
The Longitudinal Association between Multiple Frailty Criteria and Depressive Symptomatology Five Years Later in Older Adults: A Decision Tree Modelling Approach

 ,
,  ,
,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
Dependent Variable: Depression
2.3. Independent Variables
Frailty
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Binomial Regression Analysis
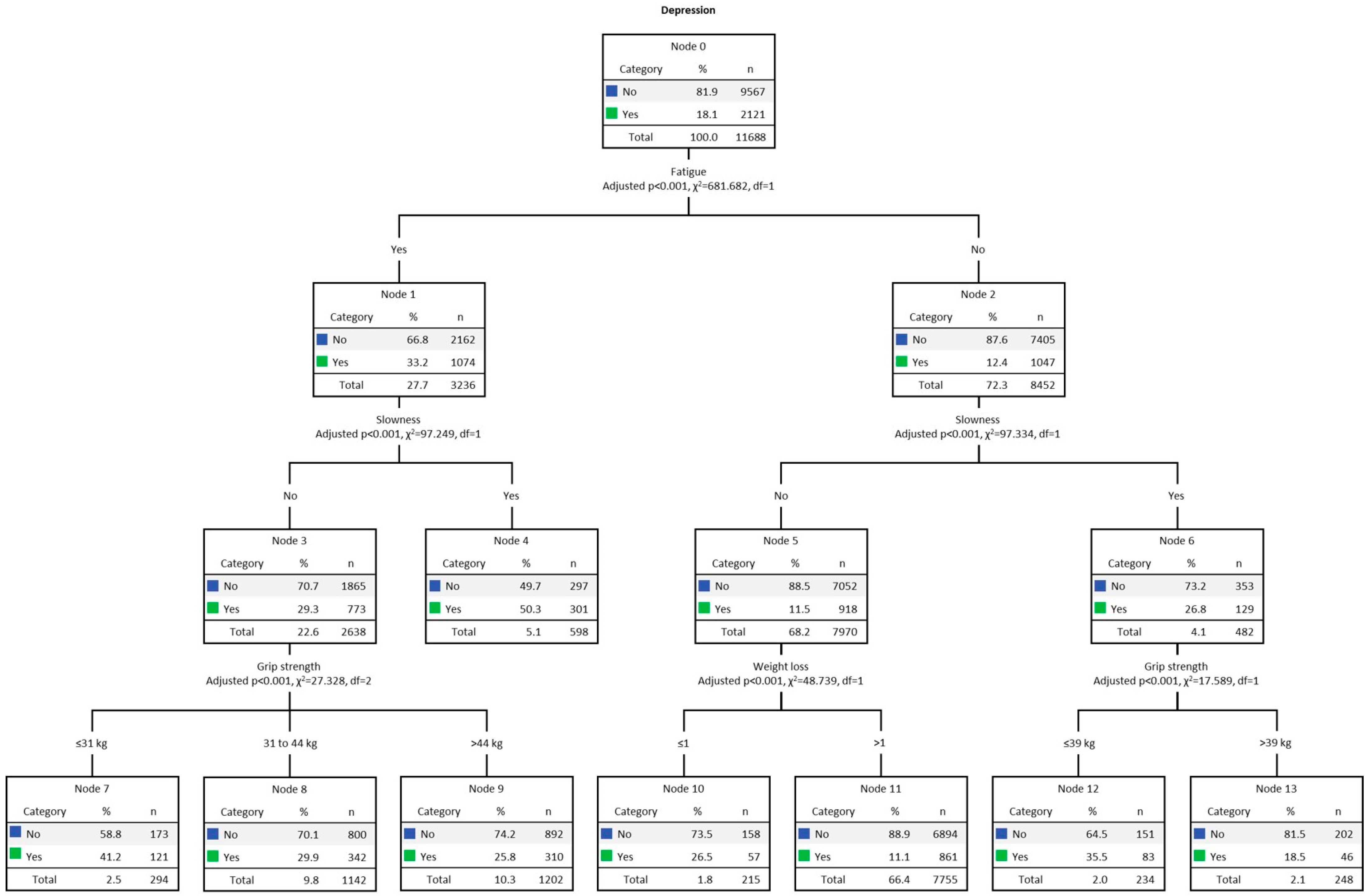
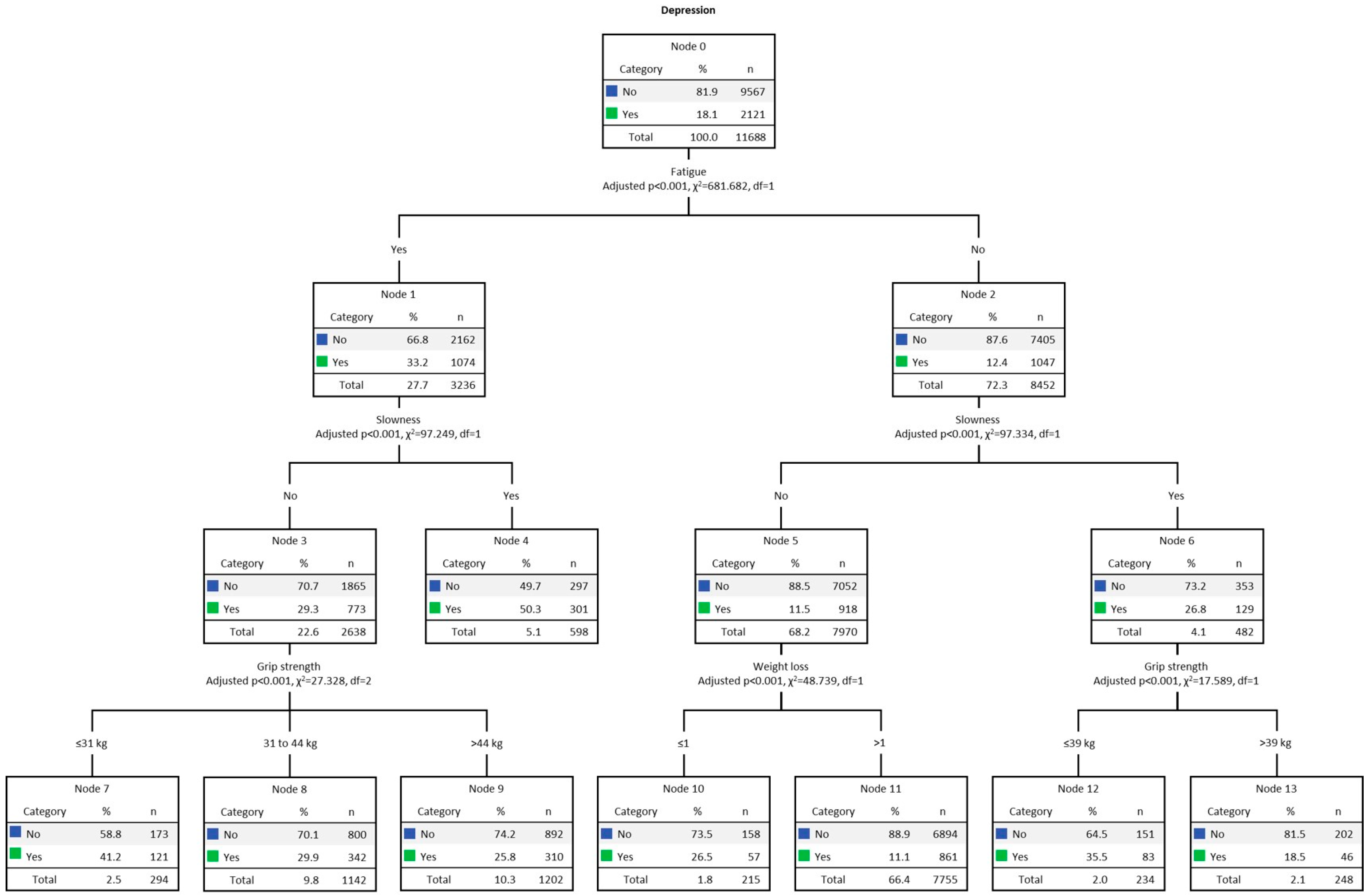
3.3. Results for Men
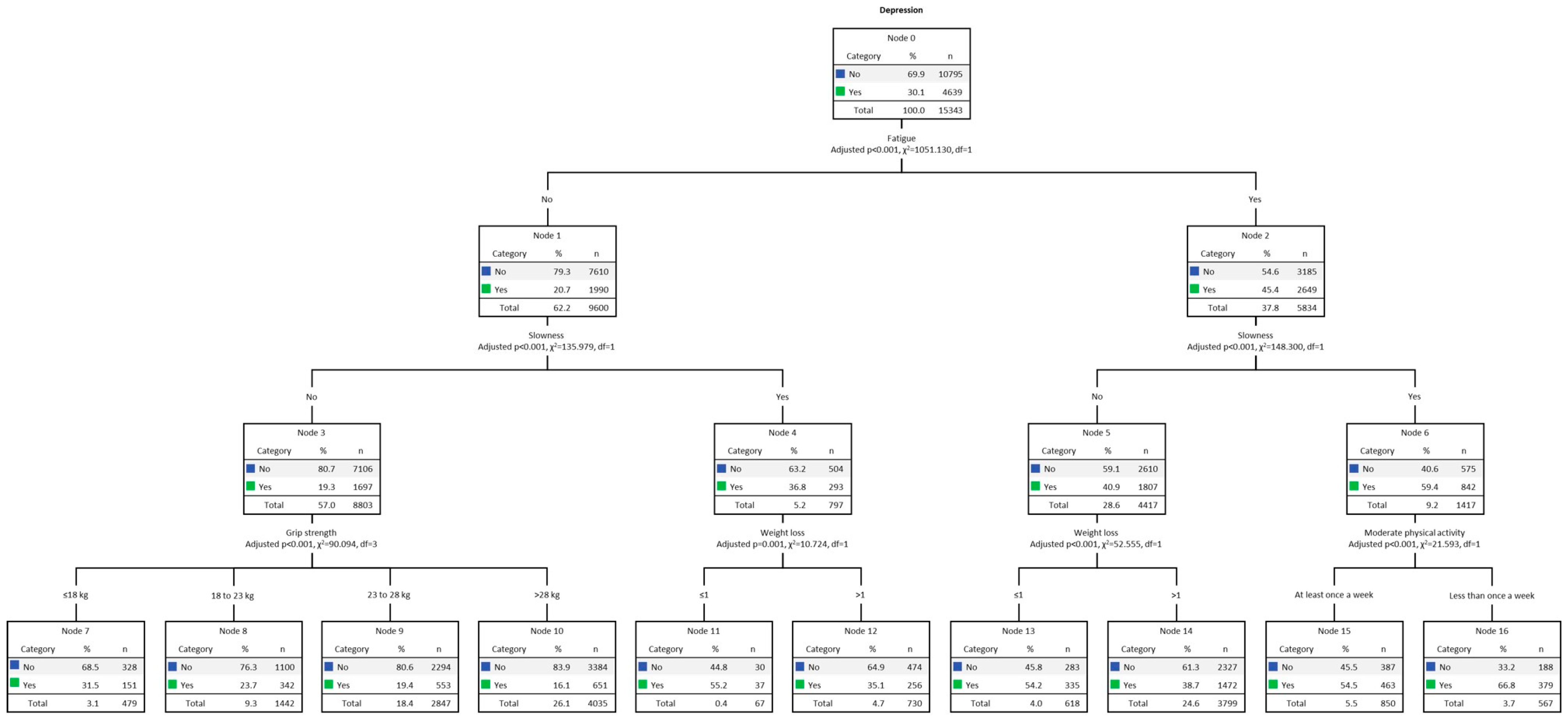
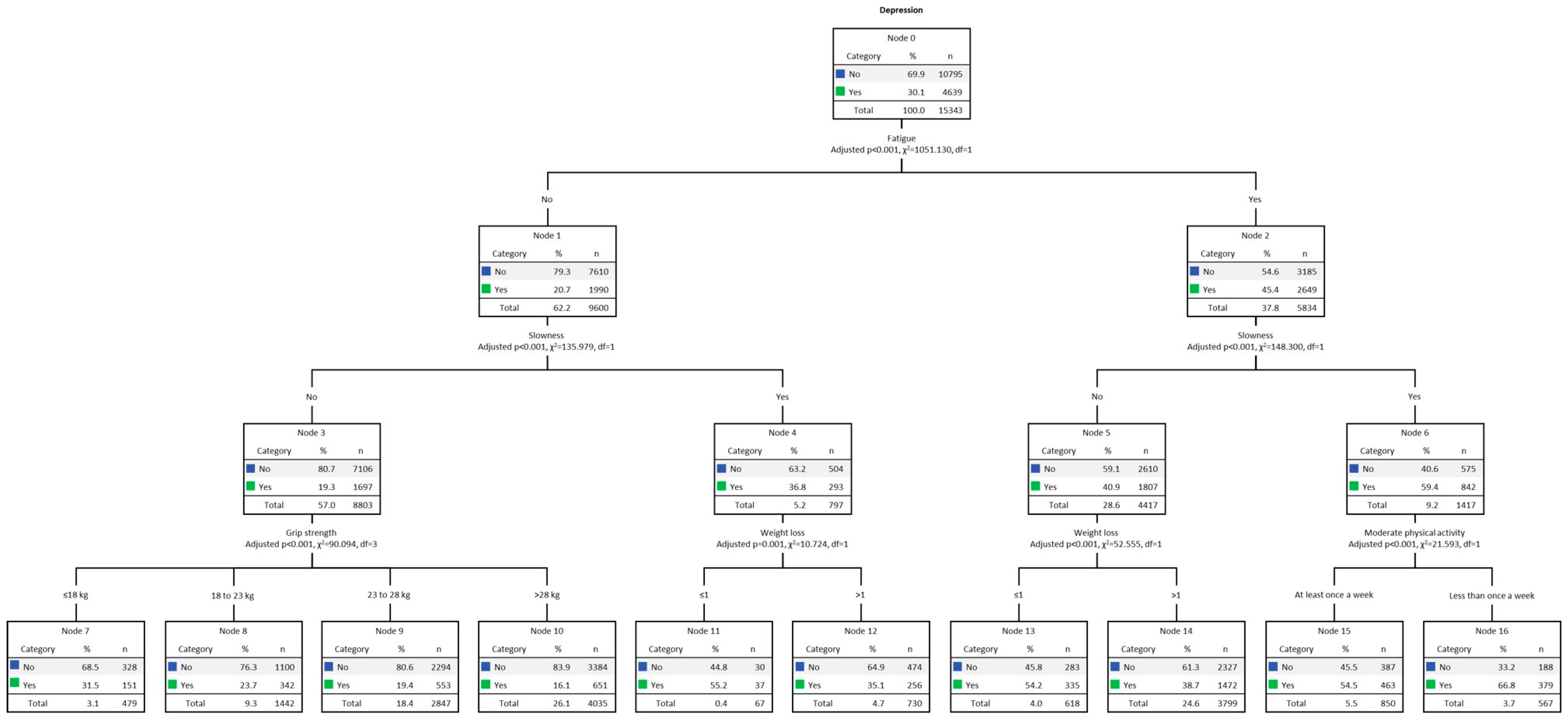
3.4. Results for Women
4. Discussion
Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bao, H.; Cao, J.; Chen, M.; Chen, M.; Chen, W.; Chen, X.; Chen, Y.; Chen, Y.; Chen, Y.; Chen, Z.; et al. Biomarkers of aging. Sci. China Life Sci. 2023, 66, 8931066. [Google Scholar]
- Hahr, J.Y. Physiology of aging. Med. Hypotheses 2019, 123, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Barter, J.D.; Foster, T.C. Aging in the Brain: New Roles of Epigenetics in Cognitive Decline. Neurosci. 2018, 24, 516–525. [Google Scholar] [CrossRef]
- Harridge, S.D.R.; Lazarus, N.R. Physical Activity, Aging, and Physiological Function. Physiology 2017, 32, 152–161. [Google Scholar] [CrossRef]
- Brown, P.J.; Ciarleglio, A.; Roose, S.P.; Montes Garcia, C.; Chung, S.; Fernandes, S.; Rutherford, B.R. Frailty and Depression in Late Life: A High-Risk Comorbidity With Distinctive Clinical Presentation and Poor Antidepressant Response. J. Gerontol. Ser. A 2022, 77, 1055–1062. [Google Scholar] [CrossRef]
- Vaughan, L.; Goveas, J.; Corbin, A. Depression and frailty in later life: A systematic review. Clin. Interv. Aging 2015, 10, 1947. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.J.; Roose, S.P.; Zhang, J.; Wall, M.; Rutherford, B.R.; Ayonayon, H.N.; Butters, M.A.; Harris, T.; Newman, A.B.; Satterfield, S.; et al. Inflammation, Depression, and Slow Gait: A High Mortality Phenotype in Later Life. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 221–227. [Google Scholar] [CrossRef]
- WHO-World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; WHO-World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Liu, Q.; He, H.; Yang, J.; Feng, X.; Zhao, F.; Lyu, J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J. Psychiatr. Res. 2020, 126, 134–140. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef]
- Buigues, C.; Padilla-Sánchez, C.; Garrido, J.F.; Navarro-Martínez, R.; Ruiz-Ros, V.; Cauli, O. The relationship between depression and frailty syndrome: A systematic review. Aging Ment. Health 2015, 19, 762–772. [Google Scholar] [CrossRef]
- Delli Zotti, G.B.; Citterio, L.; Farinone, S.; Concas, M.P.; Brioni, E.; Zagato, L.; Messaggio, E.; Faienza, S.; Simonini, M.; Napoli, A.; et al. Association between Perceived Health-Related Quality of Life and Depression with Frailty in the FRASNET Study. Int. J. Environ. Res. Public Health 2022, 19, 16776. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Cohen, A.A.; Xue, Q.