
Hypertension and Dental Implants: A Systematic Review and Meta-Analysis



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Objective
2.2. Search Strategies
2.3. Inclusion and Exclusion Criteria
2.4. Study Selection
2.5. Quality Assessment
2.6. Definitions
2.7. Data Extraction
2.8. Meta-Analysis
3. Results
3.1. Literature Search
3.2. Description of the Studies
3.3. Quality Assessment
3.4. Meta-Analysis
3.5. Meta-Regression

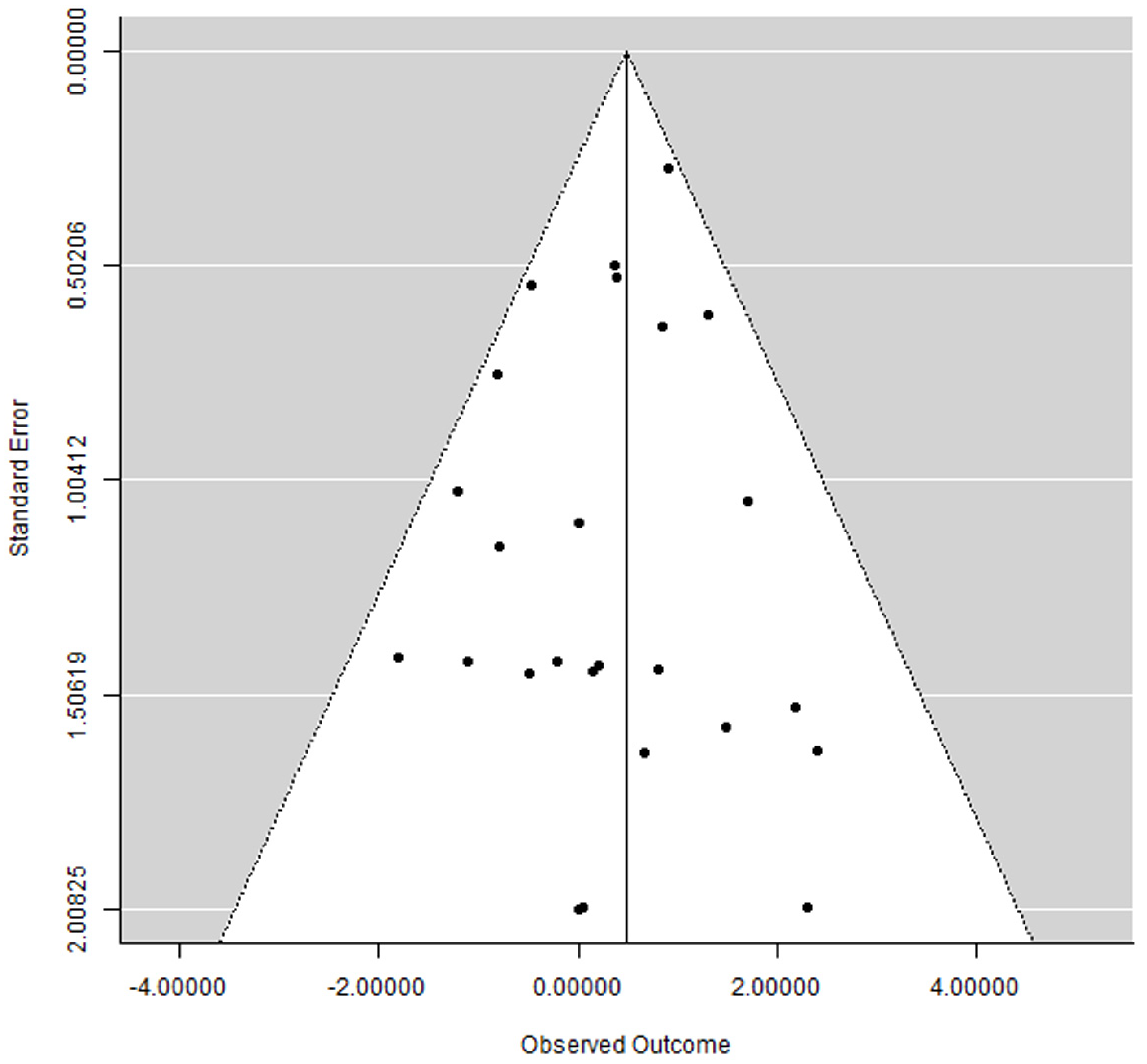
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Hypertension. Available online: https://www.who.int/health-topics/hypertension (accessed on 2 August 2023).
