

A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates

 ,
, 
 and
and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Inclusion Criteria
2.2. Quality Assessment
2.3. Data Extraction
2.4. Statistical Analysis, One- and Two-Stage Meta-Analysis with Individual Patient Data
3. Results
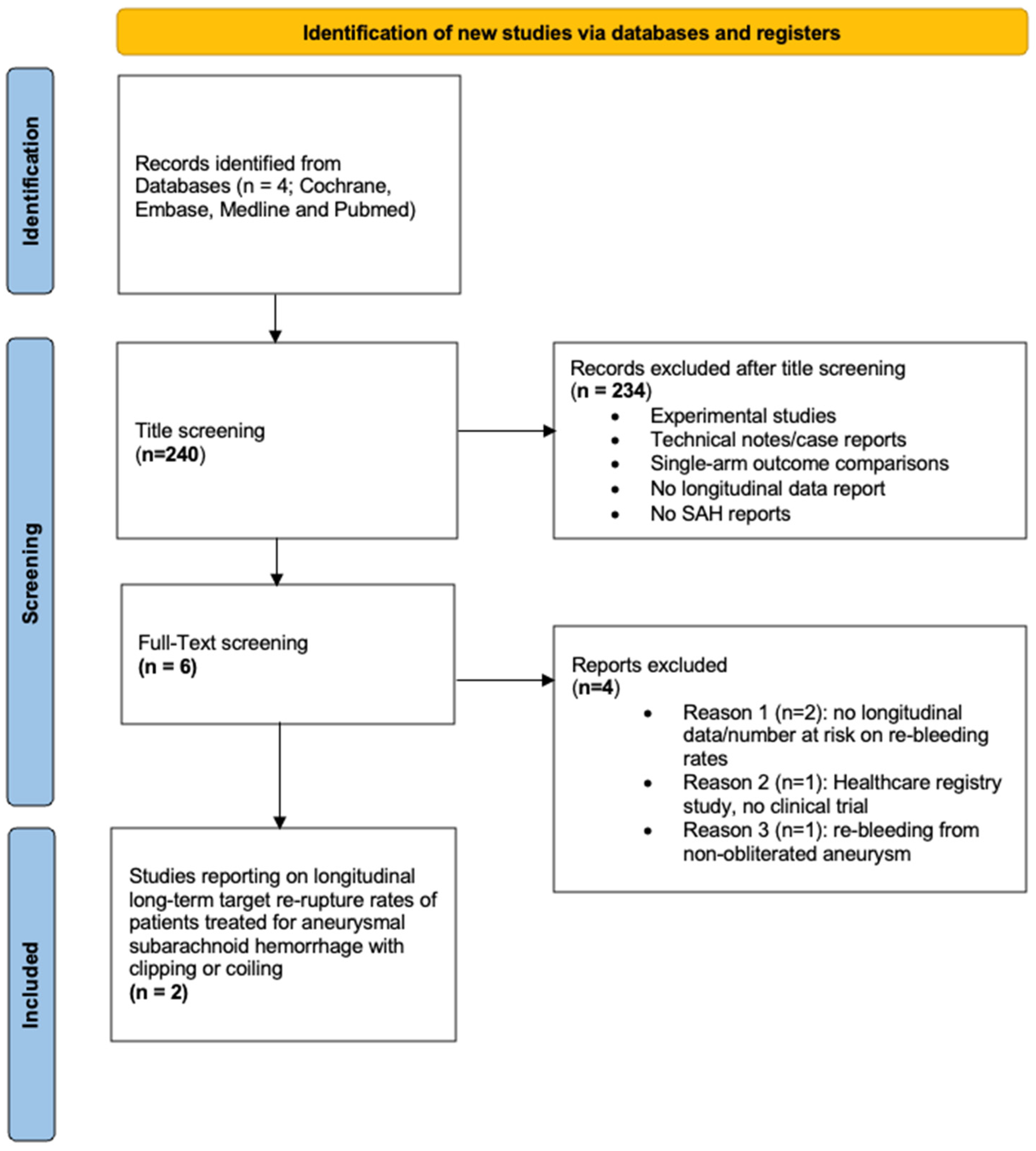
3.1. Study Selection and Study Characteristics
3.2. Individual Patient Data Cohort Characteristics
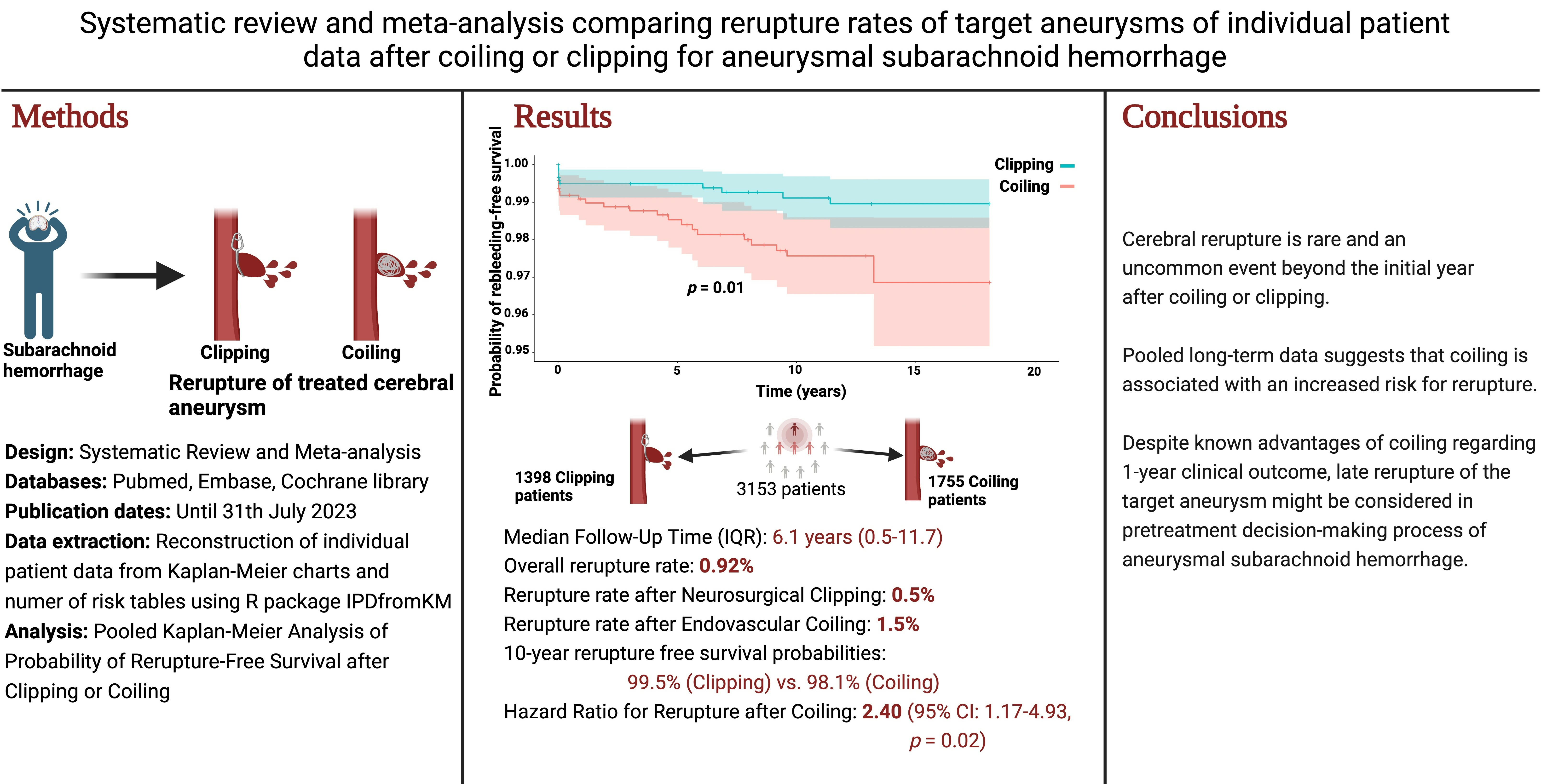
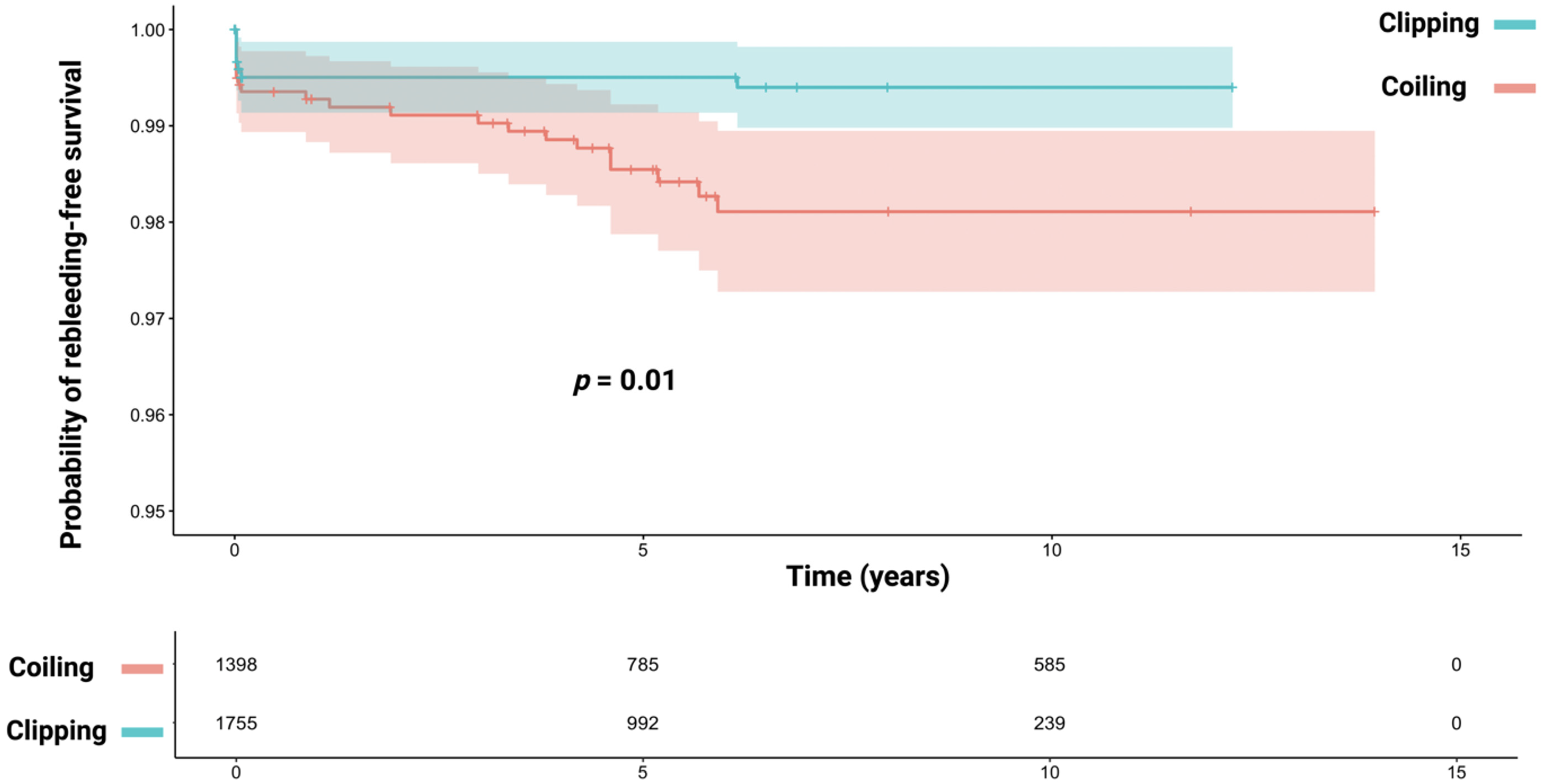
3.3. Reconstructed Pooled Rerupture-Free Survival Curves and One-Stage Meta-Analysis of the Impact of Primary Aneurysm Treatment on Rerupture-Free Survival in aSAH
3.4. Two-Stage Meta-Analysis of Treatment Modalities Regarding Target Aneurysm Rerupture Based on Inidividual Patient Data
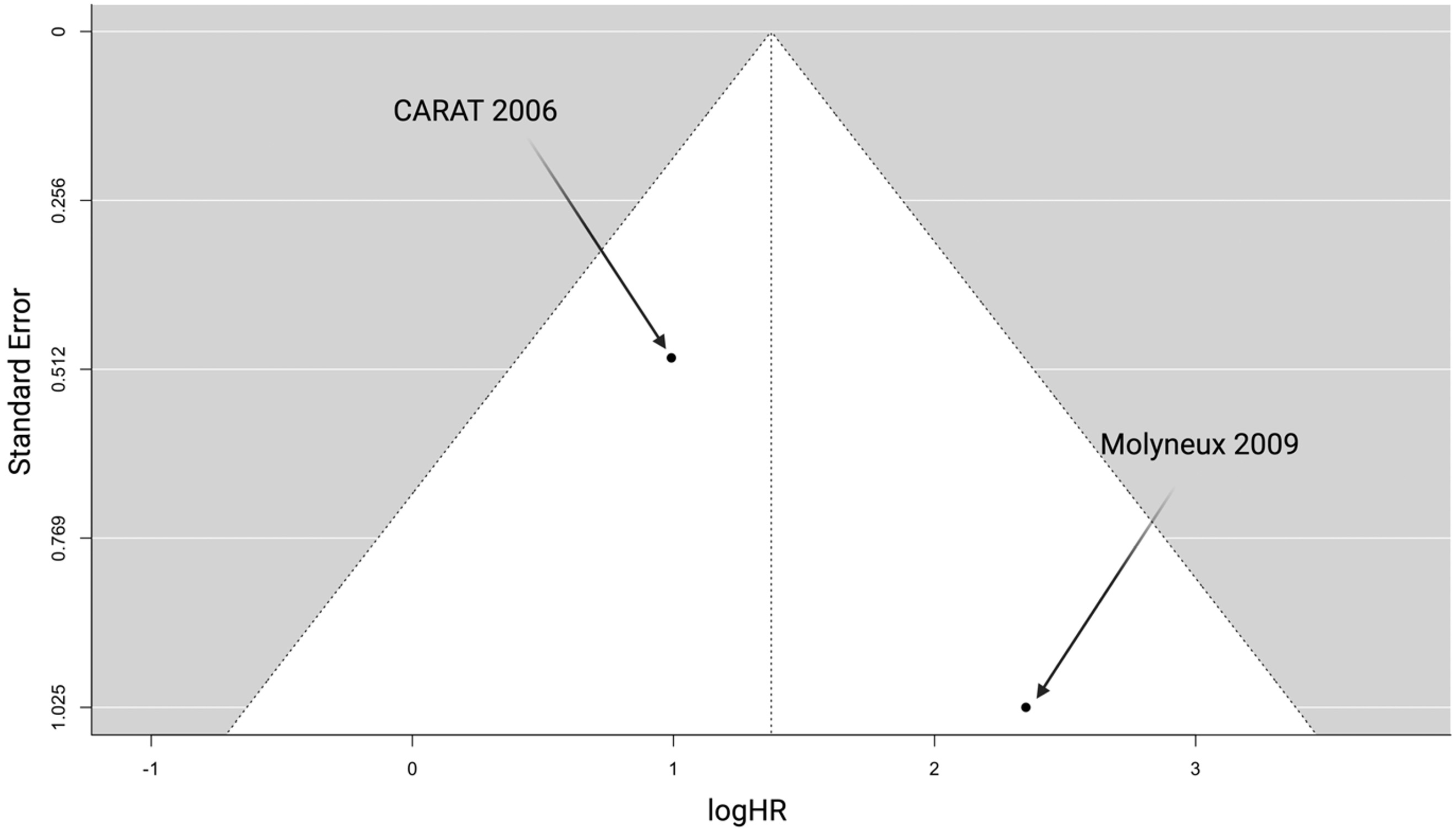
3.5. Publication Bias and Quality Evaluation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petridis, A.K.; Kamp, M.A.; Cornelius, J.F.; Beez, T.; Beseoglu, K.; Turowski, B.; Steiger, H.J. Aneurysmal Subarachnoid Hemorrhage. Dtsch. Arztebl. Int. 2017, 114, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Scibilia, A.; Rustici, A.; Linari, M.; Zenesini, C.; Belotti, L.M.B.; Dall’Olio, M.; Princiotta, C.; Cuoci, A.; Aspide, R.; Migliorino, E.; et al. Factors affecting 30-day mortality in poor-grade aneurysmal subarachnoid hemorrhage: A 10-year single-center experience. Front. Neurol. 2024, 15, 1286862. [Google Scholar] [CrossRef] [PubMed]
