
The Role of Postoperative Radiotherapy in the Management of Dermatofibrosarcoma Protuberans: A Multidisciplinary Systematic Review

 , , , ,
, , , ,  ,
,  , ,
, ,
Abstract
1. Introduction
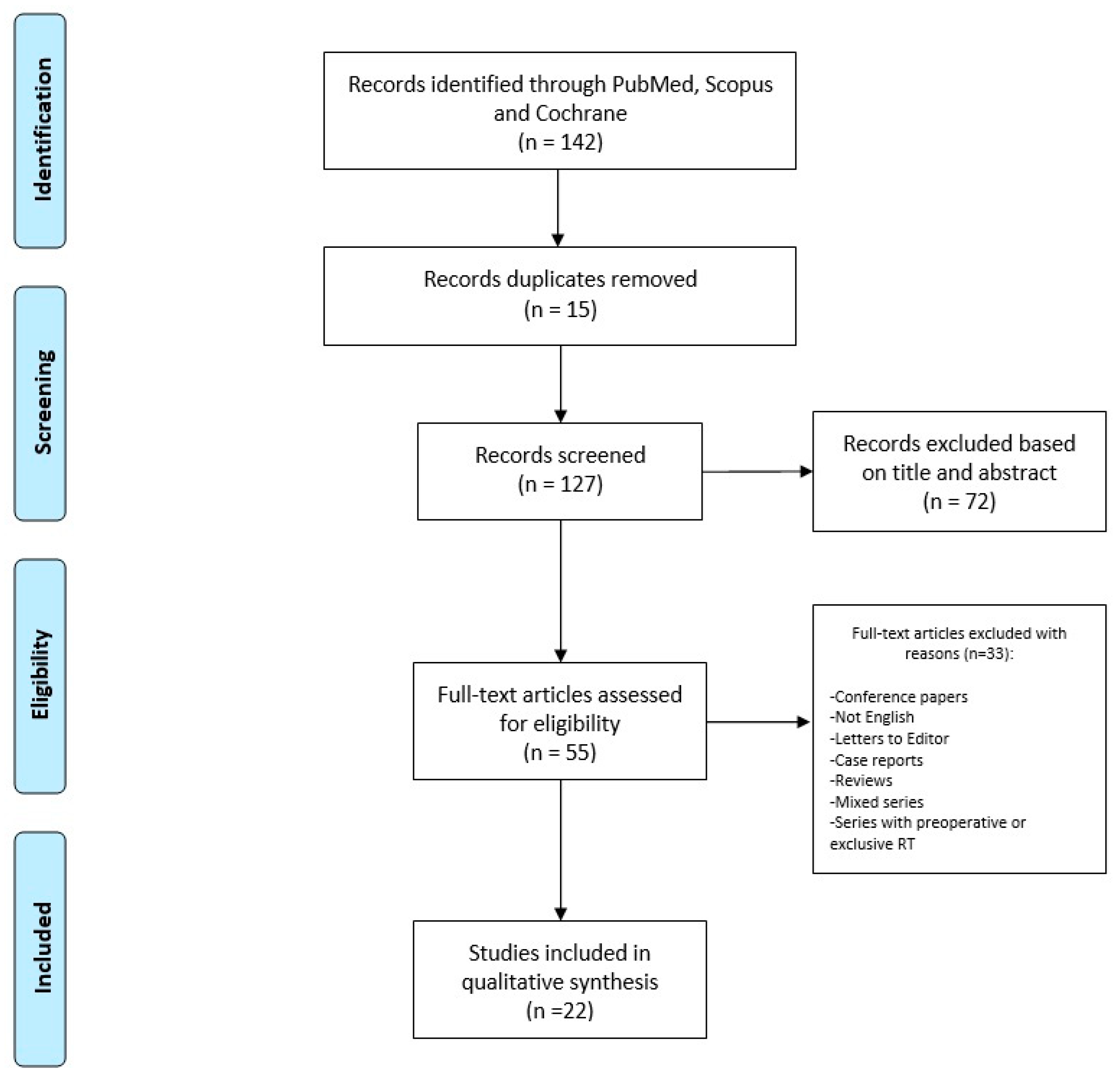
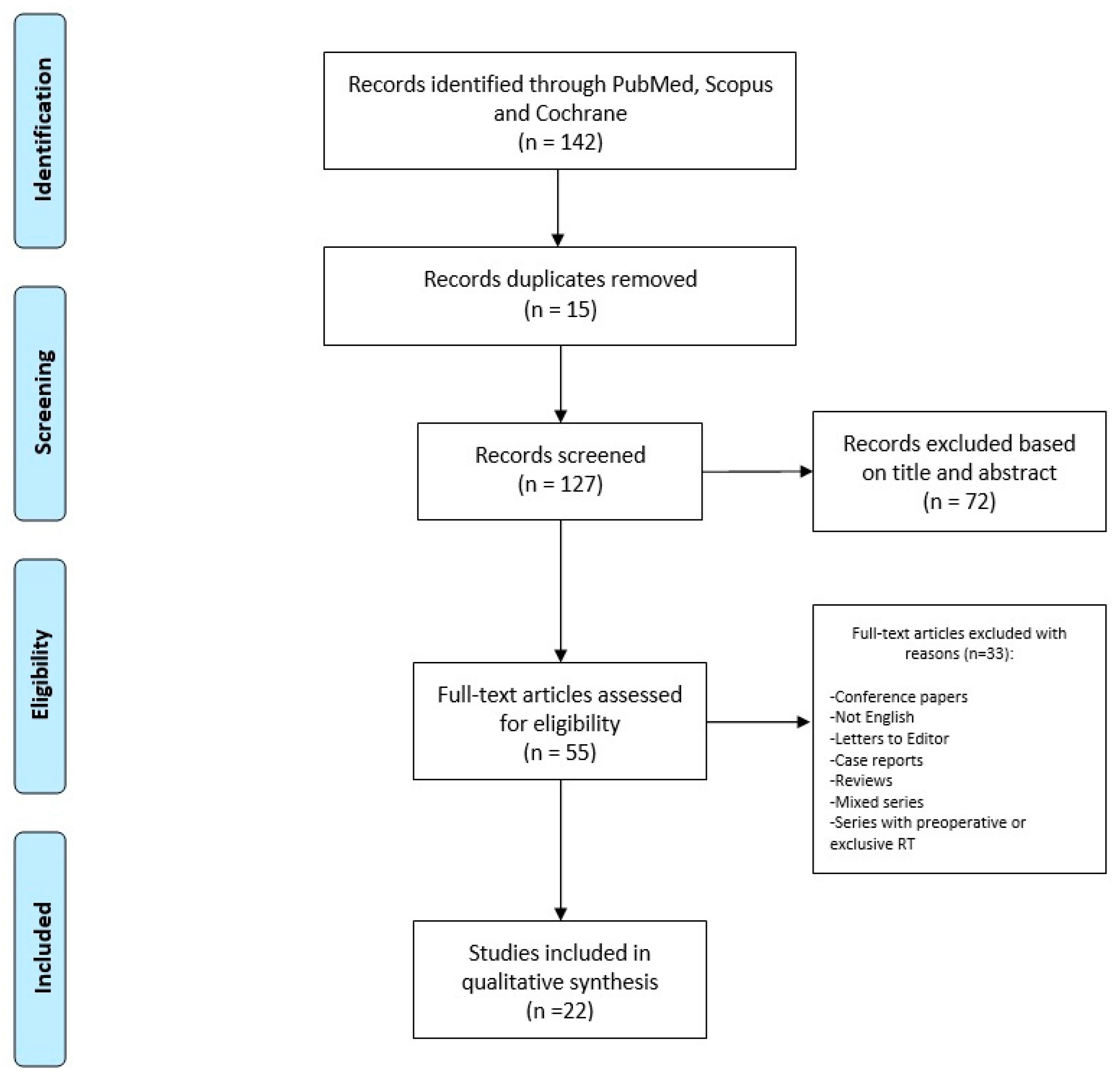
2. Materials and Methods
3. Results
Single Studies Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dai, Z.; He, Y.; Zhang, X.; Tian, Z.; Zhu, G.; Ren, Z.; Ye, L.; Liu, Z.; Ma, C.; Cao, W.; et al. Head-and-neck dermatofibrosarcoma protuberans: Survival analysis and Clinically relevant immunohistochemical indicators. Oral. Dis. 2023; early view. [Google Scholar] [CrossRef]
- Darier, S.; Ferrand, M. Dermatofibrosarcomes progressives etricidivantes on fibrosarcomes de la peau. Ann. Dermatol. Venereol. 1924, 5, 545–562. [Google Scholar]
- Hoffmann, E.D.I. Über das knollentreibende Fibrosarkom der Haut (Dermatofibrosarkoma protuberans). Dermatology 1925, 43, 1–28. [Google Scholar] [CrossRef]
- Trofymenko, O.; Bordeaux, J.S.; Zeitouni, N.C. Survival in patients with primary dermatofibrosarcoma protuberans: National Cancer Database analysis. J. Am. Acad. Dermatol. 2018, 78, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Kreicher, K.L.; Kurlander, D.E.; Gittleman, H.R.; Barnholtz-Sloan, J.S.; Bordeaux, J.S. Incidence and Survival of Primary Dermatofibrosarcoma Protuberans in the United States. Dermatol. Surg. 2016, 42, S24–S31. [Google Scholar] [CrossRef] [PubMed]
- Bowne, W.B.; Antonescu, C.R.; Leung, D.H.; Katz, S.C.; Hawkins, W.G.; Woodruff, J.M.; Brennan, M.F.; Lewis, J.J. Dermatofibrosarcoma protuberans: A clinicopathologic analysis of patients treated and followed at a single institution. Cancer 2000, 88, 2711–2720. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.K.; Jacobs, I.A.; Salti, G.I. Outcomes of surgery for dermatofibrosarcoma protuberans. Eur. J. Surg. Oncol. 2004, 30, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Gloster, H.M., Jr. Dermatofibrosarcoma protuberans. J. Am. Acad. Dermatol. 1996, 35, 355–374. [Google Scholar] [CrossRef]
- LeBlanc, J.; Chan, C.; Zedlitz, A. Dermatofibrosarcoma protuberans. Cutis 2017, 100, E6–E7. [Google Scholar]
- Behfar, K.N.; Mendeszoon, M.J.; Chrzan, J.S.; Habershaw, G.M. Dermatofibrosarcoma protuberans of the hallux. J. Am. Podiatr. Med. Assoc. 1996, 86, 126–128. [Google Scholar] [CrossRef]
- Assassa, G.S.; Siegel, M.E.; Chen, D.C.; Ansari, A.N. Dermatofibrosarcoma protuberans of the toe. Findings on multiple imaging modalities. Clin. Nucl. Med. 1993, 18, 978–980. [Google Scholar] [CrossRef] [PubMed]
