

The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia

 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion
2.3. Definitions for Severe COVID-19 Pneumonia
2.4. Clinical and Laboratory Investigations
2.5. Study Outcomes
2.6. Statistical Analysis
2.6.1. Determination of Candidate Prognostic Factors
2.6.2. NEWS2 and NEWS2 Plus Scoring Assignment
2.6.3. Model Performances of NEWS2 and NEWS2 Plus
3. Results
3.1. Demographic and Clinical Features
3.2. Treatment, Complications, and Outcomes of the Patients
3.3. Prognostic Factors for Severe COVID-19 Pneumonia: NEWS2 and Others
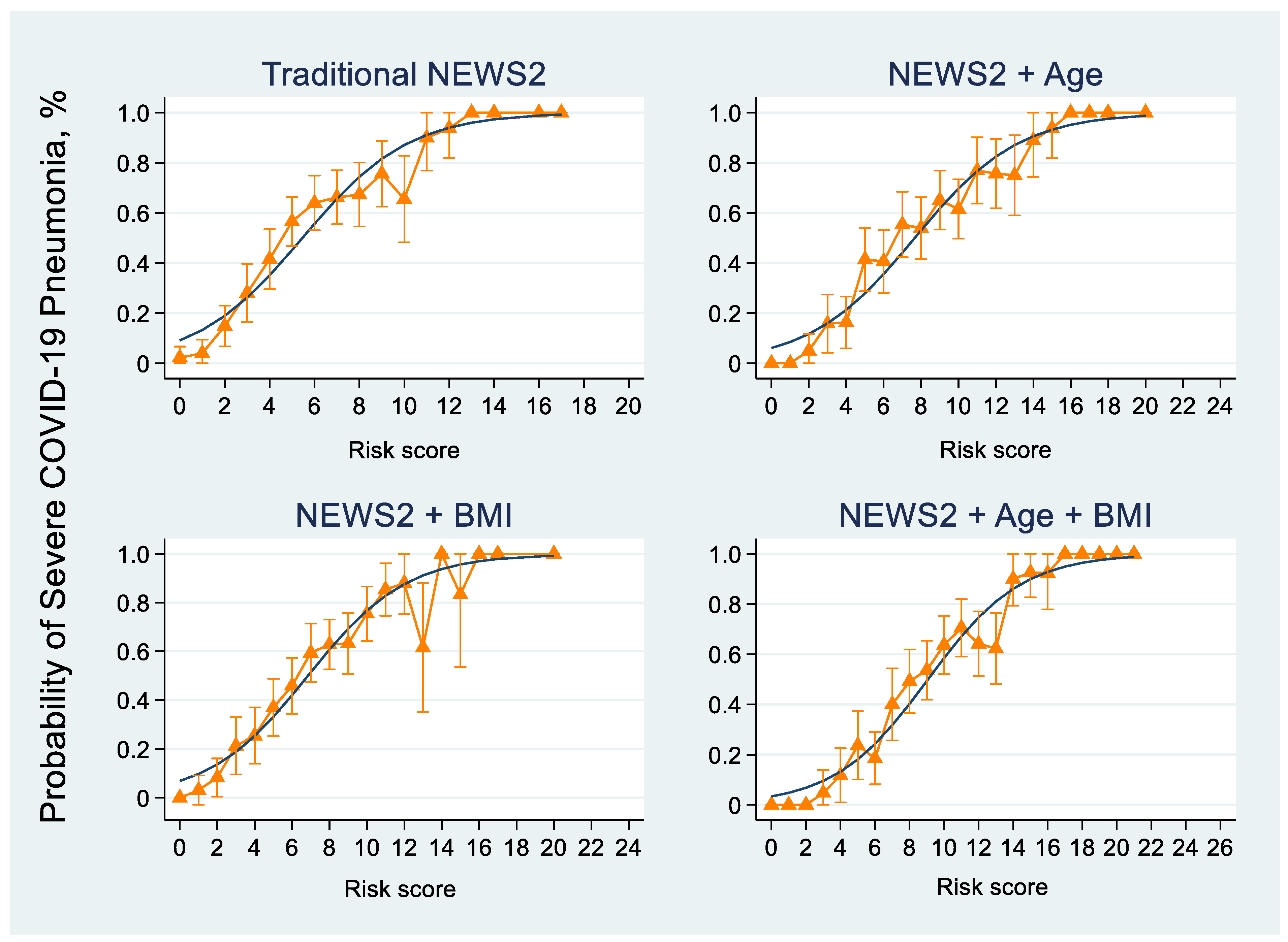
3.4. NEWS2 and NEWS2 Plus Models to Determine Severe COVID-19 Pneumonia
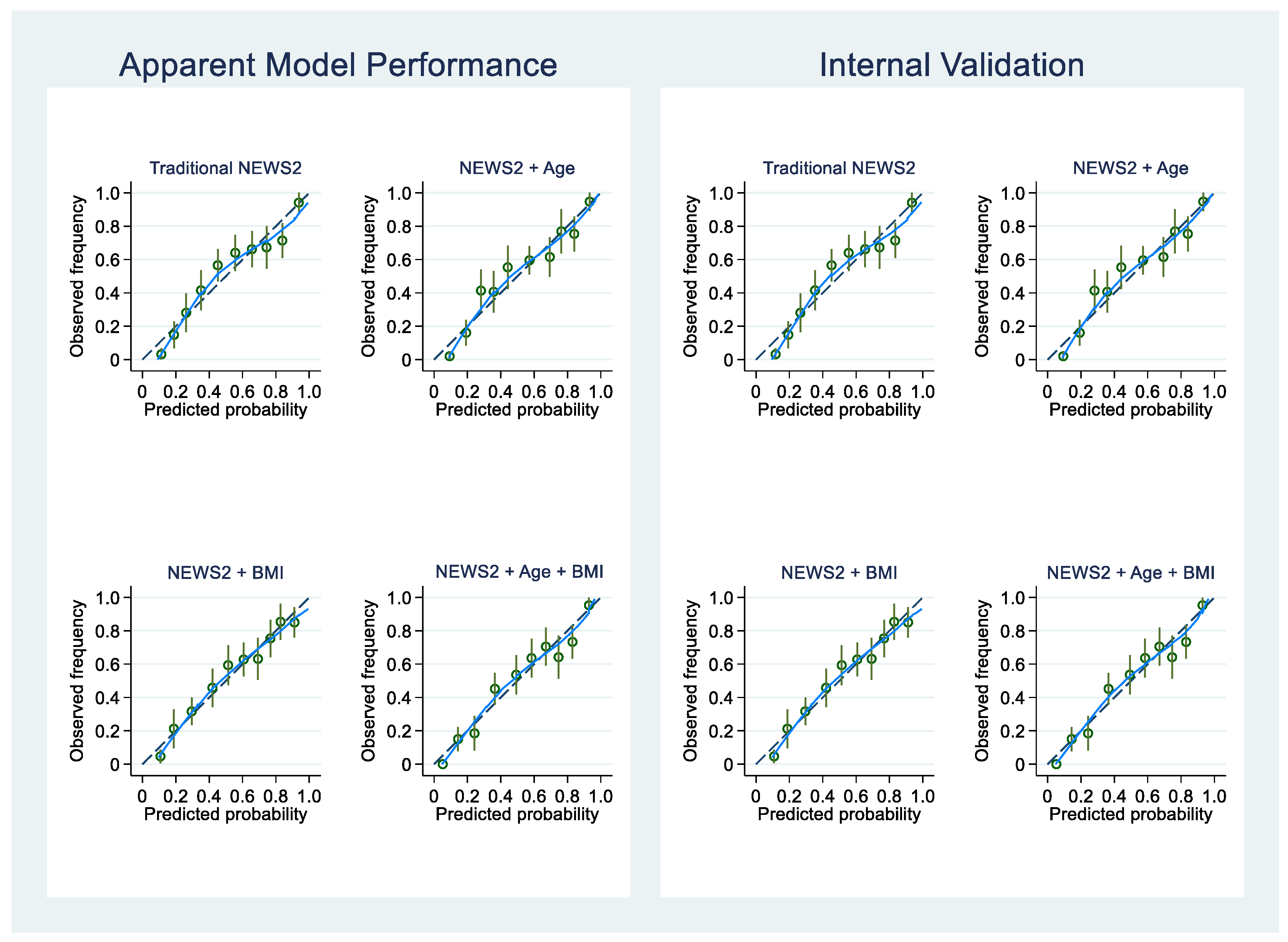
3.5. The Performance of NEWS2 and NEWS2 Plus Models
3.6. Diagnostic Performance of NEWS2 and NEWS2 Plus for Severe COVID-19 Pneumonia
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV): Situation Report, 1; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated With In-Hospital Mortality in a US National Sample of Patients With COVID-19. JAMA Netw. Open 2020, 3, e2029058. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Vignon, P.; Mekontso-Dessap, A.; Tran, S.; Prat, G.; Chew, M.; Balik, M.; Sanfilippo, F.; Banauch, G.; Clau-Terre, F.; et al. Echocardiography findings in COVID-19 patients admitted to intensive care units: A multi-national observational study (the ECHO-COVID study). Intensive Care Med. 2022, 48, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Vieillard-Baron, A.; Evrard, B.; Prat, G.; Chew, M.S.; Balik, M.; Clau-Terré, F.; De Backer, D.; Mekontso Dessap, A.; Orde, S.; et al. Echocardiography phenotypes of right ventricular involvement in COVID-19 ARDS patients and ICU mortality: Post-hoc (exploratory) analysis of repeated data from the ECHO-COVID study. Intensive Care Med. 2023, 49, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, J.C.; Jayarajah, U.; Riza, R.; Abeysuriya, V.; Seneviratne, S.L. Gastrointestinal manifestations in COVID-19. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1362–1388. [Google Scholar] [CrossRef]
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous signs in COVID-19 patients: A review. Dermatol. Ther. 2020, 33, e13549. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef]
- Su, Y.; Ju, M.J.; Xie, R.C.; Yu, S.J.; Zheng, J.L.; Ma, G.G.; Liu, K.; Ma, J.F.; Yu, K.H.; Tu, G.W.; et al. Prognostic Accuracy of Early Warning Scores for Clinical Deterioration in Patients With COVID-19. Front. Med. 2020, 7, 624255. [Google Scholar] [CrossRef]
- Baker, K.F.; Hanrath, A.T.; van der Loeff, I.S.; Kay, L.J.; Back, J.; Duncan, C.J. National Early Warning Score 2 (NEWS2) to identify inpatient COVID-19 deterioration: A retrospective analysis. Clin. Med. 2021, 21, 84–89. [Google Scholar] [CrossRef]
- De Socio, G.V.; Gidari, A.; Sicari, F.; Palumbo, M.; Francisci, D. National Early Warning Score 2 (NEWS2) better predicts critical Coronavirus Disease 2019 (COVID-19) illness than COVID-GRAM, a multi-centre study. Infection 2021, 49, 1033–1038. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Marks, M.; Samuels, T.H.A.; Luintel, A.; Rampling, T.; Chowdhury, H.; Quartagno, M.; Nair, A.; Lipman, M.; Abubakar, I.; et al. Systematic evaluation and external validation of 22 prognostic models among hospitalised adults with COVID-19: An observational cohort study. Eur. Respir. J. 2020, 56, 2003498. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.; Cheng, W.; Wang, X.; Ling, F.; Mu, L.; Li, C.; Huo, X.; Ebell, M.H.; Huang, H.; Zhu, L.; et al. A Risk Classification Model to Predict Mortality Among Laboratory-Confirmed Avian Influenza A H7N9 Patients: A Population-Based Observational Cohort Study. J. Infect. Dis. 2019, 220, 1780–1789. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19: Interim Guidance, 27 May 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance, 13 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Marshall, J.C.; Murthy, S.; Diaz, J.; Adhikari, N.K.; Angus, D.C.; Arabi, Y.M.; Baillie, K.; Bauer, M.; Berry, S.; Blackwood, B.; et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Healthcare-Associated Infection Treatment and Prevention Working Group (COVID-19 Response Committee). Updated 28 January 2021 for Medical Professionals and Public Health Personnel. Guidelines on Clinical Practice, Diagnosis, Treatment, and Prevention of Healthcare-Associated Infection for COVID-19. 2021. Available online: https://ddc.moph.go.th/viralpneumonia/eng/file/guidelines/g_CPG_28jan21.pdf (accessed on 28 January 2021).
