

Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature

 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
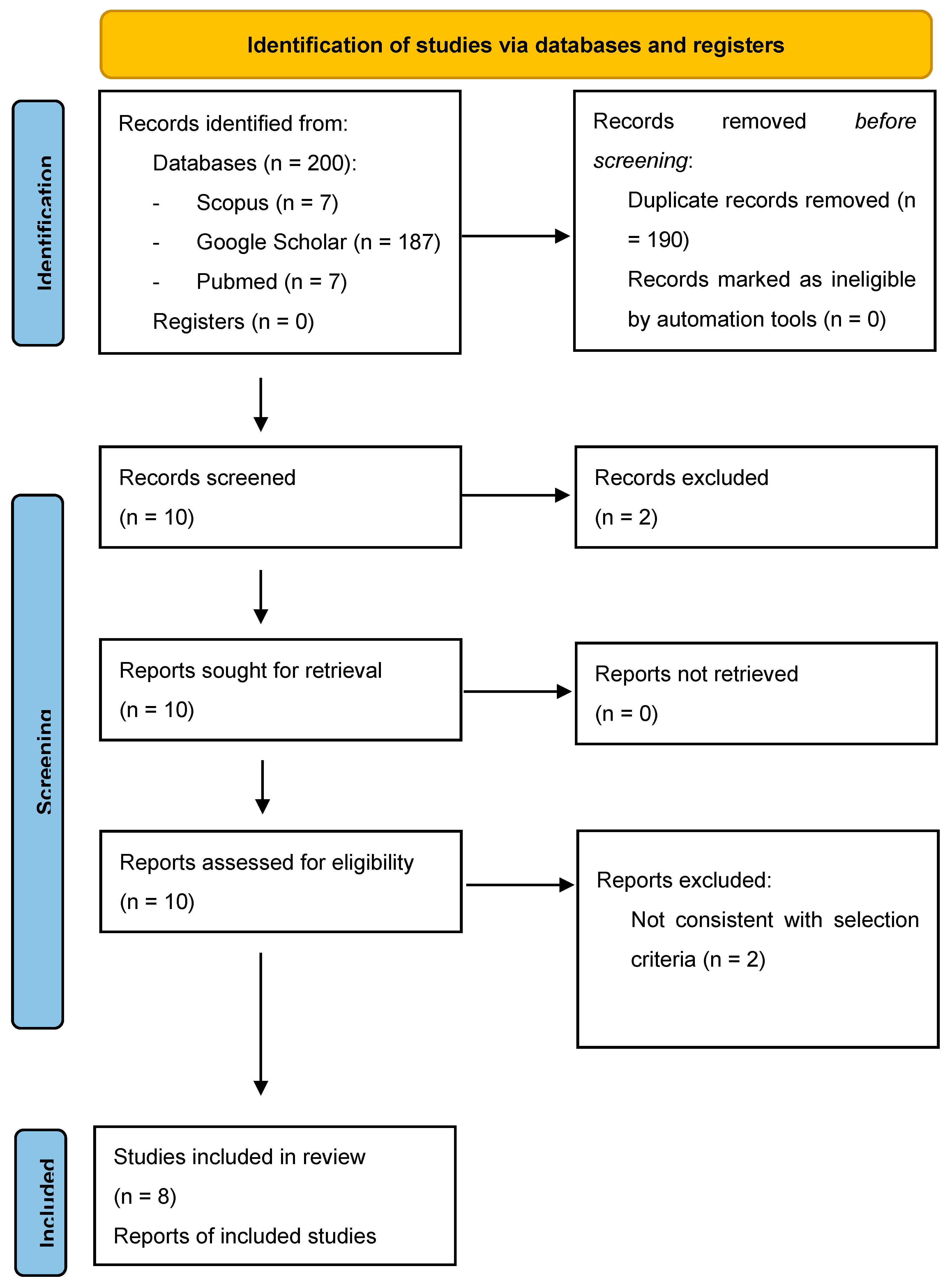
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Redline, R.W. Classification of placental lesions. Am. J. Obstet. Gynecol. 2015, 213 (Suppl. S4), S21–S28. [Google Scholar] [CrossRef]
- Carlucci, S.; Stabile, G.; Sorrentino, F.; Nappi, L.; Botta, G.; Menato, G.; Masturzo, B. The singular case of multiple chorangioma syndrome in an IVF pregnancy. Analysis of the case and review of literature. Placenta 2021, 103, 120–123. [Google Scholar] [CrossRef]
- Soper, J.T. Gestational Trophoblastic Disease: Current Evaluation and Management. Obstet. Gynecol. 2021, 137, 355–370, Erratum in: Obstet Gynecol. 2022, 139, 149. [Google Scholar] [CrossRef]
- Carlucci, S.; Stabile, G.; Catagini, S.; Borghi, C.; Scutiero, G.; Morano, D.; Greco, P. Fetal disseminated intravascular coagulopathy, hydrops and massive umbilical vein thrombosis consequence of a rare placental condition: Multifocal chorangiomatosis. J. Matern.-Fetal Neonatal Med. 2022, 35, 4009–4013. [Google Scholar] [CrossRef] [PubMed]
- Khong, T.Y. Chorangioma with trophoblastic proliferation. Virchows Arch. 2000, 436, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Gallot, D.; Sapin, V.; Beaufrère, A.-M.; Boda, C.; Laurichesse-Delmas, H.; Déchelotte, P.; Lémery, D. Récurrence de chorio-angiomes multiples: à propos d’un cas. [Recurrence of multiple chorio-angiomas: A case-report]. Gynecol. Obstet. Fertil. 2003, 31, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Faes, T.; Pecceu, A.; Van Calenbergh, S.; Moerman, P. Chorangiocarcinoma of the placenta: A case report and clinical review. Placenta 2012, 33, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Guschmann, M.; Schulz-Bischof, K.; Vogel, M. Inzidentelles Chorangiokarzinom. Fallbericht, Immunhistochemie und Theorien zur möglichen Histogenese. [Incidental chorangiocarcinoma. Case report, immunohistochemistry and theories of possible histogenesis]. Pathologe 2003, 24, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Trask, C.; Lage, J.M.; Roberts, D.J. A second case of "chorangiocarcinoma" presenting in a term asymptomatic twin pregnancy: Choriocarcinoma in situ with associated villous vascular proliferation. Int. J. Gynecol. Pathol. 1994, 13, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Prospero International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 10 December 2022).
- Tufanaru, C. Chapter 3: Systematic reviews of effectiveness. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Jauniaux, E.; Zucker, M.; Meuris, S.; Verhest, A.; Wilkin, P.; Hustin, J. Chorangiocarcinoma: An unusual tumour of the placenta. The missing link? Placenta 1988, 9, 607–613. [Google Scholar] [CrossRef]
- Ariel, I.; Boldes, R.; Weintraub, A.; Reinus, C.; Beller, U.; Arbel, R. Chorangiocarcinoma: A case report and review of the literature. Int. J. Gynecol. Pathol. 2009, 28, 267–271. [Google Scholar] [CrossRef]
- Huang, B.; Zhang, Y.-P.; Yuan, D.-F.; Yang, R.; Wang, C.; Wu, R.-F. Chorangiocarcinoma: A case report and clinical review. Int. J. Clin. Exp. Med. 2015, 8, 16798–16802. [Google Scholar] [PubMed]
- García-Molina, F.; Heredia-Oliva, L.; Castaño, M.D.; Andrada-Becerra, E. Corangiocarcinoma. A propósito de un caso. Rev. Española De Patol. 2016, 50, 229–233. [Google Scholar] [CrossRef]
