Abstract
Background: Previous research has established good test–retest reliability for isokinetic dynamometry in fibromyalgia. However, the reliability of this test under dual-task conditions has not been investigated in fibromyalgia. Methods: A total of 10 women with fibromyalgia participated in this study. Participants completed the concentric/concentric test. The dual-task condition involved subtracting two by two while performing the test. Results: Reliability analysis under the single condition showed “poor” to “excellent” values for maximum peak torque in knee extension and “moderate” to “excellent” values for average. “Poor” to “excellent” reliability values were found in knee flexion for the maximum and average. Dual-task condition in knee extension ranged from “moderate” to “excellent” for maximum and average values, and in knee flexion, it ranged from “poor” to “excellent” for maximum value and from “moderate” to “excellent” for average value. Conclusions: Isokinetic dynamometry demonstrated sufficient reliability for measuring strength in knee extension maximum and average during single-task and dual-task conditions, along with knee flexion dual-task average in fibromyalgia. For knee flexion single-task maximum and average and knee flexion dual-task maximum, we did not obtain sufficiently reliable measurements. Only the concentric/concentric test has been studied, and future studies with a larger sample size are needed in order to generalize the results.
1. Introduction
Fibromyalgia (FM) affects 0.2–6.6% of the general population and predominantly women over 50 years [1]. Individuals with FM, in addition to experiencing widespread chronic pain, may endure other symptoms such as muscle stiffness, persistent fatigue, disrupted sleep patterns, and an increased susceptibility to mood disorders, such as anxiety and depression [2]. This symptomatology can result in both cognitive impairment [3,4] and physical limitations [5,6,7]. Regarding physical limitations, there is generally a reduction in muscle strength in both the upper and lower limbs [8]. In the lower limbs, people with FM exhibit lower muscle strength, fatigue resistance, and static endurance [6,9,10,11,12]. Specifically, muscle strength in the quadriceps is diminished, probably due to reduced muscle mass [13,14] or reduced muscle strength per cross-sectional area [15,16]. Therefore, muscle function is globally impaired in FM people [6], as is their overall functionality [12]. In this context, peak torque of the lower limbs has been studied in individuals with FM, along with its potential association with the risk of falls [17].
As a result of their symptoms, FM people often experience a decline in their quality of life [18], partly due to the challenges they face in performing their activities of daily living [19]. It is rare to perform a task simultaneously every day. Instead, daily living activities often involve performing two tasks simultaneously, such as walking and talking or climbing stairs while thinking about something, a concept known as dual-task (DT) [20,21]. When attention is distributed between two simultaneous activities, a decrease in performance on both tasks may be experienced, in contrast to when they are performed individually [22], and healthy nervous systems have been shown to have limitations in information processing, which affects the ability to multitask [23]. In individuals with neurodegenerative diseases, these limitations may manifest themselves more markedly and significantly affect the performance of their daily tasks [24]. The relative change in performance associated with dual-task performance is known as dual-task interference, and it has been shown that individuals with neurological deficits may be particularly susceptible to this interference, as increased attentional demands to control motor performance reduce the availability of attentional resources to perform simultaneous secondary tasks [24]. In this way, it has been noted that individuals with FM exhibit more significant interference when performing two tasks simultaneously compared to healthy individuals, consequently affecting their performance in one or both tasks [25,26,27,28,29].
Several studies have already focused on assessing the reliability of various tests and measures under DT conditions [30,31,32]. This is crucial, since evaluating these activities taking into account not only physical demands but also cognitive factors such as attention and executive functions makes them more representative of real-life demands [20,21,33]. In this context, reliable tests to assess muscle strength are fundamental. Reliability refers to the consistency of the results when the same methodology is applied under similar conditions [34]. One of the reliable methods for measuring lower limb muscle strength in FM is isokinetic dynamometry [35], which is one of the most commonly employed tools in this context [6,8,9,11,12,14,15,16,36,37,38]. This method enables the measurement of dynamic muscle strength through electromechanical devices that maintain a constant velocity of movement while keeping the resistance consistent throughout the range of motion [39,40].
To the best of our knowledge, no previous study has evaluated the reliability of this test in FM people during DT conditions. Therefore, the present study aimed to analyze the test–retest reliability of the maximum (Max) and average (Avg) peak torque knee flexion and extension under single-task (ST) and DT conditions. Thus, we hypothesized that good test–retest reliability would be achieved in isokinetic dynamometry, both in ST and DT conditions, in line with findings from previous studies [35].
2. Materials and Methods
2.1. Participants
A sample size of 10 Caucasian women with FM from Caceres (Spain) with two observations per subject achieved 81% power to detect an intraclass correlation of 0.95 under the alternative hypothesis when the intraclass correlation under the null hypothesis is 0.75 using an F-test with a significance level of 0.05. The convenience sample was recruited from a local association to participate in this test–retest study. The PASS software (version 11.0; PASS; Kaysville, UH, USA) was employed to calculate the power and the sample size.
The inclusion criteria were set as follows: (a) women aged 30–75 years; (b) capable of effective communication with the research staff; (c) having read, comprehended, and signed the informed consent form; (d) confirmed diagnosis of fibromyalgia by a rheumatologist according to the American College of Rheumatology criteria [41].