- Steyerberg, E.W.; Borsboom, G.J.; van Houwelingen, H.C.; Eijkemans, M.J.; Habbema, J.D. Validation and updating of predictive logistic regression models: A study on sample size and shrinkage. Stat. Med. 2004, 23, 2567–2586. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation 2007, 115, 928–935. [Google Scholar] [CrossRef]
- Kerr, K.F.; McClelland, R.L.; Brown, E.R.; Lumley, T. Evaluating the incremental value of new biomarkers with integrated discrimination improvement. Am. J. Epidemiol. 2011, 174, 364–374. [Google Scholar] [CrossRef]
- Leening, M.J.; Vedder, M.M.; Witteman, J.C.; Pencina, M.J.; Steyerberg, E.W. Net reclassification improvement: Computation, interpretation, and controversies: A literature review and clinician’s guide. Ann. Intern. Med. 2014, 160, 122–131. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172, discussion 207–112. [Google Scholar] [CrossRef]
- Zhang, K.; Zhang, X.; Ding, W.; Xuan, N.; Tian, B.; Huang, T.; Zhang, Z.; Cui, W.; Huang, H.; Zhang, G. The Prognostic Accuracy of National Early Warning Score 2 on Predicting Clinical Deterioration for Patients With COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 699880. [Google Scholar] [CrossRef]
- Tantrakarnapa, K.; Bhopdhornangkul, B. Challenging the spread of COVID-19 in Thailand. One Health 2020, 11, 100173. [Google Scholar] [CrossRef] [PubMed]
- Yorsaeng, R.; Suntronwong, N.; Thongpan, I.; Chuchaona, W.; Lestari, F.B.; Pasittungkul, S.; Puenpa, J.; Atsawawaranunt, K.; Sharma, C.; Sudhinaraset, N.; et al. The impact of COVID-19 and control measures on public health in Thailand, 2020. PeerJ 2022, 10, e12960. [Google Scholar] [CrossRef] [PubMed]
- Issac, A.; Radhakrishnan, R.V.; Vijay, V.R.; Stephen, S.; Krishnan, N.; Jacob, J.; Jose, S.; Azhar, S.M.; Nair, A.S. An examination of Thailand’s health care system and strategies during the management of the COVID-19 pandemic. J. Glob. Health 2021, 11, 03002. [Google Scholar] [CrossRef] [PubMed]
- Williams, B. The National Early Warning Score 2 (NEWS2) in patients with hypercapnic respiratory failure. Clin. Med. 2019, 19, 94–95. [Google Scholar] [CrossRef]
- Liao, X.; Wang, B.; Kang, Y. Novel coronavirus infection during the 2019-2020 epidemic: Preparing intensive care units-the experience in Sichuan Province, China. Intensive Care Med. 2020, 46, 357–360. [Google Scholar] [CrossRef]
- Colombo, C.J.; Colombo, R.E.; Maves, R.C.; Branche, A.R.; Cohen, S.H.; Elie, M.C.; George, S.L.; Jang, H.J.; Kalil, A.C.; Lindholm, D.A.; et al. Performance Analysis of the National Early Warning Score and Modified Early Warning Score in the Adaptive COVID-19 Treatment Trial Cohort. Crit. Care Explor. 2021, 3, e0474. [Google Scholar] [CrossRef]
- Volff, M.; Tonon, D.; Bourenne, J.; Simeone, P.; Velly, L. No added value of the modified NEWS score to predict clinical deterioration in COVID-19 patients. Anaesth. Crit. Care Pain Med. 2020, 39, 577–578. [Google Scholar] [CrossRef]
