
Monocyte Chemoattractant Protein-1 as a Biomarker in Acute Ischemic Stroke: A Prospective Pilot Study

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
2.3. Ethical Review Board
3. Results
3.1. Baseline Characteristics
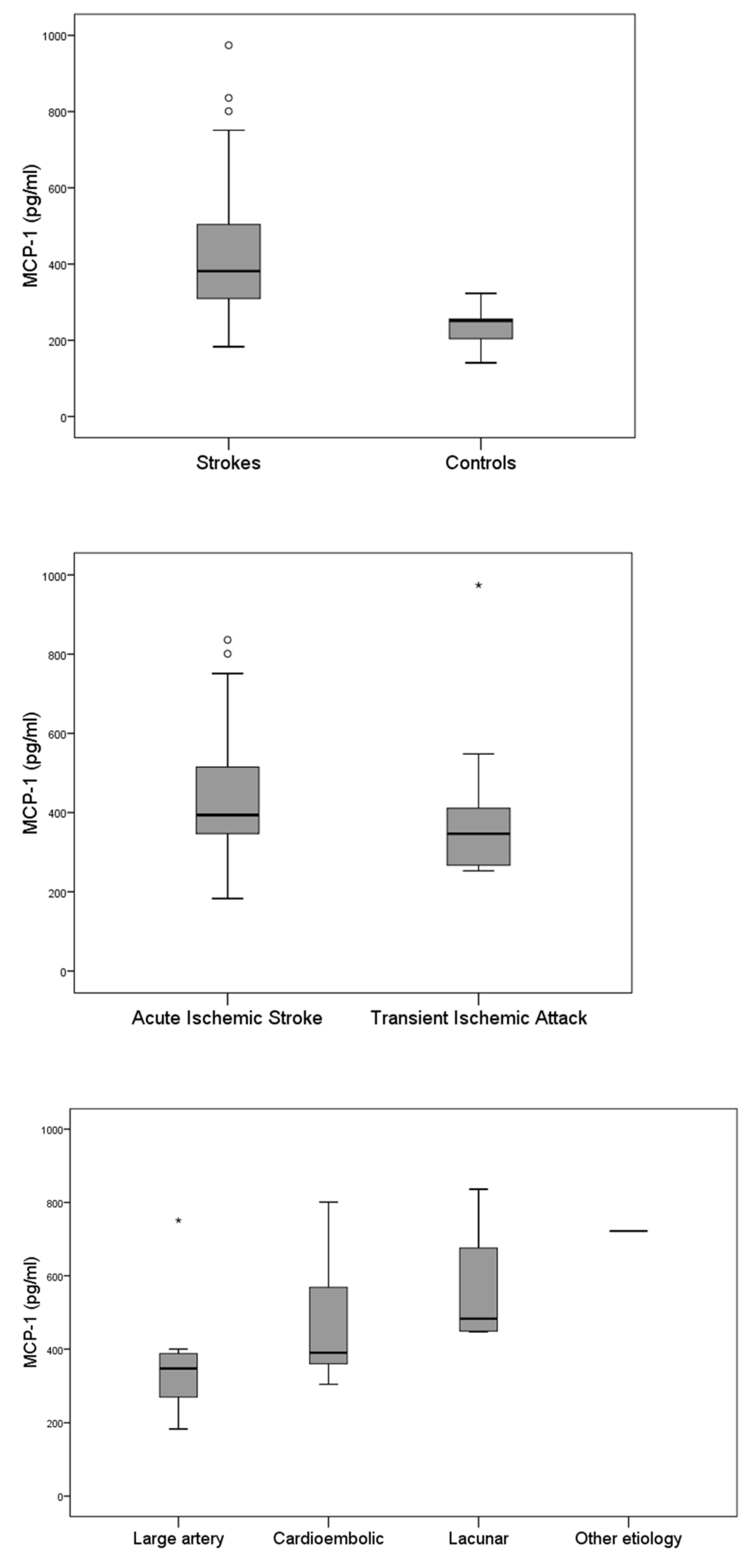
3.2. MCP-1 Levels at Admission and Correlation with Baseline Characteristics
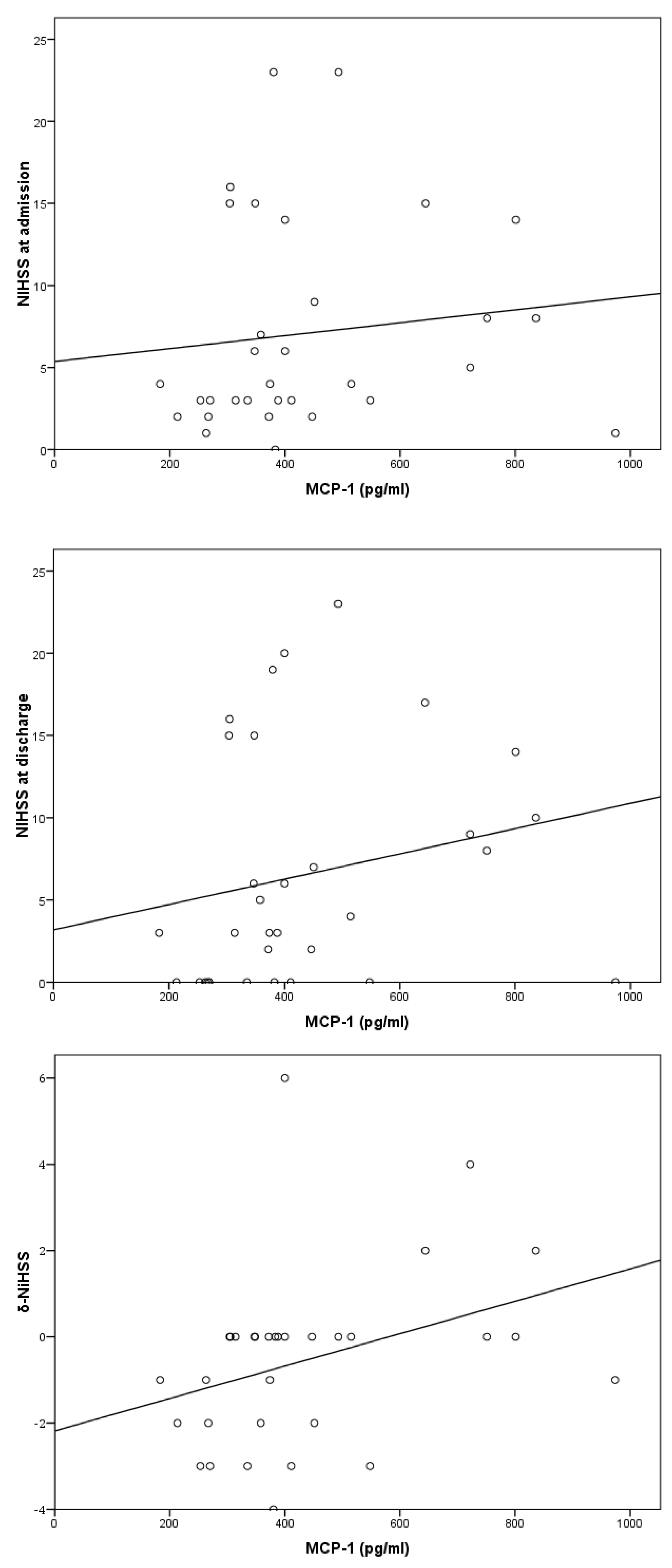
3.3. Correlation of MCP-1 Levels and Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| δ-NIHSS | NIHSS change from admission to discharge |
| Adm | Admission |
| AF | Atrial fibrillation |
| AIS | Acute ischemic stroke |
| CCL2 | Chemokine (C-C motif) ligand 2 |
| CCR2 | C-C chemokine receptor type 2 |
| CN | Coronary disease |
| DaysHosp | Days of hospital stay |
| Diff | Difference |
| Dis | Discharge |
| DM | Diabetes mellitus |
| HbA1c | Hemoglobin A1c |
| HDL-cholesterol | High-density lipoprotein–cholesterol |
| LDL-cholesterol | Low-density lipoprotein–cholesterol |
| MCP-1 | Monocyte chemotactic protein-1 |
| mRS | Modified Rankin score |
| NIHSS | National Institutes of Health Stroke Scale |
| PVD | Peripheral vascular disease |
| Pre | Prior to admission |
| SPSS | Statistical package for the social sciences |
| TIA | Transient ischemic attack |
| TOAST | Trial of Org 10,172 in acute stroke treatment |
References
- GBD 2021 Causes of Death Collaborators. Global Burden of 288 Causes of Death and Life Expectancy Decomposition in 204 Countries and Territories and 811 Subnational Locations, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2100–2132. