
EEG Maturational Age Estimation: A Comparison of Visual and Automated Interpretation of the EEG in Preterm Infants

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. EEG Data
2.3. Statistical Analysis
3. Results
3.1. Patients
3.2. EEG Data
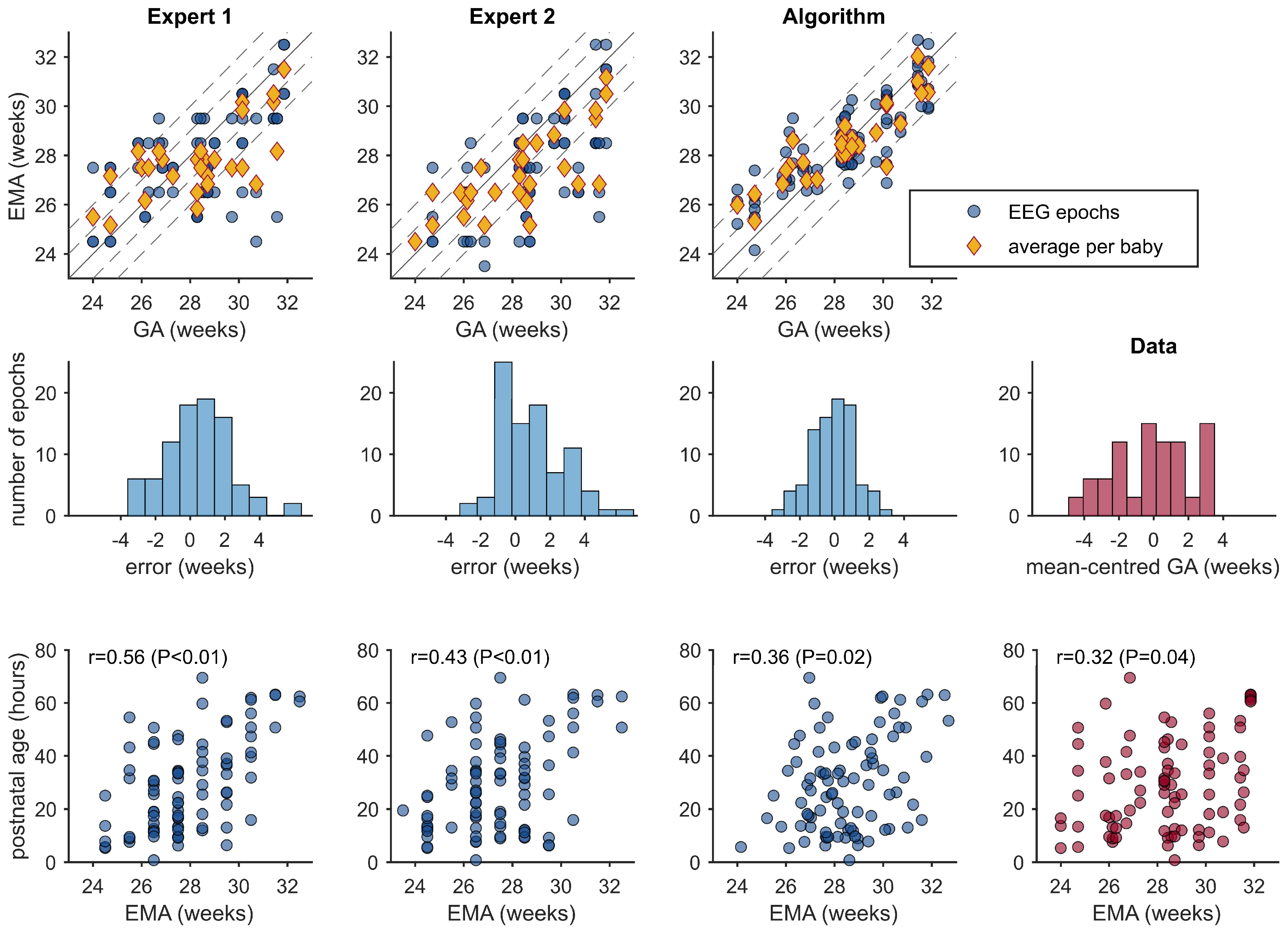
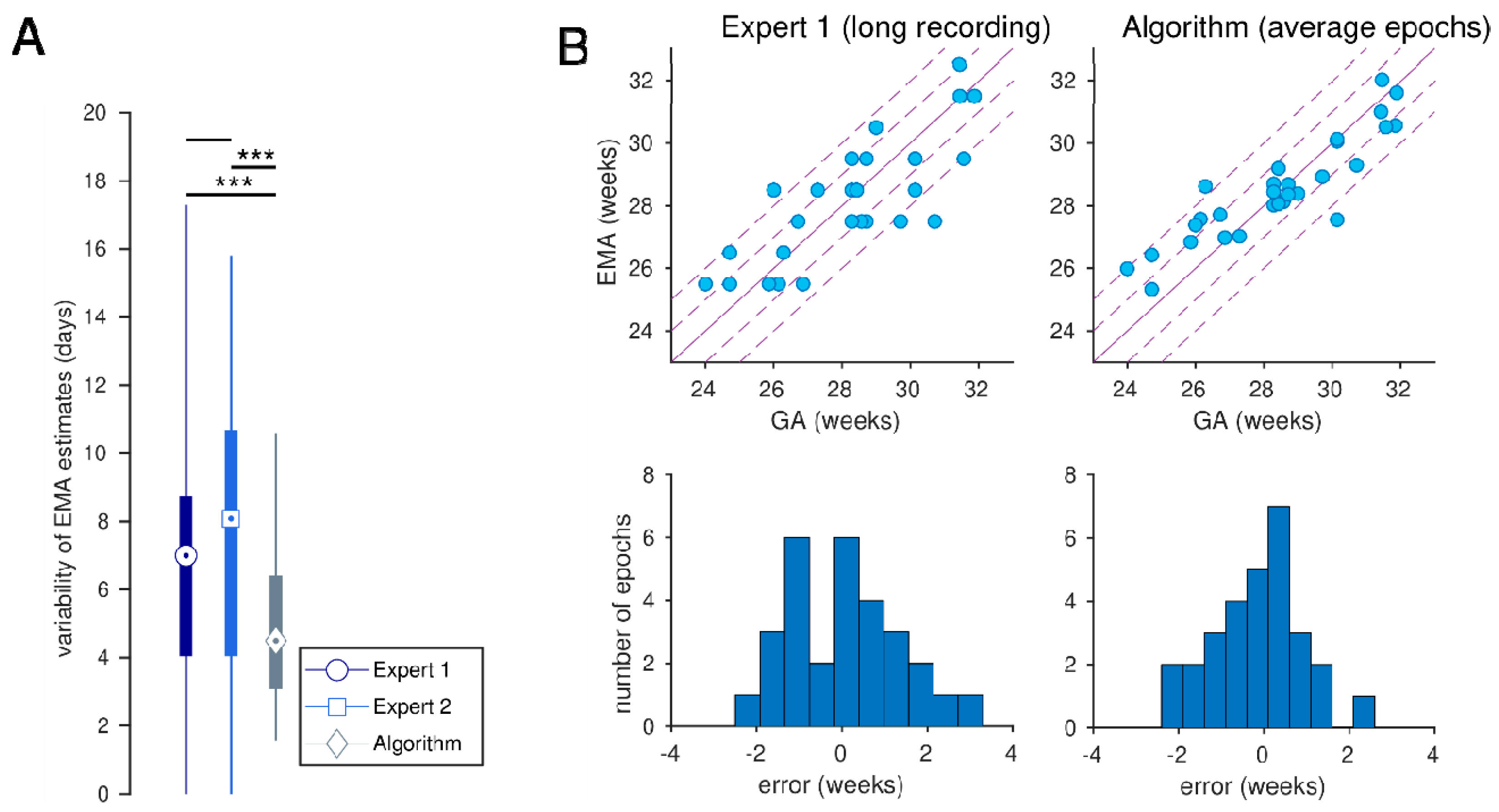
3.3. EMA Estimations
3.4. Mixed-Effects Models Postnatal Age
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EMA | EEG maturational age |
| PNA | Post-natal age |
| GA | Gestational age |
| NICU | Neonatal Intensive Care Unit |
| ICH-GCP | International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use of Good Clinical Practice |
| IVH | Intra-ventricular hemorrhage |
| PVL | Periventricular leukomalacia |
| EEG | Electroencephalogram |
| SD | Standard deviation |
| SDE | Standard deviation error |
| CRIB | Clinical risk for babies |
| IQR | Interquartile range |
References
- Hagen, C.M.; Hansen, T.W. Deaths in a neonatal intensive care unit: A 10-year perspective. Pediatr. Crit. Care Med. 2004, 5, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.; Hennessy, E.M.; Myles, J.; Johnson, S.J.; Draper, E.S.; Costeloe, K.L.; Marlow, N. Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: The EPICure studies. BMJ 2012, 345, e7961. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus-Brisac, C. The electroencephalogram of the premature infant. Wld. Neurol. 1962, 3, 5–15. [Google Scholar]
- Dreyfus-Brisac, C.; Flescher, J.; Plassart, E. L’électroencéphalogramme: Critère d’âge conceptionnel du nouveau-né à terme et prématuré. Biol. Neonat. 1962, 4, 154–173. [Google Scholar] [CrossRef]
- Dreyfus-Brisac, C. The electroencephalogram of the premature infant and full-term newborn: Normal and abnormal development of waking and sleeping patterns. In Neurological and Electroencephalographic Correlative Studies in Infancy; Kelleway, P., Petersén, I., Eds.; Grune and Stratton: New York, NY, USA, 1964; pp. 186–207. [Google Scholar]