- Huespe, I.; Carboni Bisso, I.; Di Stefano, S.; Terrasa, S.; Gemelli, N.A.; Las Heras, M. COVID-19 Severity Index: A predictive score for hospitalized patients. Med. Intensiva 2020, 46, 98–101. [Google Scholar] [CrossRef]
- Gidari, A.; De Socio, G.V.; Sabbatini, S.; Francisci, D. Predictive value of National Early Warning Score 2 (NEWS2) for intensive care unit admission in patients with SARS-CoV-2 infection. Infect. Dis. 2020, 52, 698–704. [Google Scholar] [CrossRef]
- Myrstad, M.; Ihle-Hansen, H.; Tveita, A.A.; Andersen, E.L.; Nygard, S.; Tveit, A.; Berge, T. National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from Covid-19—A prospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 66. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Prakash, J.; Bhattacharya, P.K.; Yadav, A.K.; Kumar, A.; Tudu, L.C.; Prasad, K. ROX index as a good predictor of high flow nasal cannula failure in COVID-19 patients with acute hypoxemic respiratory failure: A systematic review and meta-analysis. J. Crit. Care 2021, 66, 102–108. [Google Scholar] [CrossRef]
- Poopipatpab, S.; Nuchpramool, P.; Phairatwet, P.; Lertwattanachai, T.; Trongtrakul, K. The use of respiratory rate-oxygenation index to predict failure of high-flow nasal cannula in patients with coronavirus disease 2019-associated acute respiratory distress syndrome: A retrospective study. PLoS ONE 2023, 18, e0287432. [Google Scholar] [CrossRef]
- Prower, E.; Grant, D.; Bisquera, A.; Breen, C.P.; Camporota, L.; Gavrilovski, M.; Pontin, M.; Douiri, A.; Glover, G.W. The ROX index has greater predictive validity than NEWS2 for deterioration in Covid-19. EClinicalMedicine 2021, 35, 100828. [Google Scholar] [CrossRef]
- Sattar, N.; McInnes, I.B.; McMurray, J.J.V. Obesity Is a Risk Factor for Severe COVID-19 Infection: Multiple Potential Mechanisms. Circulation 2020, 142, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Sawadogo, W.; Tsegaye, M.; Gizaw, A.; Adera, T. Overweight and obesity as risk factors for COVID-19-associated hospitalisations and death: Systematic review and meta-analysis. BMJ Nutr. Prev. Health 2022, 5, 10–18. [Google Scholar] [CrossRef]
- Kappen, T.H.; Vergouwe, Y.; van Klei, W.A.; van Wolfswinkel, L.; Kalkman, C.J.; Moons, K.G. Adaptation of clinical prediction models for application in local settings. Med. Decis. Mak. 2012, 32, E1–E10. [Google Scholar] [CrossRef]
- Tajarernmuang, P.; Sanwirat, P.; Inchai, J.; Phinyo, P.; Limsukon, A. The National Early Warning Score 2(NEWS2) to Predict Early Progression to Severe Community-Acquired Pneumonia. Trop. Med. Infect. Dis. 2023, 8, 68. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | All Cases (n = 725) | Severe (n = 350) | Non-Severe (n = 375) | p-Value |
|---|---|---|---|---|
| Baseline demographics | ||||
| Age (yr) | 46.7 ± 17.4 | 53.0 ± 16.3 | 40.9 ± 16.5 | <0.001 |
| Male, n (%) | 372 (51.3) | 195 (55.8) | 177 (47.2) | 0.026 |