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Diseases and Injuries Collaborators. Global Incidence, Prevalence, Years Lived with Disability (YLDs), Disability-Adjusted Life-Years (DALYs), and Healthy Life Expectancy (HALE) for 371 Diseases and Injuries in 204 Countries and Territories and 811 Subnational Locations, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2133–2161. [Google Scholar] [CrossRef]
- Anderer, S. Stroke Deaths and Burden Increased Around the World From 1990 to 2021. JAMA 2024, 332, 1509. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Leducq Transatlantic Network on Atherothrombosis Inflammation in Atherosclerosis: From Pathophysiology to Practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef]
- Ahola-Olli, A.V.; Würtz, P.; Havulinna, A.S.; Aalto, K.; Pitkänen, N.; Lehtimäki, T.; Kähönen, M.; Lyytikäinen, L.-P.; Raitoharju, E.; Seppälä, I.; et al. Genome-Wide Association Study Identifies 27 Loci Influencing Concentrations of Circulating Cytokines and Growth Factors. Am. J. Hum. Genet. 2017, 100, 40–50. [Google Scholar] [CrossRef]
- Malik, R.; Chauhan, G.; Traylor, M.; Sargurupremraj, M.; Okada, Y.; Mishra, A.; Rutten-Jacobs, L.; Giese, A.-K.; van der Laan, S.W.; Gretarsdottir, S.; et al. Multiancestry Genome-Wide Association Study of 520,000 Subjects Identifies 32 Loci Associated with Stroke and Stroke Subtypes. Nat. Genet. 2018, 50, 524–537. [Google Scholar] [CrossRef] [PubMed]
- Georgakis, M.K.; Gill, D.; Rannikmäe, K.; Traylor, M.; Anderson, C.D.; Lee, J.-M.; Kamatani, Y.; Hopewell, J.C.; Worrall, B.B.; Bernhagen, J.; et al. Genetically Determined Levels of Circulating Cytokines and Risk of Stroke. Circulation 2019, 139, 256–268. [Google Scholar] [CrossRef]