The exclusion criteria were: (a) presence of psychiatric or neurological disorders; (b) receiving pharmacological treatment for depression or anxiety; (c) abuse or dependency on substances; (d) inability to engage in physical exertion due to contraindications; (e) injury to the leg affecting the flexion and extension of the knee; and (f) pregnancy status.
The present study was approved by the Research Ethics Committee of the University of Extremadura (approval reference: 192/2021). All participants were informed about the procedures and gave their written informed consent following the updated Declaration of Helsinki.
2.2. Instruments and Procedure
Participants were asked about years with FM, their level of education—primary education or elementary school graduate, professional training or secondary education, university studies—and the Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR) was administered [42]. This questionnaire is validated for people with FM and consists of 21 items, with a maximum score of 100 indicating the worst outcomes [43]. In addition, the Spanish version of the International Physical Activity Questionnaire (IPAQ) was used to assess physical activity and inactivity in this study, reporting the physical activity classification based on the different activities developed at work, for getting around, during leisure time, and for household tasks [44]. The Montreal Cognitive Assessment (MoCA) was also employed. MoCA is a concise cognitive screening tool that assesses various cognitive abilities, including attention, concentration, executive functions, memory, language, visual-constructional skills, calculation, and orientation [45]. MoCA has been found to be more sensitive than MMSE in individuals with FM [46]. Furthermore, a cut-off score of 23 out of 30 has been established to enhance diagnostic accuracy, effectively reducing the false positive rate [47]. Finally, age and anthropometric measurements were acquired using a Tanita Body Composition Analyzer BC-418 MA (Tanita Corp., Tokyo, Japan) and a stadiometer SECA 769 column scale (SECA Corp, Hanover, MD, USA).
In line with previous research addressing the reliability of isokinetic parameters in FM, the same procedure was performed on two different occasions, specifically on days 1 and 2, with an interval of 7 days between them [35]. The testing exclusively involved the dominant leg, and the evaluation of the weight of the limb and gravity adjustments were conducted using dynamometric software.
The test was performed using the isokinetic dynamometer (Multi-Joint 3, Biodex Medical Systems, Inc., Shirley, NY, USA). The test consists of the consecutive performance of five concentric actions, specifically for knee flexion and extension, constituting the concentric/concentric test [39,48]. These actions are carried out without interruption at a velocity of 60°/s within a range of motion from 0 to 90 degrees, where 0 degrees corresponds to full extension and 90 degrees represents flexion [48]. The setup and positioning instructions for knee extension/flexion provided by the manufacturer were followed. Each participant was attached to the dynamometer seat, aligning their knee axis with the dynamometer’s axis. The dynamometer was kept untilted at 0°, with the seat and isokinetic dynamometer positioned at 90° and the seatback tilt set at 85°. The dynamometer software was used to assess the weight of the leg being tested. In addition, to ensure the consistency of the measurements, a calibration of the system was performed before starting the test, following the indications provided in the application/operation manual provided by the manufacturer.
The testing protocol includes several steps: First, a general warm-up comprising 10 squats without load was performed. Following the general warm-up, participants engaged in a familiarization phase or specific warm-up, during which they completed 10 consecutive knee flexion and extension repetitions at a speed of 120°/s. There was a 1 min rest period before starting the final test.
During the DT conditions, participants simultaneously performed the concentric/concentric test described above and, at the same time, a cognitive task. Specifically, the cognitive task required participants to subtract numbers two by two from a value greater than 100, which was chosen at random, being odd or even [30].
2.3. Statistical Analysis
Statistical analysis was conducted using the Statistical Package for the Social Sciences software (SPSS, version 24.0; IBM Corp., Armonk, NY, USA) to analyze the data. The mean and standard deviation of each variable were calculated to characterize the sample, and the Max and Avg peak torques in knee extension and flexion were calculated for the test and retest. The 3.1 (two-way mixed effects, single rater/measurement) model was used to estimate the intraclass correlation coefficient (ICC) and the 95% confidence intervals of the peak torque knee extension and flexion under single and dual-task conditions, following the recommendations provided by Weir [49] and Koo [50]. The ICC classification was interpreted according to the guidelines proposed by Koo [50], where ICC values lower than 0.50 indicate “poor” reliability, values between 0.50 and 0.75 indicate “moderate” reliability, values between 0.75 and 0.90 indicate “good” reliability, and values higher than 0.90 indicate “excellent” reliability.
The absolute reliability was extracted by calculating the standard error of measurements (SEM) using the following formula:
where SD is the mean SD of the 5 repetitions in the test and retest for the average peak torque or the mean SD of the highest repetition in the test and retest for the Max peak torque.
To demonstrate if the change score in individual performance represents real and reliable change, the smallest real difference (SRD) was obtained using the following formula:
Both SEM and SRD were converted into percentages. The results of these percentages were calculated according to the following formula, , where the mean is the average of the test and retest.
To identify the level of agreement between the test and retest, Bland–Altman plots were performed for Max peak torque and Avg peak torque under single and dual-task conditions [51].
Moreover, to understand whether there was a relationship between test performance, the impact of the FM, and years of FM symptomatology, Spearman’s Rho correlation analysis was performed between the peak and average value of the test in single and dual-task conditions and the FIQR values and years of FM symptomatology. The statistical significance was set at the p ≤ 0.05 level.