- NCD Risk Factor Collaboration. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- El-Bikai, R.; Tahir, M.R.; Tremblay, J.; Joffres, M.; Šeda, O.; Šedová, L.; Awadalla, P.; Laberge, C.; Knoppers, B.M.; Dumas, P.; et al. Association of age-dependent height and bone mineral density decline with increased arterial stiffness and rate of fractures in hypertensive individuals. J. Hypertens. 2015, 33, 727–735; discussion 735. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Hsu, J.F.; Jee, W.S.; Matthews, J.L. Evidence for reduced cancellous bone mass in the spontaneously hypertensive rat. Bone Miner. 1993, 20, 251–264. [Google Scholar] [CrossRef]
- Humar, R.; Zimmerli, L.; Battegay, E. Angiogenesis and hypertension: An update. J. Hum. Hypertens. 2009, 23, 773–782. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontol. 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Saghiri, M.A.; Asatourian, A.; Garcia-Godoy, F.; Sheibani, N. The role of angiogenesis in implant dentistry part I: Review of titanium alloys, surface characteristics and treatments. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e514–e525. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Amato, A.; Chiacchio, A.; Sisalli, L.; Giordano, F. Do Systemic Diseases and Medications Influence Dental Implant Osseointegration and Dental Implant Health? An Umbrella Review. Dent. J. 2023, 11, 146. [Google Scholar] [CrossRef]
- Belbasis, L.; Bellou, V.; Ioannidis, J.P.A. Conducting umbrella reviews. BMJ Med. 2022, 1, e000071. [Google Scholar] [CrossRef]
- Mishra, S.K.; Sonnahalli, N.K.; Chowdhary, R. Do antihypertensive medications have an effect on dental implants? A systematic review. Oral Maxillofac. Surg. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- NIH. Quality Assessment Tool for Case Series Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 15 January 2020).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Schmid, J. Pathogenesis of implant failures. Periodontol. 2000 1994, 4, 127–138. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing the fracture of dental implants. Clin. Implant. Dent. Relat. Res. 2018, 20, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D. Principles of and procedures for systematic reviews. In Systematic Reviews in Health Care: Meta-Analysis in Context; Egger, M., Smith, G.D., Altman, D.G., Eds.; BMJ Books: London, UK, 2003; pp. 23–42. [Google Scholar]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef]
- Wallace, B.C.; Lajeunesse, M.J.; Dietz, G.; Dahabreh, I.J.; Trikalinos, T.A.; Schmid, C.H.; Gurevitch, J. OpenMEE: Intuitive, open-source software for meta-analysis in ecology and evolutionary biology. Methods Ecol. Evol. 2017, 8, 941–947. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implant. Res. 2008, 19, 670–676. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Michiles, K.; Teughels, W.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of failures up to abutment connection with modified surface oral implants. J. Clin. Periodontol. 2008, 35, 51–57. [Google Scholar] [CrossRef]
- Altay, M.A.; Tozoğlu, S.; Yıldırımyan, N.; Özarslan, M.M. Is History of Periodontitis a Risk Factor for Peri-implant Disease? A Pilot Study. Int. J. Oral Maxillofac. Implant. 2018, 33, 152–160. [Google Scholar] [CrossRef]
- Bertl, K.; Ebner, M.; Knibbe, M.; Pandis, N.; Kuchler, U.; Ulm, C.; Stavropoulos, A. How old is old for implant therapy in terms of early implant losses? J. Clin. Periodontol. 2019, 46, 1282–1293. [Google Scholar] [CrossRef]