- Madden, C.; Spector, A.; Siddiqui, S.; Mirkin, G.; Yim, J.; Hao, X. Dermatofibrosarcoma Protuberans on Adult Toes: A Case Report and Review of the Literature. Anticancer Res. 2019, 39, 2105–2111. [Google Scholar] [CrossRef] [PubMed]
- Takahira, T.; Oda, Y.; Tamiya, S.; Higaki, K.; Yamamoto, H.; Kobayashi, C.; Izumi, T.; Tateishi, N.; Iwamoto, Y.; Tsuneyoshi, M. Detection of COL1A1-PDGFB fusion transcripts and PDGFB/PDGFRB mRNA expression in dermatofibrosarcoma protuberans. Mod. Pathol. 2007, 20, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.G.; Gonda, P.; Sheppard, P.; Keohane, S. Dermatofibrosarcoma Protuberans of the Scalp: A Challenging Tumor with a Proposed Modification to the Slow Mohs Technique. Dermatol. Surg. 2020, 46, 1742–1745. [Google Scholar] [CrossRef] [PubMed]
- Bouhani, M.; Fertani, Y.; Zemni, I.; Adouni, O.; Bouida, A.; Chargui, R.; Khaled, R. Dermatofibrosarcoma Protuberans of the Breast in Man: An Extremely Rare Entity with a Review of the Literature. J. Investig. Med. High. Impact Case Rep. 2019, 7, 2324709619875634. [Google Scholar] [CrossRef]
- Vecchio, G.M.; Broggi, G.; Mulè, A.; Piombino, E.; Magro, G. Dermatofibrosarcoma protuberans: A tumor in the wide spectrum of the bland-looking spindle cell lesions of the breast. Pathologica 2019, 111, 87–91. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Chen, R.; Tang, Z.; Liu, S. A Rare Malignant Disease, Dermatofibrosarcoma Protuberans of the Breast: A Retrospective Analysis and Review of Literature. Biomed. Res. Int. 2020, 2020, 8852182. [Google Scholar] [CrossRef] [PubMed]
- Edelweiss, M.; Malpica, A. Dermatofibrosarcoma protuberans of the vulva: A clinicopathologic and immunohistochemical study of 13 cases. Am. J. Surg. Pathol. 2010, 34, 393–400. [Google Scholar] [CrossRef]
- Ugurel, S.; Kortmann, R.D.; Mohr, P.; Mentzel, T.; Garbe, C.; Breuninger, H.; Bauer, S.; Grabbe, S. S1 guidelines for dermatofibrosarcoma protuberans (DFSP)—Update 2018. J. Dtsch. Dermatol. Ges. 2019, 17, 663–668. [Google Scholar] [CrossRef]
- Ionescu, S.; Nicolescu, A.C.; Madge, O.L.; Simion, L.; Marincas, M.; Ceausu, M. Intra-Abdominal Malignant Melanoma: Challenging Aspects of Epidemiology, Clinical and Paraclinical Diagnosis and Optimal Treatment-A Literature Review. Diagnostics 2022, 12, 2054. [Google Scholar] [CrossRef]
- Gheoca Mutu, D.E.; Avino, A.; Balcangiu-Stroescu, A.E.; Mehedințu, M.; Bălan, D.G.; Brîndușe, L.A.; Popescu, A.M.; Ionescu, D.; Cristea, B.M.; Tomescu, L.F.; et al. Histopathological evaluation of cutaneous malignant melanoma: A retrospective study. Exp. Ther. Med. 2022, 23, 402. [Google Scholar] [CrossRef]