3. Results
The main characteristics of the women are shown in Table 1. The results showed that the participants had an age of 48.50 (7.79), ranging from 36 to 62 years, indicating a moderate severity impact of the disease [52]. They suffered 12.44 (6.37) years of the disease since diagnosis and did not exhibit cognitive impairment [47]. Regarding their educational level, 4 participants completed primary or elementary school, 4 had professional training or secondary education, and 2 had university studies. Moreover, eight women were identified as being moderately physically active, one woman as being intensely physically active, and one woman as being low in physical activity, according to the values reported in the IPAQ questionnaire. Regarding medication intake, 10 individuals were taking NSAIDs, and 2 were taking opioids.

Table 1.
Descriptive characteristics of the participants.
The descriptive data of the test and retest for the Max peak torque and the Avg peak torque of the five repetitions of knee extension and flexion under single and DT conditions are shown in Table 2. First, reliability analysis showed that the women with FM reported under the single condition “poor” to “excellent” reliability values for Max peak torque in knee extension and “moderate” to “excellent” reliability values for Avg peak torque. However, “poor” to “excellent” reliability values were found in knee flexion for the Max and Avg peak torque. Secondly, reliability values for the dual-task condition in knee extension ranged from “moderate” to “excellent” for Max and Avg values, and in knee flexion ranged from “poor” to “excellent” for Max value and from “moderate” to “excellent” for Avg value. Finally, SEM and SRD values were also reported (see Table 2).
Table 2.
Maximum and average peak torque reliability under single and dual-task conditions.
To obtain a more comprehensive analysis, the level of agreement for the test and retest under single and DT conditions was analyzed through the Bland–Altman plots depicted in Figure 1.
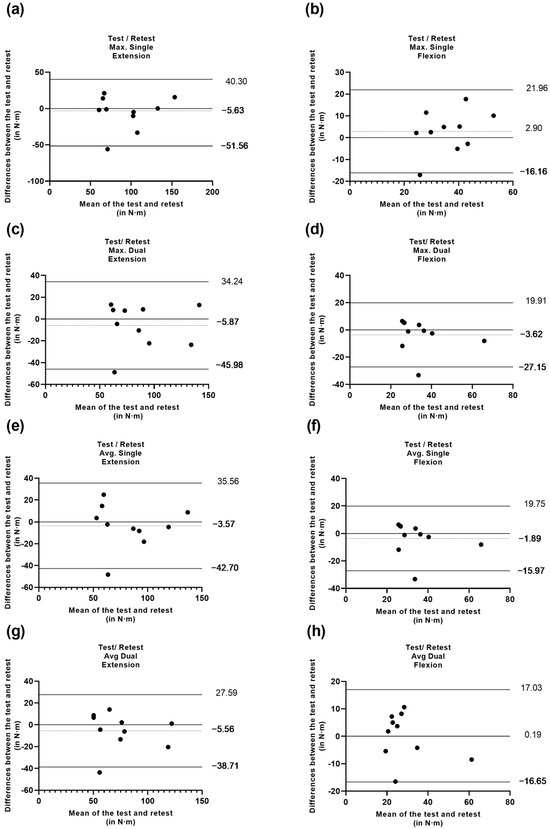
Figure 1.
(a) differences between test and retest vs. the mean of the two measurements of peak torque maximum in extension under the single condition; (b) differences between test and retest vs. the mean of the two measurements of peak torque maximum in flexion under the single condition; (c) differences between test and retest vs. the mean of the two measurements of peak torque maximum in extension under the dual-task condition; (d) differences between test and retest vs. the mean of the two measurements of peak torque maximum in flexion under the dual-task condition; (e) differences between test and retest vs. the mean of the two measurements of peak torque average in extension under the single condition; (f) differences between test and retest vs. the mean of the two measurements of peak torque average in flexion under the single condition; (g) differences between test and retest vs. the mean of the two measurements of peak torque average in extension under the dual-task condition; (h) differences between test and retest vs. the mean of the two measurements of peak torque average in flexion under the dual-task condition.
Finally, the correlation analysis between the performance obtained in the test through the peak and average values in flexion and extension in single and dual-task conditions was not significantly related to the impact of the disease nor the years of FM symptomatology (see Supplementary Material Table S1). All values showed a p-value > 0.05.
4. Discussion
The main objective of this study was to establish the test–retest reliability of isokinetic dynamometry during DT conditions in FM people. To our knowledge, no previous study has reported the reliability of isokinetic knee measurements in FM patients under DT conditions. The findings support the application of DT conditions as a reliable tool for assessing physical fitness in real-life conditions. However, some measures did not yield values that were sufficiently high (>0.8) [53], and confidence intervals exhibited significant variability in the majority of cases. The ICC values for peak torque measurements in the present study indicate that the reliability of the isokinetic dynamometry, under DT conditions in both knee flexion and extension, ranged from “moderate” to “good” for maximum and average values. In particular, the test could be considered sufficiently reliable for measuring strength in knee extension maximum and average during both ST and DT conditions, as well as knee flexion DT average. However, for the other measurements—specifically, knee flexion ST maximum and average and knee flexion DT maximum—we did not obtain sufficiently reliable measurements.
