
Effectiveness of a Web-Guided Self-Managed Telerehabilitation Program Enhanced with Outdoor Physical Activity on Physical Function, Physical Activity Levels and Pain in Patients with Knee Osteoarthritis: A Randomized Controlled Trial

 ,
,  ,
,  ,
, 
Abstract

1. Introduction
2. Methods
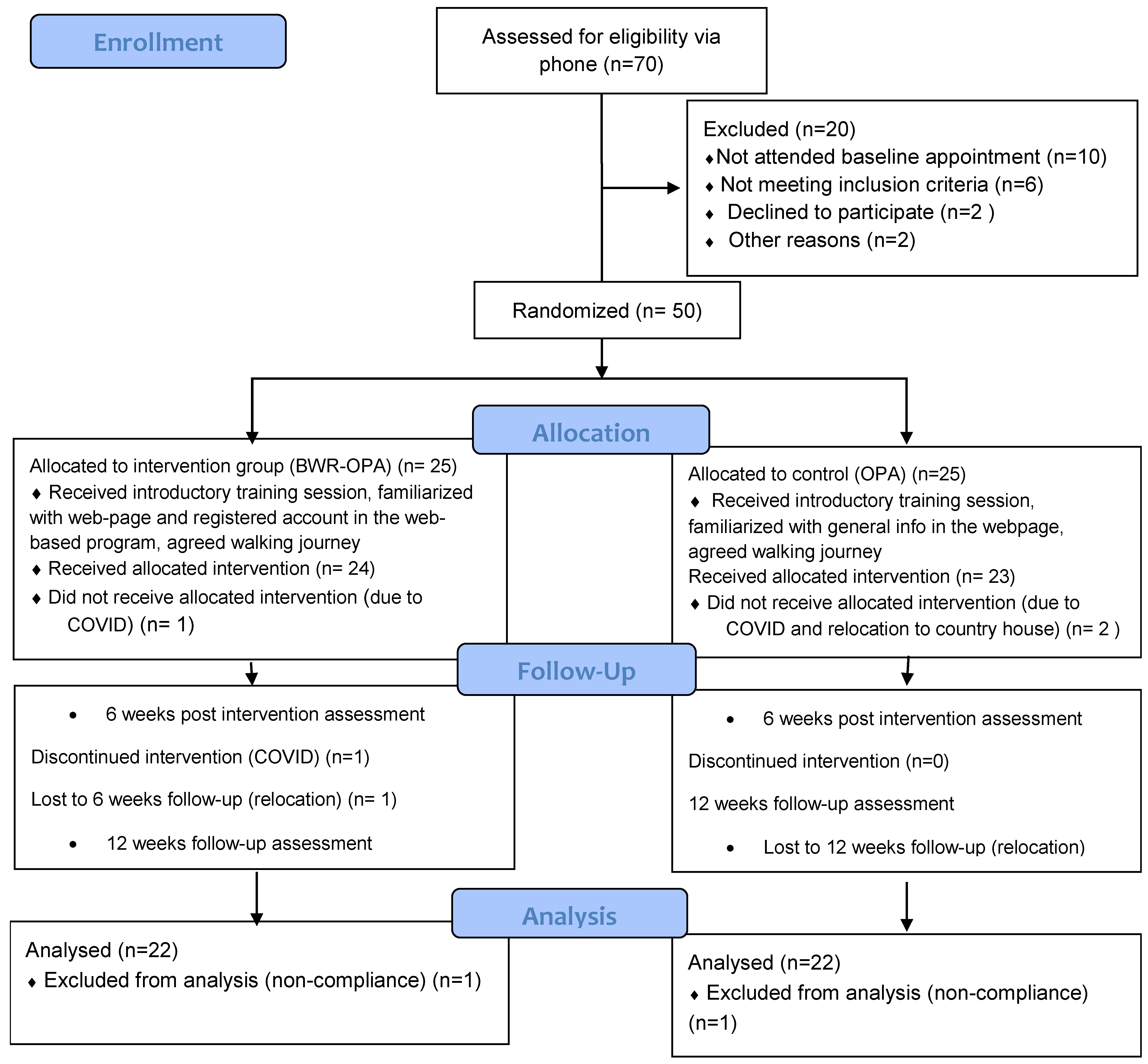
2.1. Study Participants
- clinical (clinical criteria: age ≥ 45 years, activity-related knee pain and morning knee stiffness ≤ 30 min) or radiographic diagnosis of knee OA;
- knee pain on most days for 3 months or more;
- average overall knee pain severity of 4 or greater on an 11-point numeric rating scale (NPRS) during the previous week;
- own a smart phone device or tablet;
- home internet access;
- ability to consent, participate and complete assessments.
