

Calculation of Oxygen Uptake during Ambulatory Cardiac Rehabilitation

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Design
2.3. Cardiac Rehabilitation and Cardiopulmonary Exercise Testing
2.4. Calculations for Estimation of Oxygen Uptake
2.5. Statistical Analysis
3. Results
3.1. Subjects
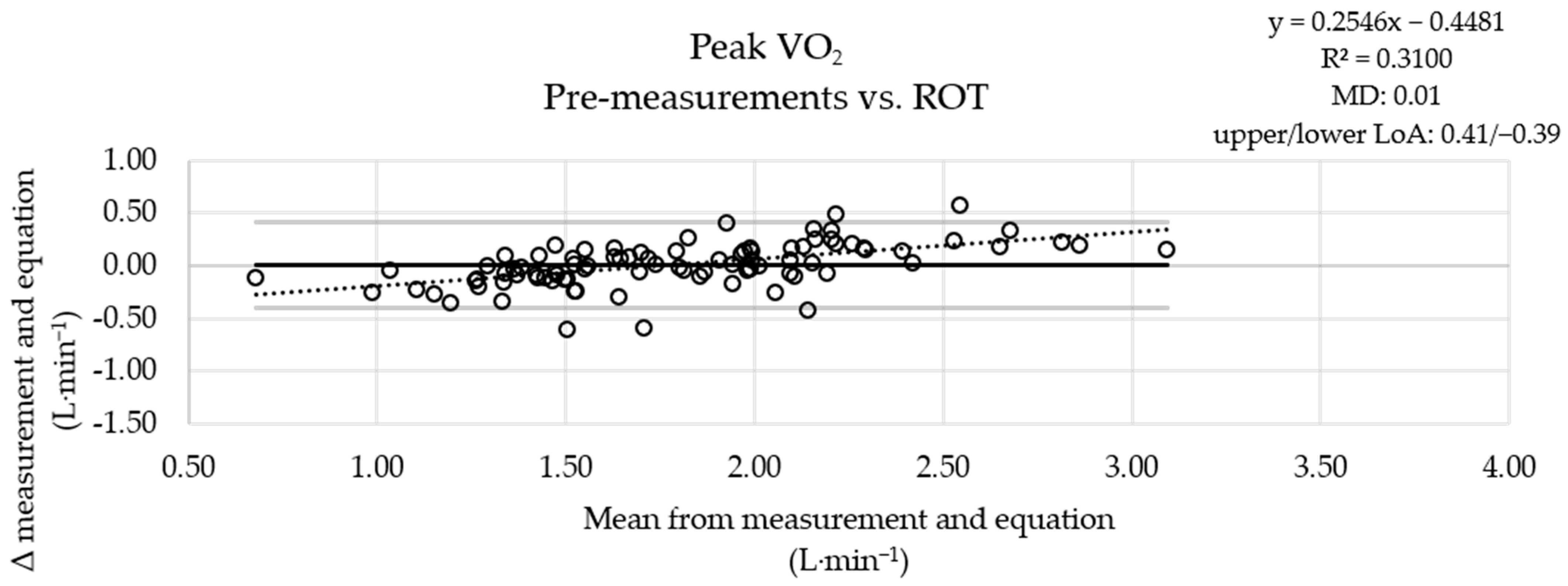
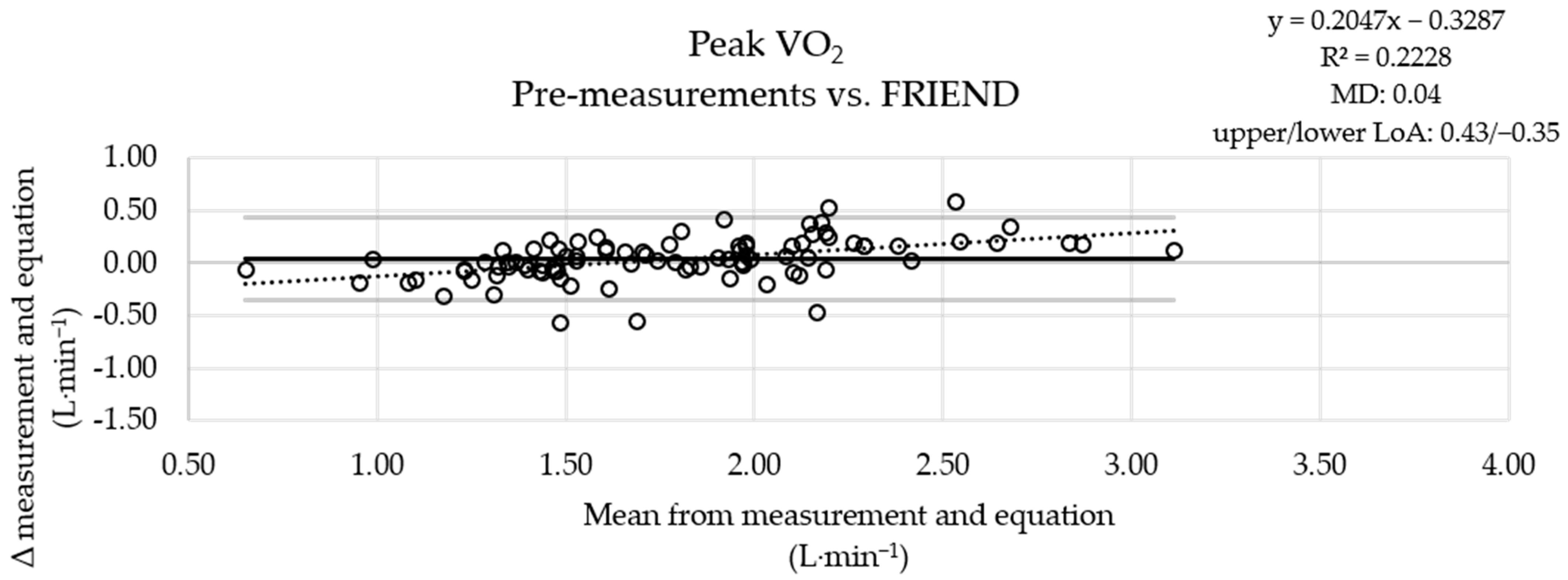
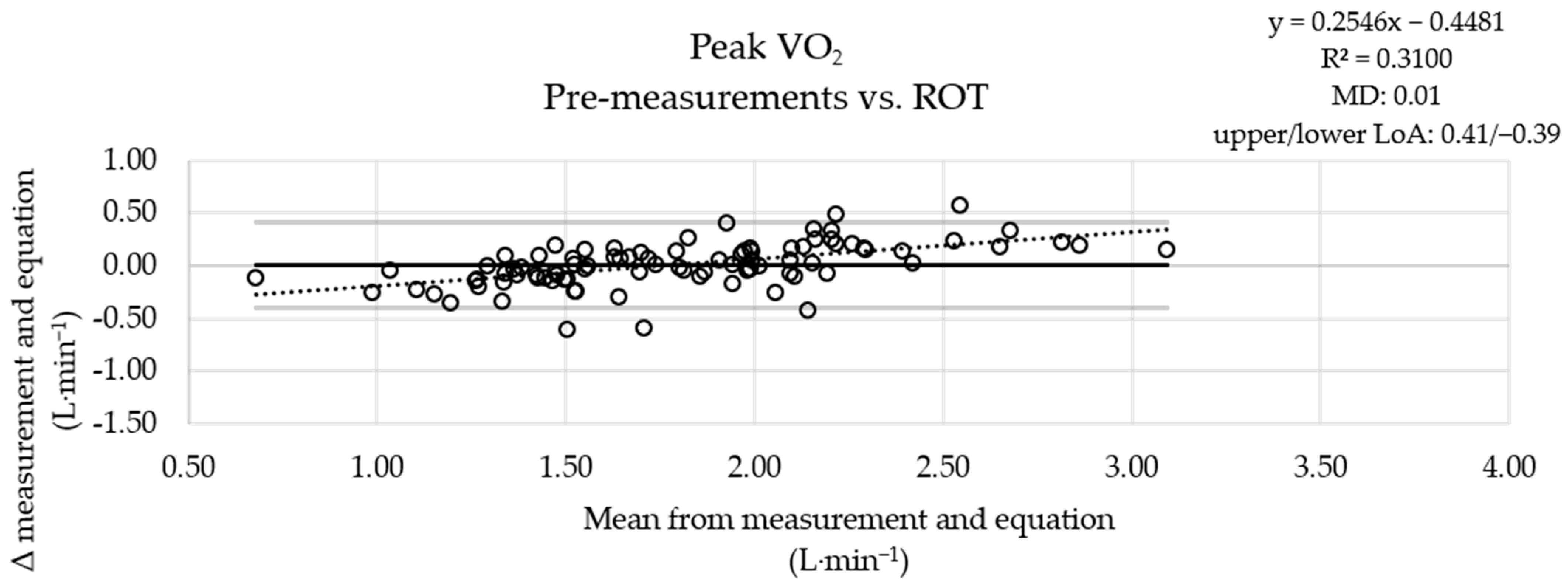
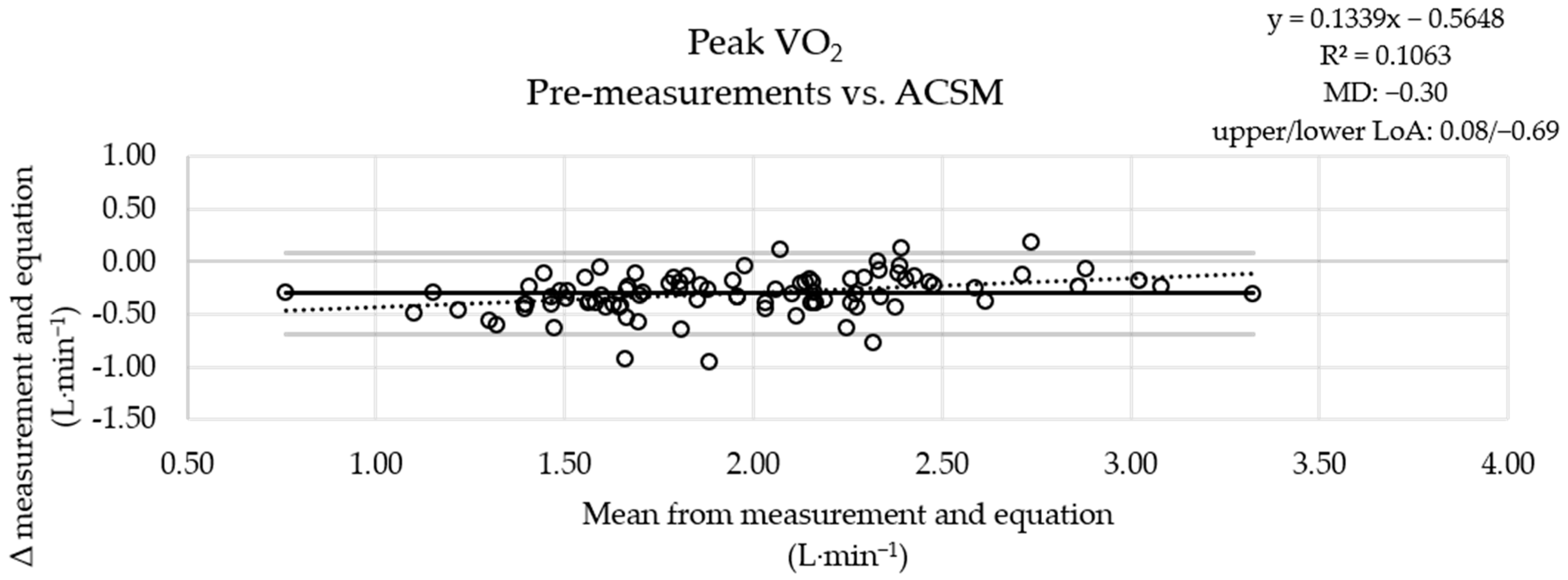
3.2. Evaluations of Peak Work Rates
3.3. Evaluations of Fixed Work Rates
4. Discussion
4.1. Highlights
4.2. Classifications
4.3. Applications
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laveneziana, P.; Di Paolo, M.; Palange, P. The clinical value of cardiopulmonary exercise testing in the modern era. Eur. Respir. Rev. 2021, 30, 200187. [Google Scholar] [CrossRef] [PubMed]
- Nelson, N.; Asplund, C.A. Exercise Testing: Who, When, and Why? PM R 2016, 8, S16–S23. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A. Cardiopulmonary Exercise Testing: Basics of Methodology and Measurements. Ann. Am. Thorac. Soc. 2017, 14, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason-Wehrens, B.; Schmidt, T.; Schwaab, B. Cardiopulmonary exercise testing for exercise prescription in cardiac rehabilitation. Herzschrittmacherther. Elektrophysiol. 2023, 34, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A.; Hamm, L.F.; Jones, A.M.; McBride, P.E.; Moholdt, T.; Stone, J.A.; Urhausen, A.; Williams, M.A.; European Association for Cardiovascular Prevention and Rehabilitation; American Association of Cardiovascular and Pulmonary Rehabilitation; et al. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: A joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac Rehabilitation. Eur. J. Prev. Cardiol. 