- Spetzler, R.F.; McDougall, C.G.; Zabramski, J.M.; Albuquerque, F.C.; Hills, N.K.; Russin, J.J.; Partovi, S.; Nakaji, P.; Wallace, R.C. The Barrow Ruptured Aneurysm Trial: 6-year results. J. Neurosurg. 2015, 123, 609–617. [Google Scholar] [CrossRef]
- Bakker, N.A.; Metzemaekers, J.D.; Groen, R.J.; Mooij, J.J.; Van Dijk, J.M. International subarachnoid aneurysm trial 2009: Endovascular coiling of ruptured intracranial aneurysms has no significant advantage over neurosurgical clipping. Neurosurgery 2010, 66, 961–962. [Google Scholar] [CrossRef]
- Hoh, B.L.; Ko, N.U.; Amin-Hanjani, S.; Chou, S.H.-Y.; Cruz-Flores, S.; Dangayach, N.S.; Derdeyn, C.P.; Du, R.; Hänggi, D.; Hetts, S.W.; et al. 2023 Guideline for the Management of Patients with Aneurysmal Subarachnoid Hemorrhage: A Guideline from the American Heart Association/American Stroke Association. Stroke 2023, 54, e314–e370. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Sprengers, M.E.; van Rooij, W.J.; Sluzewski, M.; Majoie, C.B.; Wermer, M.J.; Rinkel, G.J. Long-term recurrent subarachnoid hemorrhage after adequate coiling versus clipping of ruptured intracranial aneurysms. Stroke 2009, 40, 1758–1763. [Google Scholar] [CrossRef]
- Yu, L.B.; Fang, Z.J.; Yang, X.J.; Zhang, D. Management of Residual and Recurrent Aneurysms After Clipping or Coiling: Clinical Characteristics, Treatments, and Follow-Up Outcomes. World Neurosurg. 2019, 122, e838–e846. [Google Scholar] [CrossRef] [PubMed]
