Telerehabilitation for Neurological Motor Impairment: A Systematic Review and Meta-Analysis on Quality of Life, Satisfaction, and Acceptance in Stroke, Multiple Sclerosis, and Parkinson’s Disease

 , , ,
, , ,  , and
, and  on behalf of the RIN_TR_Group
on behalf of the RIN_TR_Group
Abstract
1. Introduction
1.1. Description of the Conditions
1.2. Description of the Intervention
1.3. Why It Is Important to Conduct This Review
1.4. Objectives
2. Materials and Methods
2.1. Electronic Searches
2.2. Study Selection
2.3. Outcomes
2.4. Data Extraction and Management
- Citation details: authors, year of publication;
- Aim of the study;
- Study type;
- Participant details (e.g., diagnosis, age, gender distribution, disease severity, months/years since the event, number of patients per group);
- Intervention (i.e., type and dose);
- TR method (e.g., hardware, software, and type of connection, delivery mode);
- Assessment time points;
- Outcome measures (related to our study objectives: QoL, satisfaction, and acceptance);
- Conclusions of the studies.
2.5. Assessment of Risk of Bias in Included Studies
2.6. Measures of Treatment Effect
2.7. Dealing with Missing Data
2.8. Subgroup Analysis and Investigation of Heterogeneity
2.9. Data Synthesis
3. Results
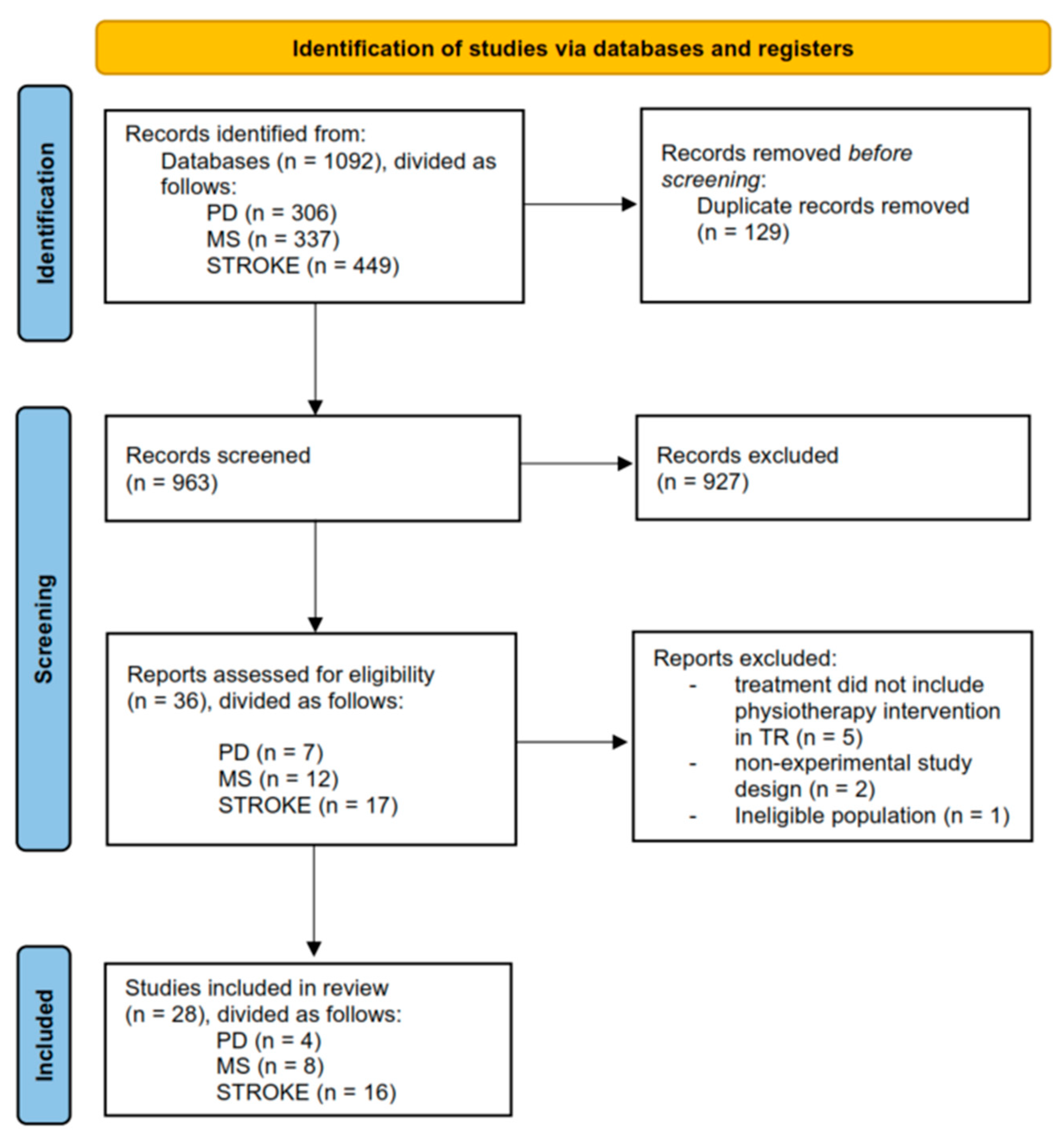
3.1. Results of the Search
3.2. Included Studies
3.3. Excluded Studies
3.4. Risk of Bias in Included Studies
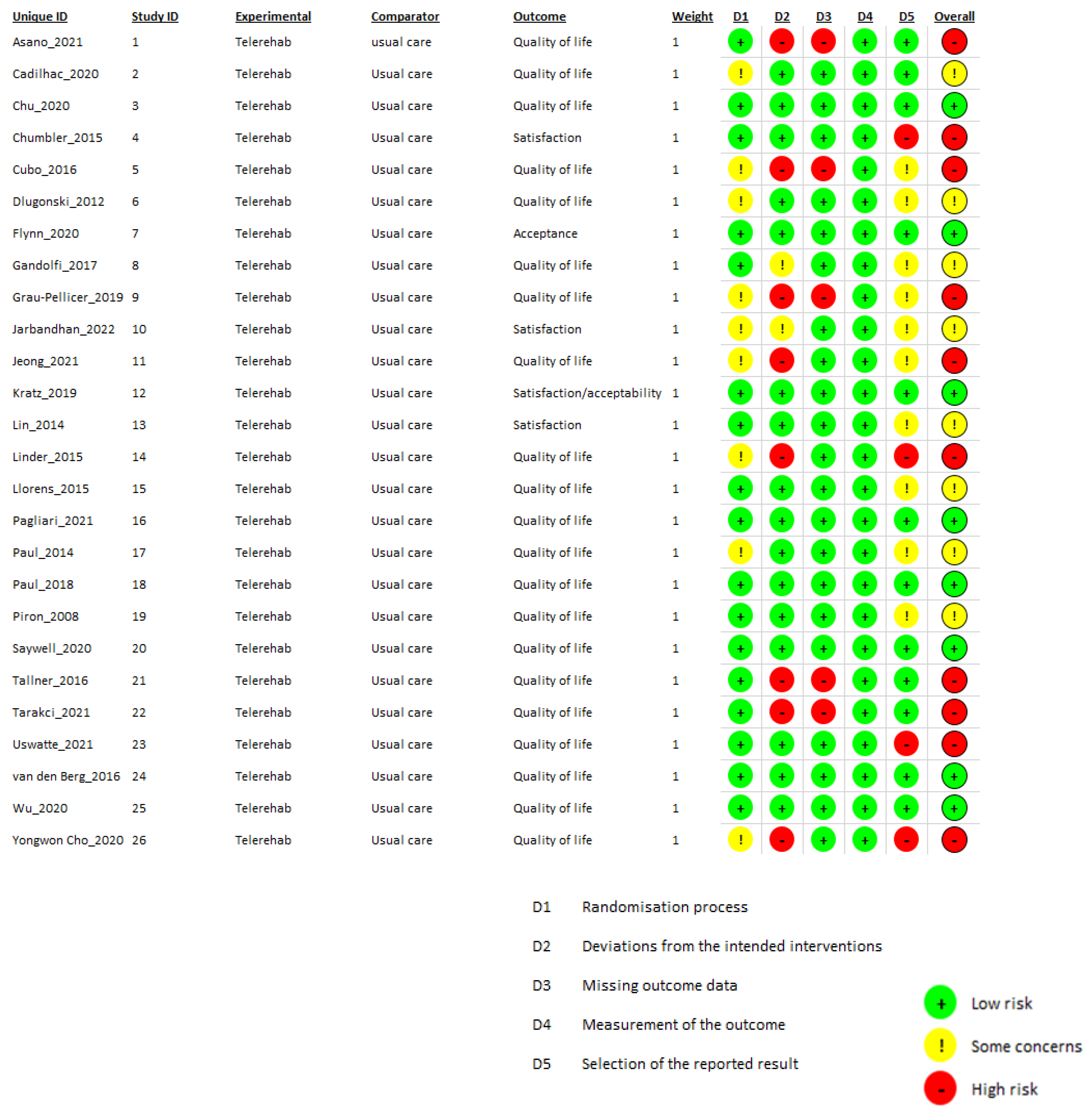
3.4.1. Risk of Bias in Randomized Studies
- -
- Bias arising from the randomization process: 17 studies [16,24,28,29,32,34,35,36,37,39,42,43,44,45,46,48,49,51] received a low risk of bias while the other 9 raised some concerns. These concerns primarily stemmed from the lack of information regarding participant allocation blinding during the randomization phase. In addition, in one study [26], the experimental group was statistically more active at the baseline; in three studies [27,41,47], some information regarding how the randomization process was conducted was missing. Baseline data for the participants were missing in one study [27] and in two [33,40] the randomization process was adjusted to balance the two groups or to follow the personal preferences of the participants.
- -
- Bias due to deviations from intended interventions: In 16 studies, the domain received a low risk-of-bias rating. Two studies [31,49] raised some concerns among reviewers, and eight studies received a high risk-of-bias rating due to the exclusion of some data from the final analysis for a high number of patients who did not complete the study [24,27,30,33,41,45,46,47].
- -
- -
- Bias in measurement of the outcome: All studies in this domain received a low risk-of-bias judgement.
- -
- Bias in selection of the reported result: Twelve studies received a low risk-of-bias judgment. Ten studies raised some concerns, and four studies received a high risk-of-bias judgment. Seven studies modified data from the protocol, introducing variations in assessment scales, outcomes, and the expected timepoints for evaluations. These modifications led to a high risk-of-bias judgment in four studies [28,29,33,36], and raised concerns in two studies [30,31].
3.4.2. Risk of Bias in Non-Randomized Studies
3.5. Effect of Interventions
3.5.1. Comparison 1. TR versus Conventional Treatment in Stroke, MS, and PD—Outcome: QoL
3.5.2. Comparison 2. Synchronous TR versus Conventional Treatment in Stroke and PD—Outcome: QoL
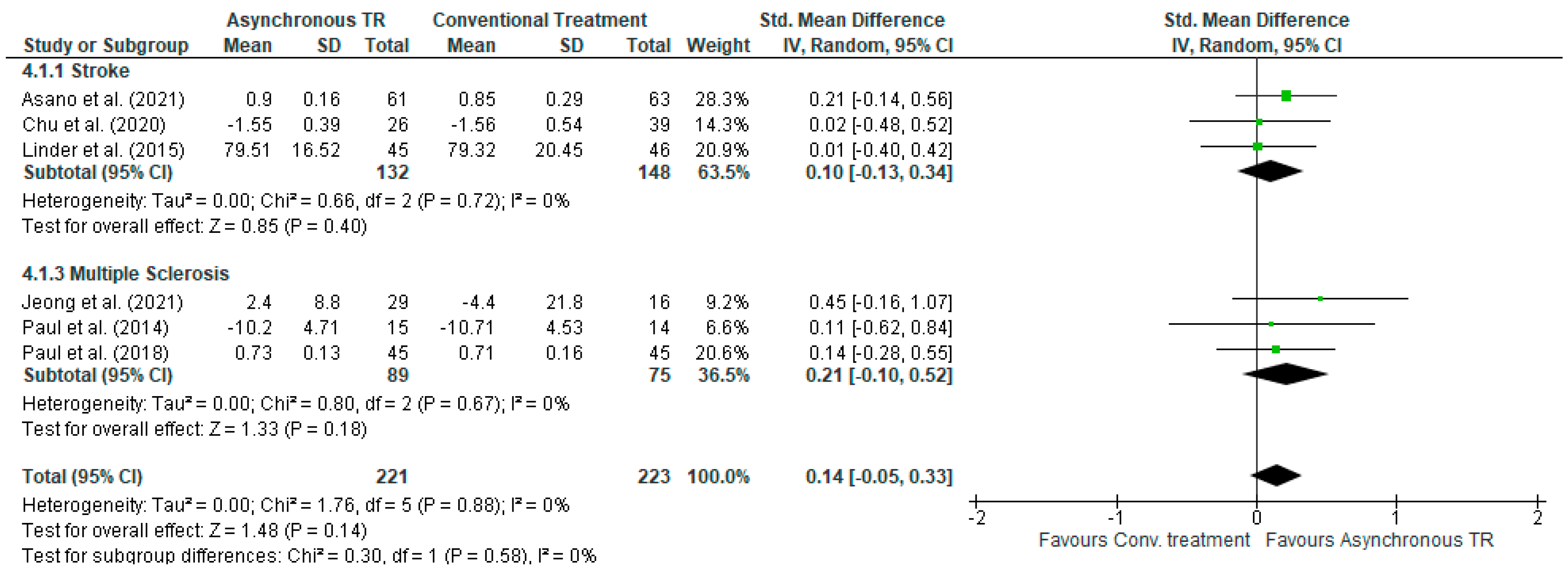
3.5.3. Comparison 3. Asynchronous TR versus Conventional Treatment in Stroke and MS—Outcome: QoL
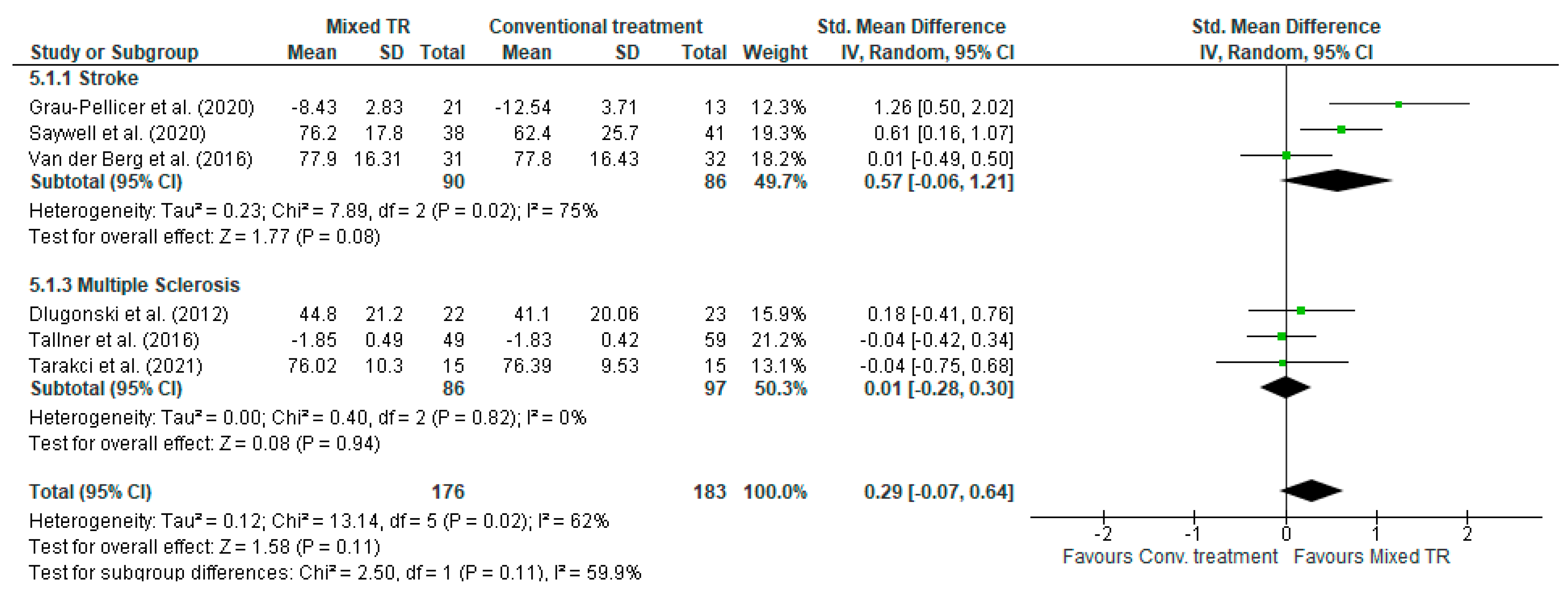
3.5.4. Comparison 4. Mixed TR versus Conventional Treatment-Subgroups Stroke and MS—Outcome: QoL
3.6. Narrative Synthesis
3.6.1. Effects of Telerehabilitation Compared to Conventional Treatment for Improving Patients’ Satisfaction
3.6.2. Effects of Telerehabilitation Compared to Conventional Treatment for Acceptance
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
- #1 (“Stroke”[Mesh] OR “Brain Ischemia”[Mesh] OR “Hemorrhagic Stroke”[Mesh] OR “stroke”[All Fields] OR “cva”[All Fields] OR “post stroke”[All Fields] OR hemiplegia[MeSH] OR cerebrovascular disorders [MeSH] OR basal ganglia cerebrovascular disease [MeSH] OR carotid artery diseases [MeSH] OR intracranial arterial diseases [MeSH] OR intracranial hemorrhages [MeSH] OR “brain injuries” OR “brain injury, chronic” OR poststroke OR “post-stroke”)
- #2 ((“Telerehabilitation”[Mesh]) OR (“Telemedicine”[Mesh]) OR (“Telecommunications”[Mesh]) OR (“telehealth”[All Fields]) OR (“telemedicine”[All Fields]) OR (“telerehabilitation”[All Fields]) OR (videoconferenc*) OR (teletreatment*) OR (“teletherapy”[All Fields]) OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 (“randomized controlled trial*” [MeSH Terms] OR “randomized controlled trial*” [tiab] OR “controlled clinical trial*”[tiab] OR “randomized controlled trial*”[ptyp] OR “controlled clinical trial*”[ptyp] OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3
- #1 ((“Stroke”/de) OR (“Brain Ischemia”/de) OR (“Hemorrhagic Stroke”/de) OR (“stroke”) OR (“cva”) OR (“post stroke”) OR (hemiplegia/de) OR cerebrovascular disorders/de OR basal ganglia cerebrovascular disease/de OR carotid artery diseases/de OR intracranial arterial diseases/de OR intracranial hemorrhages/de OR “brain injuries” OR “brain injury, chronic” OR poststroke OR post-stroke)
