


Functional Outcomes in Upper Limb Replantation—A Systematic Review
 ,
,  and
and 
Abstract
1. Introduction
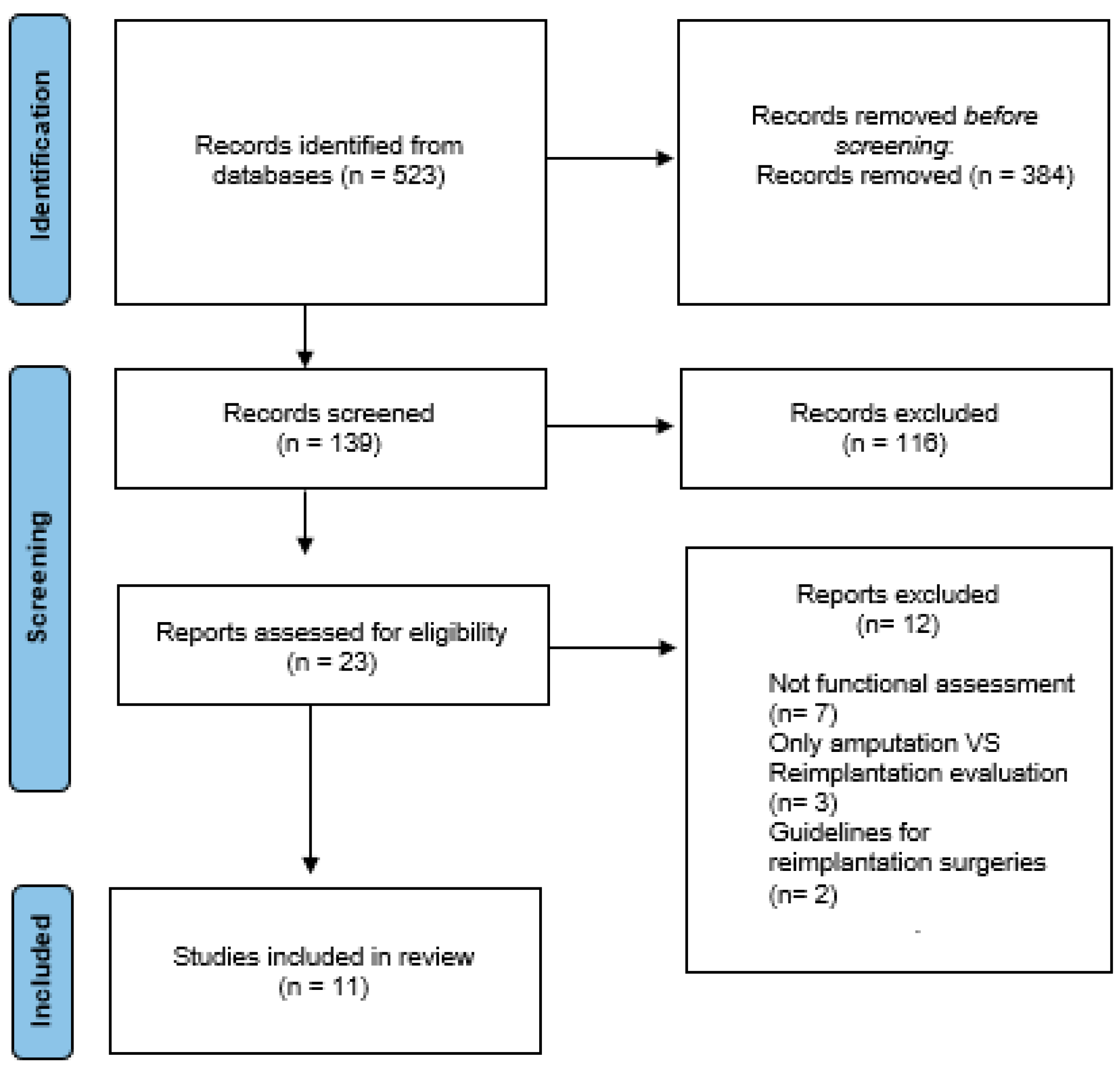
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Medling, B.D.; Bueno, R.A.; Russell, R.C.; Neumeister, M.W. Replantation outcomes. Clin. Plast. Surg. 2007, 34, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.H. Practical Tips to Improve Efficiency and Success in Upper Limb Replantation. Plast. Reconstr. Surg. 2019, 144, 878e–911e. [Google Scholar] [CrossRef] [PubMed]
- Barbary, S.; Dap, F.; Dautel, G. Finger replantation: Surgical technique and indications. Chir. Main 2013, 32, 363–372. [Google Scholar] [CrossRef]
- Sears, E.; Chung, K. Reimplantación de lesiones por avulsión de dedos: Una revisión sistemática de la supervivencia y los resultados funcionales. J. Hand Surg. Am. 2011, 36, 386–394. [Google Scholar] [CrossRef]
- Atkin Sara, E.; Winterton Robert, I.S.; Kay Simón, P. Upper limb amputations: Where, when and how to replant. Orthopaedics and trauma. Curr. Orthop. 2008, 22, 31–41. [Google Scholar] [CrossRef]
- Lara Guerrero, M.; Camporro Fernández, D.; Fernández Tárano, L.; García del Pozo, E. Measurement of replantation out-comes at Central University Hospital of Asturias (Spain): A retrospective study. Cir. Plást. Iberolati-Noam. Abril-Junio 2023, 49, 177–186. [Google Scholar]
- Camporro Fernández, D.; Barrio, L.; García del Pozo, E.; Contreras Pedraza, D.; Matarranz Faya, A. Principios de evalua¬ción y resultados funcionales en los reimplantes de miembro superior. Cir. Plást. Iberolatinoam. 2012, 38, 247–256. [Google Scholar] [CrossRef]
- Chuang, D.C.; Lai, J.B.; Cheng, S.L.; Jain, V.; Lin, C.H.; Chen, H.C. Traction avulsion amputation of the major upper limb: A proposed new classification, guidelines for acute management, and strategies for secondary reconstruction. Plast. Reconstr. Surg. 2001, 108, 1624–1638. [Google Scholar] [CrossRef]
- Tamai, S. Twenty years experience of limb replantation. Review of 293 upper limb reimplants. J. Hand Surg. 1982, 7, 549–556. [Google Scholar] [CrossRef]
- Ono, S.; Chung, K.C. Efficiency in Digital and Hand Replantation. Clin. Plast. Surg. 2019, 46, 359–370. [Google Scholar] [CrossRef]
- Khan, N.; Rashid, M.; Rashid, H.; Rehman Sarwar, S.; Khalid Choudry, U.; Khurshid, M. Resultados funcionales de los procedimientos secundarios en el reimplante y revascularización de las extremidades superiores. Cureus2 2019, 11, 5164. [Google Scholar] [CrossRef]
- Bott, S.; Rachunek, K.; Medved, F.; Bott, T.; Daigeler, A.; Wahler, T. Resultado funcional después del reimplante de dedos versus amputación. J. Orthop. Traumatol. 2022, 23, 35. [Google Scholar] [CrossRef] [PubMed]