- Stewart, L.A.; Tierney, J.F. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval. Health Prof. 2002, 25, 76–97. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F.; PRISMA-IPD Development Group. Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: The PRISMA-IPD Statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Wenig, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Rakap, S.; Rakap, S.; Evran, D.; Cig, O. Comparative evaluation of the reliability and validity of three data extraction programs: UnGraph, GraphClick, and DigitizeIt. Comput. Hum. Behav. 2016, 55, 159–166. [Google Scholar] [CrossRef]
- Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: Reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2021, 21, 111. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.4; Cochrane: London, UK, 2023. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- CARAT Investigators. Rates of delayed rebleeding from intracranial aneurysms are low after surgical and endovascular treatment. Stroke 2006, 37, 1437–1442. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.; Birks, J.; Ramzi, N.; Yarnold, J.; Sneade, M.; Rischmiller, J.; ISAT Collaborators. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): Long-term follow-up. Lancet Neurol. 2009, 8, 427–433. [Google Scholar] [CrossRef]
- Wermer, M.J.; Greebe, P.; Algra, A.; Rinkel, G.J. Incidence of recurrent subarachnoid hemorrhage after clipping for ruptured intracranial aneurysms. Stroke 2005, 36, 2394–2399. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, A.; Kerr, R.; Stratton, I.; Sandercock, P.; Clarke, M.; Shrimpton, J.; Holman, R.; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet 2002, 360, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Spetzler, R.F.; McDougall, C.G.; Zabramski, J.M.; Albuquerque, F.C.; Hills, N.K.; Nakaji, P.; Karis, J.P.; Wallace, R.C. Ten-year analysis of saccular aneurysms in the Barrow Ruptured Aneurysm Trial. J. Neurosurg. 2019, 132, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, A.J.; Birks, J.; Clarke, A.; Sneade, M.; Kerr, R.S. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet 2015, 385, 691–697. [Google Scholar] [CrossRef]
- Li, H.; Pan, R.; Wang, H.; Rong, X.; Yin, Z.; Milgrom, D.P.; Shi, X.; Tang, Y.; Peng, Y. Clipping versus coiling for ruptured intracranial aneurysms: A systematic review and meta-analysis. Stroke 2013, 44, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Benaissa, A.; Barbe, C.; Pierot, L. Analysis of recanalization after endovascular treatment of intracranial aneurysm (ARETA trial): Presentation of a prospective multicenter study. J. Neuroradiol. 2015, 42, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Dowd, C.F.; Higashida, R.T.; Lawton, M.T.; Duckwiler, G.R.; Gress, D.R.; CARAT Investigators. Predictors of rehemorrhage after treatment of ruptured intracranial aneurysms: The Cerebral Aneurysm Rerupture After Treatment (CARAT) study. Stroke 2008, 39, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Ling, X.; Petersen, J.D.; Liu, J.; Xiao, A.; Huang, J. Clipping versus coiling for aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis of prospective studies. Neurosurg. Rev. 2022, 45, 1291–1302. [Google Scholar] [CrossRef] [PubMed]