-L.; Walston, J.; Bandeen-Roche, K.; Varadhan, R. The physical frailty syndrome as a transition from homeostatic symphony to cacophony. Nat. Aging 2021, 1, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Andrade-Gómez, E.; Martínez-Gómez, D.; Rodríguez-Artalejo, F.; García-Esquinas, E. Sedentary behaviors, physical activity, and changes in depression and psychological distress symptoms in older adults. Depress. Anxiety 2018, 35, 884–897. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Savva, G.M.; Kenny, R.; Lawlor, B.A. What predicts persistent depression in older adults across Europe? Utility of clinical and neuropsychological predictors from the SHARE study. J. Affect. Disord. 2013, 147, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Jürschik, P.; Nunin, C.; Botigué, T.; Escobar, M.A.; Lavedán, A.; Viladrosa, M. Prevalence of frailty and factors associated with frailty in the elderly population of Lleida, Spain: The FRALLE survey. Arch. Gerontol. Geriatr. 2012, 55, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Collard, R.M.; Comijs, H.C.; Naarding, P.; Penninx, B.W.; Milaneschi, Y.; Ferrucci, L.; Oude Voshaar, R.C. Frailty as a Predictor of the Incidence and Course of Depressed Mood. J. Am. Med. Dir. Assoc. 2015, 16, 509–514. [Google Scholar] [CrossRef]
- Marconcin, P.; Peralta, M.; Ferrari, G.; Gaspar de Matos, M.; Espanha, M.; Murawska-Ciałowicz, E.; Marques, A. The Association of Grip Strength with Depressive Symptoms among Middle-Aged and Older Adults with Different Chronic Diseases. Int. J. Environ. Res. Public Health 2020, 17, 6942. [Google Scholar] [CrossRef]
- Aichberger, M.C.; Schouler-Ocak, M.; Mundt, A.; Busch, M.A.; Nickels, E.; Heimann, H.M.; Ströhle, A.; Reischies, F.M.; Heinz, A.; Rapp, M.A. Depression in middle-aged and older first generation migrants in Europe: Results from the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. Psychiatry 2010, 25, 468–475. [Google Scholar] [CrossRef]
- Lindwall, M.; Larsman, P.; Hagger, M.S. The reciprocal relationship between physical activity and depression in older European adults: A prospective cross-lagged panel design using SHARE data. Health Psychol. 2011, 30, 453–462. [Google Scholar] [CrossRef]
- Braam, A.W.; Delespaul, P.; Beekman, A.T.F.; Deeg, D.J.H.; Pèrés, K.; Dewey, M.; Kivelä, S.-L.; Lawlor, B.A.; Magnússon, H.; Meller, I.; et al. National context of healthcare, economy and religion, and the association between disability and depressive symptoms in older Europeans: Results from the EURODEP concerted action. Eur. J. Ageing 2004, 1, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Sasaki, Y.; Son, B.-K.; Tanaka, T.; Lyu, W.; Tsuchiya-Ito, R.; Kitamura, S.; Dregan, A.; Hotopf, M.; Iwagami, M.; et al. Association of coexistence of frailty and depressive symptoms with mortality in community-dwelling older adults: Kashiwa Cohort Study. Arch. Gerontol. Geriatr. 2023, 119, 105322. [Google Scholar] [CrossRef] [PubMed]
- Girgus, J.S.; Yang, K. Gender and depression. Curr. Opin. Psychol. 2015, 4, 53–60. [Google Scholar] [CrossRef]