- Tsai, Y.J.; Lin, P.Y.; Chew, K.Y.; Chiang, Y.C. Dermatofibrosarcoma protuberans in children and adolescents: Clinical presentation, histology, treatment, and review of the literature. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1222–1229. [Google Scholar] [CrossRef]
- Apalla, Z.; Liopyris, K.; Kyrmanidou, E.; Fotiadou, C.; Sgouros, D.; Patsatsi, A.; Trakatelli, M.G.; Kalloniati, E.; Lallas, A.; Lazaridou, E. Clinical and Dermoscopic Characteristics of Cutaneous Sarcomas: A Literature Review. Diagnostics 2023, 13, 1822. [Google Scholar] [CrossRef]
- Bernard, J.; Poulalhon, N.; Argenziano, G.; Debarbieux, S.; Dalle, S.; Thomas, L. Dermoscopy of dermatofibrosarcoma protuberans: A study of 15 cases. Br. J. Dermatol. 2013, 169, 85–90. [Google Scholar] [CrossRef]
- Liang, C.A.; Jambusaria-Pahlajani, A.; Karia, P.S.; Elenitsas, R.; Zhang, P.D.; Schmults, C.D. A systematic review of outcome data for dermatofibrosarcoma protuberans with and without fibrosarcomatous change. J. Am. Acad. Dermatol. 2014, 71, 781–786. [Google Scholar] [CrossRef]
- Mentzel, T.; Beham, A.; Katenkamp, D.; Dei Tos, A.P.; Fletcher, C.D. Fibrosarcomatous (“high-grade”) dermatofibrosarcoma protuberans: Clinicopathologic and immunohistochemical study of a series of 41 cases with emphasis on prognostic significance. Am. J. Surg. Pathol. 1998, 22, 576–587. [Google Scholar] [CrossRef]
- Mareş, T.; Răducu, L.; Avino, A.; Gheoca-Mutu, D.E.; Teodoreanu, R.N.; Jecan, C.R. Dermatofibrosarcoma Protuberans: One Centre Experience. Chirurgia 2022, 117, 601–617. [Google Scholar] [CrossRef]
- Saiag, P.; Grob, J.J.; Lebbe, C.; Malvehy, J.; del Marmol, V.; Pehamberger, H.; Peris, K.; Stratigos, A.; Middelton, M.; Basholt, L.; et al. Diagnosis and treatment of dermatofibrosarcoma protuberans. European consensus-based interdisciplinary guideline. Eur. J. Cancer 2015, 51, 2604–2608. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, A.; Abeni, D.; Rusciani, A.; Cigna, E.; Wolter, M.; Scuderi, N.; Rusciani, L.; Kaufmann, R.; Podda, M. Dermatofibrosarcoma protuberans: Wide local excision vs. Mohs micrographic surgery. Cancer Treat. Rev. 2008, 34, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Metgudmath, R.B.; Metgudmath, A.R.; Das, A.T.; Malur, P.R. Dermatofibrosarcoma Protuberans of Face: A Rare Entity and Review of Literature. Indian. J. Otolaryngol. Head. Neck Surg. 2022, 74, 5469–5472. [Google Scholar] [CrossRef]