- #2 (“Telerehabilitation”/de OR “Telemedicine”/de OR “Telecommunications”/de OR “telehealth” OR “telemedicine” OR “telerehabilitation” OR videoconferenc* OR teletreatment* OR “teletherapy” OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 (“randomized controlled trial*”/de OR “randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3
- #1
- MeSH descriptor: [Stroke] explode all trees
- #2
- MeSH descriptor: [Brain Ischemia] explode all trees
- #3
- MeSH descriptor: [Hemorrhagic Stroke] explode all trees
- #4
- MeSH descriptor: [Hemiplegia] explode all trees
- #5
- MeSH descriptor: [Cerebrovascular Disorders] explode all trees
- #6
- MeSH descriptor: [Basal Ganglia Cerebrovascular Disease] explode all trees
- #7
- MeSH descriptor: [Carotid Artery Diseases] explode all trees
- #8
- MeSH descriptor: [Intracranial Arterial Diseases] explode all trees
- #9
- MeSH descriptor: [Intracranial Hemorrhages] explode all trees
- #10
- (“stroke” OR “cva” OR “post stroke” OR “brain injuries” OR “brain injury, chronic” OR “poststroke” OR “post-stroke”):ti,ab,kw (Word variations have been searched)
- #11
- MeSH descriptor: [Telerehabilitation] explode all trees
- #12
- MeSH descriptor: [Telemedicine] explode all trees
- #13
- MeSH descriptor: [Telecommunications] explode all trees
- #14
- (“telehealth” OR “telemedicine” OR “telerehabilitation” OR “videoconferenc*” OR “teletreatment*” OR “Teletheraphy” OR “Distance Education” OR “Telepractice” OR “Virtual conferenc*” OR “Tele-rehabilitation” OR “Remote rehabilitation”):ti,ab,kw (Word variations have been searched)
- #15
- MeSH descriptor: [Randomized Controlled Trial] explode all trees
- #16
- ((“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized controlled trial*”)):ti,ab,kw (Word variations have been searched)
- #17
- #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10
- #18
- #11 OR #12 OR #13 #14
- #19
- #15 OR #16 602107
- #20
- #17 AND #18 AND #19
- TS = (“Stroke” OR “Brain Ischemia” OR “Hemorrhagic Stroke” OR “cva” OR “post stroke” OR hemiplegia OR “cerebrovascular disorders” OR “basal ganglia cerebrovascular disease” OR “carotid artery diseases” OR “intracranial arterial diseases” OR “intracranial hemorrhages” OR “brain injuries” OR “brain injury, chronic” OR poststroke OR ”post-stroke”)
- TS = (“Telerehabilitation” OR “Telemedicine” OR “Telecommunications” OR “telehealth” OR videoconferenc* OR teletreatment* OR “teletherapy” OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- WC = (rehabilitation)
- TS = (“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”)
- #1 (“Parkinson Disease” [Mesh] OR “Parkinson Disease” OR “Parkinson”)
- #2 ((“Telerehabilitation”[Mesh]) OR (“Telemedicine”[Mesh]) OR (“Telecommunications”[Mesh]) OR (“telehealth”[All Fields]) OR (“telemedicine”[All Fields]) OR (“telerehabilitation”[All Fields]) OR (videoconferenc*) OR (teletreatment*) OR (“teletherapy”[All Fields]) OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 “randomized controlled trial*” [MeSH Terms] OR “randomized controlled trial*” [tiab] OR “controlled clinical trial*”[tiab] OR “randomized controlled trial*”[ptyp] OR “controlled clinical trial*”[ptyp] OR “quasi-randomized control trial*”
- #1 AND #2 AND #3
- #1 (“Parkinson Disease”/de OR “Parkinson Disease” OR “Parkinson”)
- #2 ((“Telerehabilitation”/de) OR (“Telemedicine”/de) OR (“Telecommunications”/de) OR (“telehealth”) OR (“telemedicine”) OR (“telerehabilitation”) OR (videoconferenc*) OR (teletreatment*) OR (“teletherapy”) OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 “randomized controlled trial*”/de OR “randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”
- #1 AND #2 AND #3
- #1 TS = (”Parkinson Disease” OR Parkinson)
- #2 TS = (“Telerehabilitation” OR “Telemedicine” OR “Telecommunications” OR “telehealth” OR videoconferenc* OR teletreatment* OR “teletherapy” OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 WC = (rehabilitation)
- #4 TS = (“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3 AND #4
- #1
- MeSH descriptor: [Parkinson Disease] explode all trees
- #2
- “Parkinson Disease” OR “Parkinson”
- #3
- MeSH descriptor: [Telerehabilitation] explode all trees
- #4
- MeSH descriptor: [Telemedicine] explode all trees
- #5
- MeSH descriptor: [Telecommunications] explode all trees
- #6
- (“telehealth” OR “telemedicine” OR “telerehabilitation” OR “videoconferenc*” OR “teletreatment*” OR “Teletheraphy” OR “Distance Education” OR “Telepractice” OR “Virtual conferenc*” OR “Tele-rehabilitation” OR “Remote rehabilitation”):ti,ab,kw (Word variations have been searched)
- #7
- MeSH descriptor: [Randomized Controlled Trial] explode all trees
- #8
- ((“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized controlled trial*”)):ti,ab,kw (Word variations have been searched)
- #9
- #1 OR #2
- #10
- #3 OR #4 OR #5 OR #6
- #11
- #7 OR #8
- #12
- #9 AND #10 AND #11
- #1 (“Multiple Sclerosis”[Mesh] OR “Multiple Sclerosis, Chronic Progressive”[Mesh] OR “Multiple Sclerosis” OR “Multiple Sclerosis, Chronic Progressive” OR “Multiple Sclerosis, Relapsing-Remitting”[Mesh] OR “Multiple Sclerosis, Relapsing-Remitting”)
