179.5) Lowest: 95.5 ± 12.7 | - | 150 (range 120–193.8) | 13 (19.1) | 6 (range 6–7) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giordano, A.; Balla, A.; Prosperi, P.; Morales-Conde, S.; Bergamini, C. Robotic vs. Laparoscopic Adrenalectomy for Pheochromocytoma—A Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 3806. https://doi.org/10.3390/jcm14113806
Giordano A, Balla A, Prosperi P, Morales-Conde S, Bergamini C. Robotic vs. Laparoscopic Adrenalectomy for Pheochromocytoma—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2025; 14(11):3806. https://doi.org/10.3390/jcm14113806
Chicago/Turabian StyleGiordano, Alessio, Andrea Balla, Paolo Prosperi, Salvador Morales-Conde, and Carlo Bergamini. 2025. "Robotic vs. Laparoscopic Adrenalectomy for Pheochromocytoma—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 14, no. 11: 3806. https://doi.org/10.3390/jcm14113806
APA StyleGiordano, A., Balla, A., Prosperi, P., Morales-Conde, S., & Bergamini, C. (2025). Robotic vs. Laparoscopic Adrenalectomy for Pheochromocytoma—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 14(11), 3806. https://doi.org/10.3390/jcm14113806