


Minimally Invasive Donors Right Hepatectomy versus Open Donors Right Hepatectomy: A Meta-Analysis


Abstract
1. Introduction
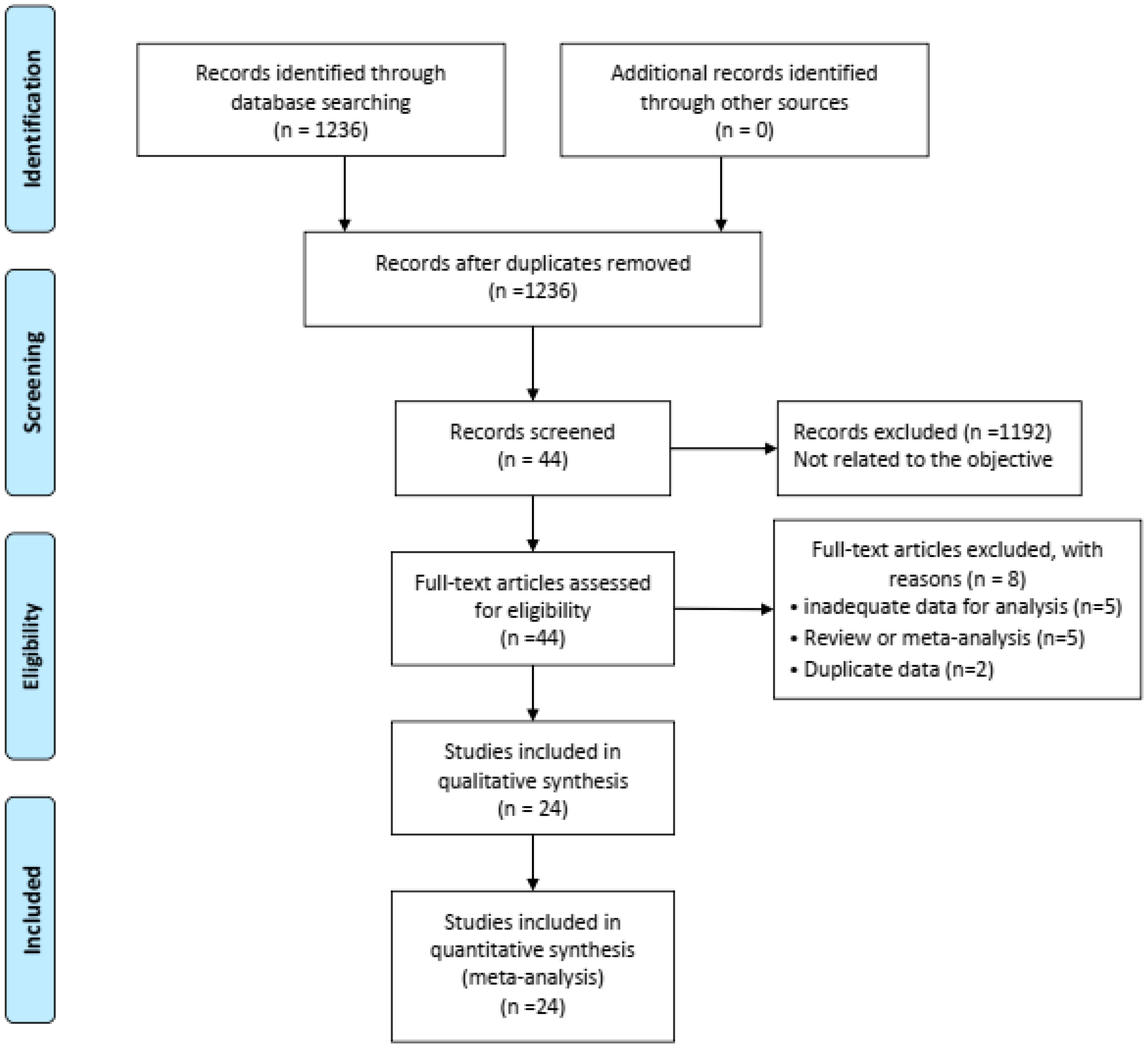
1.1. Search Strategy and Study Selection
1.2. Inclusion and Exclusion Criteria
1.3. Data Extraction and Quality Assessment
1.4. Statistical Analysis
2. Results
2.1. Search Results and Characteristics of the Included Studies
2.2. Perioperative Outcomes
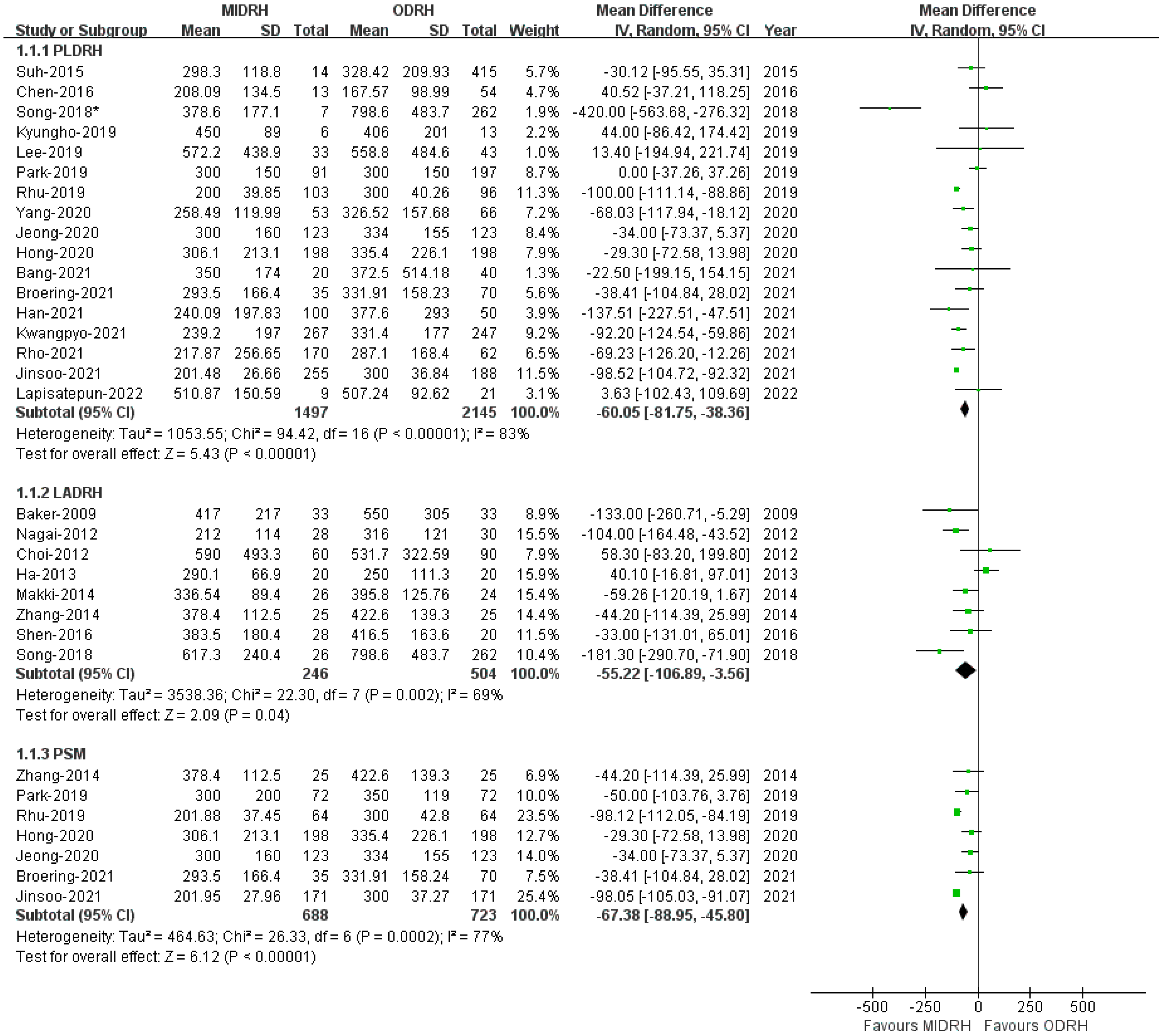
Intraoperative Blood Loss
2.3. Operative Time
2.4. Length of Hospital Stay (LOS)
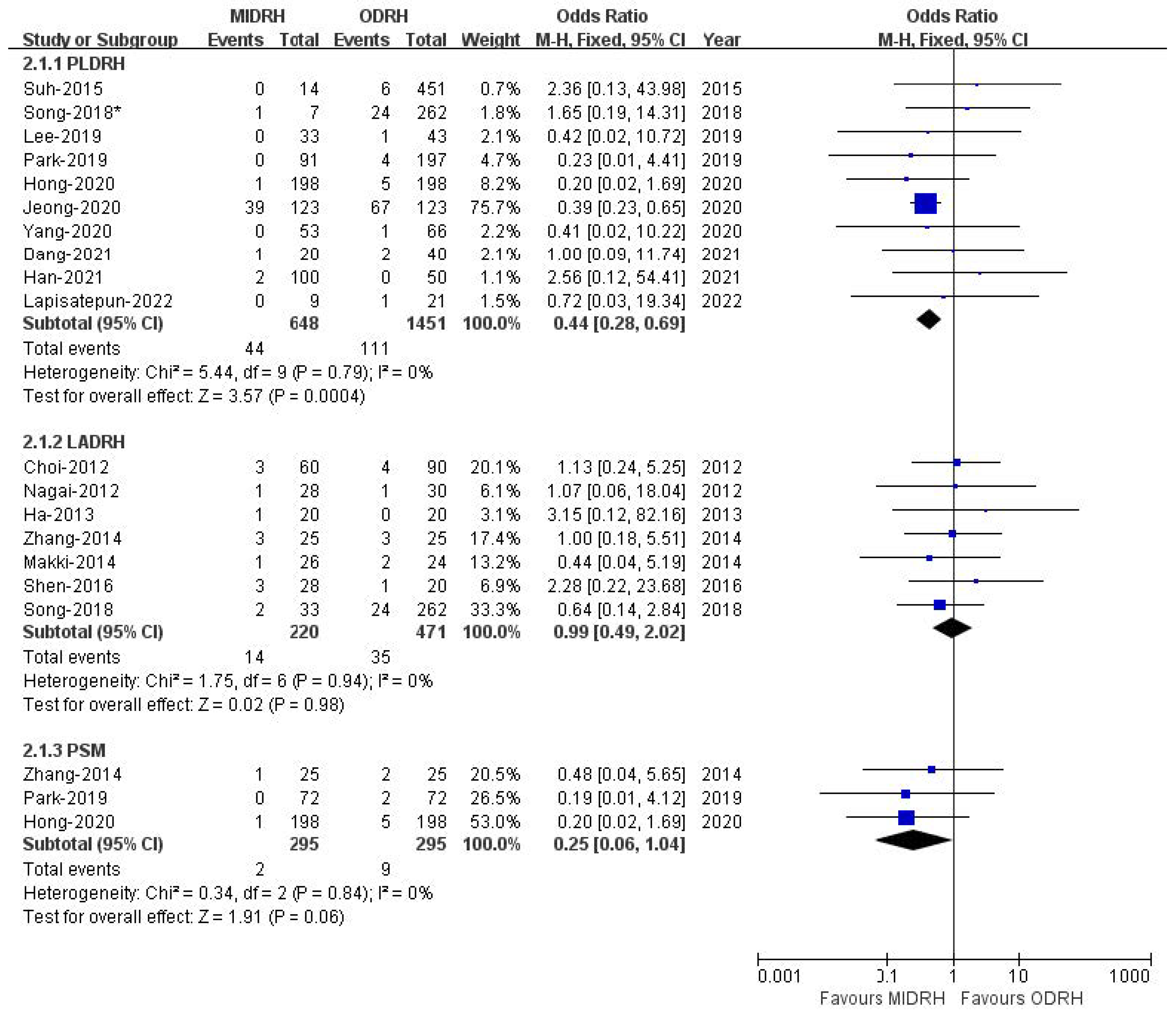
2.5. Pulmonary Complications
2.6. Postoperative Transfusion
2.7. Wound
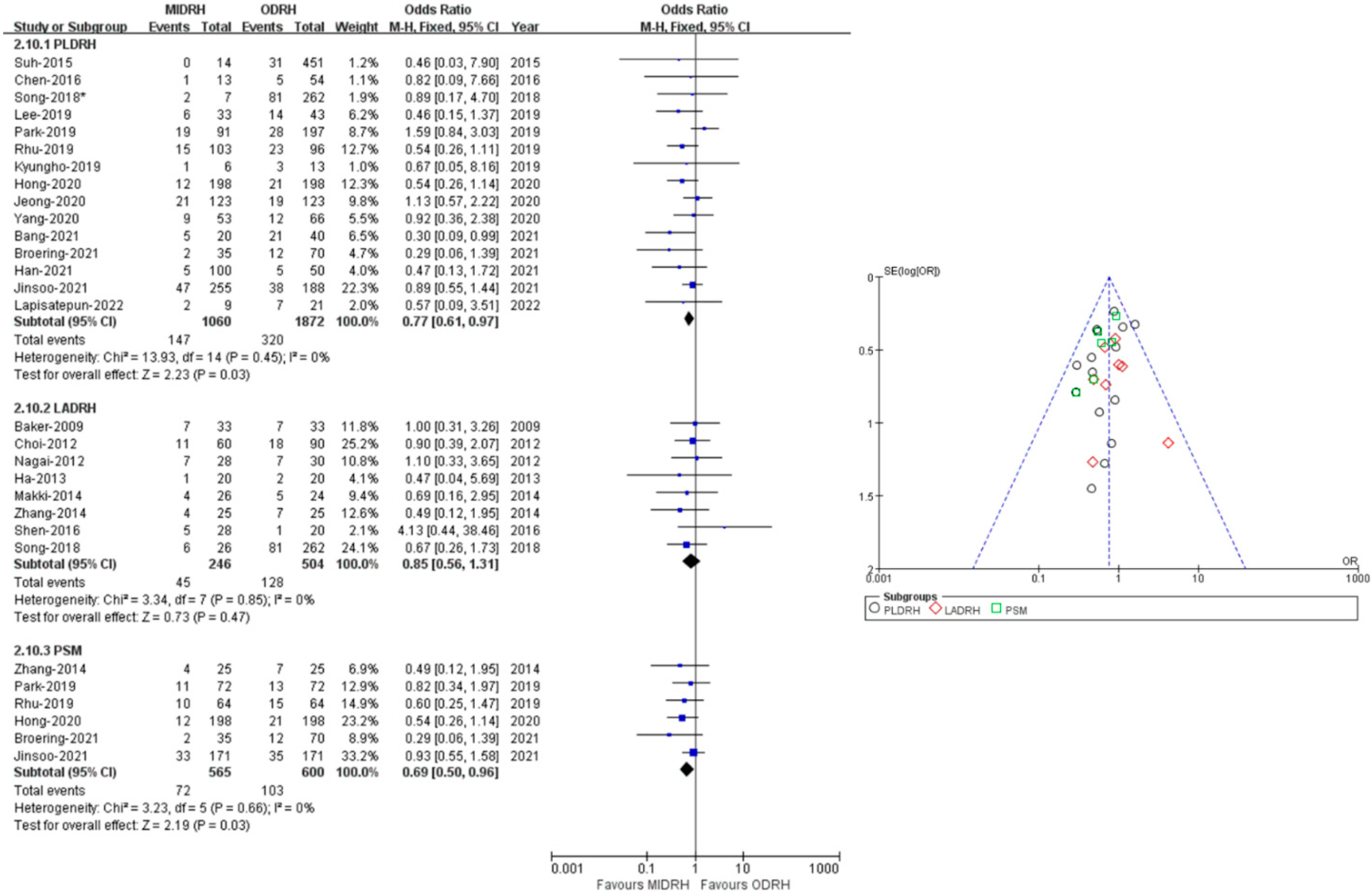
2.8. Overall Complication Rate
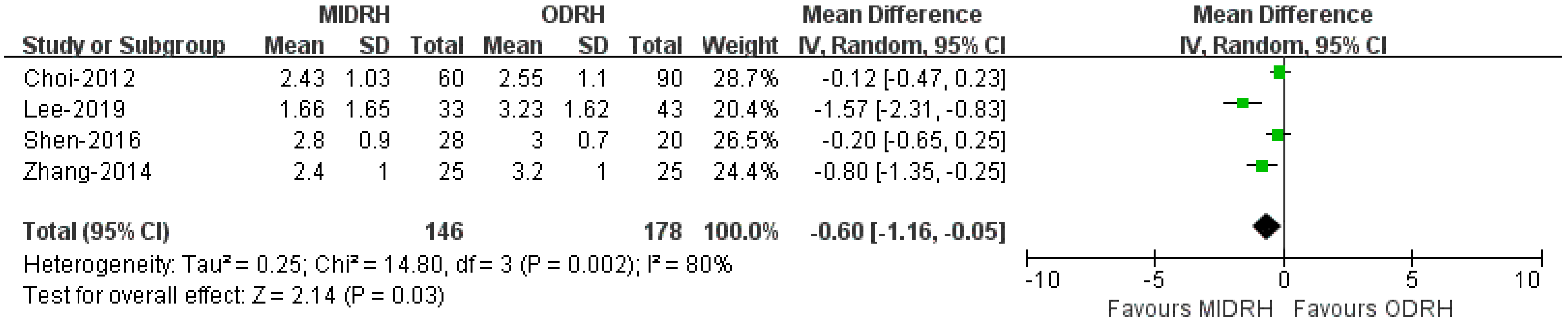
2.9. Self-Infused Morphine Consumption (Days)
2.10. Other Outcomes
2.11. Publication Bias
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lo, C.-M.; Fan, S.T.; Liu, C.L.; Yong, B.H.; Wong, Y.; Lau, G.K.; Lai, C.L.; Ng, I.O.; Wong, J. Lessons Learned from One Hundred Right Lobe Living Donor Liver Transplants. Ann. Surg. 2004, 240, 151–158. [Google Scholar] [CrossRef]
- Cherqui, D.; Ciria, R.; Kwon, C.H.D.; Kim, K.-H.; Broering, D.; Wakabayashi, G.; Samstein, B.; Troisi, R.; Han, H.S.; Rotellar, F.; et al. Expert Consensus Guidelines on Minimally Invasive Donor Hepatectomy for Living Donor Liver Transplantation from Innovation to Implementation: A Joint Initiative from the International Laparoscopic Liver Society (ILLS) and the Asian-Pacific Hepato-Pancreato-Biliary Association (A-PHPBA). Ann. Surg. 2021, 273, 96–108. [Google Scholar] [PubMed]
- Soubrane, O.; Perdigao Cotta, F.; Scatton, O. Pure laparoscopic right hepatectomy in a living donor. Am. J. Transplant. 2013, 13, 2467–2471. [Google Scholar] [CrossRef] [PubMed]
- Han, E.S.; Lee, K.-W.; Suh, K.-S.; Yi, N.-J.; Choi, Y.; Hong, S.K.; Lee, J.-M.; Hong, K.P.; Hong, S.Y.; Suh, S. Shorter operation time and improved surgical outcomes in laparoscopic donor right hepatectomy compared with open donor right hepatectomy. Surgery 2021, 170, 1822–1829. [Google Scholar] [CrossRef] [PubMed]
- Lapisatepun, W.; Junrungsee, S.; Chotirosniramit, A.; Udomsin, K.; Lapisatepun, W.; Chanthima, P.; Boonsri, S.; Lorsomradee, S. Comparative outcomes of pure laparoscopic and open donor right hepatectomy: The first report from a Southeast Asian transplant center. BMC Surg. 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Hong, K.; Hong, S.K.; Han, E.S.; Suh, S.; Hong, S.Y.; Lee, J.-M.; Choi, Y.; Yi, N.-J.; Lee, K.-W.; Suh, K.-S. Pure Laparoscopic vs. Open Right Hepatectomy in Living Liver Donors: Bench-Surgery Time. Front. Surg. 2021, 8, 771026. [Google Scholar] [CrossRef]