- Krishnaswamy, G.; Kelley, J.; Yerra, L.; Smith, J.K.; Chi, D.S. Human Endothelium as a Source of Multifunctional Cytokines: Molecular Regulation and Possible Role in Human Disease. J. Interferon Cytokine Res. 1999, 19, 91–104. [Google Scholar] [CrossRef]
- Lin, J.; Kakkar, V.; Lu, X. Impact of MCP-1 in Atherosclerosis. Curr. Pharm. Des. 2014, 20, 4580–4588. [Google Scholar] [CrossRef]
- Deo, R.; Khera, A.; McGuire, D.K.; Murphy, S.A.; de Meo Neto, J.P.; Morrow, D.A.; de Lemos, J.A. Association among Plasma Levels of Monocyte Chemoattractant Protein-1, Traditional Cardiovascular Risk Factors, and Subclinical Atherosclerosis. J. Am. Coll. Cardiol. 2004, 44, 1812–1818. [Google Scholar] [CrossRef]
- Namiki, M.; Kawashima, S.; Yamashita, T.; Ozaki, M.; Hirase, T.; Ishida, T.; Inoue, N.; Hirata, K.; Matsukawa, A.; Morishita, R.; et al. Local Overexpression of Monocyte Chemoattractant Protein-1 at Vessel Wall Induces Infiltration of Macrophages and Formation of Atherosclerotic Lesion: Synergism with Hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Georgakis, M.K.; Malik, R.; Björkbacka, H.; Pana, T.A.; Demissie, S.; Ayers, C.; Elhadad, M.A.; Fornage, M.; Beiser, A.S.; Benjamin, E.J.; et al. Circulating Monocyte Chemoattractant Protein-1 and Risk of Stroke: Meta-Analysis of Population-Based Studies Involving 17 180 Individuals. Circ. Res. 2019, 125, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- FineTest® Human MCP-1 (Monocyte Chemotactic Protein 1) ELISA Kit. Available online: https://www.fn-test.com/product/eh0222/ (accessed on 1 September 2022).