- Sagar, N.; Tanwar, P.; Khurana, N.; Kashyap, P. Placental Chorangiocarcinoma: Case Report with Literature Review of a Rare Entity. Placental Chorangiocarcinoma: Case Report with Literature Review of a Rare Entity. Turk Patoloji Derg. 2022, 38, 292–296. [Google Scholar] [CrossRef]
- Benirschke, K.; Kaufmann, P.; Baergen, R.N. Pathology of the Human Placenta; Springer: New York, NY, USA, 2005. [Google Scholar]
- Ogino, S.; Redline, R.W. Villous capillary lesions of the placenta: Distinctions between chorangioma, chorangiomatosis, and chorangiosis. Hum Pathol. 2000, 31, 945–954. [Google Scholar] [CrossRef]
- Majlessi, H.F.; Wagner, K.M.; Brooks, J.J. Atypical cellular chorangioma of the placenta. Int. J. Gynecol. Pathol. 1983, 1, 403–408. [Google Scholar] [CrossRef]
- Mesia, A.F.; Mo, B.P.; Ylagan, L.R. Atypical cellular chorangioma. Arch. Pathol. Lab. Med. 1999, 123, 536–538. [Google Scholar] [CrossRef]
- Vellone, V.G.; Calamaro, P.; Vignale, C.; Novaro, G.; Penna, L.; Fulcheri, E. Atypical Cellular Chorangioma: A Potential Diagnostic Pitfall With Worrisome Aspects but a Favorable Prognosis. Int. J. Surg. Pathol. 2015, 23, 364–368. [Google Scholar] [CrossRef]
- Mao, T.-L.; Seidman, J.D.; Kurman, R.J.; Shih, I.-M. Cyclin E and p16 immunoreactivity in epithelioid trophoblastic tumor—An aid in differential diagnosis. Am. J. Surg. Pathol. 2006, 30, 1105–1110. [Google Scholar] [CrossRef]
- Benirschke, K.; Burton, G.J.; Baergen, R.N. Pathology of the Human Placenta, 6th ed.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Kurman, R.J.; Ellenson, L.H.; Ronnett, B.M. Blaustein’s Pathology of the Female Genital Tract, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Di Massa, G.; Stabile, G.; Romano, F.; Balduit, A.; Mangogna, A.; Belmonte, B.; Canu, P.; Bertucci, E.; Ricci, G.; Salviato, T. CD133 Expression in Placenta Chorioangioma Presenting as a Giant Asymptomatic Mass. Medicina 2021, 57, 162. [Google Scholar] [CrossRef] [PubMed]
- Mao, T.L.; Kurman, R.J.; Jeng, Y.M.; Huang, W.; Shih, I.M. HSD3B1 as a novel trophoblast-associated marker that assists in the differential diagnosis of trophoblastic tumors and tumorlike lesions. Am. J. Surg. Pathol. 2008, 32, 236–242. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Study Type | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 |
|---|---|---|---|---|---|---|---|---|---|
| Jauniaux et al. (1988) [13] Placenta | Case report |  | | | | | | | |
| Trask C. et al. (1994) [9] Int J Gynecol Pathol | Case report | | | | | | | Not applicable | |
| Ariel I. et al. (2009) [14] Int J Gynecol Pathol | Case report | | Not applicable | | | | | | |
| Guschmann M. et al. (2003) [8] Pathologe | Case report | | Unclear | | | | | | Unclear |
| Faes T. et al. (2012) [7] Placenta | Case report | | | | | | | | |
| Huang B. et al. (2015) [15] Int J Clin Exp Med | Case report | | Not applicable | | | | | | |
| Garcìa-Molina F. et al. (2016) [16] Patalogìa | Case report | | | | | | | Not applicable | Unclear |
| Sagar N. et al. (2021) [17] Turk Patoloji Derg | Case report | | | | | | | Not applicable | Unclear |
