
Occlusal Caries Detection with Intraoral Scanners in Pediatric Dentistry: A Comparative Clinical Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Group
2.3. Standardization, Calibration and Blinding
2.4. Caries Detection Methods
2.4.1. Visual Examination
2.4.2. Diagnocam
2.4.3. Trios 4
2.4.4. Emerald S
2.5. Statistical Analysis
2.5.1. Reliability
2.5.2. Sensitivity and Specificity
- -
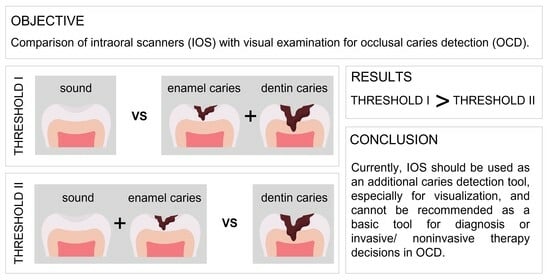
- Threshold I: sound (0) versus overall caries (pooled data of enamel (1) and dentin caries (2)).
- -
- Threshold II: pooled data of sound (0) and enamel caries (1) versus dentin caries (2).
3. Results
3.1. Reliability
3.2. Sensitivity and Specificity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tabatabaian, F.; Namdari, M.; Mahshid, M.; Vora, S.R.; Mirabbasi, S. Accuracy and precision of intraoral scanners for shade matching: A systematic review. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Giese-Kraft, K.; Fischer, M.; Schulze, K.; Schlueter, N.; Ganss, C. Visualization of dental plaque with a 3D-intraoral-scanner-A tool for whole mouth planimetry. PLoS ONE 2022, 17, e0276686. [Google Scholar] [CrossRef] [PubMed]
- Yun, D.; Choi, D.S.; Jang, I.; Cha, B.K. Clinical application of an intraoral scanner for serial evaluation of orthodontic tooth movement: A preliminary study. Korean J. Orthod. 2018, 48, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Angelone, F.; Ponsiglione, A.M.; Ricciardi, C.; Cesarelli, G.; Sansone, M.; Amato, F. Diagnostic Applications of Intraoral Scanners: A Systematic Review. J. Imaging 2023, 9, 134. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Schupp, B.; Schmidt, A.; Wöstmann, B.; Baresel, I.; Krämer, N.; Schulz-Weidner, N. New Caries Diagnostic Tools in Intraoral Scanners: A Comparative In Vitro Study to Established Methods in Permanent and Primary Teeth. Sensors 2022, 22, 2156. [Google Scholar] [CrossRef]
- Poorterman, J.H.; Aartman, I.H.; Kalsbeek, H. Underestimation of the prevalence of approximal caries and inadequate restorations in a clinical epidemiological study. Community Dent. Oral Epidemiol. 1999, 27, 331–337. [Google Scholar] [CrossRef]
- Poorterman, J.H.; Aartman, I.H.; Kieft, J.A.; Kalsbeek, H. Value of bite-wing radiographs in a clinical epidemiological study and their effect on the DMFS index. Caries Res. 2000, 34, 159–163. [Google Scholar] [CrossRef]
- Schaefer, G.; Pitchika, V.; Litzenburger, F.; Hickel, R.; Kühnisch, J. Evaluation of occlusal caries detection and assessment by visual inspection, digital bitewing radiography and near-infrared light transillumination. Clin. Oral Investig. 2018, 22, 2431–2438. [Google Scholar] [CrossRef]
- Schwendicke, F.; Splieth, C.; Breschi, L.; Banerjee, A.; Fontana, M.; Paris, S.; Burrow, M.F.; Crombie, F.; Page, L.F.; Gatón-Hernández, P.; et al. When to intervene in the caries process? An expert Delphi consensus statement. Clin. Oral Investig. 2019, 23, 3691–3703. [Google Scholar] [CrossRef]
- Kühnisch, J.; Ekstrand, K.R.; Pretty, I.; Twetman, S.; van Loveren, C.; Gizani, S.; Spyridonos Loizidou, M. Best clinical practice guidance for management of early caries lesions in children and young adults: An EAPD policy document. Eur. Arch. Paediatr. Dent. 2016, 17, 3–12. [Google Scholar] [CrossRef]
- Atena, G.; Daniela, J.; Aurora Doris, F. Caries Management Aided by Fluorescence-Based Devices. In Dental Caries; IntechOpen: Rijeka, Croatia, 2022. [Google Scholar]
- Kühnisch, J.; Bücher, K.; Henschel, V.; Albrecht, A.; Garcia-Godoy, F.; Mansmann, U.; Hickel, R.; Heinrich-Weltzien, R. Diagnostic performance of the universal visual scoring system (UniViSS) on occlusal surfaces. Clin. Oral Investig. 2011, 15, 215–223. [Google Scholar] [CrossRef]