By analyzing the data obtained in the DT condition to show the variability of the results in the isokinetic test due to measurement error, our study reported percentages to quantify the accuracy of the scores. In this sense, there was a 12.37 and 11.64% probability (with a 95% confidence interval) that a repeated measurement in the isokinetic dynamometry test would show a difference of 10.78 N·m and 8.71 N·m from the initial knee extension score for the maximum and average values, respectively. Similarly, there was a 19.35 and 15.70% probability that a repeated measure in the isokinetic dynamometry test showed a difference of 6.64 N·m and 4.49 N·m in knee flexion score for the maximum and average values, respectively. Considering that the SEM provides a range of scores in which the actual score of a specific test is expected to lie, achieving the lowest possible SEM values is crucial to ensuring higher reliability [53].
In terms of the minimum amount of change that must be observed in a score for it to be considered a real or significant change beyond measurement error, our study also reported the %SRD. In this line, in the scores obtained in the DT condition, the %SRD ranged between 34.28 and 53.65% in its maximum values for extension and flexion, respectively, and between 32.27 and 43.52% in its average values for extension and flexion. The SRD results suggest that improvements greater than 29.87 N·m at peak and 24.14 N·m at average peak in knee extension, as well as 18.41 N·m and 12.44 N·m in knee flexion, indicate changes that are not attributable to measurement error or subject variability and are relevant information for researchers and exercise and health professionals. Although this measure has been previously reported in other populations [54,55], its application in isokinetic dynamometry under DT conditions in women with FM has not been previously investigated.
Our reliability results differ slightly from those previously reported in FM [35], which only measured the performance of this isokinetic test in the ST condition. Furthermore, if we compare the values obtained in our study for the DT condition, they differ slightly from those of the study mentioned above. However, it is essential to note that the study conducted by Adsuar, Olivares, del Pozo-Cruz, Parraca, and Gusi [35] did not report mean peak torque values and analyzed the maximum of three repetitions. In contrast, our analysis was based on a maximum of five repetitions and considered the average value of the five repetitions as a more ecological and representative measure of the participants’ performance.
Given that the results obtained in our study have shown variability in ICC values, different factors may have influenced this aspect.
We must emphasize that we have a small sample and that the symptoms of FM can change. Although in our study no significant relationships were found between the performance obtained in the test, the impact of the disease, and the years with FM in the different conditions, taking into account the pain at baseline, individual variability in the pain threshold or muscle fatigue experienced during the isokinetic test may have altered the participants’ performance. In this sense, future studies must contemplate these aspects to obtain more precise information and determine whether the variability in the results may be due to these factors [56]. It would be desirable to replicate this study with a larger sample to more accurately determine the reliability of isokinetic dynamometry for measuring lower limb strength in ST [35] and DT conditions in women with FM.
Our results could have yielded lower values than other investigations due to the type of warm-up performed. In this line, Bishop [57] suggests that a warm-up performed at ~40–60% VO2 max for 5 to 10 min, followed by a 5 min recovery, will improve short-term performance. However, to avoid bias in our results, we followed the same warm-up protocol specified in our study for the test and retest. More research is needed to understand the ergogenic effects of warm-up on short-term performance, as it remains controversial [57].
Following a detailed analysis, significant variability in confidence intervals has been observed in both the ST and DT conditions, particularly in knee flexion. The ICC for maximum knee flexion peak torque was (0.72, 95% CI −0.13–0.93) and (0.77 95% CI 0.09–0.94) for average peak torque in the ST condition compared to (0.90 95% CI 0.03–0.94) and (0.91 95% CI 0.51–0.98) in the DT condition. This difference in results could be attributed to the possibility that individuals with FM might pay more attention to pain awareness during flexion, depending on the pain level they experience at that moment or the fear of experiencing that pain. However, an interesting issue was that the reliability value slightly increased in the DT condition. This could be explained by the potential for individuals to divert their focus to the cognitive task effectively and thus not pay attention to the level of pain they may be experiencing at the time. In this regard, a negative relationship has been observed between pain sensitivity and functional capacity in specific tests [58]. Individuals with FM struggle to regulate their emotional states, facing difficulties in concentration and task performance during negative mood states, which has a significant impact on pain severity and disability severity [59]. In addition, pain-related fear has been associated with increased pain, decreased tolerance to physical performance, reduced cognitive performance speed, increased sensitivity to painful points, and increased interference with other attention-demanding tasks [60]. Therefore, greater attention to pain, and its variability, could contribute to less reliable test results, highlighting the potential benefits of introducing a simultaneous cognitive task (DT) to assess lower limb strength in FM.
In this context, de Gier, Peters, and Vlaeyen [60] have found that tolerance to physical performance increases when distraction is introduced by a simultaneous cognitive task. In chronic pain patients, Rode et al. [61] have also demonstrated that the inclusion of a distracting task significantly enhances physical performance, elevating the initial tolerance level to a comparable level to that of pain-free controls. Our results could support the hypothesis that, although pain captures attention, it can be interrupted by employing another distracting task. This makes sense considering that in FM, pain has been observed to interfere with attention, involving the utilization of neural resources engaged in both processes [62]. In our study, the results were apparently slightly better in DT than when the test was performed without the cognitive task. Nevertheless, it is essential to consider that the interpretation of these results may be influenced by various pain-related characteristics (intensity, novelty, and predictability of threatening stimuli, as well as the tendency to catastrophize pain and heightened somatic awareness) and environmental factors (distractibility of pain and its emotional content and arousal properties) [43].