2013, 20, 442–467. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Guazzi, M.; Bandera, F.; Ozemek, C.; Systrom, D.; Arena, R. Cardiopulmonary Exercise Testing: What Is its Value? J. Am. Coll. Cardiol. 2017, 70, 1618–1636. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Tan, L.; Carey-Jones, S.; Riddell, N.; Davies, R.; Brownsdon, A.; Kelson, M.; Williams-Thomas, R.; Busse, M.; Davies, M.M.; et al. Can wearable technology be used to approximate cardiopulmonary exercise testing metrics? Perioper. Med. 2021, 10, 9. [Google Scholar] [CrossRef]
- Thompson, W.R.; Gordon, N.F.; Pescatello, L.S. ACSM s Guidelines for Exercise Testing and Prescription, 8th ed.; LippincotWilliams & Wilkins: Philadelphia, PA, USA, 2009. [Google Scholar]
- Kokkinos, P.; Kaminsky, L.A.; Arena, R.; Zhang, J.; Myers, J. A new generalized cycle ergometry equation for predicting maximal oxygen uptake: The Fitness Registry and the Importance of Exercise National Database (FRIEND). Eur. J. Prev. Cardiol. 2018, 25, 1077–1082. [Google Scholar] [CrossRef]
- Kokkinos, P.; Kaminsky, L.A.; Arena, R.; Zhang, J.; Franklin, B.; Kraus, W.; Triantafyllidi, H.; Benas, D.; Whellan, D.J.; Myers, J. New Equations for Predicting Maximum Oxygen Uptake in Patients With Heart Failure. Am. J. Cardiol. 2020, 128, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Winkert, K.; Kirsten, J. Cardiopulmonary Exercise Testing—Methodological Aspects. Dtsch. Z. Sportmed. 2022, 73, 184–188. [Google Scholar] [CrossRef]