| Reference | Maternal Age | GA at Delivery (Weeks), Parity Singleton/Twin | Placental Weight (g) | Ultrasound Features | Macroscopic Examination Tumor Size | Microscopic Examination | Immunostaining | Maternal b-HCG (Baseline, Follow-Ups) | Fetal Assessment | Follow-Up | Maternal Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jauniaux E. et al., 1988 [13] | 35 | 35 w, 3003 CS for shoulder presentation and vaginal bleeding Singleton | 600 | Not determined | Well-demarcated round nodule, multilobulated, limited by a white pseudocapsule 1.5 × 1.5 cm | Well-differentiated capillary pattern supported by chorionic stroma cells and fibrous tissue with an outer layer of syncytiotrophoblast and cytotrophoblast with nuclear atypia | -PAS-positive fibrin deposition in the area close to the tumor -hCG strongly positive in the trophoblastic layer and pseudocapsule -hPL positive to syncytium of the villi | -Not determined -Below detection 6 months after delivery | Normal | 9 months | Normal |
| Trask C. et al., 1994 [9] | 36 | 36 w, 1011 Spontaneous labor and delivery Twin BC/BA | 250 (presenting twin placenta) | Not determined | Firm lesion similar to an infarct 3 × 2.5 cm | Stem villi with pronounced proliferation of villous stromal vessels, circumferential proliferation of malignant trophoblast protruding in the intervillous space (nuclear atypia, high mitotic rate) | -keratin (E1/AE3, Boehringer-Mannheim, Indianapolis, IN, U.S.A.) reactivity in the abnormal trophoblast -hCG positive -hPL weak and focal at the malignant trophoblast, strong in the normal syncytiotrophoblast | -Not determined -698 mIU/mL 7 days after delivery -Below detection 29 days and 3 months after delivery | Normal | 7 days 29 days 3 months | Normal |
| Ariel I. et al., 2009 [14] | 23 | 37 w, 0000 Spontaneous labor and CS for condylomata Singleton | 678 | Thick lesion of 5–6 cm with hyperechogenic and hypoechogenic areas without hypervascularization | Well-demarcated mass with alternating red and yellowish tissue on cut sections 8 × 5 cm | Malignant epithelial tumor with central necrosis forming a complex branching structure within a chorangioma (mitotic rate >90%, pleomorphic nuclei) | -Panytokeratin positive -b-HCG positive -hsd3b1 focally positive -hPL weakly positive | -Consistent with GA at baseline -Below detection 1 month after delivery | Normal | 1 month after delivery | Normal |
| Guschmann M. et al., 2003 [8] | 31 | 34 w, 1001 CS for fetal distress and FGR Singleton | 496 | Not determined | Nodule with grey-yellow foci 3 cm | Villi surrounded by syncytiotrophoblast atypia and chorangiosis with adjacent areas of necrosis (nuclear atypia, mitoses) | -bHCG at the syncytiotrophoblast -hPL weak and prevalent at the intermediate trophoblast -VEGF, bFGF, Ang-1,2, PDGF expression at the trophoblast similar to normal villi | -Consistent with GA at baseline -Not determined | FGR | Not determined | Normal |
| Faes T. et al., 2012 [7] | 36 | 40 w, 2002 Spontaneous labor and delivery Singleton | 812 | Nodule of 8 × 7 cm with hyperechogenic and hypoechogenic areas with hypervascularisation at the border. Supplying artery PI 0.87, RI 0.58, PSF 39.34 cm/s. | Firm reddish-brown tumor with a lobulated appearance on section with multiple small white nodules 8 × 7 cm | Dilated angiomatous vessels filled up with neoplastic cell proliferation and separated by fibrous septa containing numerous capillary-type blood vessels; extensive central necrosis with dystrophic calcification (nuclei pleomorphism, multinucleation, high mitotic rate). | -AE1/AE3 cytoplasmic positivity -p63 nuclear staining -inhibin-alfa focal positivity -b-HCG strong positivity at the margins -Ki-67 high proliferation index | -Not determined -Below detection 1 month after delivery | Normal | 1 month after delivery | Normal |