- Urbaniak, J.R.; Evans, J.P.; Bright, D.S. Microvascular management of ring avulsion injuries. J. Hand Surg. Am. 1981, 6, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.; Werntz, J.; Wolff, T.W. Ring avulsion injuries: Classification and prognosis. J. Hand Surg. Am. 1989, 14 Pt 1, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, T.; Buchler, U. Lesiones complejas graves en la extremidad superior: Revascularización y reimplantación. J. Hand Surg. Am. 1991, 16, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Laing, T.; Cassell, O.; O’Donovan, D.; Eadie, P. Resultados funcionales a largo plazo de reimplantes importantes de extremidades. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 931–934. [Google Scholar] [CrossRef]
- Mattiassich, G.; Rittenschober, F.; Dorninger, L.; Rois, J.; Mittermayr, R.; Ortmaier, R.; Ponschab, M.; Katzensteiner, K.; Larcher, L. Resultado a largo plazo tras el reimplante de una extremidad superior después de una amputación traumática mayor. Trastor. Musculoesquelético BMC 2017, 18, 77. [Google Scholar] [CrossRef]
- Molski, M. Replantation of fingers and hands after avulsion and crush injuries. J. Plast. Reconstr. Aesthetic Surg. 2007, 60, 748–754. [Google Scholar] [CrossRef]
- Battison, B.; Tos, P.; Clemente, A.; Pontini, I. Actualities in big segment replantation surgery. J. Plast. Reconstr. Aesthetic Surg. 2007, 60, 849–855. [Google Scholar] [CrossRef]
- Sebastin, S.; Chung, K. Desafíos en la medición de los resultados después de la reimplantación digital. Cirugía Semin. Plast. 2013, 27, 174–181. [Google Scholar] [CrossRef]
- Hudak, P.; Amadio, P.; Bombardier, C. Desarrollo de una medida de resultado de las extremidades superiores: El DASH (discapacidades del brazo, hombro y mano) [corregido]. El Grupo Colaborativo de Extremidades Superiores (UECG). Soy. J. Ind. Med. 1996, 29, 302–308. [Google Scholar] [CrossRef]
- Carlsson, I.; Cederlund, R.; Höglund, P.; Lundborg, G.; Rosén, B. Lesiones en las manos y sensibilidad al frío: Confiabilidad y validez de los cuestionarios de sensibilidad al frío. Disabil. Rehabil. 2008, 30, 1920–1928. [Google Scholar] [CrossRef]
- Gummesson, C.; Ward, M.; Atroshi, I. Las discapacidades abreviadas del cuestionario de brazo, hombro y mano (QuickDASH): Validez y confiabilidad basadas en respuestas dentro del cuestionario DASH completo. Trastor. Musculoesquelético BMC 2006, 8, 44. [Google Scholar] [CrossRef]
- Chen, Z.; Yu, H. Procedimientos actuales en China sobre reimplantación de extremidades y dedos amputados. Clin. Orthop. Relat. Res. 1987, 215, 15–23. [Google Scholar]
- Chung, K.; Pillsbury, M.; Walters, M.; Hayward, R. Pruebas de confiabilidad y validez del Michigan Hand Outcomes Questionnaire. Cirugía Mano J. Am. 1998, 23, 575–587. [Google Scholar] [CrossRef]
- Colen, L.; Bunkis, J.; Gordon, L.; Walton, R. Evaluación funcional de la transferencia de rayos para la pérdida digital central. D. Mano Surg. 1985, 10, 232–237. [Google Scholar] [CrossRef]
- Goodson, A.; McGregor, A.; Douglas, J.; Taylor, P. Evaluación clínica cuantitativa directa de la función de la mano: Utilidad y reproducibilidad. Hombre Allí. 2007, 12, 144–152. [Google Scholar] [CrossRef]