- Söchtig, F.; Hickel, R.; Kühnisch, J. Caries detection and diagnostics with near-infrared light transillumination: Clinical experiences. Quintessence Int. 2014, 45, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Sürme, K.; Kara, N.B.; Yilmaz, Y. In Vitro Evaluation of Occlusal Caries Detection Methods in Primary and Permanent Teeth: A Comparison of CarieScan PRO, DIAGNOdent Pen, and DIAGNOcam Methods. Photobiomodul. Photomed. Laser Surg. 2020, 38, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Kapor, S.; Rankovic, M.J.; Khazaei, Y.; Crispin, A.; Schüler, I.; Krause, F.; Lussi, A.; Neuhaus, K.; Eggmann, F.; Michou, S.; et al. Systematic review and meta-analysis of diagnostic methods for occlusal surface caries. Clin. Oral Investig. 2021, 25, 4801–4815. [Google Scholar] [CrossRef] [PubMed]
- Lennon, Á.M.; Brune, L.; Techert, S.; Buchalla, W. Fluorescence Spectroscopy Shows Porphyrins Produced by Cultured Oral Bacteria Differ Depending on Composition of Growth Media. Caries Res. 2023, 57, 74–86. [Google Scholar] [CrossRef]
- Braga, M.M.; de Benedetto, M.S.; Imparato, J.C.; Mendes, F.M. New methodology to assess activity status of occlusal caries in primary teeth using laser fluorescence device. J. Biomed. Opt. 2010, 15, 047005. [Google Scholar] [CrossRef][Green Version]
- Matos, R.; Novaes, T.F.; Braga, M.M.; Siqueira, W.L.; Duarte, D.A.; Mendes, F.M. Clinical performance of two fluorescence-based methods in detecting occlusal caries lesions in primary teeth. Caries Res. 2011, 45, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Tassoker, M.; Ozcan, S.; Karabekiroglu, S. Occlusal Caries Detection and Diagnosis Using Visual ICDAS Criteria, Laser Fluorescence Measurements, and Near-Infrared Light Transillumination Images. Med. Princ. Pract. 2019, 29, 25–31. [Google Scholar] [CrossRef]
- Lussi, A.; Megert, B.; Longbottom, C.; Reich, E.; Francescut, P. Clinical performance of a laser fluorescence device for detection of occlusal caries lesions. Eur. J. Oral Sci. 2001, 109, 14–19. [Google Scholar] [CrossRef]
- BaniHani, A.; Santamaría, R.M.; Hu, S.; Maden, M.; Albadri, S. Minimal intervention dentistry for managing carious lesions into dentine in primary teeth: An umbrella review. Eur. Arch. Paediatr. Dent. 2022, 23, 667–693. [Google Scholar] [CrossRef]
- Metzger, Z.; Colson, D.G.; Bown, P.; Weihard, T.; Baresel, I.; Nolting, T. Reflected near-infrared light versus bite-wing radiography for the detection of proximal caries: A multicenter prospective clinical study conducted in private practices. J. Dent. 2022, 116, 103861. [Google Scholar] [CrossRef]
- Pieper, K.; Blumenstein, A. Die Zahnmedizinische Untersuchung Im Rahmen Der Gruppenprophylaxe: Ein Leitfaden Für Die Edv-Gestützte Erfolgskontrolle; Druckhaus Marburg: Marburg, Germany, 1993. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral. Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef]
- Michou, S.; Lambach, M.S.; Ntovas, P.; Benetti, A.R.; Bakhshandeh, A.; Rahiotis, C.; Ekstrand, K.R.; Vannahme, C. Author Correction: Automated caries detection in vivo using a 3D intraoral scanner. Sci. Rep. 2022, 12, 13240. [Google Scholar] [CrossRef]
- Walsh, L. Caries Diagnosis Aided by Fluorescence. In Dental Caries; IntechOpen: Rijeka, Croatia, 2018. [Google Scholar]
- Karlsson, L. Caries Detection Methods Based on Changes in Optical Properties between Healthy and Carious Tissue. Int. J. Dent. 2010, 2010, 270729. [Google Scholar] [CrossRef]
- Jablonski-Momeni, A.; Jablonski, B.; Lippe, N. Clinical performance of the near-infrared imaging system VistaCam iX Proxi for detection of approximal enamel lesions. BDJ Open 2017, 3, 17012. [Google Scholar] [CrossRef]