- Labaka, A.; Goñi-Balentziaga, O.; Lebeña, A.; Pérez-Tejada, J. Biological Sex Differences in Depression: A Systematic Review. Biol. Res. Nurs. 2018, 20, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Agostino, D.; Wu, Y.-T.; Daskalopoulou, C.; Hasan, M.T.; Huisman, M.; Prina, M. Global trends in the prevalence and incidence of depression:a systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 235–243. [Google Scholar] [CrossRef]
- Swetlitz, N. Depression’s Problem With Men. AMA J. Ethics 2021, 23, E586–E589. [Google Scholar] [PubMed]
- Park, C.; Ko, F.C. The Science of Frailty. Clin. Geriatr. Med. 2021, 37, 625–638. [Google Scholar] [CrossRef]
- Gordon, E.H.; Peel, N.M.; Samanta, M.; Theou, O.; Howlett, S.E.; Hubbard, R.E. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 2017, 89, 30–40. [Google Scholar] [CrossRef]
- Balaj, M.; McNamara, C.L.; Eikemo, T.A.; Bambra, C. The social determinants of inequalities in self-reported health in Europe: Findings from the European social survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27, 107–114. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Bristle, J.; Andersen-Ranberg, K.; Brugiavini, A.; Jusot, F.; Litwin, H.; Weber, G. Health and Socio-Economic Status over the Life Course; Börsch-Supan, A., Bristle, J., Andersen-Ranberg, K., Brugiavini, A., Jusot, F., Litwin, H., Weber, G., Eds.; De Gruyter: Berlin, Germany; Boston, MA, USA, 2019; ISBN 9783110617245. [Google Scholar]
- Kilner, J.M.; Lemon, R.N. What We Know Currently about Mirror Neurons. Curr. Biol. 2013, 23, R1057–R1062. [Google Scholar] [CrossRef]
- Bai, Z.; Xu, Z.; Xu, X.; Qin, X.; Hu, W.; Hu, Z. Association between social capital and depression among older people: Evidence from Anhui Province, China. BMC Public Health 2020, 20, 1560. [Google Scholar] [CrossRef]
- Battista, K.; Patte, K.A.; Diao, L.; Dubin, J.A.; Leatherdale, S.T. Using Decision Trees to Examine Environmental and Behavioural Factors Associated with Youth Anxiety, Depression, and Flourishing. Int. J. Environ. Res. Public Health 2022, 19, 10873. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Prince, M.J.; Reischies, F.; Beekman, A.T.; Fuhrer, R.; Jonker, C.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; Fichter, M.; et al. Development of the EURO-D scale—A European, Union initiative to compare symptoms of depression in 14 European centres. Br. J. Psychiatry 1999, 174, 330–338. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Walsh, C.D.; Lawlor, B.A.; Kenny, R.A. A Frailty Instrument for primary care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010, 10, 57. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.L. The International Standard Classification of Education 2011. In Comparative Social Research; Emerald Group Publishing Limited: Montreal, QC, USA, 2013; Volume 30, pp. 365–379. ISBN 9781781905371. [Google Scholar]
- WHO-World Health Organization. Overweight and Obesity; WHO-World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hansen, H.; Schäfer, I.; Schön, G.; Riedel-Heller, S.; Gensichen, J.; Weyerer, S.; Petersen, J.J.; König, H.-H.; Bickel, H.; Fuchs, A.; et al. Agreement between self-reported and general practitioner-reported chronic conditions among multimorbid patients in primary care—Results of the MultiCare Cohort Study. BMC Fam. Pract. 2014, 15, 39. [Google Scholar] [CrossRef] [PubMed]