- Baker, T.B.; Jay, C.L.; Ladner, D.P.; Preczewski, L.B.; Clark, L.; Holl, J.; Abecassis, M.M. Laparoscopy-assisted and open living donor right hepatectomy: A comparative study of outcomes. Surgery 2009, 146, 817–825. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; You, Y.K.; Na, G.H.; Hong, T.H.; Shetty, G.S.; Kim, D.G. Single-port laparoscopy-assisted donor right hepatectomy in living donor liver transplantation: Sensible approach or unnecessary hindrance? Transplant. Proc. 2012, 44, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Nagai, S.; Brown, L.; Yoshida, A.; Kim, D.; Kazimi, M.; Abouljoud, M.S. Mini-incision right hepatic lobectomy with or without laparoscopic assistance for living donor hepatectomy. Liver Transplant. 2012, 18, 1188–1197. [Google Scholar] [CrossRef]
- Ha, T.; Hwang, S.; Ahn, C.; Kim, K.; Moon, D.; Song, G.; Jung, D.; Park, G.; Namgoong, J.; Park, C.; et al. Role of Hand-Assisted Laparoscopic Surgery in Living-Donor Right Liver Harvest. Transplant. Proc. 2013, 45, 2997–2999. [Google Scholar] [CrossRef]
- Makki, K.; Chorasiya, V.K.; Sood, G.; Srivastava, P.K.; Dargan, P.; Vij, V. Laparoscopy-assisted hepatectomy versus conventional (open) hepatectomy for living donors: When you know better, you do better. Liver Transplant. 2014, 20, 1229–1236. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, J.; Yan, L.; Li, B.; Wen, T.; Xu, M.; Wang, W.; Zhao, J.; Wei, Y. Comparison of Laparoscopy-Assisted and Open Donor Right Hepatectomy: A Prospective Case-Matched Study from China. J. Gastrointest. Surg. 2014, 18, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.; Lee, K.; Lee, J.; Choi, Y.; Yi, N.; Suh, K. Clinical outcomes of and patient satisfaction with different incision methods for donor hepatectomy in living donor liver transplantation. Liver Transplant. 2015, 21, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Wu, C.; Hu, R.; Ho, C.; Lee, P.; Lai, H.; Lin, M.; Wu, Y. Robotic liver donor right hepatectomy: A pure, minimally invasive approach. Liver Transplant. 2016, 22, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Zhang, W.; Jiang, L.; Yan, L.; Yang, J. Comparison of Upper Midline Incision with and without Laparoscopic Assistance for Living-Donor Right Hepatectomy. Transplant. Proc. 2016, 48, 2726–2731. [Google Scholar] [CrossRef]
- Song, J.-L.; Yang, J.; Wu, H.; Yan, L.-N.; Wen, T.-F.; Wei, Y.-G.; Yang, J.-Y. Pure laparoscopic right hepatectomy of living donor is feasible and safe: A preliminary comparative study in China. Surg. Endosc. 2018, 32, 4614–4623. [Google Scholar] [CrossRef]