- Tsurumi, A.; Tsurumi, Y.; Negoro, M.; Tsugane, S.; Ryuge, M.; Susaki, N.; Fukuoka, T.; Miyachi, S. Delayed rupture of a basilar artery aneurysm treated with coils: Case report and review of the literature. J. Neuroradiol. 2013, 40, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, S.K.; Shapiro, S.A.; Cohen-Gadol, A.A.; Sahlein, D.H. Endovascular Retreatment of Previously Ruptured Coiled Cerebral Aneurysm Remnants Significantly Reduces Rebleed Rate. World Neurosurg. 2021, 147, e382–e387. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.J.; Park, Y.K.; Cho, D.Y.; Choi, J.H.; Kim, B.S.; Shin, Y.S. Predictors of the Effects of Flow Diversion in Very Large and Giant Aneurysms. AJNR Am. J. Neuroradiol. 2021, 42, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Cagnazzo, F.; Ahmed, R.; Dargazanli, C.; Lefevre, P.H.; Gascou, G.; Derraz, I.; Kalmanovich, S.A.; Riquelme, C.; Bonafe, A.; Costalat, V. Treatment of Wide-Neck Intracranial Aneurysms with the Woven EndoBridge Device Associated with Stenting: A Single-Center Experience. AJNR Am. J. Neuroradiol. 2019, 40, 820–826. [Google Scholar] [CrossRef]
- Park, K.Y.; Jang, C.K.; Lee, J.W.; Kim, D.J.; Kim, B.M.; Chung, J. Preliminary experience of stent-assisted coiling of wide-necked intracranial aneurysms with a single microcatheter. BMC Neurol. 2019, 19, 245. [Google Scholar] [CrossRef]