2.2. Study Design and Procedures
2.2.1. Randomization, Allocation Concealment and Blinding
2.2.2. Study Groups
2.2.3. Outcomes
2.2.4. Data Analysis
3. Results
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Mahir, L.; Belhaj, K.; Zahi, S.; Azanmasso, H.; Lmidmani, F.; El Fatimi, A. Impact of knee osteoarthritis on the quality of life. Ann. Phys. Rehabil. Med. 2016, 59, e159. [Google Scholar] [CrossRef]
- Available online: https://www.nice.org.uk/about/what-we-do/into-practice/measuring-the-use-of-nice-guidance/impact-of-our-guidance/nice-impact-arthritis/osteoarthritis (accessed on 29 November 2023).
- Kanavaki, A.M.; Rushton, A.; Efstathiou, N.; Alrushud, A.; Klocke, R.; Abhishek, A.; Duda, J.L. Barriers and facilitators of physical activity in knee and hip osteoarthritis: A systematic review of qualitative evidence. BMJ Open 2017, 7, e017042. [Google Scholar] [CrossRef]
- Ingelsrud, L.H.; Roos, E.M.; Gromov, K.; Jensen, S.S.; Troelsen, A. Patients report inferior quality of care for knee osteoarthritis prior to assessment for knee replacement surgery—A cross-sectional study of 517 patients in Denmark. Acta Orthop. 2020, 91, 82–87. [Google Scholar] [CrossRef]
- Hagen, K.B.; Smedslund, G.; Østerås, N.; Jamtvedt, G. Quality of Community-Based Osteoarthritis Care: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2016, 68, 1443–1452. [Google Scholar] [CrossRef]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef]
- Barlow, J.; Wright, C.; Sheasby, J.; Turner, A.; Hainsworth, J. Self-management approaches for people with chronic conditions: A review. Patient Educ. Couns. 2002, 48, 177–187. [Google Scholar] [CrossRef]
- Carnes, D.; Homer, K.E.; Miles, C.L.; Pincus, T.; Underwood, M.; Rahman, A.; Taylor, S.J. Effective Delivery Styles and Content for Self-management Interventions for Chronic Musculoskeletal Pain: A systematic literature review. Clin. J. Pain 2012, 28, 344–354. [Google Scholar] [CrossRef]
- Wu, S.-F.V.; Kao, M.-J.; Wu, M.-P.; Tsai, M.-W.; Chang, W.-W. Effects of an osteoarthritis self-management programme. J. Adv. Nurs. 2011, 67, 1491–1501. [Google Scholar] [CrossRef]
- Wu, Z.; Zhou, R.; Zhu, Y.; Zeng, Z.; Ye, Z.; Wang, Z.; Liu, W.; Xu, X. Self-Management for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Res. Manag. 2022, 2022, 2681240. [Google Scholar] [CrossRef]
- Ravalli, S.; Castrogiovanni, P.; Musumeci, G. Exercise as medicine to be prescribed in osteoarthritis. World J. Orthop. 2019, 10, 262–267. [Google Scholar] [CrossRef]
- Eyles, J.P.; Hunter, D.J.; Bennell, K.L.; Dziedzic, K.S.; Hinman, R.S.; van der Esch, M.; Holden, M.A.; Bowden, J.L.; Quicke, J.; Skou, S.; et al. Joint Effort Initiative Members. Priorities for the effective implementation of osteoarthritis management programs: An OARSI international consensus exercise. Osteoarthr. Cartil. 2019, 27, 1270–1279. [Google Scholar] [CrossRef]
- Shuyler, K.S.; Knight, K.M. What Are Patients Seeking When They Turn to the Internet? Qualitative Content Analysis of Questions Asked by Visitors to an Orthopaedics Web Site. J. Med. Internet Res. 2003, 5, e24. [Google Scholar] [CrossRef]