- Lee, B.; Choi, Y.; Han, H.; Yoon, Y.; Cho, J.Y.; Kim, S.; Kim, K.H.; Hyun, I.G. Comparison of pure laparoscopic and open living donor right hepatectomy after a learning curve. Clin. Transplant. 2019, 33, e13683. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kwon, D.C.H.; Choi, G.-S.; Kim, S.J.; Lee, S.-K.; Kim, J.M.; Lee, K.W.; Chung, Y.J.; Kim, K.S.; Lee, J.S.; et al. Safety and Risk Factors of Pure Laparoscopic Living Donor Right Hepatectomy: Comparison to Open Technique in Propensity Score–matched Analysis. Transplantation 2019, 103, e308–e316. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Shehta, A.; Lee, J.-M.; Hong, S.K.; Yoon, K.C.; Cho, J.-H.; Yi, N.-J.; Lee, K.-W.; Suh, K.-S. Pure 3D laparoscopy versus open right hemihepatectomy in a donor with type II and III portal vein variations. Ann. Hepato-Biliary-Pancreat. Surg. 2019, 23, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.S.; Wi, W.; Chung, Y.J.; Kim, J.M.; Choi, G.-S.; Kwon, C.H.D.; Han, S.; Gwak, M.S.; Kim, G.S.; Ko, J.S. Comparison of perioperative outcomes between pure laparoscopic surgery and open right hepatectomy in living donor hepatectomy: Propensity score matching analysis. Sci. Rep. 2020, 10, 5314. [Google Scholar] [CrossRef]
- Rhu, J.; Choi, G.; Kwon, C.H.D.; Kim, J.M.; Joh, J. Learning curve of laparoscopic living donor right hepatectomy. Br. J. Surg. 2020, 107, 278–288. [Google Scholar] [CrossRef]
- Yang, J.; Kim, J.M.; Rhu, J.; Kim, S.; Lee, S.; Choi, G.-S.; Joh, J.-W. Comparison of liver regeneration in laparoscopic versus open right hemihepatectomy for adult living donor liver transplantation. Ann. Hepato-Biliary-Pancreat. Surg. 2020, 24, 33–37. [Google Scholar] [CrossRef]
- Bang, Y.J.; Jun, J.H.; Gwak, M.S.; Ko, J.S.; Kim, J.M.; Choi, G.S.; Joh, J.W.; Kim, G.S. Postoperative outcomes of purely laparoscopic donor hepatectomy compared to open living donor hepatectomy: A preliminary observational study. Ann. Surg. Treat. Res. 2021, 100, 235–245. [Google Scholar] [CrossRef]
- Rho, S.Y.; Lee, J.G.; Joo, D.J.; Kim, M.S.; Kim, S.I.; Han, D.H. Outcomes of Robotic Living Donor Right Hepatectomy from 52 Consecutive Cases: Comparison with Open and Laparoscopy-Assisted Donor Hepatectomy. HPB 2021, 23, S105. [Google Scholar] [CrossRef]
- Rhu, J.; Kim, M.S.; Choi, G.; Kim, J.M.; Kwon, C.H.D.; Joh, J. Laparoscopic Living Donor Right Hepatectomy Regarding the Anatomical Variation of the Portal Vein: A Propensity Score–Matched Analysis. Liver Transplant. 2021, 27, 984–996. [Google Scholar] [CrossRef]
- Hong, S.K.; Tan, M.Y.; Worakitti, L.; Lee, J.M.; Cho, J.H.; Yi, N.J. Pure Laparoscopic Versus Open Right Hepatectomy in Live Liver Donors: A Propensity Score-matched Analysis. Ann. Surg. 2020, 275, e206–e212. [Google Scholar] [CrossRef]
- Broering, D.C.; Elsheikh, Y.; Alnemary, Y.; Zidan, A.; Elsarawy, A.; Saleh, Y.; Alabbad, S.; Sturdevant, M.; Wu, Y.M.; Troisi, R.I. Robotic Versus Open Right Lobe Donor Hepatectomy for Adult Living Donor Liver Transplantation: A Propensity Score-Matched Analysis. Liver Transplant. 2020, 26, 1455–1464. [Google Scholar] [CrossRef]