- Dreyfus-Brisac, C. Ontogénèse du sommeil chez le premature humain: Etude polygraphique. In Regional Development of the Brain in Early Life; Minkowski, A., Ed.; Blackwell: Oxford, UK, 1967; pp. 437–457. [Google Scholar]
- Scher, M.S.; Steppe, D.A.; Dokianakis, S.G.; Guthrie, R.D. Maturation of phasic and continuity measures during sleep in preterm neonates. Pediatr. Res. 1994, 36, 732–737. [Google Scholar] [CrossRef]
- Scher, M.S.; Steppe, D.A.; Banks, D.L.; Guthrie, R.D.; Sclabassi, R.J. Maturational trends of EEG-sleep measures in the healthy preterm neonate. Pediatr. Neurol. 1995, 12, 314–322. [Google Scholar] [CrossRef]
- Selton, D.; Andre, M.; Hascoët, J.M. Normal EEG in very premature infants: Reference criteria. Clin. Neurophysiol. 2000, 111, 2116–2124. [Google Scholar] [CrossRef]
- Vecchierini, M.F.; d’Allest, A.M.; Verpillat, P. EEG patterns in 10 extreme premature neonates with normal neurological outcome: Qualitative and quantitative data. Brain Dev. 2003, 25, 330–337. [Google Scholar] [CrossRef]
- Biagioni, E.; Frisone, M.F.; Laroche, S.; Kapetanakis, B.A.; Ricci, D.; Adeyi-Obe, M.; Lewis, H.; Kennea, N.; Cioni, G.; Cowan, F.; et al. Maturation of cerebral electrical activity and development of cortical folding in young very preterm infants. Clin. Neurophysiol. 2007, 118, 53–59. [Google Scholar] [CrossRef]
- Vecchierini, M.F.; André, M.; d’Allest, A.M. Normal EEG of premature infants born between 24 and 30 weeks gestational age: Terminology, definitions and maturation aspects. Neurophysiol. Clin. 2007, 37, 311–323. [Google Scholar] [CrossRef]
- André, M.; Lamblin, M.D.; d’Allest, A.M.; Curzi-Dascalova, L.; Moussalli-Salefranque, F.; SNguyenThe, T.; Vecchierini-Blineau, M.F.; Wallois, F.; Walls-Esquivel, E.; Plouin, P. Electroencephalography in premature and full-term infants. Developmental features and glossary. Neurophysiol. Clin. 2010, 40, 59–124. [Google Scholar] [CrossRef] [PubMed]