- Brott, T.; Adams, H.P.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of Acute Cerebral Infarction: A Clinical Examination Scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P.; Davis, P.H.; Leira, E.C.; Chang, K.C.; Bendixen, B.H.; Clarke, W.R.; Woolson, R.F.; Hansen, M.D. Baseline NIH Stroke Scale Score Strongly Predicts Outcome after Stroke: A Report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology 1999, 53, 126–131. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver Agreement for the Assessment of Handicap in Stroke Patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Yamagami, S.; Tamura, M.; Hayashi, M.; Endo, N.; Tanabe, H.; Katsuura, Y.; Komoriya, K. Differential Production of MCP-1 and Cytokine-Induced Neutrophil Chemoattractant in the Ischemic Brain after Transient Focal Ischemia in Rats. J. Leukoc. Biol. 1999, 65, 744–749. [Google Scholar] [CrossRef]
- Meisel, C.; Schwab, J.M.; Prass, K.; Meisel, A.; Dirnagl, U. Central Nervous System Injury-Induced Immune Deficiency Syndrome. Nat. Rev. Neurosci. 2005, 6, 775–786. [Google Scholar] [CrossRef]
- Chen, Y.; Hallenbeck, J.M.; Ruetzler, C.; Bol, D.; Thomas, K.; Berman, N.E.J.; Vogel, S.N. Overexpression of Monocyte Chemoattractant Protein 1 in the Brain Exacerbates Ischemic Brain Injury and Is Associated with Recruitment of Inflammatory Cells. J. Cereb. Blood Flow Metab. 2003, 23, 748–755. [Google Scholar] [CrossRef]
- Bonifačić, D.; Toplak, A.; Benjak, I.; Tokmadžić, V.S.; Lekić, A.; Kučić, N. Monocytes and Monocyte Chemoattractant Protein 1 (MCP-1) as Early Predictors of Disease Outcome in Patients with Cerebral Ischemic Stroke. Wien. Klin. Wochenschr. 2016, 128, 20–27. [Google Scholar] [CrossRef]
- Rhodes, J. Peripheral Immune Cells in the Pathology of Traumatic Brain Injury? Curr. Opin. Crit. Care 2011, 17, 122–130. [Google Scholar] [CrossRef]
- Pius, P.; Li, C.; Theertham, A.; Khanna, S.; Bhat, A. Differentiation of Cardioembolic and Non-Cardioembolic Stroke Subtypes Based on Clinical and Echocardiographic Parameters: A Systematic Review and Meta-Analysis. Heart Lung Circ. 2024, 33, S182. [Google Scholar] [CrossRef]
- Hart, R.G.; Pearce, L.A.; Miller, V.T.; Anderson, D.C.; Rothrock, J.F.; Albers, G.W.; Nasco, E. Cardioembolic vs. Noncardioembolic Strokes in Atrial Fibrillation: Frequency and Effect of Antithrombotic Agents in the Stroke Prevention in Atrial Fibrillation Studies. Cerebrovasc. Dis. 2000, 10, 39–43. [Google Scholar] [CrossRef]
- Arboix, A.; Massons, J.; García-Eroles, L.; Targa, C.; Comes, E.; Parra, O. Clinical Predictors of Lacunar Syndrome Not Due to Lacunar Infarction. BMC Neurol. 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Worthmann, H.; Tryc, A.B.; Goldbecker, A.; Ma, Y.T.; Tountopoulou, A.; Hahn, A.; Dengler, R.; Lichtinghagen, R.; Weissenborn, K. The Temporal Profile of Inflammatory Markers and Mediators in Blood after Acute Ischemic Stroke Differs Depending on Stroke Outcome. Cerebrovasc. Dis. 2010, 30, 85–92. [Google Scholar] [CrossRef]
- Michel, P.; Odier, C.; Rutgers, M.; Reichhart, M.; Maeder, P.; Meuli, R.; Wintermark, M.; Maghraoui, A.; Faouzi, M.; Croquelois, A.; et al. The Acute STroke Registry and Analysis of Lausanne (ASTRAL): Design and Baseline Analysis of an Ischemic Stroke Registry Including Acute Multimodal Imaging. Stroke 2010, 41, 2491–2498. [Google Scholar] [CrossRef] [PubMed]
- Worthmann, H.; Dengler, R.; Schumacher, H.; Schwartz, A.; Eisert, W.G.; Lichtinghagen, R.; Weissenborn, K. Monocyte Chemotactic Protein-1 as a Potential Biomarker for Early Anti-Thrombotic Therapy after Ischemic Stroke. Int. J. Mol. Sci. 2012, 13, 8670–8678. [Google Scholar] [CrossRef]