- Cabrera-Domínguez, J.; Castellanos-Cosano, L.; Torres-Lagares, D.; Machuca-Portillo, G. A Prospective Case-Control Clinical Study of Titanium-Zirconium Alloy Implants with a Hydrophilic Surface in Patients with Type 2 Diabetes Mellitus. Int. J. Oral Maxillofac. Implant. 2017, 32, 1135–1144. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Analysis of risk factors for cluster behavior of dental implant failures. Clin. Implant. Dent. Relat. Res. 2017, 19, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Coskunses, F.M.; Tak, Ö. Clinical performance of narrow-diameter titanium-zirconium implants in immediately loaded fixed full-arch prostheses: A 2-year clinical study. Int. J. Implant. Dent. 2021, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Grandi, T.; Guazzi, P.; Samarani, R.; Garuti, G.; Grandi, G. Immediate loading of two unsplinted implants retaining the existing complete mandibular denture in elderly edentulous patients: 1-year results from a multicentre prospective cohort study. Eur. J. Oral Implantol. 2012, 5, 61–68. [Google Scholar]
- Grandi, T.; Guazzi, P.; Samarani, R.; Grandi, G. Immediate loading of four (all-on-4) post-extractive implants supporting mandibular cross-arch fixed prostheses: 18-month follow-up from a multicentre prospective cohort study. Eur. J. Oral Implantol. 2012, 5, 277–285. [Google Scholar] [PubMed]
- Krennmair, S.; Weinländer, M.; Forstner, T.; Krennmair, G.; Stimmelmayr, M. Factors affecting peri-implant bone resorption in four Implant supported mandibular full-arch restorations: A 3-year prospective study. J. Clin. Periodontol. 2016, 43, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.T.; Tran, D.; Jeng, M.D.; Shen, Y.T. Survival rates of hybrid rough surface implants and their alveolar bone level alterations. J. Periodontol. 2018, 89, 1390–1399. [Google Scholar] [CrossRef]
- Lee, K.J.; Cha, J.K.; Sanz-Martin, I.; Sanz, M.; Jung, U.W. A retrospective case series evaluating the outcome of implants with low primary stability. Clin. Oral Implant. Res. 2019, 30, 861–871. [Google Scholar] [CrossRef]
- Lobato, R.P.B.; Kinalski, M.A.; Martins, T.M.; Agostini, B.A.; Bergoli, C.D.; Dos Santos, M.B.F. Influence of low-level laser therapy on implant stability in implants placed in fresh extraction sockets: A randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 261–269. [Google Scholar] [CrossRef]
- Malo, P.; de Araujo Nobre, M.; Lopes, A.; Ferro, A.; Botto, J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A longitudinal study with 10 to 18 years of follow-up. Clin. Implant. Dent. Relat. Res. 2019, 21, 565–577. [Google Scholar] [CrossRef]
- Malo, P.; de Araujo Nobre, M.; Lopes, A.; Ferro, A.; Nunes, M. The All-on-4 concept for full-arch rehabilitation of the edentulous maxillae: A longitudinal study with 5-13 years of follow-up. Clin. Implant. Dent. Relat. Res. 2019, 21, 538–549. [Google Scholar] [CrossRef]
- Moy, P.K.; Medina, D.; Shetty, V.; Aghaloo, T.L. Dental implant failure rates and associated risk factors. Int. J. Oral Maxillofac. Implant. 2005, 20, 569–577. [Google Scholar]
- Park, J.C.; Baek, W.S.; Choi, S.H.; Cho, K.S.; Jung, U.W. Long-term outcomes of dental implants placed in elderly patients: A retrospective clinical and radiographic analysis. Clin. Oral Implant. Res. 2017, 28, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Song, Y.W.; Sanz-Martin, I.; Cha, J.K.; Lee, J.S.; Jung, U.W. Clinical benefits of ridge preservation for implant placement compared to natural healing in maxillary teeth: A retrospective study. J. Clin. Periodontol. 2020, 47, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Ofec, R.; Eliyahu, G.; Ruban, A.; Sterer, N. Long Term Follow-Up of Dental Implants Placed in Autologous Onlay Bone Graft. Clin. Implant. Dent. Relat. Res. 2016, 18, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Seki, K.; Hasuike, A.; Iwano, Y.; Hagiwara, Y. Influence of antihypertensive medications on the clinical parameters of anodized dental implants: A retrospective cohort study. Int. J. Implant. Dent. 2020, 6, 32. [Google Scholar] [CrossRef]