The assessment of DT conditions in fitness tests has been evaluated and proven reliable, aligning more closely with real-life conditions. It requires heightened attentional resources and engagement of executive functions [33], which are impaired in individuals with FM [63,64,65]. In this sense, the reliability of different tests such as the chair stand test [30], 10 m walking test [31], Timed Up and Go test (TUG) [31], arm curl test [30], and 3 m walking backward test (3MBWT) [32] have been investigated under DT conditions among people with FM. The findings from our study can complement previous research, expanding the range of reliable tests for assessing performance in DT situations in individuals with FM. Moreover, it presents a relevant interest in assessing physical performance since people with FM show lower values in peak torque than healthy people [17]. Furthermore, there is an association between a high prevalence of falls with lower functional performance and lower limb strength [17]. Therefore, it would be beneficial to use tests that consider DT performance to continue studying falls in FM, as may occur during activities of daily living.
The present study has some limitations. First, the sample was relatively small, and comprised solely of women, preventing the generalization of the results to the male population. However, it is essential to note that the morphological differences in the musculature can generate significant alterations in the mechanical properties of the muscles depending on the sex [66]. In this sense, future studies should consider this aspect to elucidate possible sex-related differences. Secondly, the age of the sample was between 30 and 75, a wide range that could influence both physical and cognitive performance. Third, individual variability in pain threshold and muscle fatigue experienced during the isokinetic test could have altered the performance of the participants. Fourth, the absence of specific neurological assessments to exclude co-existing neuropathies or other neurological conditions that might impact muscle strength testing complicates the interpretation of results solely attributable to FM. Fifth, only the concentric/concentric test was performed, so the results cannot be compared with other studies using different tests. Therefore, further studies exploring alternative tests are needed.
5. Conclusions
Isokinetic dynamometry demonstrated sufficient reliability for measuring strength in knee extension maximum and average during both single-task and dual-task conditions, as well as knee flexion dual-task average. However, for knee flexion single-task maximum and average and knee flexion dual-task maximum, we did not obtain sufficiently reliable measurements. Only the concentric/concentric test has been studied, and future studies with a larger sample size are needed in order to generalize the results.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm13051288/s1, Table S1. Correlation between the performance obtained in the isokinetic test under single and dual-task conditions in test and retest, FIQR and years of fibromyalgia symptomatology.
Author Contributions
Conceptualization, M.C.G.-A., S.V. and N.G.; methodology, M.C.G.-A., S.V., J.L.L.-L. and F.J.D.-M.; formal analysis, J.L.L.-L. and S.V.; investigation, M.C.G.-A. and M.M.-A.; resources, F.J.D.-M. and M.M.-A.; data curation, M.M.-A. and F.J.D.-M.; writing—original draft preparation, M.C.G.-A. and J.L.L.-L.; writing—review and editing, S.V. and N.G.; visualization, M.M.-A. and F.J.D.-M.; supervision, J.L.L.-L., S.V. and N.G.; funding acquisition, S.V. and N.G. All authors have read and agreed to the published version of the manuscript.
Funding
The author M.C.G.-A. was supported by an internship contract (Resolution no. 552/2020) from the Junta de Extremadura (Regional Government of Extremadura), Extremadura Public Employment Service (SEXPE) and the European Social Fund (ESF/FSE) “a way of doing Europe”. The author J.L.L.-L. was supported by a grant from the Spanish Ministry of Education, Culture, and Sport (FPU18/05655). The funders played no role in the study design, the data collection, and analysis, the decision to publish, or the preparation of the manuscript. In the framework of the Spanish National R + D + i Plan, the current study was co-funded by the Spanish Ministry of Sciences and Innovation (reference PID2019-107191RB-I00/AEI/10.13039/501100011033). This study was also funded by the Research Grant for Groups (GR21176) funded by the Junta de Extremadura and the European Regional Development Fund (ERDF/FEDER) “a way of doing Europe”. This study was supported by the Biomedical Research Networking Center on Frailty and Healthy Aging (CIBERFES) and FEDER funds from the European Union (CB16/10/00477) “a way of doing Europe”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and is currently approved by the Research Ethics Committee of the University of Extremadura (approval reference: 192/2021; approval date: 15 December 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data will not be shown publicly, as patients will give their consent for the information to be kept confidential.
Acknowledgments
We are very grateful the collaboration with the Extremadura Association of Fibromyalgia (AFIBROEX) in Caceres to facilitate the recruitment of participants.