- Niemarkt, H.J.; Andriessen, P.; Peters, C.H.; Pasman, J.W.; Zimmermann, L.J.; BambangOetomo, S. Quantitative analysis of maturational changes in EEG background activity in very preterm infants with a normal neurodevelopment at 1 year of age. Early Hum. Dev. 2010, 86, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, E.; Lloyd, R.O.; Mathieson, S.; Boylan, G.B. A review of important electroencephalogram features for the assessment of brain maturation in premature infants. Acta Paediatr. 2017, 106, 1394–1408. [Google Scholar] [CrossRef]
- Watanabe, K.; Hayakawa, F.; Okumura, A. Neonatal EEG: A powerful tool in the assessment of brain damage in preterm infants. Brain Dev. 1999, 21, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Meijer, R.F.; Wang, X.; van Ooijen, I.M.; van der Velde, B.; Dudink, J.; Benders, M.J.N.L.; Tataranno, M.L. The relationship between early life EEG and brain MRI in preterm infants: A systematic review. Clin. Neurophysiol. 2025, 170, 168–179. [Google Scholar] [CrossRef]
- Beniczky, S.; Aurlien, H.; Brøgger, J.C.; Fuglsang-Frederiksen, A.; Martins-da-Silva, A.; Trinka, E.; Visser, G.; Rubboli, G.; Hjalgrim, H.; Stefan, H.; et al. Standardized computer-based organized reporting of EEG: SCORE. Epilepsia 2013, 54, 1112–1124. [Google Scholar] [CrossRef]
- Beniczky, S.; Aurlien, H.; Brøgger, J.C.; Hirsch, L.J.; Schomer, D.L.; Trinka, E.; Pressler, R.M.; Wennberg, R.; Visser, G.H.; Eisermann, M.; et al. Standardized computer-based organized reporting of EEG: SCORE—Secondversion. Clin. Neurophysiol. 2017, 128, 2334–2346. [Google Scholar] [CrossRef]
- Palmu, K.; Stevenson, N.; Wikström, S.; Hellström-Westas, L.; Vanhatalo, S.; Palva, J.M. Optimization of an NLEO-based algorithm for automated detection of spontaneous activity transients in early preterm EEG. Physiol. Measur. 2010, 31, N85–N93. [Google Scholar] [CrossRef]
- Jennekens, W.; Ruijs, L.S.; Lommen, C.M.L.; Niemarkt, H.J.; Pasman, J.W.; van Kranen-Mastenbroek, V.H.J.M.; Wijn, P.F.F.; van Pul, C.; Andriessen, P. Automatic burst detection for the EEG of the preterm infant. Physiol. Measur. 2011, 32, 1623–1637. [Google Scholar] [CrossRef]