| Body mass index (kg/m2) | 26.6 ± 6.5 | 27.5 ± 6.6 | 25.8 ± 6.2 | <0.001 |
| Current smoker, n (%) | 53 (7.3) | 31 (8.8) | 22 (5.8) | 0.188 |
| Pre-existing comorbidities, n (%) | ||||
| Hypertension | 253 (34.9) | 162 (46.4) | 91 (24.3) | <0.001 |
| Diabetes mellitus | 89 (12.3) | 58 (16.6) | 31 (8.3) | 0.001 |
| Respiratory diseases | 33 (4.5) | 15 (4.3) | 18 (4.8) | 0.859 |
| Chronic kidney disease | 30 (4.1) | 22 (6.3) | 8 (2.1) | 0.008 |
| Heart diseases | 27 (3.8) | 16 (4.7) | 11 (3.0) | 0.264 |
| Others | 28 (3.8) | 16 (4.6) | 12 (3.2) | 0.441 |
| Onset before hospitalization (days) | 3 (2, 5) | 4 (2, 6) | 3 (2, 5) | 0.005 |
| Vital signs | ||||
| Body temperature (°C) | 37.1 ± 0.9 | 37.2 ± 1.0 | 37.0 ± 0.9 | 0.002 |
| Heart rate (beats/min) | 93 ± 18 | 91 ± 18 | 94 ± 18 | 0.040 |
| Respiratory rate (breathes/min) | 24 ± 6 | 26 ± 7 | 22 ± 5 | <0.001 |
| Systolic blood pressure (mmHg) | 127 ± 20 | 129 ± 20 | 124 ±19 | 0.001 |
| Diastolic blood pressure (mmHg) | 78 ± 13 | 78 ± 13 | 78 ± 12 | 0.691 |
| Pulse oximetry (%) at room air | 93.4 ± 6.3 | 90.8 ± 7.8 | 95.3 ± 3.1 | <0.001 |
| NEWS2 * | 5 (3, 7) | 6 (4, 9) | 3 (2, 5) | <0.001 |
| Laboratory investigations | ||||
| Hemoglobin (g/dL) | 13.3 ± 2.1 | 13.4 ± 2.0 | 13.3 ± 2.4 | 0.402 |
| White blood cells (103 cells/mm3) | 7.3 ± 3.7 | 8.3 ± 4.1 | 6.4 ± 2.9 | <0.001 |
| Absolute lymphocyte count 106 (/mm3) | 1.26 ± 0.77 | 1.07 ± 0.66 | 1.48 ± 0.82 | <0.001 |
| Blood urea nitrogen (mg/dL) | 13 (10, 19) | 16 (12, 23) | 11 (9, 15) | <0.001 |
| Creatinine (mg/dL) * | 0.8 (0.7, 1.1) | 0.9 (0.7, 1.2) | 0.8 (0.7, 1.0) | 0.001 |
| D-dimer (ng/mL) * | 473 (322, 1019) | 509 (367, 1058) | 382 (262, 689) | 0.001 |
| C-reactive protein (mg/L) * | 61.1 (17.4, 115.5) | 75.8 (40.1, 134.9) | 27.8 (7.7, 82.3) | <0.001 |
| Procalcitonin (ng/mL) * | 0.11 (0.06, 0.28) | 0.13 (0.07, 0.3) | 0.06 (0.04, 0.12) | <0.001 |
| Lactate dehydrogenase (U/L) * | 354 (260, 474) | 413 (322, 559) | 271 (219, 395) | <0.001 |
| ESR (mm/hour) * | 36 (19, 58) | 40 (23, 58) | 30 (14, 54.7) | <0.001 |
| Multilobe involvement #, n (%) | 586 (80.8) | 326 (93.1) | 260 (69.3) | <0.001 |
| Variables | All Cases (n = 725) | Severe (n = 350) | Non-Severe (n = 375) | p-Value |
|---|---|---|---|---|
| Treatments, n (%) | ||||
| Antiviral drugs | ||||
| Favipiravir | 588 (81.2) | 242 (69.3) | 346 (92.3) | <0.001 |
| Remdesivir | 327 (45.2) | 274 (78.5) | 53 (14.1) | <0.001 |
| Steroids | 615 (84.8) | 347 (99.1) | 268 (71.5) | <0.001 |
| Oral steroids | 306 (42.2) | 190 (54.3) | 116 (30.9) | < 0.001 |
| Systemic steroids | 544 (75.1) | 325 (92.9) | 219 (58.6) | <0.001 |
| Vasopressor | 73 (10.1) | 71 (20.2) | 1 (0.3) | <0.001 |
| Tocilizumab | 68 (9.4) | 68 (19.4) | 0 (0.0) | <0.001 |
| High-flow oxygen nasal cannula | 306 (42.2) | 306 (87.4) | 0 (0.0) | <0.001 |
| Mechanical ventilator | 110 (15.2) | 110 (31.4) | 0 (0.0) | <0.001 |
| Outcomes | ||||