- Fields, R.C.; Hameed, M.; Qin, L.X.; Moraco, N.; Jia, X.; Maki, R.G.; Singer, S.; Brennan, M.F. Dermatofibrosarcoma protuberans (DFSP): Predictors of recurrence and the use of systemic therapy. Ann. Surg. Oncol. 2011, 18, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Henry, O.S.; Platoff, R.; Cerniglia, K.S.; Batchu, S.; Goodwin, B.J.; Sandilos, G.; Adams, A.; Hong, Y.K. Tyrosine kinase inhibitors versus radiation therapy in unresectable dermatofibrosarcoma protuberans (DFSP): A narrative systematic review. Am. J. Surg. 2023, 225, 268–274. [Google Scholar] [CrossRef]
- Du, K.; Li, J.; Tang, L.; Lin, X.; Kong, X.; Liao, X.; Peng, Q.; Dong, Y.; He, J.; Huang, Y.; et al. Role of postoperative radiotherapy in dermatofibrosarcoma protuberans: A propensity score-matched analysis. Radiat. Oncol. 2019, 14, 20. [Google Scholar] [CrossRef]
- Williams, N.; Morris, C.G.; Kirwan, J.M.; Dagan, R.; Mendenhall, W.M. Radiotherapy for dermatofibrosarcoma protuberans. Am. J. Clin. Oncol. 2014, 37, 430–432. [Google Scholar] [CrossRef]
- Hamid, R.; Hafeez, A.; Darzi, M.A.; Zaroo, I.; Rasool, A.; Rashid, H. Outcome of wide local excision in dermatofibrosarcoma protuberans and use of radiotherapy for margin-positive disease. Indian. Dermatol. Online J. 2013, 4, 93–96. [Google Scholar] [CrossRef]
- Uysal, B.; Sager, O.; Gamsiz, H.; Cicek, A.; Demiral, S.; Dincoglan, F.; Surenkok, S.; Demiriz, M.; Beyzadeoglu, M. Evaluation of the role of radiotherapy in the management of dermatofibrosarcoma protuberans. J. BUON 2013, 18, 268–273. [Google Scholar] [PubMed]
- Castle, K.O.; Guadagnolo, B.A.; Tsai, C.J.; Feig, B.W.; Zagars, G.K. Dermatofibrosarcoma protuberans: Long-term outcomes of 53 patients treated with conservative surgery and radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 585–590. [Google Scholar] [CrossRef]
- Palmerini, E.; Gambarotti, M.; Staals, E.L.; Zanella, L.; Sieberova, G.; Longhi, A.; Cesari, M.; Bonarelli, S.; Picci, P.; Ruggieri, P.; et al. Fibrosarcomatous changes and expression of CD34+ and apolipoprotein-D in dermatofibrosarcoma protuberans. Clin. Sarcoma Res. 2012, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Archontaki, M.; Korkolis, D.P.; Arnogiannaki, N.; Konstantinidou, C.; Georgopoulos, S.; Dendrinos, P.; Zarkadas, G.; Kokkalis, G. Dermatofibrosarcoma protuberans: A case series of 16 patients treated in a single institution with literature review. Anticancer Res. 2010, 30, 3775–3779. [Google Scholar] [PubMed]