Conflicts of Interest
The authors declare no conflicts of interest. The funders will have no role in the design of the study, the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Marques, A.P.; Santo, A.d.S.d.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Reyes Del Paso, G.A.; Pulgar, A.; Duschek, S.; Garrido, S. Cognitive impairment in fibromyalgia syndrome: The impact of cardiovascular regulation, pain, emotional disorders and medication. Eur. J. Pain 2012, 16, 421–429. [Google Scholar] [CrossRef]
- Gelonch, O.; Garolera, M.; Valls, J.; Rosselló, L.; Pifarré, J. Cognitive complaints in women with fibromyalgia: Are they due to depression or to objective cognitive dysfunction? J. Clin. Exp. Neuropsychol. 2017, 39, 1013–1025. [Google Scholar] [CrossRef]
- Gaudreault, N.; Boulay, P. Cardiorespiratory fitness among adults with fibromyalgia. Breathe 2018, 14, e25–e33. [Google Scholar] [CrossRef]
- Maquet, D.; Croisier, J.L.; Renard, C.; Crielaard, J.M. Muscle performance in patients with fibromyalgia. Jt. Bone Spine 2002, 69, 293–299. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Gallego-Diaz, J.M.; Adsuar, J.C.; Domínguez-Muñoz, F.J.; Olivares, P.R.; Gusi, N. Fear of Falling in Women with Fibromyalgia and Its Relation with Number of Falls and Balance Performance. Biomed Res. Int. 2015, 2015, 589014. [Google Scholar] [CrossRef][Green Version]
- Cardoso Fde, S.; Curtolo, M.; Natour, J.; Lombardi Júnior, I. Assessment of quality of life, muscle strength and functional capacity in women with fibromyalgia. Rev. Bras. Reumatol. 2011, 51, 338–343, 349–350. [Google Scholar] [PubMed]
- Yetişgin, A.; Tiftik, T.; Kara, M.; Karabay, İ.; Akkuş, S.; Ersöz, M. Isokinetic muscle performance of the hip and ankle muscles in women with fibromyalgia. Int. J. Rheum. Dis. 2016, 19, 551–556. [Google Scholar] [CrossRef]
- Tavares, L.F.; Germano Maciel, D.; Pereira Barros da Silva, T.Y.; Brito Vieira, W.H. Comparison of functional and isokinetic performance between healthy women and women with fibromyalgia. J. Bodyw. Mov. Ther. 2020, 24, 248–252. [Google Scholar] [CrossRef]
- Nørregaard, J.; Bülow, P.M.; Lykkegaard, J.J.; Mehlsen, J.; Danneskiold-Samsøoe, B. Muscle strength, working capacity and effort in patients with fibromyalgia. Scand. J. Rehabil. Med. 1997, 29, 97–102. [Google Scholar]
- Panton, L.B.; Kingsley, J.D.; Toole, T.; Cress, M.E.; Abboud, G.; Sirithienthad, P.; Mathis, R.; McMillan, V. A comparison of physical functional performance and strength in women with fibromyalgia, age- and weight-matched controls, and older women who are healthy. Phys. Ther. 2006, 86, 1479–1488. [Google Scholar] [CrossRef]
- Bachasson, D.; Guinot, M.; Wuyam, B.; Favre-Juvin, A.; Millet, G.Y.; Levy, P.; Verges, S. Neuromuscular fatigue and exercise capacity in fibromyalgia syndrome. Arthritis Care Res. 2013, 65, 432–440. [Google Scholar] [CrossRef]
- Borman, P.; Celiker, R.; Hasçelik, Z. Muscle performance in fibromyalgia syndrome. Rheumatol. Int. 1999, 19, 27–30. [Google Scholar] [CrossRef]
- Nørregaard, J.; Bülow, P.M.; Danneskiold-Samsøe, B. Muscle strength, voluntary activation, twitch properties, and endurance in patients with fibromyalgia. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Nørregaard, J.; Bülow, P.M.; Vestergaard-Poulsen, P.; Thomsen, C.; Danneskiold-Samøe, B. Muscle strength, voluntary activation and cross-sectional muscle area in patients with fibromyalgia. Br. J. Rheumatol. 1995, 34, 925–931. [Google Scholar] [CrossRef]
- Góes, S.M.; Leite, N.; Shay, B.L.; Homann, D.; Stefanello, J.M.; Rodacki, A.L. Functional capacity, muscle strength and falls in women with fibromyalgia. Clin. Biomech. 2012, 27, 578–583. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. Fibromyalgia and quality of life: A comparative analysis. J. Rheumatol. 1993, 20, 475–479. [Google Scholar] [PubMed]
- Huijnen, I.P.; Verbunt, J.A.; Meeus, M.; Smeets, R.J. Energy Expenditure during Functional Daily Life Performances in Patients with Fibromyalgia. Pain Pract. 2015, 15, 748–756. [Google Scholar] [CrossRef]
- Yuan, J.; Blumen, H.M.; Verghese, J.; Holtzer, R. Functional connectivity associated with gait velocity during walking and walking-while-talking in aging: A resting-state fMRI study. Hum. Brain Mapp. 2015, 36, 1484–1493. [Google Scholar] [CrossRef]
- Pedullà, L.; Tacchino, A.; Podda, J.; Bragadin, M.M.; Bonzano, L.; Battaglia, M.A.; Bove, M.; Brichetto, G.; Ponzio, M. The patients’ perspective on the perceived difficulties of dual-tasking: Development and validation of the Dual-Task Impact on Daily-Living Activities Questionnaire (DIDA-Q). Mult. Scler. Relat. Disord. 2020, 46, 102601. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Eskes, G. Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Front. Hum. Neurosci. 2015, 9, 225. [Google Scholar] [CrossRef] [PubMed]