- #2 ((“Telerehabilitation”[Mesh]) OR (“Telemedicine”[Mesh]) OR (“Telecommunications”[Mesh]) OR (“telehealth”[All Fields]) OR (“telemedicine”[All Fields]) OR (“telerehabilitation”[All Fields]) OR (videoconferenc*) OR (teletreatment*) OR (“teletherapy”[All Fields]) OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 (“randomized controlled trial*” [MeSH Terms] OR “randomized controlled trial*” [tiab] OR “controlled clinical trial*”[tiab] OR “randomized controlled trial*”[ptyp] OR “controlled clinical trial*”[ptyp] OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3
- #1 (“Multiple Sclerosis”/de OR “Multiple Sclerosis, Chronic Progressive”/de OR “Multiple Sclerosis” OR “Multiple Sclerosis, Chronic Progressive” OR “Multiple Sclerosis, Relapsing-Remitting”/de OR “Multiple Sclerosis, Relapsing-Remitting”)
- #2 (“Telerehabilitation”/de OR “Telemedicine”/de OR “Telecommunications”/de OR “telehealth” OR “telemedicine” OR “telerehabilitation” OR videoconferenc* OR teletreatment* OR “teletherapy” OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 (“randomized controlled trial*”/de OR “randomized controlled trial*” OR “controlled clinical trial*” OR “randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3
- #1
- MeSH descriptor: [Multiple Sclerosis] explode all trees
- #2
- MeSH descriptor: [Multiple Sclerosis, Chronic Progressive] explode all trees
- #3
- MeSH descriptor: [Multiple Sclerosis, Relapsing-Remitting] explode all trees
- #4
- (“multiple sclerosis” OR “mutiple sclerosis, relapsing-remitting” OR “Multiple sclerosis, Chronic Progressive”):ti,ab,kw
- #5
- MeSH descriptor: [Telerehabilitation] explode all trees
- #6
- MeSH descriptor: [Telemedicine] explode all trees
- #7
- MeSH descriptor: [Telecommunications] explode all trees
- #8
- (“telehealth” OR “telemedicine” OR “telerehabilitation” OR “videoconferenc*” OR “teletreatment*” OR “Teletheraphy” OR “Distance Education” OR “Telepractice” OR “Virtual conferenc*” OR “Tele-rehabilitation” OR “Remote rehabilitation”):ti,ab,kw (Word variations have been searched)
- #9
- MeSH descriptor: [Randomized Controlled Trial] explode all trees
- #10
- ((“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized controlled trial*”)):ti,ab,kw (Word variations have been searched)
- #11
- #1 OR #2 OR #3 OR #4
- #12
- #5 OR #6 OR #7 OR #8
- #13
- #9 OR #10
- #14
- #11 AND #12 AND #13
- #1 TS = (”Multiple Sclerosis” OR “Multiple Sclerosis, Chronic Progressive” OR “Multiple Sclerosis, Relapsing-Remitting”)
- #2 TS = (“Telerehabilitation” OR “Telemedicine” OR “Telecommunications” OR “telehealth” OR videoconferenc* OR teletreatment* OR “teletherapy” OR “Distance Education” OR Telepractice OR “Virtual Conferenc*” OR “Tele-rehabilitation” OR “Remote Rehabilitation”)
- #3 WC = (rehabilitation)
- #4 TS = (“randomized controlled trial*” OR “controlled clinical trial*” OR “quasi-randomized control trial*”)
- #1 AND #2 AND #3 AND #4
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathology | Study | Satisfaction | Outcome Measures | Findings | Acceptance | Outcome Measures | Findings |
|---|---|---|---|---|---|---|---|
| Stroke | Asano et al., 2018 [24] | N/A * | N/A | N/A | Present | Expressed as a calculation of hours of therapy sessions conducted. | There was no significant difference in the median time spent on rehabilitation and exercise between the two groups. |
| Benvenuti et al., 2014 [25] | Present | Structured interviews using Likert-type scales were administered to participants and caregivers. | The intervention received high satisfaction ratings and produced no adverse events. | Present | An evaluation questionnaire augmented by several dimensions from the Unified Theory of User Acceptance and Use of Technology (UTAUT). | 50 subjects were highly adherent to the study protocol, 88 demonstrated average adherence, and 30 low adherence. | |
| Cadilhac et al., 2020 [26] | Present | Survey utilizing closed and open question formats. Participants provided feedback on program aspects (benefits, willingness to continue, and likelihood of recommending to other stroke survivors). The intervention group shared input on electronic health support (message details, support duration). | More than 85% of participants in both groups found the goal-setting form beneficial for developing their goals. Additionally, both the intervention (92%) and control (72%) groups agreed that clinicians were helpful in goal development, with a non-significant difference. | Present | Survey utilizing closed and open question formats. Perceived benefit of the electronic health support (intervention group only). | No unintended harms or effects were reported. In total, 77% of participants believed that text or email messages helped them to achieve their goals and were a good way to receive education about stroke. Participants were comfortable with technology use and felt that the system was easy to understand. | |
| Chumbler et al., 2015 [29] | Present | Stroke-specific satisfaction With care (SSPSC) questionnaire and interview consisting of 13 closed-ended questions (using a 5-point Likert-type scale) and 4 open-ended questions. | Participants reported a greater effect on hospital satisfaction than home satisfaction. Subjects were satisfied with the in-home intervention, finding it convenient, useful and expressing comfort with being videotaped during sessions. | N/A | N/A | N/A | |