| ICU admission | 338/725 (46.6) | 338/350 (96.6) | 0/375 (0.0) | <0.001 |
| ICU mortality | 55/446 (12.3) | 55/338 (16.3) | 0/0 (0.0) | <0.001 |
| Hospital mortality | 57/725 (7.9) | 57/350 (16.3) | 0/375 (0.0) | <0.001 |
| ICU length of stay | 4 (7, 11) | 8 (5, 12) | 4 (2, 6) | <0.001 |
| Hospital length of stay | 9 (5, 13) | 10 (6, 14) | 8 (5, 13) | <0.001 |
| Complication, n (%) | ||||
| ARDS requiring IMV | 47 (6.5) | 47 (13.4) | 0 (0) | <0.001 |
| Acute kidney injury | 46 (6.3) | 36 (10.3) | 10 (2.7) | <0.001 |
| HAP/VAP | 57 (7.9) | 39 (11.1) | 18 (4.8) | 0.002 |
| Pulmonary embolism | 8 (1.1) | 6 (1.7) | 2 (0.5) | 0.164 |
| Variables | Univariable OR (95%CI) | p-Value | Multivariable OR (95%CI) | p-Value |
|---|---|---|---|---|
| NEWS2 | 1.523 (1.424–1.629) | <0.001 | 1.459 (1.361–1.565) | <0.001 |
| Age | 1.044 (1.034–1.054) | <0.001 | 1.040 (1.028–1.052) | <0.001 |
| Male | 1.407 (1.050–1.886) | 0.022 | - | - |
| Body mass index | 1.042 (1.018–1.067) | 0.001 | 1.077 (1.044–1.110) | <0.001 |
| Current smoker | 1.196 (0.986–1.450) | 0.069 | - | - |
| Hypertension | 1.603 (1.389–1.851) | <0.001 | - | - |
| Diabetes mellitus | 2.226 (1.408–3.521) | 0.001 | - | - |
| Respiratory diseases | 0.888 (0.440–1.790) | 0.740 | - | - |
| Chronic kidney disease | 3.084 (1.353–7.065) | 0.007 | - | - |
| Heart diseases | 1.585 (0.725–3.464) | 0.248 | - | - |
| Other diseases | 1.449 (0.676–3.108) | 0.341 | - | - |
| Variables | Univariable OR | p-Value | Multivariable OR | p-Value | Coefficient | Score |
|---|---|---|---|---|---|---|
| (95%CI) | (95%CI) | |||||
| NEWS2 | 1.523 (1.424–1.629) | <0.001 | 1.459 (1.361–1.565) | <0.001 | 0.378 | 1 |
| Age (yr) | 1.044 (1.034–1.054) | <0.001 | 1.040 (1.028–1.052) | <0.001 | - | - |
| <40 | Ref | 0 | ||||
| 40–59 | 3.369 (2.349–4.832) | <0.001 | 2.827 (1.826–4.375) | <0.001 | 1.039 | 3 |
| ≥60 | 4.934 (3.325–7.324) | <0.001 | 4.211 (2.564–6.918) | <0.001 | 1.438 | 4 |
| BMI (kg/m2) | 1.042 (1.018–1.067) | 0.001 | 1.077 (1.044–1.110) | <0.001 | - | - |
| <24.9 | Ref | 0 | ||||
| 25.0–29.9 | 1.560 (1.093–2.226) | 0.014 | 1.909 (1.233–2.956) | 0.004 | 0.647 | 2 |
| ≥30.0 | 1.799 (1.248–2.593) | 0.002 | 2.819 (1.760–4.514) | <0.001 | 1.036 | 3 |
| Determinants | Apparent Model Performance | Bootstrap Internal Validation | ||||||
|---|---|---|---|---|---|---|---|---|
| NEWS2 | NEWS2 + Age | NEWS2 + BMI | NEWS2 + Age + BMI | NEWS2 | NEWS2 + Age | NEWS2 + BMI | NEWS2 + Age + BMI | |
| Score range | 0 to 20 | 0 to 24 | 0 to 23 | 0 to 27 | 0 to 20 | 0 to 24 | 0 to 23 | 0 to 27 |
| C-statistic (95% CI) | 0.798 (0.767–0.83) | 0.811 (0.780–0.841) | 0.800 (0.768–0.832) | 0.821 (0.791–0.850) | 0.797 (0.766–0.831) | 0.810 (0.780–0.843) | 0.800 (0.769–0.831) | 0.821 (0.792–0.852) |
| Difference in C statistic (95% CI) | Ref | 0.012 (−0.005–0.029) | 0.001 (−0.013–0.016) | 0.022 (0.005–0.040) | Ref | 0.012 (−0.005–0.029) | 0.001 (−0.013–0.016) | 0.022 (0.005–0.040) |