- Heuvel, S.T.; Suurmeijer, A.; Pras, E.; Van Ginkel, R.J.; Hoekstra, H.J. Dermatofibrosarcoma protuberans: Recurrence is related to the adequacy of surgical margins. Eur. J. Surg. Oncol. 2010, 36, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Dagan, R.; Morris, C.G.; Zlotecki, R.A.; Scarborough, M.T.; Mendenhall, W.M. Radiotherapy in the treatment of dermatofibrosarcoma protuberans. Am. J. Clin. Oncol. 2005, 28, 537–539. [Google Scholar] [CrossRef]
- DuBay, D.; Cimmino, V.; Lowe, L.; Johnson, T.M.; Sondak, V.K. Low recurrence rate after surgery for dermatofibrosarcoma protuberans: A multidisciplinary approach from a single institution. Cancer 2004, 100, 1008–1016. [Google Scholar] [CrossRef]
- Sun, L.M.; Wang, C.J.; Huang, C.C.; Leung, S.W.; Chen, H.C.; Fang, F.M.; Huang, E.Y.; Lee, S.P. Dermatofibrosarcoma protuberans:treatment results of 35 cases. Radiother. Oncol. 2000, 57, 175–181. [Google Scholar] [CrossRef]
- Stojadinovic, A.; Karpoff, H.M.; Antonescu, C.R.; Shah, J.P.; Singh, B.; Spiro, R.H.; Dumornay, W.; Shaha, A.R. Dermatofibrosarcoma protuberans of the head and neck. Ann. Surg. Oncol. 2000, 7, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Ballo, M.T.; Zagars, G.K.; Pisters, P.; Pollack, A. The role of radiation therapy in the management of dermatofibrosarcoma protuberans. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Haas, R.L.; Keus, R.B.; Loftus, B.M.; Rutgers, E.J.; van Coevorden, F.; Bartelink, H. The role of radiotherapy in the local management of dermatofibrosarcoma protuberans. Soft Tissue Tumours Working Group. Eur. J. Cancer 1997, 33, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Suit, H.; Spiro, I.; Mankin, H.J.; Efird, J.; Rosenberg, A.E. Radiation in management of patients with dermatofibrosarcoma protuberans. J. Clin. Oncol. 1996, 14, 2365–2369. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.B.; Suit, H.D.; Rosenberg, A.E.; Wood, W.C. Dermatofibrosarcoma protuberans treated with radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1989, 17, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, T.; Yamamoto, H.; Oda, Y. Current Update on the Molecular Biology of Cutaneous Sarcoma: Dermatofibrosarcoma Protuberans. Curr. Treat. Options Oncol. 2019, 20, 29. [Google Scholar] [CrossRef]
- McArthur, G. Molecularly targeted treatment for dermatofibrosarcoma protuberans. Semin. Oncol. 2004, 31, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Lemm, D.; Mügge, L.O.; Mentzel, T.; Höffken, K. Current treatment options in dermatofibrosarcoma protuberans. J. Cancer Res. Clin. Oncol. 2009, 135, 653–665. [Google Scholar] [CrossRef]
- Sundram, U.N. Review: Dermatofibrosarcoma protuberans: Histologic approach and updated treatment recommendations. Clin. Adv. Hematol. Oncol. 2009, 7, 406–408. [Google Scholar] [PubMed]