| Grau-Pellicer et al., 2020 [30] | Present | Ad hoc questionnaire to assess satisfaction in relationship with the benefits obtained (use of app, improvement of physical condition, gait capacity, balance, expectations, and self-efficacy). | Most patients reported a high level of satisfaction, with all expressing a favourable opinion in recommending the treatment to others. No adverse effect was reported. | N/A | N/A | N/A | |
| Jarbandhan et al., 2022 [31] | Present | A self-developed questionnaire consisting of 7 Likert scale questions and an optional open-ended question for system improvement recommendations. | Participants, in general, had a positive experience with the program. Some of them expressed a preference for a longer duration of the program or sessions. | Present | Expressed through adherence to the treatment. | Participants perceived the intervention as supportive. Adherence to the treatment was influenced by factors such as the rainy season and associated infrastructural issues (n = 2), participants’ medical status (n = 3), and insufficient motivation to continue the program without direct supervision (n = 1). Notably, no adverse events were reported. | |
| Lin et al., 2014 [32] | Present | A questionnaire survey derived from the “Successes of the technology acceptance model” and the “Model of information systems technology” (David [1989], DeLone and McLean [2003]). Each item was assessed using a Likert scale, and the values for each dimension were obtained by averaging the scores of the corresponding items within that dimension. | Overall, participants in both groups expressed a high level of satisfaction, perception of ease of use, and a positive attitude toward TR system, with a willingness to recommend it to others. The results showed no significant differences in all items, except for perceived usefulness and perceived satisfaction of system in the TR group. | N/A | N/A | N/A | |
| Piron et al., 2008 [34] | Present | 12-item questionnaire, derived from a validated scale (Monnin 2002), measuring the patient’s satisfaction with physical therapy, patient’s attitude towards the treatment, the patient–therapist relationship, and global opinion about the treatment performed. Each item was measured with a Likert scale. | The two groups reported similar levels of satisfaction, with no significant differences in most aspects, including treatment comprehension, equipment, user-friendliness, and the patient–therapist relationship. | N/A | N/A | N/A | |
| Uswatte et al., 2021 [36] | Present | Participant opinion survey [64] assessing perceptions about the therapeutic value and difficulty of the interventions before and after treatment. This consisted of a 7-point Likert scale and 1 open-ended question. | Participants expressed high satisfaction with the intervention received and moderate satisfaction regarding the perceived difficulty of the intervention. | N/A | N/A | N/A | |
| Cho et al., 2022 [27] | Present | A 10-item, 7-point Likert scale related to the patients’ satisfaction with the therapy program and the exercises assigned to them. The final session was employed as the indicator of overall satisfaction with the therapy. | The increased use of goal adjustment strategies led to greater satisfaction at the end of therapy, supporting the notion that motivational benefits derived from goal adjustment positively influenced overall satisfaction. Patient satisfaction was not linked to the actual level of arm motor status recovery. | N/A | N/A | N/A | |
| Parkinson’s Disease | Cubo et al., 2017 [47] | Present | A visual analogic scale. Collection of the number of technical problems associated with the use of the device. | Treatment was feasible and patients were satisfied when it is was used in conjunction with their regular clinical visits and telephone/email support. | N/A | N/A | N/A |
| Flynn et al., 2021 [48] | N/A | N/A | N/A | Present | Examined using a participant questionnaire about the program. Participants were also interviewed about their experiences of exercise at home and in a center. | Questionnaire was completed by 88% of participants at the end of Week 5 and 85% at the end of Week 10. At Week 5, all participants reported finding the exercise helpful, group exercising satisfying, and would recommend it to others. By Week 10, center-based group participants echoed these sentiments. However, home-based group participants found the exercise helpful and could follow the program, but only 53% found it satisfying, and 6% did not recommend it. | |
| Gandolfi et al., 2017 [49] | Present | A questionnaire investigating domains considered relevant for the patient; responses for each domain were marked on a 5-point Likert-type scale. Patients were provided with a logbook to record their feelings and any difficulties or adverse events they had experienced at each training session. | No statistically significant difference in satisfaction rates between the two groups. | N/A | N/A | N/A | |