- Gwet, K.L. Computing inter-rater reliability and its variance in the presence of high agreement. Br. J. Math. Stat. Psychol. 2008, 61, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; Wiley: Hoboken, NJ, USA, 2000. [Google Scholar]
- Diniz, M.B.; Boldieri, T.; Rodrigues, J.A.; Santos-Pinto, L.; Lussi, A.; Cordeiro, R.C. The performance of conventional and fluorescence-based methods for occlusal caries detection: An in vivo study with histologic validation. J. Am. Dent. Assoc. 2012, 143, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.S.; Alfaraj, A.; Lippert, F.; Yang, C.C. Performance of the caries diagnosis feature of intraoral scanners and near-infrared imaging technology-A narrative review. J. Prosthodont. 2023, 32, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Stookey, G.K. Quantitative light fluorescence: A technology for early monitoring of the caries process. Dent. Clin. N. Am. 2005, 49, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Qudeimat, M.A.; Alomari, Q.D.; Altarakemah, Y.; Alshawaf, N.; Honkala, E.J. Variables affecting the inter- and intra-examiner reliability of ICDAS for occlusal caries diagnosis in permanent molars. J. Public Health Dent. 2016, 76, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Kühnisch, J.; Berger, S.; Goddon, I.; Senkel, H.; Pitts, N.; Heinrich-Weltzien, R. Occlusal caries detection in permanent molars according to WHO basic methods, ICDAS II and laser fluorescence measurements. Community Dent. Oral Epidemiol. 2008, 36, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Kopycka-Kedzierawski, D.T.; McLaren, S.W.; Billings, R.J. Advancement Of Teledentistry At The University Of Rochester’s Eastman Institute For Oral Health. Health Aff. 2018, 37, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Jan, J.; Bakar, W.Z.W.; Mathews, S.; Uzamere, E.; Okoye, L.; Amaechi, B. Clinical Trial of the Canary System for Proximal Caries Detection: A Comparative Study. CJAST 2021, 40, 38–50. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Teeth | Permanent Teeth | ||||||
|---|---|---|---|---|---|---|---|
| Threshold | Caries Detection Method | Sensitivity | Specificity | AUC | Sensitivity | Specificity | AUC |
| I | Diagnocam | 0.934 | 0.873 | 0.903 | 0.938 | 0.876 | 0.907 |
| Trios 4 | 0.840 | 0.804 | 0.822 | 0.887 | 0.765 | 0.826 | |
| Emerald S | 0.925 | 0.876 | 0.900 | 0.938 | 0.872 | 0.907 | |
| II | Diagnocam | 0.691 | 0.979 | 0.835 | 0.836 | 0.974 | 0.905 |
| Trios 4 | 0.589 | 0.980 | 0.784 | 0.655 | 0.977 | 0.816 | |
| Emerald S | 0.737 | 0.976 | 0.857 | 0.810 | 0.976 | 0.893 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz-Weidner, N.; Gruber, M.; Wöstmann, B.; Uebereck, C.F.; Krämer, N.; Schlenz, M.A. Occlusal Caries Detection with Intraoral Scanners in Pediatric Dentistry: A Comparative Clinical Study. J. Clin. Med. 2024, 13, 925. https://doi.org/10.3390/jcm13040925
Schulz-Weidner N, Gruber M, Wöstmann B, Uebereck CF, Krämer N, Schlenz MA. Occlusal Caries Detection with Intraoral Scanners in Pediatric Dentistry: A Comparative Clinical Study. Journal of Clinical Medicine. 2024; 13(4):925. https://doi.org/10.3390/jcm13040925
Chicago/Turabian StyleSchulz-Weidner, Nelly, Marina Gruber, Bernd Wöstmann, Constanze Friederike Uebereck, Norbert Krämer, and Maximiliane Amelie Schlenz. 2024. "Occlusal Caries Detection with Intraoral Scanners in Pediatric Dentistry: A Comparative Clinical Study" Journal of Clinical Medicine 13, no. 4: 925. https://doi.org/10.3390/jcm13040925
APA StyleSchulz-Weidner, N., Gruber, M., Wöstmann, B., Uebereck, C. F., Krämer, N., & Schlenz, M. A. (2024). Occlusal Caries Detection with Intraoral Scanners in Pediatric Dentistry: A Comparative Clinical Study. Journal of Clinical Medicine, 13(4), 925. https://doi.org/10.3390/jcm13040925