- Koolen, N.; Jansen, K.; Vervisch, J.; Matic, V.; DeVos, M.; Naulaers, G.; Van Huffel, S. Line length as a robust method to detect high-activity events: Automated burst detection in premature EEG recordings. Clin. Neurophysiol. 2014, 125, 1985–1994. [Google Scholar] [CrossRef]
- Stevenson, N.J.; Oberdorfer, L.; Koolen, N.; O’Toole, J.M.; Werther, T.; Klebermass-Schrehof, K.; Vanhatalo, S. Functionalmaturation in preterm infants measured by serial recording of cortical activity. Sci. Rep. 2017, 7, 12969. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, N.J.; Oberdorfer, L.; Tataranno, M.L.; Breakspear, M.; Colditz, P.B.; de Vries, L.S.; Benders, M.J.; Klebermass-Schrehof, K.; Vanhatalo, S.; Roberts, J.A. Automated cot-side tracking of functional brain age in preterm infants. Ann. Clin. Transl. Neurol. 2020, 7, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, N.J.; Tataranno, M.L.; Kaminska, A.; Pavlidis, E.; Clancy, R.R.; Griesmaier, E.; Roberts, J.A.; Klebermass-Schrehof, K.; Vanhatalo, S. Reliability and accuracy of EEG interpretation for estimating age in preterm infants. Ann. Clin. Transl. Neurol. 2020, 7, 1564–1573. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, N.J.; Nordvik, T.; Espeland, C.N.; Giordano, V.; Moltu, S.J.; Larsson, P.G.; Klebermaß-Schrehof, K.; Stiris, T.; Vanhatalo, S. Inter-site generalizability of EEG based age prediction algorithms in the preterm infant. Physiol. Meas. 2023, 44, 07NT01. [Google Scholar] [CrossRef]
- O’Toole, J.M.; Boylan, G.B.; Lloyd, R.O.; Goulding, R.M.; Vanhatalo, S.; Stevenson, N.J. Detecting bursts in the EEG of very and extremely premature infants using a multi-feature approach. Med. Eng. Phys. 2017, 45, 42–50. [Google Scholar] [CrossRef]
- O’Toole, J.M.; Boylan, G.B.; Vanhatalo, S.; Stevenson, N.J. Estimating functional brain maturity in very and extremely preterm neonates using automated analysis of the electroencephalogram. Clin. Neurophysiol. 2016, 127, 2910–2918. [Google Scholar] [CrossRef]