| Multiple Sclerosis | Dlugonski et al., 2012 [40] | Present | Ad hoc process evaluation questionnaire, containing 5 Likert items and 1 open-ended final feedback. | Participants expressed high satisfaction with the overall program, staff, and the provided pedometer. The satisfaction with the website itself was slightly lower. In open-ended feedback, participants expressed a desire for more interaction with others, but some found the forum section of the website challenging to use. All participants indicated they would recommend the program to others. | N/A | N/A | N/A |
| Kratz et al., 2020 [42] | N/A | N/A | N/A | Present | The client satisfaction questionnaire (CSQ-8) | For the experimental group, the treatment was highly feasible and acceptable. Attendance rates were higher for the experimental group. | |
| Paul et al., 2014 [43] | Present | Ad hoc questionnaire based on Finkelstein 2008. | Treatment was a feasible method for delivering physiotherapy and was deemed acceptable by individuals moderately affected by MS. Evaluation questionnaire responses indicated that the system was easy to use and received high ratings from participants. | Present | Telephone interviews recorded, transcribed, and verified. Emerging themes and sub-themes were identified and agreed between two independent researchers. | Treatment was considered acceptable, usable, and convenient. | |
| Paul et al., 2019 [44] | N/A | N/A | N/A | Present | Semi-structured telephone interviews with physiotherapists and participants, investigating their reasons for taking part in the study, their views of the assessments and intervention, any issues faced, the perceived benefit, and recommendations for a future trials. | The treatment was feasible and acceptable to both participants and physiotherapists, with no intervention-related adverse events. |
References
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Amatya, B. Rehabilitation in Multiple Sclerosis: A Systematic Review of Systematic Reviews. Arch. Phys. Med. Rehabil. 2017, 98, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Pallant, J.F. Use of the International Classification of Functioning, Disability and Health (ICF) to identify preliminary comprehensive and brief core sets for multiple sclerosis. Disabil. Rehabil. 2007, 29, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Yang, Y.; Zhang, L.; Zhang, Q.; Balbuena, L.; Ungvari, G.S.; Zang, Y.F.; Xiang, Y.T. Quality of life in Parkinson’s disease: A systematic review and meta-analysis of comparative studies. CNS Neurosci. Ther. 2021, 27, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lima, M.J.M.; Brasileiro, I.C.; Lima, T.L.; Braga-Neto, P. Quality of life after stroke: Impact of clinical and sociodemographic factors. Clinics 2018, 73, e418. [Google Scholar] [CrossRef]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and recovery of motor function: A systematic review and meta-analysis. J. Telemed. Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef]
- Theodoros, D.G. Telerehabilitation for service delivery in speech-language pathology. J. Telemed. Telecare 2008, 14, 221–224. [Google Scholar] [CrossRef]
- Shem, K.; Irgens, I.; Alexander, M. Chapter 2—Getting Started: Mechanisms of Telerehabilitation. In Telerehabilitation; Alexander, M., Ed.; Elsevier: New Delhi, India, 2022; pp. 5–20. [Google Scholar]
- Temkin, A.J.; Ulicny, G.R.; Vesmarovich, S.H. Telerehab. A perspective of the way technology is going to change the future of patient treatment. Rehab Manag. 1996, 9, 28–30. [Google Scholar]
- Tchero, H.A.-O.; Tabue Teguo, M.A.-O.; Lannuzel, A.A.-O.; Rusch, E.A.-O. Telerehabilitation for Stroke Survivors: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2018, 20, e10867. [Google Scholar] [CrossRef]
- Truijen, S.A.-O.; Abdullahi, A.A.-O.; Bijsterbosch, D.; van Zoest, E.; Conijn, M.; Wang, Y.; Struyf, N.; Saeys, W.A.-O. Effect of home-based virtual reality training and telerehabilitation on balance in individuals with Parkinson disease, multiple sclerosis, and stroke: A systematic review and meta-analysis. Neurol. Sci. 2022, 43, 2995–3006. [Google Scholar] [CrossRef] [PubMed]
- Nikolaev, V.A.; Nikolaev, A.A. Recent trends in telerehabilitation of stroke patients: A narrative review. NeuroRehabilitation 2022, 51, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Goffredo, M.; Baglio, F.; Proietti, S.; Maggioni, G.; Turolla, A.; Pournajaf, S.; Jonsdottir, J.; Zeni, F.; Federico, S.; Cacciante, L.; et al. Efficacy of non-immersive virtual reality-based telerehabilitation on postural stability in Parkinson’s disease: A multicenter randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2023, 59. [Google Scholar] [CrossRef] [PubMed]
- Goffredo, M.; Pagliari, C.; Turolla, A.; Tassorelli, C.; Di Tella, S.; Federico, S.; Pournajaf, S.; Jonsdottir, J.; De Icco, R.; Pellicciari, L.; et al. Non-Immersive Virtual Reality Telerehabilitation System Improves Postural Balance in People with Chronic Neurological Diseases. J. Clin. Med. 2023, 12, 3178. [Google Scholar] [CrossRef] [PubMed]