- Yeow, M.; Soh, S.; Starkey, G.; Perini, M.V.; Koh, Y.X.; Tan, E.K.; Chan, C.Y.; Raj, P.; Goh, B.K.P.; Kabir, T. A systematic review and network meta-analysis of outcomes after open, mini-laparotomy, hybrid, totally laparoscopic, and robotic living donor right hepatectomy. Surgery 2022, 172, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.-M.; Fan, S.-T.; Liu, C.-L.; Wei, W.; Lo, R.J.W.; Lai, C.-L.; Chan, J.K.F.; Ng, I.O.-L.; Fung, A.; Wong, J. Adult-to-adult living donor liver transplantation using extended right lobe grafts. Ann. Surg. 1997, 226, 261–270. [Google Scholar] [CrossRef]
- Nguyen, K.T.; Gamblin, T.C.; Geller, D.A. World review of laparoscopic liver resection-2804 patients. Ann. Surg. 2009, 250, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wu, Y.-R.; Wu, B.; Lu, M.-Q. Surgical and oncologic outcomes following laparoscopic versus open liver resection for hepatocellular carcinoma: A meta-analysis. Hepatol. Res. 2012, 42, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Mirnezami, R.; Mirnezami, A.H.; Chandrakumaran, K.; Abu Hilal, M.; Pearce, N.W.; Primrose, J.N.; Sutcliffe, R.P. Short- and long-term outcomes after laparoscopic and open hepatic resection: Systematic review and meta-analysis. HPB 2011, 13, 295–308. [Google Scholar] [CrossRef]
- Mizuguchi, T.; Kawamoto, M.; Meguro, M.; Shibata, T.; Nakamura, Y.; Kimura, Y.; Furuhata, T.; Sonoda, T.; Hirata, K. Laparoscopic hepatectomy: A systematic review, meta-analysis, and power analysis. Surg. Today 2011, 41, 39–47. [Google Scholar] [CrossRef]
- Marubashi, S.; Nagano, H. Laparoscopic living-donor hepatectomy: Review of its current status. Ann. Gastroenterol. Surg. 2021, 5, 484–493. [Google Scholar] [CrossRef]
- Au, K.P.; Chok, K.S.H. Minimally invasive donor hepatectomy, are we ready for prime time? World J. Gastroenterol. 2018, 24, 2698–2709. [Google Scholar] [CrossRef]
- Hori, T.; Kaido, T.; Iida, T.; Yagi, S.; Uemoto, S. Comprehensive guide to laparoscope-assisted graft harvesting in live donors for living-donor liver transplantation: Perspective of laparoscopic vision. Ann. Gastroenterol. 2017, 30, 118–126. [Google Scholar] [CrossRef]
- Cauchy, F.; Schwarz, L.; Scatton, O.; Soubrane, O. Laparoscopic liver resection for living donation: Where do we stand? World J. Gastroenterol. 2014, 20, 15590–15598. [Google Scholar] [CrossRef] [PubMed]
- Lai, Q.; Pinheiro, R.; Sandri, G.B.L.; Spoletini, G.; Melandro, F.; Guglielmo, N.; Di Laudo, M.; Frattaroli, F.M.; Berloco, P.B.; Rossi, M. Laparoscopy in Liver Transplantation: The Future Has Arrived. HPB Surg. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wu, W.; Liu, C.; Liu, T.; Xiao, H. Comparison of laparoscopic and open living donor hepatectomy: A meta-analysis. Medicine 2021, 100, e26708. [Google Scholar] [CrossRef]