- Loh, W.-Y. Fifty Years of Classification and Regression Trees. Int. Stat. Rev. 2014, 82, 329–348. [Google Scholar] [CrossRef]
- Akca, N.; Sönmez, S.; Yılmaz, A. Determinants of health expenditure in OECD countries: A decision tree model. Pakistan J. Med. Sci. 2017, 33, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Charbuty, B.; Abdulazeez, A. Classification Based on Decision Tree Algorithm for Machine Learning. J. Appl. Sci. Technol. Trends 2021, 2, 20–28. [Google Scholar] [CrossRef]
- Song, Y.Y.; Lu, Y. Decision tree methods: Applications for classification and prediction. Shanghai Arch. Psychiatry 2015, 27, 130–135. [Google Scholar]
- Strain, T.; Wijndaele, K.; Sharp, S.J.; Dempsey, P.C.; Wareham, N.; Brage, S. Impact of follow-up time and analytical approaches to account for reverse causality on the association between physical activity and health outcomes in UK Biobank. Int. J. Epidemiol. 2020, 49, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Marconcin, P.; Barak, S.; Ferrari, G.; Gouveia, É.R.; de Maio Nascimento, M.; Willig, R.; Varela, M.; Marques, A. Prevalence of Frailty and Its Association with Depressive Symptoms among European Older Adults from 17 Countries: A 5-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 14055. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.-M. The prediction model of suicidal thoughts in Korean adults using Decision Tree Analysis: A nationwide cross-sectional study. PLoS ONE 2019, 14, e0223220. [Google Scholar] [CrossRef]
- Daniya, T.; Geetha, M.; Suresh Kumar, K. Classification and regression trees with Gini Index. Adv. Math. Sci. J. 2020, 9, 8237–8247. [Google Scholar] [CrossRef]
- Avendano, M.; Mackenbach, J. Informe Share Health and Health Care. In Changes in Physical Health among Older Europeans; Borsch-Supan, A., Brugiavini, A., Jurges, H., Eds.; Health, Ageing and Retirement in Europe 2004–2007; Mannheim Research Institute for the Economics of Ageng: Mannheim, Germany, 2008; pp. 118–124. [Google Scholar]
- Shi, J.; Yang, Z.; Song, X.; Yu, P.; Fang, X.; Tang, Z.; Peng, D.; Mitnitski, A.; Rockwood, K. Sex Differences in the Limit to Deficit Accumulation in Late Middle-Aged and Older Chinese People: Results From the Beijing Longitudinal Study of Aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Ning, H.-T.; Du, Y.; Zhao, L.-J.; Tian, Q.; Feng, H.; Deng, H.-W. Racial and gender differences in the relationship between sarcopenia and bone mineral density among older adults. Osteoporos. Int. 2021, 32, 841–851. [Google Scholar] [CrossRef]
- Chang, E.; Varghese, M.; Singer, K. Gender and Sex Differences in Adipose Tissue. Curr. Diab. Rep. 2018, 18, 69. [Google Scholar] [CrossRef]
- Redondo-Sendino, Á.; Guallar-Castillón, P.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender differences in the utilization of health-care services among the older adult population of Spain. BMC Public Health 2006, 6, 155. [Google Scholar] [CrossRef]