- Pagliari, C.; Di Tella, S.; Jonsdottir, J.; Mendozzi, L.; Rovaris, M.; De Icco, R.; Milanesi, T.; Federico, S.; Agostini, M.; Goffredo, M.; et al. Effects of home-based virtual reality telerehabilitation system in people with multiple sclerosis: A randomized controlled trial. J. Telemed. Telecare 2021, 0(0), 1357633X211054839. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health; ICF: Geneva, Switzerland, 2001. [Google Scholar]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ Open 2016, 355, i4919. [Google Scholar] [CrossRef]
- Collaboration, T.C. Review Manager (RevMan), 5.4; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Julian Higgins, J.T. Choosing effect measures and computing estimates of effect. Subsection 6.5.2.2 Obtaining standard deviations from standard errors and confidence intervals for group means. In Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2023; Chapter 6. [Google Scholar]
- Asano, M.; Tai, B.C.; Chen, C.; Yen, S.C.; Tay, A.; Cheong, A.; Ng, Y.S.; De Silva, D.A.; Caves, K.; Kumar, Y.; et al. Home-based tele-rehabilitation presents comparable and positive impact on self-reported functional outcomes as center-based rehabilitation: Singapore tele-technology aided rehabilitation in stroke (STARS) trial. Ann. Phys. Rehabil. Med. 2018, 61, e22–e23. [Google Scholar] [CrossRef]
- Benvenuti, F.; Stuart, M.; Cappena, V.; Gabella, S.; Corsi, S.; Taviani, A.; Albino, A.; Scattareggia Marchese, S.; Weinrich, M. Community-based exercise for upper limb paresis: A controlled trial with telerehabilitation. Neurorehabil Neural Repair 2014, 28, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, D.A.; Andrew, N.E.; Busingye, D.; Cameron, J.; Thrift, A.G.; Purvis, T.; Li, J.C.; Kneebone, I.; Thijs, V.; Hackett, M.L.; et al. Pilot randomised clinical trial of an eHealth, self-management support intervention (iVERVE) for stroke: Feasibility assessment in survivors 12-24 months post-event. Pilot Feasibility Stud. 2020, 6, 172. [Google Scholar] [CrossRef]
- Cho, Y.; Hamm, J.M.; Heckhausen, J.; Cramer, S.C. The role of goal adjustment during rehabilitation from stroke. Appl. Psychol. Health Well Being 2022, 14, 26–43. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.; Bu, X.; Sun, Z.; Wang, Y.; Feng, W.; Xiao, L.; Jiang, F.; Tang, X. Feasibility of a Nurse-Trained, Family Member-Delivered Rehabilitation Model for Disabled Stroke Patients in Rural Chongqing, China. J. Stroke Cerebrovasc Dis. 2020, 29, 105382. [Google Scholar] [CrossRef] [PubMed]
- Chumbler, N.R.; Li, X.; Quigley, P.; Morey, M.C.; Rose, D.; Griffiths, P.; Sanford, J.; Hoenig, H. A randomized controlled trial on Stroke telerehabilitation: The effects on falls self-efficacy and satisfaction with care. J. Telemed. Telecare 2015, 21, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Grau-Pellicer, M.; Lalanza, J.F.; Jovell-Fernandez, E.; Capdevila, L. Impact of mHealth technology on adherence to healthy PA after stroke: A randomized study. Top Stroke Rehabil. 2020, 27, 354–368. [Google Scholar] [CrossRef]
- Jarbandhan, A.; Toelsie, J.; Veeger, D.; Bipat, R.; Vanhees, L.; Buys, R. Feasibility of a home-based physiotherapy intervention to promote post-stroke mobility: A randomized controlled pilot study. PLoS ONE 2022, 17, e0256455. [Google Scholar] [CrossRef]
- Lin, K.H.; Chen, C.H.; Chen, Y.Y.; Huang, W.T.; Lai, J.S.; Yu, S.M.; Chang, Y.J. Bidirectional and multi-user telerehabilitation system: Clinical effect on balance, functional activity, and satisfaction in patients with chronic stroke living in long-term care facilities. Sensors 2014, 14, 12451–12466. [Google Scholar] [CrossRef]
- Linder, S.M.; Rosenfeldt, A.B.; Bay, R.C.; Sahu, K.; Wolf, S.L.; Alberts, J.L. Improving Quality of Life and Depression After Stroke Through Telerehabilitation. Am. J. Occup. Ther. 2015, 69, 6902290020p1–6902290020p10. [Google Scholar] [CrossRef]
- Piron, L.; Turolla, A.; Tonin, P.; Piccione, F.; Lain, L.; Dam, M. Satisfaction with care in post-stroke patients undergoing a telerehabilitation programme at home. J. Telemed. Telecare 2008, 14, 257–260. [Google Scholar] [CrossRef]
- Saywell, N.L.; Vandal, A.C.; Mudge, S.; Hale, L.; Brown, P.; Feigin, V.; Hanger, C.; Taylor, D. Telerehabilitation After Stroke Using Readily Available Technology: A Randomized Controlled Trial. Neurorehabil. Neural Repair. 2021, 35, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Uswatte, G.; Taub, E.; Lum, P.; Brennan, D.; Barman, J.; Bowman, M.H.; Taylor, A.; McKay, S.; Sloman, S.B.; Morris, D.M.; et al. Tele-rehabilitation of upper-extremity hemiparesis after stroke: Proof-of-concept randomized controlled trial of in-home Constraint-Induced Movement therapy. Restor. Neurol. Neurosci. 2021, 39, 303–318. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, M.; Crotty, M.P.; Liu, E.; Killington, M.; Kwakkel, G.P.; van Wegen, E. Early Supported Discharge by Caregiver-Mediated Exercises and e-Health Support After Stroke: A Proof-of-Concept Trial. Stroke 2016, 47, 1885–1892. [Google Scholar] [CrossRef]
- Vloothuis, J.D.M.; Mulder, M.; Nijland, R.H.M.; Goedhart, Q.S.; Konijnenbelt, M.; Mulder, H.; Hertogh, C.; van Tulder, M.; van Wegen, E.E.H.; Kwakkel, G. Caregiver-mediated exercises with e-health support for early supported discharge after stroke (CARE4STROKE): A randomized controlled trial. PLoS ONE 2019, 14, e0214241. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Xu, J.; Yue, C.; Li, Y.; Liang, Y. Collaborative Care Model Based Telerehabilitation Exercise Training Program for Acute Stroke Patients in China: A Randomized Controlled Trial. J. Stroke Cerebrovasc Dis. 2020, 29, 105328. [Google Scholar] [CrossRef] [PubMed]