- O’Toole, J.M.; Pavlidis, E.; Korotchikova, I.; Boylan, G.B.; Stevenson, N.J. Temporal evolution of quantitative EEG within 3 days of birth in early preterm infants. Sci. Rep. 2019, 9, 4859. [Google Scholar] [CrossRef]
- Nakagawa, S.; Schielzeth, H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods Ecol. Evol. 2013, 4, 133–142. [Google Scholar] [CrossRef]
- LeBihannic, A.; Beauvais, K.; Busnel, A.; deBarace, C.; Furby, A. Prognostic value of EEG in very premature newborns. Arch. Dis. Child. Fetal Neonatal Ed. 2012, 97, F106–F109. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | n = 29 |
|---|---|
| gestational age (weeks) | 28.4 (26.7, 30.1) |
| female | 21 (72.4%) |
| birth weight (g) | 980 (800, 1240) |
| Apgar score at 1 m | 8 (6, 8) |
| Apgar score at 5 m | 9 (8, 9) |
| pH | 7.21 (7.14, 7.28) |
| CRIB | 8 (7, 10) |
| cesarean delivery | 13 (44.8%) |
| Bayley scales III (26/29 newborns) | |
| cognitive | 95 (95, 104) |
| language | 103 (97, 111) |
| motor | 100 (97, 106) |
| Correlation | Bias (Days) | SDE (Days) | <1 Week (%) | <2 Weeks (%) | |
|---|---|---|---|---|---|
| Mean GA in cohort | 0.0 (−3.24, 3.37) | 15.7 (13.8, 17.4) | 31.0 (21.8, 41.4) | 55.2 (44.8, 65.5) | |
| Expert 1 | 0.597 (0.416, 0.737) | 3.57 (0.83, 6.44) | 13.2 (10.9, 15.3) | 40.2 (29.9, 50.6) | 72.4 (62.1, 81.6) |
| Expert 2 | 0.659 (0.530, 0.757) | 7.03 (4.43, 9.61) | 12.4 (10.6, 14.0) | 46.0 (35.6, 56.3) | 72.4 (62.1, 81.6) |
| Algorithm | 0.833 (0.752, 0.890) | −0.79 (−2.75, 0.95) | 8.7 (7.3, 10.0) | 56.3 (44.8, 66.7) | 88.5 (81.6, 94.3) |
| Expert 1 (long recording) | 0.816 (0.671, 0.903) | 0.67 (−2.64, 3.91) | 9.2 (6.8, 11.3) | 51.7 (34.5, 69.0) | 86.2 (72.4, 96.6) |
| Algorithm | 0.896 | −0.79 | 7.6 | 69.0 | 93.1 |
| (average epochs) | (0.794, 0.957) | (−3.80, 1.88) | (5.4, 9.4) | (51.7, 86.2) | (82.8, 100.0) |
| Correlation | Bias (Days) | SDE (Days) | <1 Week (%) | <2 Weeks (%) | |
|---|---|---|---|---|---|
| Expert 1 | 0.704 | 3.57 | 11.3 | 44.8 | 75.9 |
| (0.438, 0.843) | (−0.35, 7.33) | (8.4, 13.5) | (27.6, 65.5) | (58.6, 89.7) | |