- Jellison, S.S.; Bibens, M.; Checketts, J.; Vassar, M. Using Google Trends to assess global public interest in osteoarthritis. Rheumatol. Int. 2018, 38, 2133–2136. [Google Scholar] [CrossRef]
- Fraval, A. Internet use by orthopaedic outpatients—Current trends and practices. Australas. Med. J. 2012, 5, 633–638. [Google Scholar] [CrossRef]
- McHugh, C.; Kostic, A.; Katz, J.; Losina, E. Effectiveness of remote exercise programs in reducing pain for patients with knee osteoarthritis: A systematic review of randomized trials. Osteoarthr. Cartil. Open 2022, 4, 100264. [Google Scholar] [CrossRef]
- Patten, R.K.; Tacey, A.; Pile, R.; Parker, A.; De Gori, M.; Tran, P.; McKenna, M.J.; Lane, R.; Apostolopoulos, V.; Said, C.M.; et al. Digital self-management interventions for osteoarthritis: A systematic scoping review of intervention characteristics, adherence and attrition. Arch. Public Health 2022, 80, 103. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.E.; Murray, T.E.; O’Rourke, A.C.; Low, C.; Veale, D.J. Readability and Quality of Online Information on Osteoarthritis: An Objective Analysis With Historic Comparison. Interact. J. Med. Res. 2019, 8, e12855. [Google Scholar] [CrossRef]
- Sullivan, B.; Abed, V.; Joiner, J.; Benningfield, M.; Landy, D.; Hawk, G.S.; Conley, C.; Jacobs, C.; Stone, A.V. The Quality of Online Information for the Treatment of Knee Osteoarthritis: A Google Study. Cureus 2022, 14, e29995. [Google Scholar] [CrossRef]
- Pisters, M.F.; Veenhof, C.; van Meeteren, N.L.U.; Ostelo, R.W.; de Bakker, D.H.; Schellevis, F.G.; Dekker, J. Long-Term effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: A systematic review. Arthritis Care Res. 2007, 57, 1245–1253. [Google Scholar] [CrossRef]
- Pisters, M.F.; Veenhof, C.; Schellevis, F.G.; Twisk, J.W.R.; Dekker, J.; De Bakker, D.H. Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee. Arthritis Care Res. 2010, 62, 1087–1094. [Google Scholar] [CrossRef]
- Davies, C.A.; Spence, J.C.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Meta-analysis of internet-delivered interventions to increase physical activity levels. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 52. [Google Scholar] [CrossRef]
- Available online: https://www.equator-network.org/reporting-guidelines/consort/ (accessed on 30 May 2023).
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; CONSORT Group. Extending the CONSORT Statement to Randomized Trials of Nonpharmacologic Treatment: Explanation and Elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef]
- Moutzouri, M.; Gioftsos, G. How effective is a blended web-based rehabilitation for improving pain, physical activity, and knee function of patients with knee osteoarthritis? Study protocol for a randomized control trial. PLoS ONE 2022, 17, e0268652. [Google Scholar] [CrossRef] [PubMed]
- Global Recommendations on Physical Activity (PA) for Health: 65 Years and above. World Health Organisation. Available online: http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/ (accessed on 30 May 2023).