- Raymond, J.; Kotowski, M.; Darsaut, T.E.; Molyneux, A.J.; Kerr, R.S. Ruptured aneurysms and the International Subarachnoid Aneurysm Trial (ISAT): What is known and what remains to be questioned. Neurochirurgie 2012, 58, 103–114, (In English, In French). [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Country | Study Interval | Study Design | Total No. | Endovascular Coiling, No. (%) | Neurosurgical Clipping, No. (%) | Follow-Up |
|---|---|---|---|---|---|---|---|
| CARAT Investigators et al., 2006 [16] | United States of America | 1 January 1996–31 December 1998 | Ambidirectional multicentric Cohort study | 1010 | 299 (29.6%) | 711 (70.4%) | Clipping: 4.4 years (mean) Coiling: 3.7 years (mean) |
| Molyneux et al., 2009 [17] | United Kingdom, several European countries, Australia, Canada, and United States of America | 1997–May 2002 | Prospective randomized multicentric study | 2143 | 1073 (50.1%) | 1070 (49.9%) | 9 years (mean) |
| Parameters | CARAT Investigators et al. [16] | Molyneux et al. [17] | p * |
|---|---|---|---|
| Sex Female Male | 696/1010 (68.9%) 314/1010 (31.1%) | 1345/2143 (62.8%) 798/2143 (37.2%) | 0.009 |
| Age (in years) | Coiling: 58.5 (mean) (SD:15.1) Clipping: 53.5 (mean) (SD:13.8) | Coiling: 52.0 (median) (IQR:44.0–60.0) Clipping: 52.0 (median) (IQR: 43–60) | NA |
| Poor-grade aSAH (WFNS or Hunt and Hess grades IV–V) | 203/1010 (20.1%) | 94/2112 (4.5%) (unavailable WFNS data in 31 patients) | 0.0001 |
| Aneurysm size >10 mm | 147/1010 (14.6%) | 155/2143 (7.2%) | 0.0001 |
| Parameters | Clipping | Coiling | p * |
|---|---|---|---|
| Sex Female Male | 1161/1781 (65.2%) 620/1781 (34.8%) | 880/1372 (64.1%) 492/1372(35.9%) | 0.57 |