- Okura, M.; Ogita, M.; Arai, H. Self-Reported Cognitive Frailty Predicts Adverse Health Outcomes for Community-Dwelling Older Adults Based on an Analysis of Sex and Age. J. Nutr. Health Aging 2019, 23, 654–664. [Google Scholar] [CrossRef]
- Mezuk, B.; Edwards, L.; Lohman, M.; Choi, M.; Lapane, K. Depression and frailty in later life: A synthetic review. Int. J. Geriatr. Psychiatry 2012, 27, 879–892. [Google Scholar] [CrossRef]
- Demichelis, O.P.; Grainger, S.A.; Hubbard, R.E.; Henry, J.D. Emotion regulation mediates the relationship between social frailty and stress, anxiety, and depression. Sci. Rep. 2023, 13, 6430. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, Y.; Sato, S.; Kitabatake, Y.; Nakamura, M.; Takeda, N.; Maruo, K.; Arao, T. Bidirectional relationship between insomnia and frailty in older adults: A 2-year longitudinal study. Arch. Gerontol. Geriatr. 2021, 97, 104519. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Bernardi, S.; Toffoli, B.; Tonon, F.; Francica, M.; Campagnolo, E.; Ferretti, T.; Comar, S.; Giudici, F.; Stenner, E.; Fabris, B. Sex Differences in Proatherogenic Cytokine Levels. Int. J. Mol. Sci. 2020, 21, 3861. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-H.; Giuliani, F. The Role of Inflammation in Depression and Fatigue. Front. Immunol. 2019, 10, 1696. [Google Scholar] [CrossRef] [PubMed]
- Köhler, O.; Krogh, J.; Mors, O.; Benros, M.E. Inflammation in Depression and the Potential for Anti-Inflammatory Treatment. Curr. Neuropharmacol. 2016, 14, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.; Passos, G.R.; Muhammed, L.; Everett, R.; Reeve, S.; Messina, S.; Probert, F.; Leite, M.I.; Palace, J. Factors associated with fatigue in CNS inflammatory diseases with AQP4 and MOG antibodies. Ann. Clin. Transl. Neurol. 2020, 7, 375–383. [Google Scholar] [CrossRef]
- Yuan, N.; Chen, Y.; Xia, Y.; Dai, J.; Liu, C. Inflammation-related biomarkers in major psychiatric disorders: A cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl. Psychiatry 2019, 9, 233. [Google Scholar] [CrossRef]
- Das, A. Psychosocial distress and inflammation: Which way does causality flow? Soc. Sci. Med. 2016, 170, 1–8. [Google Scholar] [CrossRef]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Marconcin, P.; Rúbio Gouveia, É.; de Maio Nascimento, M.; Ferrari, G.; Marques, A. Mental Health Conditions and Exercise. In Mental Health—Preventive Strategies [Working Title]; IntechOpen: London, UK, 2023. [Google Scholar]
- Haider, S.; Grabovac, I.; Dorner, T.E. Effects of physical activity interventions in frail and prefrail community-dwelling people on frailty status, muscle strength, physical performance and muscle mass—A narrative review. Wien. Klin. Wochenschr. 2019, 131, 244–254. [Google Scholar] [CrossRef]
- Zhang, S.; Xiang, K.; Li, S.; Pan, H.-F. Physical activity and depression in older adults: The knowns and unknowns. Psychiatry Res. 2021, 297, 113738. [Google Scholar] [CrossRef] [PubMed]