- Marois, R.; Ivanoff, J. Capacity limits of information processing in the brain. Trends Cogn. Sci. 2005, 9, 296–305. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, T.L.; Fritz, N.E.; Quinn, L.; Muratori, L.M. Cognitive-Motor Interference in Neurodegenerative Disease: A Narrative Review and Implications for Clinical Management. Front. Psychol. 2018, 9, 2061. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Collado-Mateo, D.; Domínguez-Muñoz, F.J.; Fuentes-García, J.P.; Gusi, N. Impact of adding a cognitive task while performing physical fitness tests in women with fibromyalgia: A cross-sectional descriptive study. Medicine 2018, 97, e13791. [Google Scholar] [CrossRef]
- Sempere-Rubio, N.; López-Pascual, J.; Aguilar-Rodríguez, M.; Cortés-Amador, S.; Espí-López, G.; Villarrasa-Sapiña, I.; Serra-Añó, P. Characterization of postural control impairment in women with fibromyalgia. PLoS ONE 2018, 13, e0196575. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Gusi, N.; Rodriguez-Generelo, S.; Martin-Gallego, J.D.; Fuentes-García, J.P.; Collado-Mateo, D. Influence of a Cell-Phone Conversation on Balance Performance in Women with Fibromyalgia: A Cross-Sectional Descriptive Study. Biomed Res. Int. 2019, 2019, 5132802. [Google Scholar] [CrossRef]
- Beyrek, B.; Naz, İ.; Emuk, Y.; Köprülüoğlu, M.; Felekoğlu, E.; Uzun, E.; Nas, K. Investigation of the dual-task performance and affecting factors in female patients with fibromyalgia syndrome. Women Health 2023, 63, 277–284. [Google Scholar] [CrossRef]
- Villafaina, S.; Polero, P.; Collado-Mateo, D.; Fuentes-García, J.P.; Gusi, N. Impact of adding a simultaneous cognitive task in the elbow’s range of movement during arm curl test in women with fibromyalgia. Clin. Biomech. 2019, 65, 110–115. [Google Scholar] [CrossRef]
- Leon-Llamas, J.L.; Villafaina, S.; Murillo-Garcia, A.; Collado-Mateo, D.; Javier Domínguez-Muñoz, F.; Sánchez-Gómez, J.; Gusi, N. Strength Assessment Under Dual Task Conditions in Women with Fibromyalgia: A Test-Retest Reliability Study. Int. J. Environ. Res. Public Health 2019, 16, 4971. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Garcia, A.; Villafaina, S.; Leon-Llamas, J.L.; Sánchez-Gómez, J.; Domínguez-Muñoz, F.J.; Collado-Mateo, D.; Gusi, N. Mobility Assessment under Dual Task Conditions in Women with Fibromyalgia: A Test-Retest Reliability Study. PM&R 2021, 13, 66–72. [Google Scholar] [CrossRef]
- Leon-Llamas, J.L.; Villafaina, S.; Murillo-Garcia, A.; Domínguez-Muñoz, F.J.; Gusi, N. Test-Retest Reliability and Concurrent Validity of the 3 m Backward Walk Test under Single and Dual-Task Conditions in Women with Fibromyalgia. J. Clin. Med. 2022, 12, 212. [Google Scholar] [CrossRef]
- Piqueres-Juan, I.; Tirapu-Ustárroz, J.; García-Sala, M. Dual performance paradigms: Their conceptual aspects. Rev. Neurol. 2021, 72, 357–367. [Google Scholar] [CrossRef]
- Ahmed, I.; Ishtiaq, S. Reliability and validity: Importance in Medical Research. J. Pak. Med. Assoc. 2021, 71, 2401–2406. [Google Scholar] [CrossRef] [PubMed]
- Adsuar, J.C.; Olivares, P.R.; del Pozo-Cruz, B.; Parraca, J.A.; Gusi, N. Test-retest reliability of isometric and isokinetic knee extension and flexion in patients with fibromyalgia: Evaluation of the smallest real difference. Arch. Phys. Med. Rehabil. 2011, 92, 1646–1651. [Google Scholar] [CrossRef]
- Hooten, W.M.; Rosenberg, C.J.; Eldrige, J.S.; Qu, W. Knee extensor strength is associated with pressure pain thresholds in adults with fibromyalgia. PLoS ONE 2013, 8, e59930. [Google Scholar] [CrossRef]
- Cubukcu, S.; Alimoglu, M.K.; Samanci, N.; Gurbuz, U. Isokinetic and Isometric Muscle Strength of the Knee Flexors and Extensors in Patients with the Fibromyalgia Syndrome and Chronic Myofascial Pain Syndrome. J. Musculoskelet. Pain 2007, 15, 49–55. [Google Scholar] [CrossRef]
- Henriksen, M.; Lund, H.; Christensen, R.; Jespersen, A.; Dreyer, L.; Bennett, R.M.; Danneskiold-Samsøe, B.; Bliddal, H. Relationships between the fibromyalgia impact questionnaire, tender point count, and muscle strength in female patients with fibromyalgia: A cohort study. Arthritis Rheum. 2009, 61, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Baltzopoulos, V.; Brodie, D.A. Isokinetic dynamometry. Applications and limitations. Sports Med. 1989, 8, 101–116. [Google Scholar] [CrossRef]