- Li, H.; Zhang, J.-B.; Chen, X.-L.; Fan, L.; Wang, L.; Li, S.-H.; Zheng, Q.-L.; Wang, X.-M.; Yang, Y.; Chen, G.-H.; et al. Different techniques for harvesting grafts for living donor liver transplantation: A systematic review and meta-analysis. World J. Gastroenterol. 2017, 23, 3730–3743. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xu, L.; Zhang, J.; Che, X. Safety and feasibility of laparoscopic living donor right hepatectomy for adult liver transplantation: A meta-analysis. HPB 2021, 23, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Lei, Z.; Gao, F.; Yang, J.; Xie, Q.; Jiang, K.; Jie, G. Minimally invasive versus open living donors right hepatectomy: A systematic review and meta-analysis. Int. J. Surg. 2021, 95, 106152. [Google Scholar] [CrossRef]
- Menon, K.; Papoulas, M.; Hakeem, A.; Heaton, N. Pure laparoscopic versus open donor hepatectomy for adult living donor liver transplantation–A systematic review and meta-analysis. J. Minimal Access Surg. 2022, 18, 1. [Google Scholar] [CrossRef]
- Zhang, B.; Pan, Y.; Chen, K.; Maher, H.; Chen, M.-Y.; Zhu, H.-P.; Zhu, Y.-B.; Dai, Y.; Chen, J.; Cai, X.-J. Laparoscopy-Assisted versus Open Hepatectomy for Live Liver Donor: Systematic Review and Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2017, 2017, 1–12. [Google Scholar] [CrossRef]
- Xu, J.; Hu, C.; Cao, H.-L.; Zhang, M.-L.; Ye, S.; Zheng, S.-S.; Wang, W.-L. Meta-Analysis of Laparoscopic versus Open Hepatectomy for Live Liver Donors. PLoS ONE 2016, 11, e0165319. [Google Scholar] [CrossRef]
- Peng, Y.; Li, B.; Xu, H.; Chen, K.; Wei, Y.; Liu, F. Pure Laparoscopic Versus Open Approach for Living Donor Right Hepatectomy: A Systematic Review and Meta-Analysis. J. Laparoendosc. Adv. Surg. Tech. Part A 2022, 32, 832–841. [Google Scholar] [CrossRef]
- Lai, Q.; Giovanardi, F.; Mennini, G.; Berardi, G.; Rossi, M. The impact of mini-invasive right hepatectomy in the setting of living donation: A meta-analysis. Updat. Surg. 2022, 74, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, C.; Nezhat, F.; Nezhat, C.; Seidman, D.S. Operative laparoscopy: Redefining the limits. J. Soc. Laparoendosc. Surg. 1997, 1, 213–216. [Google Scholar]
- Rhu, J.; Choi, G.S.; Kim, J.M.; Joh, J.; Kwon, C.H.D. Feasibility of total laparoscopic living donor right hepatectomy compared with open surgery: Comprehensive review of 100 cases of the initial stage. J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.H.D.; Choi, G.-S.; Kim, J.M.; Cho, C.W.; Rhu, J.; Soo Kim, G.; Hyun, S.D.; Jae-Won, J. Laparoscopic Donor Hepatectomy for Adult Living Donor Liver Transplantation Recipients. Liver Transplant. 