- Coll-Planas, L.; Blancafort Alias, S.; Tully, M.; Caserotti, P.; Giné-Garriga, M.; Blackburn, N.; Skjødt, M.; Wirth, K.; Deidda, M.; McIntosh, E.; et al. Exercise referral schemes enhanced by self-management strategies to reduce sedentary behaviour and increase physical activity among community-dwelling older adults from four European countries: Protocol for the process evaluation of the SITLESS randomised. BMJ Open 2019, 9, e027073. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Biddle, S.J.H.; Buman, M.P.; Chastin, S.; Ekelund, U.; Friedenreich, C.M.; Katzmarzyk, P.T.; Leitzmann, M.F.; Stamatakis, E.; van der Ploeg, H.P.; et al. New global guidelines on sedentary behaviour and health for adults: Broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.S.; Sherrington, C.; Paul, S.S.; Ramsay, E.; Chamberlain, K.; Kirkham, C.; O’Rourke, S.D.; Hassett, L.; Tiedemann, A. A combined physical activity and fall prevention intervention improved mobility-related goal attainment but not physical activity in older adults: A randomised trial. J. Physiother. 2019, 65, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Groessl, E.J.; Kaplan, R.M.; Rejeski, W.J.; Katula, J.A.; Glynn, N.W.; King, A.C.; Anton, S.D.; Walkup, M.; Lu, C.; Reid, K.; et al. Physical Activity and Performance Impact Long-term Quality of Life in Older Adults at Risk for Major Mobility Disability. Am. J. Prev. Med. 2019, 56, 141–146. [Google Scholar] [CrossRef]
- Marques, A.; Gaspar de Matos, M.; Bordado, J.; Gouveia, É.R.; Peralta, M.; Gomez-Baya, D. Different levels of physical activity and depression symptoms among older adults from 18 countries: A population-based study from the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. J. Sport Sci. 2021, 21, 887–894. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Rathnayake, N.; Alwis, G.; Lenora, J.; Lekamwasam, S. Factors associated with measures of sarcopenia in pre and postmenopausal women. BMC Womens. Health 2021, 21, 5. [Google Scholar] [CrossRef]
- Cooper, A.J.M.; Lamb, M.J.E.; Sharp, S.J.; Simmons, R.K.; Griffin, S.J. Bidirectional association between physical activity and muscular strength in older adults: Results from the UK Biobank study. Int. J. Epidemiol. 2016, 46, dyw054. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depression: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Zhang, Z.; Chen, W. A Systematic Review of the Relationship Between Physical Activity and Happiness. J. Happiness Stud. 2019, 20, 1305–1322. [Google Scholar] [CrossRef]
- Renner, S.W.; Qiao, Y.; Gmelin, T.; Santanasto, A.J.; Boudreau, R.M.; Walston, J.D.; Perls, T.T.; Christensen, K.; Newman, A.B.; Glynn, N.W. Association of fatigue, inflammation, and physical activity on gait speed: The Long Life Family Study. Aging Clin. Exp. Res. 2022, 34, 367–374. [Google Scholar] [CrossRef]
- Brach, M.; de Bruin, E.D.; Levin, O.; Hinrichs, T.; Zijlstra, W.; Netz, Y. Evidence-based yet still challenging! Research on physical activity in old age. Eur. Rev. Aging Phys. Act. 2023, 20, 7. [Google Scholar] [CrossRef]
- Howlett, S.E.; Rutenberg, A.D.; Rockwood, K. The degree of frailty as a translational measure of health in aging. Nat. Aging 2021, 1, 651–665. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Total (n = 27,122) | Men (n = 11,688) | Women (n = 15,434) | p-Value |