- Osternig, L.R. Isokinetic dynamometry: Implications for muscle testing and rehabilitation. Exerc. Sport Sci. Rev. 1986, 14, 45–80. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The Revised Fibromyalgia Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef] [PubMed]
- Roman-Viñas, B.; Serra-Majem, L.; Hagströmer, M.; Ribas-Barba, L.; Sjöström, M.; Segura-Cardona, R. International physical activity questionnaire: Reliability and validity in a Spanish population. Eur. J. Sport Sci. 2010, 10, 297–304. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Garcia, A.; Leon-Llamas, J.L.; Villafaina, S.; Rohlfs-Dominguez, P.; Gusi, N. MoCA vs. MMSE of Fibromyalgia Patients: The Possible Role of Dual-Task Tests in Detecting Cognitive Impairment. J. Clin. Med. 2021, 10, 125. [Google Scholar] [CrossRef] [PubMed]
- Carson, N.; Leach, L.; Murphy, K.J. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 2018, 33, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Coban, O.; Yildirim, N.U.; Yasa, M.E.; Akinoglu, B.; Kocahan, T. Determining the number of repetitions to establish isokinetic knee evaluation protocols specific to angular velocities of 60°/second and 180°/second. J. Bodyw. Mov. Ther. 2021, 25, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [PubMed]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Salaffi, F.; Di Carlo, M.; Arcà, S.; Galeazzi, M. Categorisation of disease severity states in fibromyalgia: A first step to support decision-making in health care policy. Clin. Exp. Rheumatol. 2018, 36, 1074–1081. [Google Scholar] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Ries, J.D.; Echternach, J.L.; Nof, L.; Gagnon Blodgett, M. Test-retest reliability and minimal detectable change scores for the timed “up & go” test, the six-minute walk test, and gait speed in people with Alzheimer disease. Phys. Ther. 2009, 89, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Pérez de Villar, L.; Martínez-Olmos, F.J.; Junqué-Jiménez, A.; Amer-Cuenca, J.J.; Martínez-Gramage, J.; Mercer, T.; Segura-Ortí, E. Test-retest reliability and minimal detectable change scores for the short physical performance battery, one-legged standing test and timed up and go test in patients undergoing hemodialysis. PLoS ONE 2018, 13, e0201035. [Google Scholar] [CrossRef] [PubMed]
- Dailey, D.L.; Frey Law, L.A.; Vance, C.G.; Rakel, B.A.; Merriwether, E.N.; Darghosian, L.; Golchha, M.; Geasland, K.M.; Spitz, R.; Crofford, L.J.; et al. Perceived function and physical performance are associated with pain and fatigue in women with fibromyalgia. Arthritis Res. Ther. 2016, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D. Warm up II: Performance changes following active warm up and how to structure the warm up. Sports Med. 2003, 33, 483–498. [Google Scholar] [CrossRef]
- Carbonell-Baeza, A.; Aparicio, V.A.; Sjöström, M.; Ruiz, J.R.; Delgado-Fernández, M. Pain and functional capacity in female fibromyalgia patients. Pain Med. 2011, 12, 1667–1675. [Google Scholar] [CrossRef]
- Trucharte, A.; Leon, L.; Castillo-Parra, G.; Magán, I.; Freites, D.; Redondo, M. Emotional regulation processes: Influence on pain and disability in fibromyalgia patients. Clin. Exp. Rheumatol. 2020, 38 (Suppl. S123), 40–46. [Google Scholar]
- de Gier, M.; Peters, M.L.; Vlaeyen, J.W. Fear of pain, physical performance, and attentional processes in patients with fibromyalgia. Pain 2003, 104, 121–130. [Google Scholar] [CrossRef]
- Rode, S.; Salkovskis, P.M.; Jack, T. An experimental study of attention, labelling and memory in people suffering from chronic pain. Pain 2001, 94, 193–203. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; de la Coba, P.; Colmenero, J.M.; Reyes Del Paso, G.A.; Duschek, S. Attentional function in fibromyalgia and rheumatoid arthritis. PLoS ONE 2021, 16, e0246128. [Google Scholar] [CrossRef] [PubMed]
- Walker, J. Fibromyalgia: Clinical features, diagnosis and management. Nurs. Stand. 2016, 31, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Bell, T.; Trost, Z.; Buelow, M.T.; Clay, O.; Younger, J.; Moore, D.; Crowe, M. Meta-analysis of cognitive performance in fibromyalgia. J. Clin. Exp. Neuropsychol. 2018, 40, 698–714. [Google Scholar] [CrossRef] [PubMed]
- Glass, J.M. Review of cognitive dysfunction in fibromyalgia: A convergence on working memory and attentional control impairments. Rheum. Dis. Clin. N. Am. 2009, 35, 299–311. [Google Scholar] [CrossRef]
- Deodato, M.; Saponaro, S.; Šimunič, B.; Martini, M.; Galmonte, A.; Murena, L.; Buoite Stella, A. Sex-based comparison of trunk flexors and extensors functional and contractile characteristics in young gymnasts. Sport Sci. Health 2023, 1–9. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).