- Hurley, M.V.; Walsh, N.E.; Mitchell, H.L.; Pimm, T.J.; Patel, A.; Williamson, E.; Jones, R.H.; Dieppe, P.A.; Reeves, B.C. Clinical effectiveness of a rehabilitation program integrating exercise, self-management, and active coping strategies for chronic knee pain: A cluster randomized trial. Arthritis Care Res. 2007, 57, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Hurley, M.V.; Walsh, N.E.; Mitchell, H.; Nicholas, J.; Patel, A. Long-term outcomes and costs of an integrated rehabilitation program for chronic knee pain: A pragmatic, cluster randomized, controlled trial. Arthritis Care Res. 2012, 64, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Rolfson, O.; Wissig, S.; van Maasakkers, L.; Stowell, C.; Ackerman, I.; Ayers, D.; Franklin, P.D. Defining an International Standard Set of Outcome Measures for Patients With Hip or Knee Osteoarthritis: Consensus of the International Consortium for Health Outcomes Measurement Hip and Knee Osteoarthritis Working Group. Arthritis Care Res. 2016, 68, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63 (Suppl. S11), S240–S252. [Google Scholar] [CrossRef]
- Dobson, F.; Hinman, R.S.; Roos, E.M.; Abbott, J.H.; Stratford, P.; Davis, A.M.; Bennell, K.L. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1042–1052. [Google Scholar] [CrossRef]
- Dobson, F.; Hinman, R.; Hall, M.; Marshall, C.; Sayer, T.; Anderson, C.; Newcomb, N.; Stratford, P.; Bennell, K. Reliability and measurement error of the Osteoarthritis Research Society International (OARSI) recommended performance-based tests of physical function in people with hip and knee osteoarthritis. Osteoarthr. Cartil. 2017, 25, 1792–1796. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, S. Psychometric evaluation of the 12-item short-form health survey (SF-12) in osteoarthritis and rheumatoid arthritis clinical trials. Clin. Ther. 2001, 23, 1080–1098. [Google Scholar] [CrossRef] [PubMed]
- Strimpakos, N.; Anastasiadi, E.; Panayiotou, G.; Athanasopoulos, S.; Karteroliotis, K.; Kapreli, E. Greek version of modified Baecke physical activity questionnaire (mBQ): Cross-cultural adaptation and psychometric properties. Physiotherapy 2013, 101, e1446–e1447. [Google Scholar] [CrossRef][Green Version]
- Terwee, C.; Bouwmeester, W.; van Elsland, S.; de Vet, H.; Dekker, J. Instruments to assess physical activity in patients with osteoarthritis of the hip or knee: A systematic review of measurement properties. Osteoarthr. Cartil. 2011, 19, 620–633. [Google Scholar] [CrossRef]