|---|---|---|---|---|
| Age (years) | <0.001 * | |||
| Total (mean ± SD) | 66.78 ± 8.86 | 67.03 ± 8.66 | 66.58 ± 9.00 | |
| 50–59 n (%) | 6333 (23.3) | 2536 (21.7) | 3797 (24.6) | |
| 60–69 n (%) | 10,792 (39.8) | 4757 (40.7) | 6035 (39.1) | |
| 70–79 n (%) | 7524 (27.8) | 3342 (28.6) | 4182 (27.1) | |
| 80–89 n (%) | 2332 (8.6) | 1005 (8.6) | 1327 (8.6) | |
| 90–99 n (%) | 138 (0.5) | 46 (0.4) | 92 (0.6) | |
| Education n (%) | <0.001 † | |||
| ISCED 0–1 | 7133 (26.3) | 2641 (22.6) | 4491 (29.1) | |
| ISCED 2–4 | 13,968 (51.5) | 6078 (52.0) | 7887 (51.1) | |
| ISCED 5–6 | 6021 (22.2) | 2969 (25.4) | 3056 (19.8) | |
| BMI | <0.001 * | |||
| Total (mean ± SD) | 27.12 ± 4.57 | 27.43 ± 4.04 | 26.88 ± 4.92 | |
| Underweight n (%) | 219 (0.8) | 28 (0.2) | 191 (1.2) | |
| Normal n (%) | 9462 (34.8) | 3320 (28.4) | 6142 (39.8) | |
| Overweight n (%) | 11,372 (41.9) | 5782 (49.5) | 5590 (36.2) | |
| Obese n (%) | 6069 (22.4) | 2558 (21.9) | 3511 (22.7) | |
| Living with partner | <0.001 † | |||
| Yes n (%) | 19,998 (73.7) | 9750 (83.4) | 10,248 (66.4) | |
| No n (%) | 7124 (26.3) | 1938 (16.6) | 5186 (33.6) | |
| Chronic disease n (%) | <0.001 † | |||
| 0 | 6636 (24.5) | 3053 (26.1) | 3582 (23.2) | |
| 1–3 | 17,370 (64.0) | 7503 (64.2) | 9867 (63.9) | |
| 4–6 | 2926 (10.8) | 1070 (9.2) | 1856 (12.0) | |
| 7–9 | 182 (0.6) | 58 (0.4) | 124 (0.7) | |
| 10–14 | 8 (0.1) | 4 (0.1) | 4 (0.1) | |
| Disability n (%) | 0.432 † | |||
| Yes n (%) | 2468 (9.1) | 1075 (9.2) | 1404 (9.1) | |
| No n (%) | 24,654 (90.9) | 10,613 (90.8) | 14,030 (90.9) | |
| DEP | <0.001 † | |||
| Total (mean ± SD) | 2.22 ± 2.10 | 1.75 ± 1.84 | 2.57 ± 2.20 | |
| No depressed n (%) | 20,745 (76.5) | 9835 (84.1) | 10,958 (70.9) | |
| Depressed n (%) | 6282 (23.2) | 1806 (15.5) | 4476 (29.0) | |
| Frailty | <0.001 † | |||
| Non-frail n (%) | 21,899 (80.7) | 10,455 (89.4) | 11,444 (67.6) | |
| Pre-frail n (%) | 3923 (14.5) | 1044 (8.9) | 2879 (21.6) | |
| Frail n (%) | 1300 (4.8) | 189 (1.6) | 1111 (10.8) | |
| Fatigue | <0.001 † | |||
| Yes n (%) | 9070 (33.4) | 3236 (27.7) | 5834 (37.8) | |
| No n (%) | 18,052 (66.6) | 8452 (72.3) | 9600 (62.2) | |
| Weight loss | <0.001 † | |||
| Yes n (%) | 1951 (7.2) | 618 (5.3) | 1333 (8.6) | |
| No n (%) | 25,171 (92.8) | 11,070 (94.7) | 14,101 (91.4) | |
| Slowness | <0.001 † | |||
| Yes n (%) | 3294 (12.1) | 1080 (9.2) | 2214 (14.3) | |
| No n (%) | 23,828 (87.9) | 10,608 (90.8) | 13,220 (85.7) | |
| MPA | <0.001 * | |||
| Total (mean ± SD) | 2.62 ± 11.54 | 2.65 ± 0.66 | 2.60 ± 0.70 | |
| <Once week n (%) | 3277 (12.1) | 1274 (10.9) | 2004 (13.0) | |
| Once week n (%) | 3642 (13.4) | 1540 (13.2) | 2102 (13.6) | |
| >Once week n (%) | 20,203 (74.5) | 8875 (75.9) | 11,328 (73.4) | |
| Grip strength (kg) | ||||
| Total (mean ± SD) | 34.26 ± 11.19 | 43.93 ± 9.44 | 26.94 ± 6.49 | <0.001 * |
| Variable | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|
| Men | ||||
| Slowness | 0.470 (0.405, 0.545) | <0.001 | 0.552 (0.478, 0.649) | <0.001 |
| Weight loss | 0.558 (0.472, 0.678) | <0.001 | 0.582 (0.488, 0.702) | <0.001 |