- Nichols, S.; Gleadall-Siddall, D.O.; Antony, R.; Clark, A.L.; Cleland, J.G.F.; Carroll, S.; Ingle, L. Estimated peak functional capacity: An accurate method for assessing change in peak oxygen consumption after cardiac rehabilitation? Clin. Physiol. Funct. Imaging 2018, 38, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Jurov, I.; Toplišek, J.; Cvijić, M. Prediction of Maximal Oxygen Consumption in Cycle Ergometry in Competitive Cyclists. Life 2023, 13, 160. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Kjeldsen, S.E.; Mundal, R.; Sandvik, L.; Erikssen, G.; Thaulow, E.; Erikssen, J. Supine and exercise systolic blood pressure predict cardiovascular death in middle-aged men. J. Hypertens. 2001, 19, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Röcker, K. Die sportmedizinische Laktatdiagnostik: Technische Rahmenbedingungen und Einsatzbereiche. Dtsch. Z. Sportmed. 2013, 64, 367–371. [Google Scholar] [CrossRef]
- Glaab, T.; Schmidt, O.; Fritsch, J. Guidance to the Interpretation of Cardiopulmonary Exercise Testing. Pneumologie 2020, 74, 88–102. [Google Scholar] [CrossRef]
- Caballero, B. Humans against Obesity: Who Will Win? Adv. Nutr. 2019, 10, S4–S9. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J.; Peterman, J.E.; Bonikowske, A.R.; Harber, M.P.; Medina Inojosa, J.R.; Lavie, C.J.; Squires, R.W. Updated Reference Standards for Cardiorespiratory Fitness Measured with Cardiopulmonary Exercise Testing: Data from the Fitness Registry and the Importance of Exercise National Database (FRIEND). Mayo Clin. Proc. 2022, 97, 285–293. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, M.; Weltman, A. Effects of pedal frequency on VO2 and work output at lactate threshold (LT), fixed blood lactate concentrations of 2 mM and 4 mM, and max in competitive cyclists. Int. J. Sports Med. 1985, 6, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.P.; Martin, P.E. Effect of cycling experience, aerobic power, and power output on preferred and most economical cycling cadences. Med. Sci. Sports Exerc. 1997, 29, 1225–1232. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Core data | |