- Capoccia, B.J.; Gregory, A.D.; Link, D.C. Recruitment of the Inflammatory Subset of Monocytes to Sites of Ischemia Induces Angiogenesis in a Monocyte Chemoattractant Protein-1-Dependent Fashion. J. Leukoc. Biol. 2008, 84, 760–768. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Kirchgessner, A.; Hofer, M. Inflammatory Mechanisms in Ischemic Stroke: Therapeutic Approaches. J. Transl. Med. 2009, 7, 97. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Acute Ischemic Stroke | Transient Ischemic Attack |
|---|---|---|
| n = 22 | n = 10 | |
| Age, years | 79 (12) | 84 (14) |
| Female sex | 10 (45.5) | 3 (30) |
| Arterial hypertension | 17 (77.3) | 8 (80) |
| Diabetes mellitus | 7 (31.8) | 2 (20) |
| Dyslipidemia | 10 (45.5) | 0 (0) |
| Atrial Fibrillation | 9 (40.9) | 5 (50) |
| Coronary artery disease | 8 (36.4) | 4 (40) |
| Peripheral artery disease | 4 (18.2) | 0 (0) |
| Previous stroke | 7 (31.8) | 6 (60) |
| Current smoking | 7 (31.8) | 3 (30) |
| MCP-1, pg/dL | 394 (210) | 346 (179) |
| LDL-cholesterol, mg/dL | 85 (59) | 97 (62) |
| HDL-cholesterol, mg/dL | 39 (24) | 35 (15) |
| Glucose, mg/dL | 116 (65) | 113 (51) |
| HBA1c, % | 6.1 (1.1) | 5.9 (0.7) |
| Systolic blood pressure, mmHg | 160 (49) | 145 (31) |
| Diastolic blood pressure, mmHg | 80 (12) | 73 (18) |
| NIHSS at admission | 7 (11) | 3 (2) |
| mRS before admission | 1 (2) | 2 (3) |
| mRS at admission | 4 (2) | 4 (3) |
| Variables | Regression Coefficient | p Value |
|---|---|---|
| Age | 2.15 | 0.574 |
| Sex | 30.73 | 0.667 |
| Arterial hypertension | 103.76 | 0.216 |
| Diabetes mellitus | −110.31 | 0.150 |
| Dyslipidemia | 32.32 | 0.151 |
| Atrial fibrilation | −14.08 | 0.152 |
| Peripheral arterial disease | 47.36 | 0.153 |
| Coronary artery disease | −112.90 | 0.154 |
| Stroke history | −10.34 | 0.155 |
| Current smoking | −81.27 | 0.156 |
| Alcohol | 66.14 | 0.157 |
| LDL-cholesterol | 1.21 | 0.158 |
| HDL-cholesterol | 1.10 | 0.159 |
| HbA1c | −7.72 | 0.160 |
| Systolic blood pressure | 0.46 | 0.161 |
| Diastolic blood pressure | 0.73 | 0.162 |
| Glucose | 1.29 | 0.164 |
| Outcomes | Regression Coefficient | p Value |
|---|---|---|
| Days of hospital stay | 0.280 | 0.725 |
| NIHSS at admission | 0.394 | 0.513 |
| NIHSS at discharge | 0.769 | 0.248 |
| δ-NIHSS | 0.376 | 0.048 |
| mRS before admission | −0.084 | 0.455 |
| mRS at admission | 0.067 | 0.623 |
| mRS at discharge | 0.214 | 0.267 |
| mRS at 6 months | 0.507 | 0.030 |
| In-hospital death | 0.173 | 0.393 |
| Death at 12 months | 0.378 | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ztriva, E.; Moschonas, I.C.; Tselepis, A.; Lambrou, D.; Ntaios, G.; Savopoulos, C.; Kaiafa, G. Monocyte Chemoattractant Protein-1 as a Biomarker in Acute Ischemic Stroke: A Prospective Pilot Study. J. Clin. Med. 2025, 14, 3295. https://doi.org/10.3390/jcm14103295
Ztriva E, Moschonas IC, Tselepis A, Lambrou D, Ntaios G, Savopoulos C, Kaiafa G. Monocyte Chemoattractant Protein-1 as a Biomarker in Acute Ischemic Stroke: A Prospective Pilot Study. Journal of Clinical Medicine. 2025; 14(10):3295. https://doi.org/10.3390/jcm14103295
Chicago/Turabian StyleZtriva, Eleftheria, Iraklis C. Moschonas, Alexandros Tselepis, Dimitrios Lambrou, Georgios Ntaios, Christos Savopoulos, and Georgia Kaiafa. 2025. "Monocyte Chemoattractant Protein-1 as a Biomarker in Acute Ischemic Stroke: A Prospective Pilot Study" Journal of Clinical Medicine 14, no. 10: 3295. https://doi.org/10.3390/jcm14103295
APA StyleZtriva, E., Moschonas, I. C., Tselepis, A., Lambrou, D., Ntaios, G., Savopoulos, C., & Kaiafa, G. (2025). Monocyte Chemoattractant Protein-1 as a Biomarker in Acute Ischemic Stroke: A Prospective Pilot Study. Journal of Clinical Medicine, 14(10), 3295. https://doi.org/10.3390/jcm14103295