- Areeudomwong, P.; Buttagat, V. Reliability and Validity of the Cross-Culturally Adapted Thai Version of the Tampa Scale for Kinesiophobia in Knee Osteoarthritis Patients. Malays. J. Med. Sci. 2017, 24, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Scopaz, K.A.; Piva, S.R.; Wisniewski, S.; Fitzgerald, G.K. Relationships of Fear, Anxiety, and Depression With Physical Function in Patients With Knee Osteoarthritis. Arch. Phys. Med. Rehabil. 2009, 90, 1866–1873. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed]
- Lyman, S.; Lee, Y.-Y.; McLawhorn, A.S.; Islam, W.; MacLean, C.H. What Are the Minimal and Substantial Improvements in the HOOS and KOOS and JR Versions After Total Joint Replacement? Clin. Orthop. Relat. Res. 2018, 476, 2432–2441. [Google Scholar] [CrossRef]
- Allen, K.; Arbeeva, L.; Callahan, L.; Golightly, Y.; Goode, A.; Heiderscheit, B.; Huffman, K.; Severson, H.; Schwartz, T. Physical therapy vs. internet-based exercise training for patients with knee osteoarthritis: Results of a randomized controlled trial. Osteoarthr. Cartil. 2018, 26, 383–396. [Google Scholar] [CrossRef]
- Moutzouri, M.; Stamouli, A.; Gioftsos, G. Effectiveness of technology-assisted rehabilitation for patients with knee osteoarthritis: A systematic review. In Proceedings of the WCPT Congress 2021, Dubai, United Arab Emirate, 8–10 April 2021. [Google Scholar]
- Bossen, D.; Veenhof, C.; Van Beek, K.E.; Spreeuwenberg, P.M.; Dekker, J.; De Bakker, D.H. Effectiveness of a Web-Based Physical Activity Intervention in Patients With Knee and/or Hip Osteoarthritis: Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e257. [Google Scholar] [CrossRef]
- Yukalang, N.; Turnbul, N.; Thongkum, W.; Wongkongdech, A.; Tudpor, K. Association between Physical Activity and Oste-oarthritis of Knee with Quality of Life in Community-Dwelling Older Adults. pHealth 2021, 285, 265–270. [Google Scholar] [CrossRef]
- Bennell, K.L.; Nelligan, R.; Dobson, F.; Rini, C.; Keefe, F.; Kasza, J.; French, S.; Bryant, C.; Dalwood, A.; Abbott, J.H.; et al. Effectiveness of an Internet-Delivered Exercise and Pain-Coping Skills Training Intervention for Persons With Chronic Knee Pain. Ann. Intern. Med. 2017, 166, 453–462. [Google Scholar] [CrossRef]
- Rini, C.; Porter, L.S.; Somers, T.J.; McKee, D.C.; DeVellis, R.F.; Smith, M.; Winkel, G.; Ahern, D.K.; Goldman, R.; Stiller, J.L.; et al. Automated Internet-based pain coping skills training to manage osteoarthritis pain. Pain 2015, 156, 837–848. [Google Scholar] [CrossRef]
- O’Moore, K.A.; Newby, J.M.; Andrews, G.; Hunter, D.J.; Bennell, K.; Smith, J.; Williams, A.D. Internet Cognitive–Behavioral Therapy for Depression in Older Adults With Knee Osteoarthritis: A Randomized Controlled Trial. Arthritis Care Res. 2017, 70, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Li, L.C.; Sayre, E.C.; Xie, H.; Falck, R.S.; Best, J.R.; Liu-Ambrose, T.; Grewal, N.; Hoens, A.M.; Noonan, G.; Feehan, L.M. Efficacy of a Community-Based Technology-Enabled Physical Activity Counseling Program for People With Knee Osteoarthritis: Proof-of-Concept Study. J. Med. Internet Res. 2018, 20, e159. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Lee, W.-C.; Hsieh, R.-L. Active video games for knee osteoarthritis improve mobility but not WOMAC score: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2020, 63, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Skrepnik, N.; Spitzer, A.; Altman, R.; Hoekstra, J.; Stewart, J.; Toselli, R. Assessing the Impact of a Novel Smartphone Application Compared with Standard Follow-Up on Mobility of Patients with Knee Osteoarthritis Following Treatment with Hylan G-F 20: A Randomized Controlled Trial. JMIR mHealth uHealth 2017, 5, e64. [Google Scholar] [CrossRef]
- Bossen, D.; Buskermolen, M.; Veenhof, C.; de Bakker, D.; Dekker, J. Adherence to a Web-Based Physical Activity Intervention for Patients with Knee and/or Hip Osteoarthritis: A Mixed Method Study. J. Med. Internet Res. 2013, 15, e223. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Dobson, F.; Hinman, R.S. Exercise in osteoarthritis: Moving from prescription to adherence. Best Pract. Res. Clin. Rheumatol. 2014, 28, 93–117. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; Van Gemert-Pijnen, J.E. Persuasive System Design Does Matter: A Systematic Review of Adherence to Web-based Interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef]
- Nelligan, R.K.; Hinman, R.S.; Kasza, J.; Crofts, S.J.C.; Bennell, K.L. Effects of a Self-directed Web-Based Strengthening Exercise and Physical Activity Program Supported by Automated Text Messages for People with Knee Osteoarthritis: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Gorber, S.C.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| BWR-OPA Mean (SD), n = 22 | OPA Mean (SD), n = 22 | ||
|---|---|---|---|
| Age (years) | 65.1 (5.3) | 63.5 (5.6) | |
| Weight (kg) | 74.7 (19.1) | 77.0 (12.7) | |
| Sex (%) | Female | 86.4 | 68.2 |
| Male | 13.6 | 31.8 | |
| Occupation (%) | Housewife | 3.0 (13.6) | 1.0 (5.9) |
| retired | 13.0 (59.1) | 15.0 (68.2) | |
| worker | 6.0 (27.3) | 6.0 (27.3) | |
| Pain NPRS (cm) | 5.5 (0.9) | 5.8 (0.8) | |
| TUG (S) | 11.1 (1.4) | 11.2 (1.9) | |
| PA (LEAS) | 8.6 (1.6) | 9.1 (1.7) | |
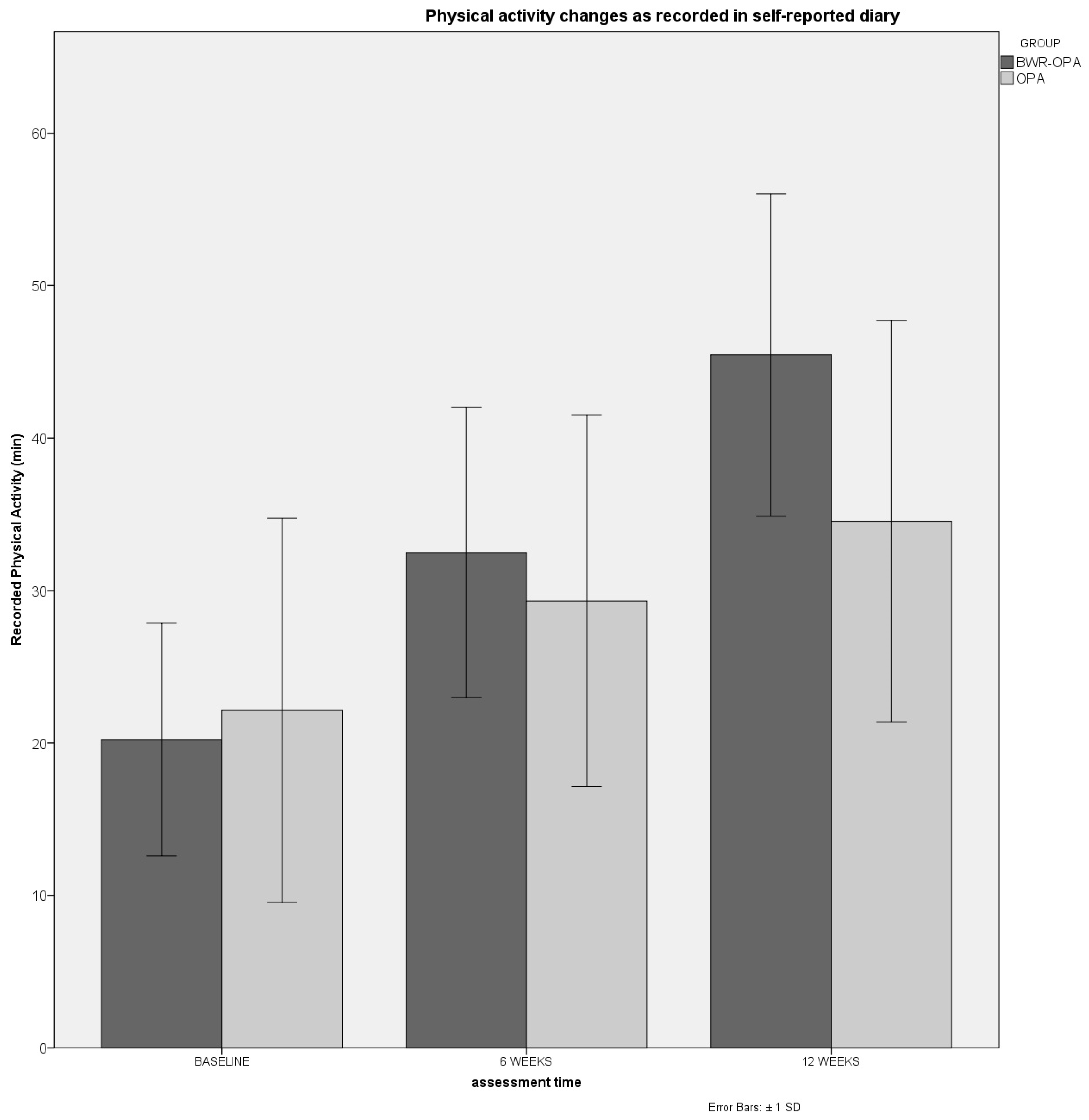
| PA (DIARY) (MIN) | 22.3 (10.1) | 22.1 (16.2) |
| Variable | Group | Baseline | 6th Week | p Value | ES Cohen’s d | 12th Week | p Value | ES Cohen’s d | |
|---|---|---|---|---|---|---|---|---|---|
| Pain | NPRS | BWR-OPA | 5.5 (0.8) | 3.4 (0.8) | ns | 2.6 | 2.4 (1.3) | 0.04 | 3.8 |
| OPA | 5.8 (0.9) | 4.0 (1.2) | 2.0 | 3.2 (1.1) | 2.8 | ||||
| KOOS-P | BWR-OPA | 28.6 (17.9) | 60.0 (15.5) | ns | 1.6 | 76.1 (14.5) | 0.001 | 2.7 | |
| OPA | 32.3 (21.8) | 61.0 (14.8) | 1.3 | 66.9 (12.3) | 1.6 | ||||