- Monnier, D.; Vidal, C.; Martin, L.; Danzon, A.; Pelletier, F.; Puzenat, E.; Algros, M.P.; Blanc, D.; Laurent, R.; Humbert, P.H.; et al. Dermatofibrosarcoma protuberans: A population-based cancer registry descriptive study of 66 consecutive cases diagnosed between 1982 and 2002. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 1237–1242. [Google Scholar] [CrossRef] [PubMed]
- Khatri, V.P.; Galante, J.M.; Bold, R.J.; Schneider, P.D.; Ramsamooj, R.; Goodnight, J.E., Jr. Dermatofibrosarcoma protuberans: Reappraisal of wide local excision and impact of inadequate initial treatment. Ann. Surg. Oncol. 2003, 10, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Gualdi, G.; La Rosa, G.; Di Buduo, A.; Paradisi, A.; Soglia, S.; Calzavara-Pinton, P.; Amerio, P. Conventional surgery compared with formalin-fixed tissue Mohs surgery (slow Mohs) for DFSP: A comparative analysis of 83 cases. J. Eur. Acad. Dermatol. Venereol. 2023, 37, e1393–e1395. [Google Scholar] [CrossRef]
- Snow, S.N.; Gordon, E.M.; Larson, P.O.; Bagheri, M.M.; Bentz, M.L.; Sable, D.B. Dermatofibrosarcoma protuberans: A report on 29 patients treated by Mohs micrographic surgery with long-term follow-up and review of the literature. Cancer 2004, 101, 28–38. [Google Scholar] [CrossRef]
- Massey, R.A.; Tok, J.; Strippoli, B.A.; Szabolcs, M.J.; Silvers, D.N.; Eliezri, Y.D. A comparison of frozen and paraffin sections in dermatofibrosarcoma protuberans. Dermatol. Surg. 1998, 24, 995–998. [Google Scholar] [CrossRef]
- Khaddaj, L.; Martinot-Duquennoy, V.; Guerreschi, P.; Mortier, L.; Calibre, C. Mohs micrographic surgery for skin cancers: A 10 year-single-center series of 548 patients treated by formalin-fixed tissue Mohs surgery assessing the impact of reduced margins. Ann. Chir. Plast. Esthet. 2021, 6, 429–439. [Google Scholar] [CrossRef]
- Sondak, V.K.; Cimmino, V.M.; Lowe, L.M.; Dubay, D.A.; Johnson, T.M. Dermatofibrosarcoma protuberans: What is the best surgical approach? Surg. Oncol. 1999, 8, 183–189. [Google Scholar] [CrossRef]
- Rutkowski, P.; Debiec-Rychter, M. Current treatment options for dermatofibrosarcoma protuberans. Expert. Rev. Anticancer Ther. 2015, 15, 901–909. [Google Scholar] [CrossRef]
- Verma, H.; Sehgal, K.; Panchal, K.B.; Chakraborty, S.; Biswas, B.; Mukherjee, G.; Midha, D.; Biswas, G. Presentation and Management of Dermatofibrosarcoma Protuberans: A Single Center Protocol. Indian. J. Surg. Oncol. 2020, 11, 35–40. [Google Scholar] [CrossRef]