- Dlugonski, D.; Motl, R.W.; Mohr, D.C.; Sandroff, B.M. Internet-delivered behavioral intervention to increase physical activity in persons with multiple sclerosis: Sustainability and secondary outcomes. Psychol. Health Med. 2012, 17, 636–651. [Google Scholar] [CrossRef] [PubMed]
- Jeong, I.C.; Karpatkin, H.; Finkelstein, J. Physical Telerehabilitation Improves Quality of Life in Patients with Multiple Sclerosis. Stud. Health Technol. Inform. 2021, 284, 384–388. [Google Scholar] [CrossRef]
- Kratz, A.L.; Atalla, M.; Whibley, D.; Myles, A.; Thurston, T.; Fritz, N.E. Calling Out MS Fatigue: Feasibility and Preliminary Effects of a Pilot Randomized Telephone-Delivered Exercise Intervention for Multiple Sclerosis Fatigue. J. Neurol. Phys. Ther. 2020, 44, 23–31. [Google Scholar] [CrossRef]
- Paul, L.; Coulter, E.H.; Miller, L.; McFadyen, A.; Dorfman, J.; Mattison, P.G. Web-based physiotherapy for people moderately affected with Multiple Sclerosis; quantitative and qualitative data from a randomized, controlled pilot study. Clin. Rehabil. 2014, 28, 924–935. [Google Scholar] [CrossRef]
- Paul, L.; Renfrew, L.; Freeman, J.; Murray, H.; Weller, B.; Mattison, P.; McConnachie, A.; Heggie, R.; Wu, O.; Coulter, E.H. Web-based physiotherapy for people affected by multiple sclerosis: A single blind, randomized controlled feasibility study. Clin. Rehabil. 2019, 33, 473–484. [Google Scholar] [CrossRef]
- Tallner, A.; Streber, R.; Hentschke, C.; Morgott, M.; Geidl, W.; Maurer, M.; Pfeifer, K. Internet-Supported Physical Exercise Training for Persons with Multiple Sclerosis-A Randomised, Controlled Study. Int. J. Mol. Sci. 2016, 17, 1667. [Google Scholar] [CrossRef] [PubMed]
- Tarakci, E.; Tarakci, D.; Hajebrahimi, F.; Budak, M. Supervised exercises versus telerehabilitation. Benefits for persons with multiple sclerosis. Acta Neurol. Scand. 2021, 144, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Cubo, E.; Mariscal, N.; Solano, B.; Becerra, V.; Armesto, D.; Calvo, S.; Arribas, J.; Seco, J.; Martinez, A.; Zorrilla, L.; et al. Prospective study on cost-effectiveness of home-based motor assessment in Parkinson’s disease. J. Telemed. Telecare 2017, 23, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.; Preston, E.; Dennis, S.; Canning, C.G.; Allen, N.E. Home-based exercise monitored with telehealth is feasible and acceptable compared to centre-based exercise in Parkinson’s disease: A randomised pilot study. Clin. Rehabil. 2021, 35, 728–739. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Geroin, C.; Dimitrova, E.; Boldrini, P.; Waldner, A.; Bonadiman, S.; Picelli, A.; Regazzo, S.; Stirbu, E.; Primon, D.; et al. Virtual Reality Telerehabilitation for Postural Instability in Parkinson’s Disease: A Multicenter, Single-Blind, Randomized, Controlled Trial. Biomed Res. Int. 2017, 2017, 7962826. [Google Scholar] [CrossRef] [PubMed]
- Isernia, S.; Di Tella, S.; Pagliari, C.; Jonsdottir, J.; Castiglioni, C.; Gindri, P.; Salza, M.; Gramigna, C.; Palumbo, G.; Molteni, F.; et al. Effects of an Innovative Telerehabilitation Intervention for People With Parkinson’s Disease on Quality of Life, Motor, and Non-motor Abilities. Front. Neurol. 2020, 11, 846. [Google Scholar] [CrossRef]
- Llorens, R.; Noe, E.; Colomer, C.; Alcaniz, M. Effectiveness, usability, and cost-benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 418–425.e412. [Google Scholar] [CrossRef]
- Finkelstein, J.; Liu, J. Usability of Telerehabilitation System Supporting Multipronged Exercise in Patients with Multiple Sclerosis. Stud. Health Technol. Inform. 2018, 251, 281–284. [Google Scholar]
- Rimmer, J.H.; Thirumalai, M.; Young, H.J.; Pekmezi, D.; Tracy, T.; Riser, E.; Mehta, T. Rationale and design of the tele-exercise and multiple sclerosis (TEAMS) study: A comparative effectiveness trial between a clinic- and home-based telerehabilitation intervention for adults with multiple sclerosis (MS) living in the deep south. Contemp. Clin. Trials 2018, 71, 186–193. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Deuel, L.M.; Voss, T.S.; Finnigan, K.; George, B.P.; Eason, S.; Miller, D.; Reminick, J.I.; Appler, A.; Polanowicz, J.; et al. Increasing access to specialty care: A pilot, randomized controlled trial of telemedicine for Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 1652–1659. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Venkataraman, V.; Grana, M.J.; Bull, M.T.; George, B.P.; Boyd, C.M.; Beck, C.A.; Rajan, B.; Seidmann, A.; Biglan, K.M. Randomized controlled clinical trial of “virtual house calls” for Parkinson disease. JAMA Neurol. 2013, 70, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Egner, A.; Phillips, V.L.; Vora, R.; Wiggers, E. Depression, fatigue, and health-related quality of life among people with advanced multiple sclerosis: Results from an exploratory telerehabilitation study. NeuroRehabilitation 2003, 18, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Robb, J.F.; Hyland, M.H.; Goodman, A.D. Comparison of telemedicine versus in-person visits for persons with multiple sclerosis: A randomized crossover study of feasibility, cost, and satisfaction. Mult. Scler. Relat. Disord. 2019, 36, 101258. [Google Scholar] [CrossRef]