| Fatigue | 0.346 (0.315, 0.387) | <0.001 | 0.369 (0.335, 0.413) | <0.001 |
| MPA | −0.910 (0.852, 0.983) | <0.001 | −0.901 (0.844, 0.976) | <0.001 |
| Grip strength | −0.978 (0.975, 0.985) | <0.001 | −0.984 (0.982, 0.994) | <0.001 |
| Women | ||||
| Slowness | 0.562 (0.513, 0.632) | <0.001 | 0.690 (0.626, 0.779) | <0.001 |
| Weight loss | 0.578 (0.516, 0.661) | <0.001 | 0.588 (0.528, 0.678) | <0.001 |
| Fatigue | 0.391 (0.363, 0.422) | <0.001 | 0.421 (0.395, 0.461) | <0.001 |
| MPA | −0.860 (0.822, 0.913) | <0.001 | −0.872 (0.833, 0.926) | <0.001 |
| Grip strength | −0.970 (0.965, 0.976) | <0.001 | −0.970 (0.973, 0.985) | <0.001 |
| Node | Node | Gain | Response | Index | ||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| 4 | 598 | 5.1% | 301 | 14.2% | 50.3% | 277.4% |
| 7 | 294 | 2.5% | 121 | 5.7% | 41.2% | 226.8% |
| 12 | 234 | 2.0% | 83 | 3.9% | 35.5% | 195.5% |
| 8 | 1142 | 9.8% | 342 | 16.1% | 29.9% | 165.0% |
| 10 | 215 | 1.8% | 57 | 2.7% | 26.5% | 146.1% |
| 9 | 1202 | 10.3% | 310 | 14.6% | 25.8% | 142.1% |
| 13 | 248 | 2.1% | 46 | 2.2% | 18.5% | 102.2% |
| 11 | 7755 | 66.4% | 861 | 40.6% | 11.1% | 61.2% |
| Node | Node | Gain | Response | Index | ||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| 16 | 567 | 3.7% | 379 | 8.2% | 66.8% | 222.4% |
| 11 | 67 | 0.4% | 37 | 0.8% | 55.2% | 183.7% |
| 15 | 850 | 5.5% | 463 | 10.0% | 54.5% | 181.2% |
| 13 | 618 | 4.0% | 335 | 7.2% | 54.2% | 180.3% |
| 14 | 3799 | 24.6% | 1472 | 31.7% | 38.7% | 128.9% |
| 12 | 730 | 4.7% | 256 | 5.5% | 35.1% | 116.7% |
| 7 | 479 | 3.1% | 151 | 3.3% | 31.5% | 104.9% |
| 8 | 1442 | 9.3% | 342 | 7.4% | 23.7% | 78.9% |
| 9 | 2847 | 18.4% | 553 | 11.9% | 14.9% | 64.6% |
| 10 | 4035 | 26.1% | 651 | 14.0% | 16.1% | 53.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, M.d.M.; Marques, A.; Gouveia, É.R.; Marconcin, P.; Peralta, M.; Ihle, A. The Longitudinal Association between Multiple Frailty Criteria and Depressive Symptomatology Five Years Later in Older Adults: A Decision Tree Modelling Approach. J. Clin. Med. 2024, 13, 1697. https://doi.org/10.3390/jcm13061697
Nascimento MdM, Marques A, Gouveia ÉR, Marconcin P, Peralta M, Ihle A. The Longitudinal Association between Multiple Frailty Criteria and Depressive Symptomatology Five Years Later in Older Adults: A Decision Tree Modelling Approach. Journal of Clinical Medicine. 2024; 13(6):1697. https://doi.org/10.3390/jcm13061697
Chicago/Turabian StyleNascimento, Marcelo de Maio, Adilson Marques, Élvio R. Gouveia, Priscila Marconcin, Miguel Peralta, and Andreas Ihle. 2024. "The Longitudinal Association between Multiple Frailty Criteria and Depressive Symptomatology Five Years Later in Older Adults: A Decision Tree Modelling Approach" Journal of Clinical Medicine 13, no. 6: 1697. https://doi.org/10.3390/jcm13061697
APA StyleNascimento, M. d. M., Marques, A., Gouveia, É. R., Marconcin, P., Peralta, M., & Ihle, A. (2024). The Longitudinal Association between Multiple Frailty Criteria and Depressive Symptomatology Five Years Later in Older Adults: A Decision Tree Modelling Approach. Journal of Clinical Medicine, 13(6), 1697. https://doi.org/10.3390/jcm13061697