- Simons, W.F.; De Smit, M.; Duyck, J.; Coucke, W.; Quirynen, M. The proportion of cancellous bone as predictive factor for early marginal bone loss around implants in the posterior part of the mandible. Clin. Oral Implant. Res. 2015, 26, 1051–1059. [Google Scholar] [CrossRef]
- Singh, R.; Parihar, A.S.; Vaibhav, V.; Kumar, K.; Singh, R.; Jerry, J.J. A 10 years retrospective study of assessment of prevalence and risk factors of dental implants failures. J. Fam. Med. Prim. Care 2020, 9, 1617–1619. [Google Scholar] [CrossRef]
- Wang, J.; Lerman, G.; Bittner, N.; Fan, W.; Lalla, E.; Papapanou, P.N. Immediate versus delayed temporization at posterior single implant sites: A randomized controlled trial. J. Clin. Periodontol. 2020, 47, 1281–1291. [Google Scholar] [CrossRef]
- Wu, X.; Al-Abedalla, K.; Eimar, H.; Arekunnath Madathil, S.; Abi-Nader, S.; Daniel, N.G.; Nicolau, B.; Tamimi, F. Antihypertensive Medications and the Survival Rate of Osseointegrated Dental Implants: A Cohort Study. Clin. Implant. Dent. Relat. Res. 2016, 18, 1171–1182. [Google Scholar] [CrossRef]
- Perez-Castrillon, L.J.; Justo, I.; Sanz-Cantalapiedra, A.; Pueyo, C.; Hernandez, G.; Duenas, A. Effect of the Antihypertensive Treatment on the Bone Mineral Density and Osteoporotic Fracture. Curr. Hypertens. Rev. 2005, 1, 61–66. [Google Scholar] [CrossRef]
- Bellido, T.; Saini, V.; Pajevic, P.D. Effects of PTH on osteocyte function. Bone 2013, 54, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Schleithoff, S.S.; Koerfer, R. Putting cardiovascular disease and vitamin D insufficiency into perspective. Br. J. Nutr. 2005, 94, 483–492. [Google Scholar] [CrossRef]
- London, G.M.; Guérin, A.P.; Verbeke, F.H.; Pannier, B.; Boutouyrie, P.; Marchais, S.J.; Mëtivier, F. Mineral metabolism and arterial functions in end-stage renal disease: Potential role of 25-hydroxyvitamin D deficiency. J. Am. Soc. Nephrol. 2007, 18, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Mosekilde, L. Vitamin D and the elderly. Clin. Endocrinol. 2005, 62, 265–281. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Yang, K.; Hu, Z.; Li, M.; Wei, H.; Tang, Z.; Chen, B.; Su, C.; Cai, D.; Xu, J. Determining the association between hypertension and bone metabolism markers in osteoporotic patients. Medicine 2021, 100, e26276. [Google Scholar] [CrossRef]
- Manrique, N.; Pereira, C.C.; Luvizuto, E.R.; Sánchez Mdel, P.; Okamoto, T.; Okamoto, R.; Sumida, D.H.; Antoniali, C. Hypertension modifies OPG, RANK, and RANKL expression during the dental socket bone healing process in spontaneously hypertensive rats. Clin. Oral Investig. 2015, 19, 1319–1327. [Google Scholar] [CrossRef]
- Shalhoub, V.; Faust, J.; Boyle, W.J.; Dunstan, C.R.; Kelley, M.; Kaufman, S.; Scully, S.; Van, G.; Lacey, D.L. Osteoprotegerin and osteoprotegerin ligand effects on osteoclast formation from human peripheral blood mononuclear cell precursors. J. Cell Biochem. 1999, 72, 251–261. [Google Scholar] [CrossRef]