| Huang B. et al., 2015 [15] | 27 | 39 w, 0000 Spontaneous labor and CS for suspicious of Macrosomia Singleton | 500 | Not determined | Firm grayish yellow-white mass with the consistency of an infarct. 5 × 4.5 cm | Abnormal trophoblastic proliferation in conjunction with a chorangioma in the stroma of chorionic villi. Cells forming solid masses with massive central coagulation necrosis surrounded by three to six layers of epithelial tumor cells (high proliferation index, mitoses) | -strong intensity for hCG, PLAP, CK, CD31 (+) and CD34 (+) in the lesion. -Ki67 high proliferation index | -Consistent with GA at baseline -Increase at 6 weeks after delivery -Below detection after 3 cycles of chemotherapy | Normal | -6 weeks after delivery -3 months after delivery | Lung metastasis at 3 months after delivery |
| Garcìa-Molina F. et al. (2016) Patalogìa [16] | 36 | 41 3013 Elective C section Twin BC/BA | 587 (fused bichorial placenta) | Not determined | Small irregular whitish area | Abnormal trophoblastic proliferation, with cellular atypia and arborescent proliferation through stromal cells and abundant vessels (cellular mitoses, coagulation necrosis, pleomorfism) | -Positivity for bHCG, CK 8–18, PAN CK -vascular proliferation vimentina and CD-34 (+) -High Ki-67 at the area of trophoblastic proliferation | -Not determined -negative at one month after delivery | Normal | 1 month after delivery | Normal |
| Sagar N. et al., 2021 [17] | 29 | 30 w, 1021 pProm, Chorionamnionitis CS Singleton | Not determined | Small hypoechoic lesion in relation to the uterine fundus with maintained uterine contour | Grey-white nodule, solid-cystic at cut section with friable areas 5.5 × 4.5 × 3 cm | Multiple well-circumscribed cellular nests with central necrosis dispersed in a chorangiomatous stroma (mitoses, apoptotic bodies, multinucleation) | -AE1/AE3, PathnSitu, U.S.A. cytokeratin positivity -b-HCH positivity -PLAP and Ki-67 | -Consistent with GA at baseline -Not determined | Normal | Not determined | Normal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stabile, G.; Scalia, M.S.; Stampalija, T.; Bruno, M.; Laganà, A.S.; Sartore, A.; Mangogna, A.; Carlucci, S. Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. J. Clin. Med. 2023, 12, 3065. https://doi.org/10.3390/jcm12093065
Stabile G, Scalia MS, Stampalija T, Bruno M, Laganà AS, Sartore A, Mangogna A, Carlucci S. Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. Journal of Clinical Medicine. 2023; 12(9):3065. https://doi.org/10.3390/jcm12093065
Chicago/Turabian StyleStabile, Guglielmo, Maria Sole Scalia, Tamara Stampalija, Matteo Bruno, Antonio Simone Laganà, Andrea Sartore, Alessandro Mangogna, and Stefania Carlucci. 2023. "Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature" Journal of Clinical Medicine 12, no. 9: 3065. https://doi.org/10.3390/jcm12093065
APA StyleStabile, G., Scalia, M. S., Stampalija, T., Bruno, M., Laganà, A. S., Sartore, A., Mangogna, A., & Carlucci, S. (2023). Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. Journal of Clinical Medicine, 12(9), 3065. https://doi.org/10.3390/jcm12093065