| Age (years) | 53.7 ± 5.9 |
| Height (cm) | 178.2 ± 7.1 |
| Body mass (kg) | 87.6 ± 12.9 |
| BMI (kg∙m−2) | 27.6 ± 3.9 |
| Prevalences of diseases | |
| I10 Essential (primary) hypertension | 50 |
| I11 Hypertensive heart disease | 28 |
| I21 Acute myocardial infarction | 56 |
| I24 Other acute ischemic heart diseases | 13 |
| I25 Chronic ischemic heart disease | 81 |
| I34 Nonrheumatic mitral valve disorders | 17 |
| I35 Nonrheumatic aortic valve disorders | 6 |
| I36 Nonrheumatic tricuspid (valve) disorders | 3 |
| Z95 Presence of cardiac and vascular implants and grafts | 83 |
| Medication | |
| Platelet aggregation inhibitors | 92 |
| Statins | 92 |
| Beta blockers | 61 |
| Antihypertensives | 28 |
| ACE inhibitors | 65 |
| Other medications | 62 |
| Performance Capability | Peak WR (watt) | Peak WR (watt∙kg−1) | Peak VO2 (L∙min−1) | Peak VO2 (mL∙min−1∙kg−1) | |
|---|---|---|---|---|---|
| Entire patient collective (n = 91) | pre post | 135.8 ± 37.7 152.7 ± 41.7 * | 1.56 ± 0.42 1.76 ± 0.47 * | 1.81 ± 0.52 1.97 ± 0.56 * | 20.7 ± 5.3 22.6 ± 6.1 * |
| Patients who achieved ≥ 100 watts in both CPET sessions (n = 83) | pre post | 141.4 ± 34.0 158.6 ± 38.2 * | 1.62 ± 0.39 1.82 ± 0.44 * | 1.88 ± 0.47 2.06 ± 0.51 * | 21.4 ± 4.9 23.5 ± 5.6 * |
| Peak VO2 Values | Measured vs. ROT | Measured vs. ACSM | Measured vs. FRIEND | |
|---|---|---|---|---|
| pre | ICC | 0.948 (0.921–0.966) | 0.870 (−0.075–0.963) | 0.952 (0.927–0.968) |
| SEM (L∙min−1) | 0.10 | 0.17 | 0.10 | |