- Suda, T.; Takahashi, N.; Udagawa, N.; Jimi, E.; Gillespie, M.T.; Martin, T.J. Modulation of osteoclast differentiation and function by the new members of the tumor necrosis factor receptor and ligand families. Endocr. Rev. 1999, 20, 345–357. [Google Scholar] [CrossRef]
- Simonet, W.S.; Lacey, D.L.; Dunstan, C.R.; Kelley, M.; Chang, M.S.; Lüthy, R.; Nguyen, H.Q.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: A novel secreted protein involved in the regulation of bone density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef]
- Prewitt, R.L.; Chen, I.I.; Dowell, R. Development of microvascular rarefaction in the spontaneously hypertensive rat. Am. J. Physiol. 1982, 243, H243–H251. [Google Scholar] [CrossRef]
- Hutchins, P.M.; Darnell, A.E. Observations of a decreased number of small arterioles in spontaneously hypertensive rats. Circ. Res. 1974, 34–35, 161–165. [Google Scholar]
- Sokolova, I.A.; Manukhina, E.B.; Blinkov, S.M.; Koshelev, V.B.; Pinelis, V.G.; Rodionov, I.M. Rarefication of the arterioles and capillary network in the brain of rats with different forms of hypertension. Microvasc. Res. 1985, 30, 1–9. [Google Scholar] [CrossRef]
- Antonios, T.F.; Singer, D.R.; Markandu, N.D.; Mortimer, P.S.; MacGregor, G.A. Structural skin capillary rarefaction in essential hypertension. Hypertension 1999, 33, 998–1001. [Google Scholar] [CrossRef] [PubMed]
- Hansen-Smith, F.M.; Morris, L.W.; Greene, A.S.; Lombard, J.H. Rapid microvessel rarefaction with elevated salt intake and reduced renal mass hypertension in rats. Circ. Res. 1996, 79, 324–330. [Google Scholar] [CrossRef]
- Serné, E.H.; Gans, R.O.; ter Maaten, J.C.; Tangelder, G.J.; Donker, A.J.; Stehouwer, C.D. Impaired skin capillary recruitment in essential hypertension is caused by both functional and structural capillary rarefaction. Hypertension 2001, 38, 238–242. [Google Scholar] [CrossRef]
- Kang, K.Y.; Kang, Y.; Kim, M.; Kim, Y.; Yi, H.; Kim, J.; Jung, H.R.; Park, S.H.; Kim, H.Y.; Ju, J.H.; et al. The effects of antihypertensive drugs on bone mineral density in ovariectomized mice. J. Korean Med. Sci. 2013, 28, 1139–1144. [Google Scholar] [CrossRef]
- Ma, L.; Ji, J.L.; Ji, H.; Yu, X.; Ding, L.J.; Liu, K.; Li, Y.Q. Telmisartan alleviates rosiglitazone-induced bone loss in ovariectomized spontaneous hypertensive rats. Bone 2010, 47, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Ames, R.W.; Orr-Walker, B.J.; Clearwater, J.M.; Horne, A.M.; Evans, M.C.; Murray, M.A.; McNeil, A.R.; Gamble, G.D. Hydrochlorothiazide reduces loss of cortical bone in normal postmenopausal women: A randomized controlled trial. Am. J. Med. 2000, 109, 362–370. [Google Scholar] [CrossRef]
- Ott, S.M.; LaCroix, A.Z.; Scholes, D.; Ichikawa, L.E.; Wu, K. Effects of three years of low-dose thiazides on mineral metabolism in healthy elderly persons. Osteoporos. Int. 2008, 19, 1315–1322. [Google Scholar] [CrossRef]
- Bolland, M.J.; Ames, R.W.; Horne, A.M.; Orr-Walker, B.J.; Gamble, G.D.; Reid, I.R. The effect of treatment with a thiazide diuretic for 4 years on bone density in normal postmenopausal women. Osteoporos. Int. 2007, 18, 479–486. [Google Scholar] [CrossRef]
- de Vries, F.; Pouwels, S.; Bracke, M.; Leufkens, H.G.; Cooper, C.; Lammers, J.W.; van Staa, T.P. Use of beta-2 agonists and risk of hip/femur fracture: A population-based case-control study. Pharmacoepidemiol. Drug Saf. 2007, 16, 612–619. [Google Scholar] [CrossRef]
- Levasseur, R.; Dargent-Molina, P.; Sabatier, J.P.; Marcelli, C.; Bréart, G. Beta-blocker use, bone mineral density, and fracture risk in older women: Results from the Epidemiologie de l’Osteoporose prospective study. J. Am. Geriatr. Soc. 2005, 53, 550–552. [Google Scholar] [CrossRef]