| Expert 2 | 0.762 | 7.03 | 10.3 | 55.2 | 82.8 |
| (0.574, 0.902) | (3.42, 10.60) | (6.9, 12.8) | (37.9, 72.4) | (69.0, 96.6) | |
| Algorithm | 0.896 | −0.79 | 7.6 | 69.0 | 93.1 |
| (0.799, 0.958) | (−3.56, 2.00) | (5.4, 9.4) | (51.7, 82.8) | (82.8, 100.0) |
| Correlation | Bias | SDE | |
|---|---|---|---|
| p a | p b | p c | |
| Expert 1 vs. Expert 2 | 0.416 (0.416) | 0.009 (0.009) | 0.584 (0.584) |
| Expert 1 vs. EMA | 0.006 (0.002) | 0.006 (0.003) | 0.175 (0.059) |
| Expert 2 vs. EMA | 0.049 (0.024) | <0.001 (<0.001) | 0.200 (0.399) |
| Expert 1 | Expert 2 | |||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| intercept (days) | 106.4 (77.7, 136.2) | <0.001 | 81.4 (45.1, 117.5) | <0.001 |
| PNA (days) | 6.57 (3.54 to 9.15) | <0.001 | 3.74 (0.47, 6.90) | 0.021 |
| GA (days) | 0.407 (0.251, 0.554) | <0.001 | 0.533 (0.349, 0.724) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlidis, E.; O’Toole, J.M.; Pisani, F.; Boylan, G.B.; Stevenson, N.J. EEG Maturational Age Estimation: A Comparison of Visual and Automated Interpretation of the EEG in Preterm Infants. J. Clin. Med. 2025, 14, 3528. https://doi.org/10.3390/jcm14103528
Pavlidis E, O’Toole JM, Pisani F, Boylan GB, Stevenson NJ. EEG Maturational Age Estimation: A Comparison of Visual and Automated Interpretation of the EEG in Preterm Infants. Journal of Clinical Medicine. 2025; 14(10):3528. https://doi.org/10.3390/jcm14103528
Chicago/Turabian StylePavlidis, Elena, John M. O’Toole, Francesco Pisani, Geraldine B. Boylan, and Nathan J. Stevenson. 2025. "EEG Maturational Age Estimation: A Comparison of Visual and Automated Interpretation of the EEG in Preterm Infants" Journal of Clinical Medicine 14, no. 10: 3528. https://doi.org/10.3390/jcm14103528
APA StylePavlidis, E., O’Toole, J. M., Pisani, F., Boylan, G. B., & Stevenson, N. J. (2025). EEG Maturational Age Estimation: A Comparison of Visual and Automated Interpretation of the EEG in Preterm Infants. Journal of Clinical Medicine, 14(10), 3528. https://doi.org/10.3390/jcm14103528