| Poor-grade aSAH (WFNS or Hunt and Hess grades IV–V) | 177/1765 (10.0%) (Not available in 1 patient in CARAT Investigators et al. [16] and in 16 patients of Molyneux et al. [17]) | 120/1357 (8.8%) (Not available in 5 patients in CARAT Investigators et al. [16] and in 15 patients of Molyneux et al. [17]) | 0.27 |
| Aneurysm size >10 mm | 110/1781 (6.2%) | 62/1372 (4.5%) | 0.048 |
| Endpoint | Study, Year | Estimated HR (95% CI) |
|---|---|---|
| Rerupture-free survival | CARAT Investigators et al., 2006 [16] | 2.70 (1.03–7.05) |
| Molyneux et al., 2009 [17] | 10.52 (1.34–82.50) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wach, J.; Vychopen, M.; Güresir, A.; Guranda, A.; Nestler, U.; Güresir, E. A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates. J. Clin. Med. 2024, 13, 1778. https://doi.org/10.3390/jcm13061778
Wach J, Vychopen M, Güresir A, Guranda A, Nestler U, Güresir E. A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates. Journal of Clinical Medicine. 2024; 13(6):1778. https://doi.org/10.3390/jcm13061778
Chicago/Turabian StyleWach, Johannes, Martin Vychopen, Agi Güresir, Alexandru Guranda, Ulf Nestler, and Erdem Güresir. 2024. "A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates" Journal of Clinical Medicine 13, no. 6: 1778. https://doi.org/10.3390/jcm13061778
APA StyleWach, J., Vychopen, M., Güresir, A., Guranda, A., Nestler, U., & Güresir, E. (2024). A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates. Journal of Clinical Medicine, 13(6), 1778. https://doi.org/10.3390/jcm13061778