- Reid, I.R.; Gamble, G.D.; Grey, A.B.; Black, D.M.; Ensrud, K.E.; Browner, W.S.; Bauer, D.C. beta-Blocker use, BMD, and fractures in the study of osteoporotic fractures. J. Bone Miner. Res. 2005, 20, 613–618. [Google Scholar] [CrossRef]
- Rejnmark, L.; Vestergaard, P.; Kassem, M.; Christoffersen, B.R.; Kolthoff, N.; Brixen, K.; Mosekilde, L. Fracture risk in perimenopausal women treated with beta-blockers. Calcif. Tissue Int. 2004, 75, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Canoy, D.; Harvey, N.C.; Prieto-Alhambra, D.; Cooper, C.; Meyer, H.E.; Åsvold, B.O.; Nazarzadeh, M.; Rahimi, K. Elevated blood pressure, antihypertensive medications and bone health in the population: Revisiting old hypotheses and exploring future research directions. Osteoporos. Int. 2022, 33, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Al Ansari, Y.; Shahwan, H.; Chrcanovic, B.R. Diabetes Mellitus and Dental Implants: A Systematic Review and Meta-Analysis. Materials 2022, 15, 3227. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Dental Implants in Patients Receiving Chemotherapy: A Meta-Analysis. Implant. Dent. 2016, 25, 261–271. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Is the intake of selective serotonin reuptake inhibitors associated with an increased risk of dental implant failure? Int. J. Oral Maxillofac. Surg. 2017, 46, 782–788. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Intake of Proton Pump Inhibitors Is Associated with an Increased Risk of Dental Implant Failure. Int. J. Oral Maxillofac. Implant. 2017, 32, 1097–1102. [Google Scholar] [CrossRef]
- Häggman-Henrikson, B.; Ali, D.; Aljamal, M.; Chrcanovic, B.R. Bruxism and dental implants: A systematic review and meta-analysis. J. Oral Rehabil. 2023, 51, 202–217. [Google Scholar] [CrossRef]
- Mustapha, A.D.; Salame, Z.; Chrcanovic, B.R. Smoking and Dental Implants: A Systematic Review and Meta-Analysis. Medicina 2021, 58, 39. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, N.; Fadhul, F.; Chrcanovic, B.R. Bisphosphonates and Dental Implants: A Systematic Review and Meta-Analysis. Materials 2023, 16, 6078. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Dental implants in irradiated versus nonirradiated patients: A meta-analysis. Head Neck 2016, 38, 448–481. [Google Scholar] [CrossRef] [PubMed]
- Bredberg, C.; Vu, C.; Häggman-Henrikson, B.; Chrcanovic, B.R. Marginal bone loss around dental implants: Comparison between matched groups of bruxer and non-bruxer patients: A retrospective case-control study. Clin. Implant. Dent. Relat. Res. 2023, 25, 124–132. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Impact of Different Surgeons on Dental Implant Failure. Int. J. Prosthodont. 2017, 30, 445–454. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamadé, L.; El-Disoki, S.; Chrcanovic, B.R. Hypertension and Dental Implants: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 499. https://doi.org/10.3390/jcm13020499
Hamadé L, El-Disoki S, Chrcanovic BR. Hypertension and Dental Implants: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(2):499. https://doi.org/10.3390/jcm13020499
Chicago/Turabian StyleHamadé, Liljan, Salma El-Disoki, and Bruno Ramos Chrcanovic. 2024. "Hypertension and Dental Implants: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 2: 499. https://doi.org/10.3390/jcm13020499
APA StyleHamadé, L., El-Disoki, S., & Chrcanovic, B. R. (2024). Hypertension and Dental Implants: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(2), 499. https://doi.org/10.3390/jcm13020499