| Functionality | KOOS-S | BWR-OPA | 58.8 (16.5) | 66.7 (16.6) | ns | 0.5 | 70.9 (14.8) | 0.005 | 0.7 |
| OPA | 60.2 (16.8) | 66.2 (16.8) | 0.4 | 68.4 (18.5) | 0.5 | ||||
| KOOS-ADL | BWR-OPA | 58.6 (14.4) | 66.0 (18.3) | ns | 0.5 | 70.9 (17.1) | ns | 0.9 | |
| OPA | 61.3 (20.4) | 66.0 (22.0) | 0.2 | 68.5 (20.6) | 0.4 | ||||
| KOOS-SP | BWR-OPA | 28.6 (17.9) | 36.5 (17.4) | ns | 0.4 | 41.3 (15.6) | ns | 0.7 | |
| OPA | 32.3 (21.8) | 40.0 (26.8) | 0.4 | 40.8 (26.8) | 0.4 | ||||
| KOOS-QoL | BWR-OPA | 42.1 (18.7) | 48.6 (18.0) | ns | 0.3 | 58.8 (14.6) | ns | 0.9 | |
| OPA | 42.8 (19.1) | 48.1 (22.1) | 0.3 | 53.7 (17.3) | 0.6 | ||||
| PA | LEAS | BWR-OPA | 8.6 (1.6) | 11.7 (2.8) | 0.001 | 1.9 | 13.5 (1.5) | 0.001 | 3.0 |
| OPA | 9.1 (1.7) | 10.1 (1.7) | 0.6 | 10.2 (1.8) | 0.6 |
| PBOMs | Group | Baseline | 6th Week | p Value | ES Cohen’s d | 12th Week | p Value | ES Cohen’s d |
|---|---|---|---|---|---|---|---|---|
| TUG test (s) | BWR-OPA | 11.1 (1.4) | 9.3 (1.3) | 0.001 | 1.3 | 7.8 (1.0) | 0.001 | 2.4 |
| OPA | 11.2 (1.9) | 10.4 (2.0) | 0.4 | 9.8 (1.9) | 0.7 | |||
| 30s CRT (n) | BWR-OPA | 16.4 (3.9) | 21.4 (5.5) | 0.001 | 1.3 | 24.2 (5.1) | 0.001 | 2.0 |
| OPA | 16.5 (4.8) | 18.1 (4.0) | 0.3 | 19.1 (4.7) | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moutzouri, M.; Koumantakis, G.A.; Hurley, M.; Kladouchou, A.G.; Gioftsos, G. Effectiveness of a Web-Guided Self-Managed Telerehabilitation Program Enhanced with Outdoor Physical Activity on Physical Function, Physical Activity Levels and Pain in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 934. https://doi.org/10.3390/jcm13040934
Moutzouri M, Koumantakis GA, Hurley M, Kladouchou AG, Gioftsos G. Effectiveness of a Web-Guided Self-Managed Telerehabilitation Program Enhanced with Outdoor Physical Activity on Physical Function, Physical Activity Levels and Pain in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(4):934. https://doi.org/10.3390/jcm13040934
Chicago/Turabian StyleMoutzouri, Maria, George A. Koumantakis, Michael Hurley, Aggeliki Georgia Kladouchou, and George Gioftsos. 2024. "Effectiveness of a Web-Guided Self-Managed Telerehabilitation Program Enhanced with Outdoor Physical Activity on Physical Function, Physical Activity Levels and Pain in Patients with Knee Osteoarthritis: A Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 4: 934. https://doi.org/10.3390/jcm13040934
APA StyleMoutzouri, M., Koumantakis, G. A., Hurley, M., Kladouchou, A. G., & Gioftsos, G. (2024). Effectiveness of a Web-Guided Self-Managed Telerehabilitation Program Enhanced with Outdoor Physical Activity on Physical Function, Physical Activity Levels and Pain in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Journal of Clinical Medicine, 13(4), 934. https://doi.org/10.3390/jcm13040934