- Buck, D.W., 2nd; Kim, J.Y.; Alam, M.; Rawlani, V.; Johnson, S.; Connor, C.M.; Dumanian, G.A.; Wayne, J.D. Multidisciplinary approach to the management of dermatofibrosarcoma protuberans. J. Am. Acad. Dermatol. 2012, 67, 861–866. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Country | N of Patients | Mean Age (Yrs) | Gender (Male/ Female) | Initial Site | Largest Size (cm) | Prior Surgery | Postoperative Radiotherapy | Indication for RT | Doses | Local Control | Median Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dai et al., 2023 [1] | China | 49 | 48 | 92.7%/7.3% | H&N 100% | 11 | 100% | 16.3% | A/S | 60 Gy | 100% | 85 |
| Mareş et al., 2022 [27] | Romania | 7 | 38 | 57.1%/42.9% | Trunk 71.4% Extremities 28.6% | >5 | 100% | 42.9% | A | 50–60 Gy | n.a. | 12 |
| Wang et al., 2020 [17] | China | 6 | 30 | 16.7%/83.3% | Trunk 100% | 3 | 100% | 33.3% | A | n.a. | 100% | 36 |
| Du et al., 2019 [33] | China | 184 | 41 | 76.1%/23.9% | H&N 17.4% Trunk 71.7% Extremities 10.9% | 20 | 100% | 23.9% | A/S | 50–66 Gy | 94.6% * | 58 |
| Tsai et al., 2014 [22] | Taiwan | 13 | 11 | 46.2%/53.8% | H&N 7.7% Trunk 69.2% Extremities 23.1% | 8 | 100% | 23.1% | A/S | n.a. | 100% | 129 |
| Williams et al., 2014 [34] | USA | 14 | 42 | 50%/50% | H&N 57.1% Trunk 7.2% Extremities 35.7% | 12 | 92.9% | 92.9% | A | 56–66 Gy | 85.7% | 126 |
| Hamid et al., 2013 [35] | India | 36 | 38 | 72.2%/27.8% | H&N 8.3% Trunk 58.4% Extremities 33.3% | 20 | 83.3% | 83.3% | A | 65–70 Gy | 80% | 68 |
| Uysal et al., 2013 [36] | Turkey | 28 | 26 | 64.3%/35.7% | H&N 14% Trunk 22% Extremities 64% | 8.4 | 89.3% | 89.3% | A/S | 50–70 Gy | 89.6% ** | 81 |
| Castle et al., 2013 [37] | USA | 53 | 41 | 57%/43% | H&N 36% Trunk 36% Extremities 28% | 25 | 100% | 87% | A/S | 60–66 Gy | 90% | 78 |
| Palmerini et al., 2012 [38] | Italy | 40 | 39 | 55%/45% | Trunk 40% Extremities 60% | n.a. | 90% | 27% | A | n.a. | 77% | 49 |
| Fields et al., 2011 [31] | USA | 244 | 42 | 50%/50% | H&N 14% Trunk 34% Extremities 52% | >5 | 100% | 5.7% | S | n.a. | 100% | 50 |
| Archontaki et al., 2010 [39] | Greece | 16 | 41 | 43.6%/56.4% | H&N 31.2% Trunk 56.3% Extremities 12.5% | 22.5 | 100% | 18.75% | A | n.a. | 100% | 44 |
| Heuvel et al., 2010 [40] | The Netherlands | 38 | 38 | 65.8%/34.2% | H&N 16.7% Trunk 66.6% Extremities 16.7% | 22 | 100% | 21% | A/S | 50–70 Gy | 87.5% | 89 |
| Dagan et al., 2005 [41] | USA | 10 | 39 | 50%/50% | H&N 60% Trunk 10% Extremities 30% | 9 | 100% | 100% | A/S | 60–65 Gy | 90% | 95 |
| DuBay et al., 2004 [42] | USA | 62 | 42 | 37%/63% | H&N 24% Trunk/Extremities 76% | 10 | 100% | 5% | S | n.a. | 100% | 53 |