2018, 24, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.K.; Lee, K.W.; Choi, Y.; Kim, H.S.; Ahn, S.W.; Yoon, K.C.; Yi, N.J.; Suh, K.S. Initial experience with purely laparoscopic living-donor right hepatectomy. Br. J. Surg. 2018, 105, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Riquelme, F.; Muñoz, C.; Ausania, F.; Hessheimer, A.J.; Torres, F.; Calatayud, D.; Sandomenico, R.; Pérez, R.G.; Ferrer, J.; Fuster, J.; et al. Laparoscopic versus open hemihepatectomy: Comprehensive comparison of complications and costs at 90 days using a propensity method. Updat. Surg. 2020, 72, 1041–1051. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author–Year | Country | Study Type | Study Interval | Sample | Sexy M/F | Age | BMI | PGV | NOS | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIDRH | ODRH | MIDRH | ODRH | MIDRH | ODRH | MIDRH | ODRH | MIDRH | ODRH | |||||
| LADRH | ||||||||||||||
| Baker [7]-2009 | USA | RS | 2004–2007 | 33 | 33 | 15/18 | 13/20 | 37 ± 10.3 | 39.1± 11.1 | 25.8 ± 4.1 | 25.9 ± 4.3 | 900 ± 215 | 914 ± 160 | 8 |
| Choi [12]-2012 | Korea | RS | 2008–2011 | 60 | 90 | 35/25 | 58/32 | 32.23 ± 10.3 | 36.8 ± 12.01 | 23.33 ± 2.64 | 23.6 ± 2.94 | NA | NA | 9 |
| Nagai [13]-2012 | USA | RS | 2000–2011 | 28 | 30 | 15/13 | 9/21 | 34.3 ± 10.1 | 38.6 ± 9.4 | 24.0 ± 3.3 | 30.1 ± 5.1 | 915 ± 361 | 800 ± 184 | 8 |
| Ha [14]-2013 | Korea | DCC | 2012–2012 | 20 | 20 | 11/9 | 17/3 | 25 ± 5.5 | 29 ± 11.1 | 23.3 ± 4.0 | 23.6 ± 3.2 | 725.1 ± 135.5 | 755.3 ± 95.7 | 8 |
| Zhang [16]-2014 | China | PSM | 2011–2013 | 25 | 25 | 13/12 | 14/11 | 37.2 ± 8.7 | 37.4 ± 10.5 | 23.8 ± 2.6 | 22.6 ± 3.0 | 629.9 ± 128.9 | 575.2 ± 136.3 | 9 |
| Makki [15]-2014 | India | RS | 2011–2013 | 26 | 24 | 13/13 | 18/6 | 27.46 ± 9.40 | 32.42 ± 8.47 | 24.23 ± 3.64 | 24.46 ± 4.39 | 755.50 ± 87.94 | 725.79 ± 134.35 | 8 |
| Shen [19]-2016 | China | RS | 2011–2013 | 28 | 20 | 15/13 | 13/7 | 40.4 ± 11.1 | 38.3 ± 11.4 | 23.1 ± 1.8 | 21.9 ± 1.9 | 634.2 ± 124.2 | 572.9 ± 122.5 | 8 |
| Song [20]-2018 | China | RS | 2001- 2017 | 26 | 262 | 15/11 | 148/114 | 40.62± 11.08 | 36.21 ± 11.00 | 23.26 ± 2.55 | 22.95 ± 2.61 | NA | NA | 8 |
| PLDRH | ||||||||||||||
| Suh [17]-2015 | Korea | RS | 2010–2013 | 14 | 415 | 1/13 | 304/111 | 24.9 ± 8.7 | 32.43 ± 9.54 | 20.9 ± 2.9 | 23.08 ± 3.12 | NA | NA | 8 |
| Chen [18]-2016 | China | RS | 2013–2015 | 13 | 54 | 4/9 | 24/30 | NA | NA | 21.94 ± 2.99 | 23.08 ± 3.52 | 605.64 ± 140.47 | NA | 8 |
| Song [20]-2018 * | China | RS | 2001–2017 | 7 | 262 | 3/4 | 148/114 | 42.71 ± 5.65 | 36.21 ± 11.00 | 23.50 ± 3.23 | 22.95 ± 2.61 | NA | NA | 7 |
| Kyungho [23]-2019 | Korea | RS | 2014–2016 | 6 | 13 | 3/3 | 6/7 | 30.33 ± 12.7 | 33.85 ± 11.8 | 23.1 ± 2.8 | 23.5 ± 3.4 | NA | NA | 8 |