- Granger, C.; Ottenbacher, K.; Fiedler, R. El sistema de datos uniforme para la rehabilitación médica. Informe de primeros ingresos de 1993. Am. J. Phys. Med. Rehabil. 1995, 74, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Dolan, P. Modelización de valoraciones para estados de salud EuroQol. Atención Méd. 1997, 35, 1095–1108. [Google Scholar] [CrossRef]
- Zung, W. Un instrumento de calificación para los trastornos de ansiedad. Psicosomativos 1971, 12, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Steer, R. Brown GKBDI-II. Inventario de depresión de Beck: Manual. In San Antonio; Psychological Corporation: New York, NY, USA, 1996. [Google Scholar]
- Carlson, E. Estudio psicométrico de una prueba breve para el trastorno de estrés postraumático: Evaluación del impacto de múltiples eventos traumáticos. Evaluación 2001, 8, 431–441. [Google Scholar] [CrossRef]
- Urbaniak, J.R.; Roth, J.H.; Nunley, J.A.; Goldner, R.D.; Koman, A. The results of replantation after single finger amputation. J. Bone Jt. Surg. Am. 1985, 67, 611–619. [Google Scholar] [CrossRef]
- Sabapathy, S.R.; Venkatramani, H.; Bharathi, R.; Bhardwaj, P. Replantation Surgery. J. Hand Surg. 2011, 36A, 1104. [Google Scholar] [CrossRef]
- Bath, A.; Acharya, A.; Narayanakurup, J.; Kumar, B.; Nagpal, P.; Kamath, A. Resultado funcional y cosmético de la amputación de rayos de un solo dígito en la mano. Cirugía Musculoesquelética 2017, 101, 275–281. [Google Scholar] [CrossRef]
- Gürbüz, K.; Yontar, Y. Una experiencia de cuatro años en un hospital comunitario con respecto a procedimientos para la reimplantación y revascularización de los dedos. Jt. Dis. Relar. Surg. 2021, 32, 383–390. [Google Scholar] [CrossRef]
- KYNg, W.; Nirmal Kaur, M.; Thoma, A. Resultados a largo plazo de reimplantes importantes de extremidades superiores. Cirugía Plástica. 2014, 22, 9–13. [Google Scholar]
- Giardi, D.; Crosio, A.; Da Rold, I.; Magistroni, E.; Tos, P.; Titolo, P.; Battiston, B.; Ciclamini, D. Resultados clínicos a largo plazo de 33 reimplantes de pulgar. Lesión 2020, 51, S71–S76. [Google Scholar] [CrossRef]
- Ciclamini, D.; Tos, P.; Magistroni, E.; Panero, B.; Titolo, P.; Da Rold, I.; Battiston, B. Resultados funcionales y subjetivos de 20 reimplantes de pulgar. Lesión 2013, 44, 504–507. [Google Scholar] [CrossRef]
- Rosberg, H.E. Discapacidad y salud después de la reimplantación o revascularización en la extremidad superior en una población del sur de Suecia: Un seguimiento retrospectivo a largo plazo. Trastor. Musculoesquelético BMC 2014, 15, 73. [Google Scholar] [CrossRef]
- Jiménez-Cortes, E.; López-Rios, A.; Vásquez-Sañudo, V.; Cardona-González, E. Estudio descriptivo de pacientes con amputación de miembro superior como posibles candidatos a trasplante de mano en Medellín, Colombia. Cureus 2022, 14, 22527. [Google Scholar] [CrossRef]
- Haas, F.; Hubner, M.; Rappl, T.; Koch, H.; Parvizi, I.; Parvizi, D. Long-term subjective and functional evaluation after thumb replantation with special attention to the Quick DASH questionnaire and a specially designed trauma score called modified mayo score. J. Trauma 2010, 20, 460–466. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Article | Type of Article | n |