| IDI (95% CI) | Ref | 2.9 (0.9–5.7) | 1.0 (0.0–2.8) | 5.3 (2.9–8.7) | Ref | 2.9 (0.5–5.3) | 1.0 (−0.3–2.4) | 5.3 (2.4–8.3) |
| NRI (95% CI) | Ref | 44.4 (30.6–59.4) | 22.1 (0.4–39.5) | 45.7 (32.1–65.0) | Ref | 44.3 (29.6–59.1) | 22.1 (4.8–39.3) | 45.7 (29.1–62.3) |
| Calibration intercept (95% CI) | 0.105 (0.071–0.156) | 0.068 (0.043–0.106) | 0.074 (0.047–0.116) | 0.035 (0.020–0.060) | 0.106 (0.089–0.126) | 0.068 (0.057–0.081) | 0.075 (0.063–0.089) | 0.035 (0.030–0.042) |
| CITL (95% CI) | 0.000 (−0.172–0.172) | 0.000 (−0.176–0.176) | 0.000 (−0.172–0.172) | 0.000 (−0.179–0.179) | −0.002 (−0.178–0.161) | −0.002 (−0.185–0.178) | −0.002 (−0.172–0.167) | −0.002 (−0.190–0.185) |
| CS (95% CI) | 1.000 (0.837–1.163) | 1.000 (0.843–1.157) | 1.000 (0.838–1.162) | 1.000 (0.845–1.155) | 0.997 (0.838–1.168) | 0.996 (0.860–1.152) | 1.001 (0.857–1.176) | 0.998 (0.865–1.154) |
| Determinants | Score | Cut-Off | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| NEWS2 | 0 to 20 | 5 | 83.7 (79.4–87.4) | 63.5 (58.4–68.5) | 68.1 (63.5–72.5) | 80.7 (75.5–85.0) |
| NEWS2 + Age | 0 to 24 | 5 | 95.4 (72.7–97.4) | 46.4 (41.3–51.6) | 62.4 (58.2–66.5) | 91.6 (86.7–95.1) |
| NEWS2 + BMI | 0 to 23 | 5 | 91.7 (88.3–94.4) | 48.0 (42.8–53.2) | 62.2 (57.9–66.4) | 86.1 (80.7–90.5) |
| NEWS2 + Age + BMI | 0 to 27 | 5 | 99.7 (98.4–100) | 26.7 (22.1–31.7) | 57.7 (53.6–61.7) | 98.9 (94.2–100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trongtrakul, K.; Tajarernmuang, P.; Limsukon, A.; Theerakittikul, T.; Niyatiwatchanchai, N.; Surasit, K.; Glunriangsang, P.; Liwsrisakun, C.; Bumroongkit, C.; Pothirat, C.; et al. The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia. J. Clin. Med. 2024, 13, 298. https://doi.org/10.3390/jcm13010298
Trongtrakul K, Tajarernmuang P, Limsukon A, Theerakittikul T, Niyatiwatchanchai N, Surasit K, Glunriangsang P, Liwsrisakun C, Bumroongkit C, Pothirat C, et al. The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia. Journal of Clinical Medicine. 2024; 13(1):298. https://doi.org/10.3390/jcm13010298
Chicago/Turabian StyleTrongtrakul, Konlawij, Pattraporn Tajarernmuang, Atikun Limsukon, Theerakorn Theerakittikul, Nutchanok Niyatiwatchanchai, Karjbundid Surasit, Pimpimok Glunriangsang, Chalerm Liwsrisakun, Chaiwat Bumroongkit, Chaicharn Pothirat, and et al. 2024. "The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia" Journal of Clinical Medicine 13, no. 1: 298. https://doi.org/10.3390/jcm13010298
APA StyleTrongtrakul, K., Tajarernmuang, P., Limsukon, A., Theerakittikul, T., Niyatiwatchanchai, N., Surasit, K., Glunriangsang, P., Liwsrisakun, C., Bumroongkit, C., Pothirat, C., Inchai, J., Chaiwong, W., Chanayat, P., & Deesomchok, A. (2024). The National Early Warning Score 2 with Age and Body Mass Index (NEWS2 Plus) to Determine Patients with Severe COVID-19 Pneumonia. Journal of Clinical Medicine, 13(1), 298. https://doi.org/10.3390/jcm13010298