| Lee [21]-2019 | Korea | RS | 2010–2017 | 33 | 43 | 19/14 | 21/22 | 31.4 ± 9.76 | 35.81 ± 10.62 | 23.97 ± 6.76 | 23.07 ± 3.00 | 750.0 ± 194 | 725.4 ± 158 | 9 |
| Park [22]-2019 | Korea | RS | 2013–2017 | 91 | 197 | 49/42 | 123/74 | 27.23 ± 7.13 | 32.23 ± 6.18 | 22.69 ± 3.52 | 23.44 ± 3.57 | 696 ± 153 | 703 ± 168 | 9 |
| Rhu [25]-2019 | Korea | RS | 2014–2018 | 103 | 96 | 58/45 | 61/35 | 35.6 ± 13.2 | 33.3 ± 11.1 | 23.8 ± 2.9 | 23.7 ± 3.1 | 757 ± 171 | 745 ± 169 | 9 |
| Hong [30]-2020 | Korea | RS, PSM | 2010–2018 | 198 | 198 | 119/79 | 120/78 | 33.1 ± 10.6 | 34.1 ± 11.2 | 23.7 ± 3.4 | 23.9 ± 3.2 | NA | NA | 9 |
| Yang [26]-2020 | Korea | RS | 2016–2017 | 53 | 66 | 25/28 | 36/30 | 32.79 ± 11.92 | 35.70 ± 12.71 | 23.49 ± 2.79 | 23.64 ± 2.68 | NA | NA | 7 |
| Bang [27]-2021 | Korea | RS | 2015–2017 | 20 | 40 | 12/8 | 25/15 | 28.1 ± 9.2 | 34.55 ± 11.77 | 23.7 ± 2.7 | 23.75 ± 2.84 | NA | NA | 8 |
| Broering [31]-2021 | Italy | PSM | 2015–2019 | 35 | 70 | 22/13 | 46/24 | 29.09 ± 6.02 | 26.85 ± 5.91 | 23.4 ± 2.84 | 24.1 ± 3.20 | 701 ± 148 | 701 ± 133 | 9 |
| Han [4]-2021 | Korea | RS | 2012–2019 | 100 | 50 | 50/50 | 31/19 | 32.86 ± 9.82 | 33.0 ± 10.4 | 22.82 ± 2.94 | 23.4 ± 3.2 | 674.89 ± 130.12 | 722.1 ± 142.0 | 8 |
| Kwangpyo [6]-2021 | Korea | RS | 2012–2019 | 267 | 247 | 151/116 | 160/87 | 33.2 ± 10.8 | 34.9 ± 11.9 | 23.7 ± 3.3 | 23.3 ± 3.3 | 716.7 ± 140.1 | 732.9 ± 153.5 | 8 |
| Rho [28]-2021 | Republic of Korea | RS | 2016–2019 | 170 | 62 | NA | NA | 34.36 ± 11.78 | 28.7 ± 8.3 | 23.03 ± 2.41 | 22.1 ± 2.4 | 764.85 ± 136.43 | 731.3 ± 124.2 | 8 |
| Jinsoo Rhu [29]-2021 | Korea | RS | 2014–2019 | 255 | 188 | 147/108 | 116/72 | 30.12 ± 3.2 | 34.15 ± 4.05 | 23.4 ± 2.8 | 23.5 ± 3.0 | NA | NA | 8 |
| Lapisatepun [5]-2022 | Thailand | RS | 2015–2021 | 9 | 21 | 1/8 | 8/13 | 35.11 ± 4.52 | 40.64 ± 4.37 | 22.47 ± 1.0 | 22.02 ± 1.11 | 701.91 ± 50.56 | 724.94 ± 55.62 | 8 |
| Jeong [24]-2020 | Korea | RS, PSM | 2013–2018 | 123 | 123 | 71/52 | 73/50 | 30.24 ± 3.70 | 31 ± 3.11 | NA | NA | NA | NA | 9 |
| PSM | ||||||||||||||
| Zhang [16]-2014 | China | PSM | 2011–2013 | 25 | 25 | 13/12 | 14/11 | 37.2 ± 8.7 | 37.4 ± 10.5 | 23.8 ± 2.6 | 22.6 ± 3.0 | 629.9 ± 128.9 | 575.2 ± 136.3 | 9 |
| Park [22]-2019 | Korea | PSM | 2013–2017 | 72 | 72 | 40/32 | 43/39 | 28.5 ± 15 | 29.5 ± 11.5 | 23.51 ± 2.83 | 23.36 ± 3.25 | 695.5 ± 154.5 | 716.5 ± 177.5 | 8 |
| Rhu [25]-2019 | Korea | PSM | 2014–2018 | 64 | 64 | 39/25 | 38/26 | 33.6 ± 12.8 | 34.1 ± 11.4 | 23.3 ± 3.2 | 24 ± 3.2 | 761 ± 125 | 764 ± 172 | 8 |
| Hong [30]-2020 | Korea | RS, PSM | 2010–2018 | 198 | 198 | 119/79 | 120/78 | 33.1 ± 10.6 | 34.1 ± 11.2 | 23.7 ± 3.4 | 23.9 ± 3.2 | NA | NA | 8 |
| Broering [31]-2021 | Italy | PSM | 2015–2019 | 35 | 70 | 22/13 | 46/24 | 29.09 ± 6.02 | 26.85 ± 5.91 | 23.4 ± 2.84 | 24.1 ± 3.20 | 701 ± 148 | 701 ± 133 | 8 |