- Wilkinson, J.R.; Spindler, M.; Wood, S.M.; Marcus, S.C.; Weintraub, D.; Morley, J.F.; Stineman, M.G.; Duda, J.E. High patient satisfaction with telehealth in Parkinson disease: A randomized controlled study. Neurology. Clin. Pract. 2016, 6, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Beit Yosef, A.; Jacobs, J.M.; Shames, J.; Schwartz, I.; Gilboa, Y. A Performance-Based Teleintervention for Adults in the Chronic Stage after Acquired Brain Injury: An Exploratory Pilot Randomized Controlled Crossover Study. Brain Sci. 2022, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.; Garzon, M.; Benavides-Varela, S.; De Pellegrin, S.; Bencini, G.; Rossi, G.; Rosadoni, S.; Mancuso, M.; Turolla, A.; Meneghello, F.; et al. Telerehabilitation in poststroke anomia. Biomed Res. Int. 2014, 2014, 706909. [Google Scholar] [CrossRef] [PubMed]
- Cacciante, L.; Kiper, P.; Garzon, M.; Baldan, F.; Federico, S.; Turolla, A.; Agostini, M. Telerehabilitation for people with aphasia: A systematic review and meta-analysis. J. Commun. Disord 2021, 92, 106111. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020, 1, CD010255. [Google Scholar] [CrossRef]
- Foong, Y.C.; Merlo, D.; Gresle, M.; Zhu, C.; Buzzard, K.; Lechner-Scott, J.; Barnett, M.; Taylor, B.; Kalincik, T.; Kilpatrick, T.; et al. The Patient-Determined Disease Steps scale is not interchangeable with the Expanded Disease Status Scale in mild to moderate multiple sclerosis. Eur. J. Neurol. 2024, 31, e16046. [Google Scholar] [CrossRef]
- Mead, G.E.; Sposato, L.A.; Sampaio Silva, G.; Yperzeele, L.; Wu, S.; Kutlubaev, M.; Cheyne, J.; Wahab, K.; Urrutia, V.C.; Sharma, V.K.; et al. A systematic review and synthesis of global stroke guidelines on behalf of the World Stroke Organization. Int. J. Stroke 2023, 18, 499–531. [Google Scholar] [CrossRef]


| Study ID | Confounding Bias | Selection Bias | Classification of Intervention Bias | Deviations from Intended Intervention Bias | Attrition Bias | Detection Bias | Reporting Bias | Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Benvenuti et al., 2014 [25] | Low risk No confounding domains identified | Serious risk Groups mixed and results were combined | Moderate risk Participants in the control group were offered to participate to the experimental intervention at the end of their assigned treatment | Critical risk 26.5% of dropout; deviations from intended intervention unbalanced between groups | Critical risk Missing outcome data; no ITT analysis performed | Low risk assessor was not blinded, but the outcome measure was a self-reported questionnaire | Serious risk Study protocol not found | Critical risk lots of dropout; no ITT; no information on study protocol. |
| Isernia et al., 2020 [50] | Low risk No confounding domains identified | Low risk All eligible participants included in the study and followed from the start of the intervention | Low risk Intervention status is well defined | Serious risk Difference in groups size (ClinicHEAD n.31; UC n. 20; HomeHEAD n. 11). Analysis for baseline differences performed only between UC and HomeHEAD groups | Low risk Multiple imputation by chained equations was performed to replace missing values to address potential biases due to incomplete follow-up | Low risk self-reported survey | Low risk no selection of the reported result found | Serious risk some concerns about deviations from intended interventions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Federico, S.; Cacciante, L.; Cieślik, B.; Turolla, A.; Agostini, M.; Kiper, P.; Picelli, A., on behalf of the RIN_TR_Group. Telerehabilitation for Neurological Motor Impairment: A Systematic Review and Meta-Analysis on Quality of Life, Satisfaction, and Acceptance in Stroke, Multiple Sclerosis, and Parkinson’s Disease. J. Clin. Med. 2024, 13, 299. https://doi.org/10.3390/jcm13010299
Federico S, Cacciante L, Cieślik B, Turolla A, Agostini M, Kiper P, Picelli A on behalf of the RIN_TR_Group. Telerehabilitation for Neurological Motor Impairment: A Systematic Review and Meta-Analysis on Quality of Life, Satisfaction, and Acceptance in Stroke, Multiple Sclerosis, and Parkinson’s Disease. Journal of Clinical Medicine. 2024; 13(1):299. https://doi.org/10.3390/jcm13010299
Chicago/Turabian StyleFederico, Sara, Luisa Cacciante, Błażej Cieślik, Andrea Turolla, Michela Agostini, Pawel Kiper, and Alessandro Picelli on behalf of the RIN_TR_Group. 2024. "Telerehabilitation for Neurological Motor Impairment: A Systematic Review and Meta-Analysis on Quality of Life, Satisfaction, and Acceptance in Stroke, Multiple Sclerosis, and Parkinson’s Disease" Journal of Clinical Medicine 13, no. 1: 299. https://doi.org/10.3390/jcm13010299
APA StyleFederico, S., Cacciante, L., Cieślik, B., Turolla, A., Agostini, M., Kiper, P., & Picelli, A., on behalf of the RIN_TR_Group. (2024). Telerehabilitation for Neurological Motor Impairment: A Systematic Review and Meta-Analysis on Quality of Life, Satisfaction, and Acceptance in Stroke, Multiple Sclerosis, and Parkinson’s Disease. Journal of Clinical Medicine, 13(1), 299. https://doi.org/10.3390/jcm13010299