| post | ICC | 0.959 (0.938–0.973) | 0.884 (−0.093–0.969) | 0.965 (0.947–0.977) |
| SEM (L∙min−1) | 0.10 | 0.18 | 0.10 |
| VO2 Values | Measured vs. ROT | Measured vs. ACSM | Measured vs. FRIEND | ||
|---|---|---|---|---|---|
| pre | 100 watts | ICC | 0.329 (−0.029–0.564) | 0.138 (−0.127–0.391) | 0.256 (−0.144–0.517) |
| SEM (L∙min−1) | 0.10 | 0.13 | 0.09 | ||
| 55% of peak WR | ICC | 0.924 (0.885–0.950) | 0.756 (−0.182–0.927) | 0.915 (0.849–0.949) | |
| SEM (L∙min−1) | 0.07 | 0.14 | 0.08 | ||
| post | 100 watts | ICC | 0.379 (0.037–0.600) | 0.172 (−0.144–0.450) | 0.278 (−0.084–0.523) |
| SEM (L∙min−1) | 0.09 | 0.12 | 0.09 | ||
| 55% of peak WR | ICC | 0.903 (0.853–0.936) | 0.788 (−0.123–0.931) | 0.898 (0.825–0.937) | |
| SEM (L∙min−1) | 0.10 | 0.15 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stephan, H.; Klophaus, N.; Wehmeier, U.F.; Tomschi, F.; Hilberg, T. Calculation of Oxygen Uptake during Ambulatory Cardiac Rehabilitation. J. Clin. Med. 2024, 13, 2235. https://doi.org/10.3390/jcm13082235
Stephan H, Klophaus N, Wehmeier UF, Tomschi F, Hilberg T. Calculation of Oxygen Uptake during Ambulatory Cardiac Rehabilitation. Journal of Clinical Medicine. 2024; 13(8):2235. https://doi.org/10.3390/jcm13082235
Chicago/Turabian StyleStephan, Holger, Nils Klophaus, Udo F. Wehmeier, Fabian Tomschi, and Thomas Hilberg. 2024. "Calculation of Oxygen Uptake during Ambulatory Cardiac Rehabilitation" Journal of Clinical Medicine 13, no. 8: 2235. https://doi.org/10.3390/jcm13082235
APA StyleStephan, H., Klophaus, N., Wehmeier, U. F., Tomschi, F., & Hilberg, T. (2024). Calculation of Oxygen Uptake during Ambulatory Cardiac Rehabilitation. Journal of Clinical Medicine, 13(8), 2235. https://doi.org/10.3390/jcm13082235