|---|---|---|
| Functional Outcomes of Secondary Procedures in Upper Extremity Replantation and Revascularization | Prospective observational study | 40 |
| Long-term outcomes of major upper extremity replantations | Prospective study | 16 |
| Disability and health after replantation or revascularization in the upper extremity in a population in southern Sweden—a retrospective long time follow up | Retrospective study | 326 |
| Long-term outcome following upper extremity replantation after major traumatic amputation | Prospective study | 16 |
| Long-term functional, subjective and psychological results after single digit replantation | Prospective study | 30 |
| A four-year community hospital experience regarding procedures for the replantation and revascularization of fingers | Prospective study | 58 |
| Upper extremity replantation results in our series and review of replantation indications | Prospective study | 14 |
| Reconstructive surgery of the amputated ring finger | Retrospective study | 9 |
| Functional and subjective results of 20 thumb replantations | Prospective study | 20 |
| Long-term clinical results of 33 thumb replantations | Retrospective study | 33 |
| Functional and cosmetic outcome of single-digit ray amputation in hand | Prospective study | 45 |
| Characteristics (n = 607) | |
|---|---|
| Age, y (mean) | 38 |
| Male | 512 |
| Female | 95 |
| Mechanism of injury (n = 518) | |
| Cut | 407 |
| Crush | 80 |
| Avulsion | 26 |
| Self-inflicted | 5 |
| Level of injury (n = 606) | |
| Arm | 14 |
| Elbow and forearm | 31 |
| Wrist | 27 |
| Metacarpal | 29 |
| Fingers | 361 |
| Thumb | 144 |
| Scales | Number of Articles in Which They Appear |
|---|---|
| DASH (n = 160) | 6 |
| QuickDASH (n = 424) | 3 |
| CISS (n = 528) | 7 |
| Chen (n = 27) | 2 |
| MHQ (n = 46) | 2 |
| RAS (n = 54) | 2 |
| ROM (n = 87) | 3 |
| FIM (n = 16) | 1 |
| EQ-5D (n = 326) | 1 |
| SAS (n = 30) | 1 |
| BDI (n = 30) | 1 |
| SPTSS (n = 30) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bueno, A.; Nevado-Sanchez, E.; Collazo, C.; De la Fuente-Anuncibay, R.; González-Bernal, J. Functional Outcomes in Upper Limb Replantation—A Systematic Review. J. Clin. Med. 2024, 13, 1289. https://doi.org/10.3390/jcm13051289
Bueno A, Nevado-Sanchez E, Collazo C, De la Fuente-Anuncibay R, González-Bernal J. Functional Outcomes in Upper Limb Replantation—A Systematic Review. Journal of Clinical Medicine. 2024; 13(5):1289. https://doi.org/10.3390/jcm13051289
Chicago/Turabian StyleBueno, Andrea, Endika Nevado-Sanchez, Carla Collazo, Raquel De la Fuente-Anuncibay, and Jerónimo González-Bernal. 2024. "Functional Outcomes in Upper Limb Replantation—A Systematic Review" Journal of Clinical Medicine 13, no. 5: 1289. https://doi.org/10.3390/jcm13051289
APA StyleBueno, A., Nevado-Sanchez, E., Collazo, C., De la Fuente-Anuncibay, R., & González-Bernal, J. (2024). Functional Outcomes in Upper Limb Replantation—A Systematic Review. Journal of Clinical Medicine, 13(5), 1289. https://doi.org/10.3390/jcm13051289