| Sun et al., 2000 [43] | Taiwan | 35 | 37 | 68.6%/31.4% | H&N 17.1%. Trunk 60% Extremities 22.9% | 25 | 100% | 28.5% | S | 46–68 Gy | 81.8% | 50 |
| Stojadinovic et al., 2000 [44] | USA | 33 | 39 | 48.5%/51.5% | H&N 100% | 8 | 100% | 12.1% | S | 60–66 Gy | 75% | 82 |
| Mentzel et al., 1998 [26] | USA | 41 | 48 | 54%/46% | H&N 12% Trunk 63% Extremities 25% | n.a. | 100% | 7.4% | A | n.a. | n.a. | 90 |
| Ballo et al., 1998 [45] | USA | 19 | 40 | 63.2%/36.8% | H&N 36.8% Trunk 42.1% Extremity 21% | 15 | 100% | 100% | A/S | 50–66 Gy | 94.7% | 72 |
| Haas et al., 1997 [46] | The Netherlands | 38 | 39 | 42.1%/57.9% | H&N 13% Trunk 44% Extremities 33% | n.a. | 100% | 44.7% | A/S | 50–66 Gy | 82.4% | 68 |
| Suit et al., 1996 [47] | USA | 18 | 46 | 61.1%/38.9% | H&N 55.5% Trunk 27.8% Extremities 16.7% | 10 | 83.3% | 66.6% | A/S | 50–67 Gy | 83.3% | 86 |
| Marks et al., 1989 [48] | USA | 10 | 44.4 | 60%/40% | H&N 50% Trunk 40% Extremities 10% | 8.5 | 70% | 70% | A/S | 60–67 Gy | 90% | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fionda, B.; Loperfido, A.; Di Stefani, A.; Lancellotta, V.; Paradisi, A.; De Angeli, M.; Cappilli, S.; Rossi, E.; Caretto, A.A.; Zinicola, T.; et al. The Role of Postoperative Radiotherapy in the Management of Dermatofibrosarcoma Protuberans: A Multidisciplinary Systematic Review. J. Clin. Med. 2024, 13, 1798. https://doi.org/10.3390/jcm13061798
Fionda B, Loperfido A, Di Stefani A, Lancellotta V, Paradisi A, De Angeli M, Cappilli S, Rossi E, Caretto AA, Zinicola T, et al. The Role of Postoperative Radiotherapy in the Management of Dermatofibrosarcoma Protuberans: A Multidisciplinary Systematic Review. Journal of Clinical Medicine. 2024; 13(6):1798. https://doi.org/10.3390/jcm13061798
Chicago/Turabian StyleFionda, Bruno, Antonella Loperfido, Alessandro Di Stefani, Valentina Lancellotta, Andrea Paradisi, Martina De Angeli, Simone Cappilli, Ernesto Rossi, Anna Amelia Caretto, Tiziano Zinicola, and et al. 2024. "The Role of Postoperative Radiotherapy in the Management of Dermatofibrosarcoma Protuberans: A Multidisciplinary Systematic Review" Journal of Clinical Medicine 13, no. 6: 1798. https://doi.org/10.3390/jcm13061798
APA StyleFionda, B., Loperfido, A., Di Stefani, A., Lancellotta, V., Paradisi, A., De Angeli, M., Cappilli, S., Rossi, E., Caretto, A. A., Zinicola, T., Schinzari, G., Gentileschi, S., Morganti, A. G., Rembielak, A., Peris, K., & Tagliaferri, L. (2024). The Role of Postoperative Radiotherapy in the Management of Dermatofibrosarcoma Protuberans: A Multidisciplinary Systematic Review. Journal of Clinical Medicine, 13(6), 1798. https://doi.org/10.3390/jcm13061798