| Jinsoo Rhu [29]-2021 | Korea | PSM | 2014–2020 | 171 | 171 | 104/67 | 105/66 | 34.12 ± 3.92 | 34.12 ± 3.92 | 23.3 ± 2.7 | 23.4 ± 3.0 | NA | NA | 8 |
| Jeong [24]-2020 | Korea | RS, PSM | 2013–2018 | 123 | 123 | 71/52 | 73/50 | 30.24 ± 3.70 | 31 ± 3.11 | NA | NA | NA | NA | 8 |
| Variables | No. of Studies | No. of Patients # | MIDRH | ODRH | OR, M-H Fixed, 95% CI OR, Fixed, Random, 95% CI MD, Random, 95% CI | p Value | I2 |
|---|---|---|---|---|---|---|---|
| Age, years | 23 | 4079 | 32.4 ± 9.8 | 34.0 ± 14.9 | −2.41 [−3.74, −1.09] | 0.0004 | 76% |
| PLDRH vs. ODRH | 15 | 3329 | 32.1 ± 9.6 | 33.5 ± 15.6 | −2.64 [−4.23, 1.05] | <0.00001 | 81% |
| LADRH vs. ODRH | 8 | 750 | 34.3 ± 10.9 | 36.3 ± 11.1 | −1.84 [−4.36, 0.69] | 0.04 | 76% |
| Gender (Female) | 23 | 4260 | 706 (44.9%) | 995 (37.0%) | 1.31 [1.06, 1.62] | 0.01 | 42% |
| PLDRH vs. ODRH | 15 | 3510 | 592 (44.6%) | 781 (35.8%) | 1.35 [1.06, 1.73] | 0.02 | 47% |
| LADRH vs. ODRH | 8 | 750 | 114 (46.3%) | 214 (42.5%) | 1.20 [0.76, 1.89] | 0.79 | 37% |
| BMI, kg/m2 | 23 | 4146 | 23.4 ± 3.2 | 23.4 ± 3.3 | −0.14 [−0.53, 0.24] | 0.46 | 64% |
| PLDRH vs. ODRH | 15 | 3396 | 23.4 ± 3.2 | 23.3 ± 3.1 | −0.08 [−0.41, 0.25] | 0.63 | 41% |
| LADRH vs. ODRH | 8 | 750 | 23.8 ± 3.2 | 23.7 ± 3.6 | −0.38 [−1.58, 0.82] | 0.54 | 81% |
| PGV | 15 | 1973 | 730.5 ± 166.4 | 720.8 ± 159.3 | −1.47 [−14.37, 11.44] | 0.82 | 30% |
| PLDRH vs. ODRH | 9 | 1661 | 723.1 ± 149.3 | 717.3 ± 152.9 | −7.25 [−21.36, 6.87] | 0.31 | 21% |
| LADRH vs. ODRH | 6 | 312 | 768.6 ± 231.9 | 740.3 ± 190.4 | 27.90 [−3.93, 59.74] | 0.09 | 16% |
| Variables | No. of Studies | No. of Patients # | MIDRH | ODRH | OR, M-H Fixed, 95% CI OR, Fixed, Random, 95% CI MD, Random, 95% CI | p Value | I2 |
|---|---|---|---|---|---|---|---|
| Intraoperative blood loss | 24 | 4329 | 283.6 ± 221.8 | 431.4 ± 342.0 | −57.86 [−77.58, −38.14] | <0.00001 | 81% |
| Operative time | 23 | 3858 | 330.5 ± 116.1 | 334.6 ± 96.1 | 30.77 [9.03, 52.51] | 0.006 | 97% |
| Length of Hospital stay | 20 | 3477 | 8.3 ± 3.0 | 9.7 ± 3.3 | −1.22 [−1.62, −0.83] | <0.00001 | 89% |
| Pulmonary complications | 9 | 2790 | 58 (6.7%) | 146 (7.6%) | 0.55 [0.38, 0.81] | 0.002 | 0% |
| Wound | 20 | 3125 | 20 (2.0%) | 81 (3.8%) | 0.45 [0.29, 0.71] | 0.0007 | 0% |
| Total complications | 22 | 3682 | 192 (14.7%) | 448 (18.9%) | 0.79 [0.64, 0.96] | 0.02 | 0% |
| Postoperative transfusion | 9 | 1553 | 20 (2.6%) | 20 (1.6%) | 1.78 [0.88, 3.59] | 0.11 | 0% |
| PLDRH vs. ODRH | 5 | 1017 | 17 (4.2%) | 11 (1.8%) | 2.90 [1.15, 7.28] | 0.02 | 0% |
| LADRH vs. ODRH | 4 | 536 | 3 (2.1%) | 9 (2.3%) | 0.68 [0.19, 2.41] | 0.55 | 0% |
| PSM | 2 | 470 | 11 (4.7%) | 2 (0.85%) | 4.78 [1.20, 18.95] | 0.03 | 0% |
| Bleeding | 13 | 2404 | 11 (1.5%) | 21 (1.3%) | 1.20 [0.59, 2.45] | 0.63 | 0% |
| PLDRH vs. ODRH | 8 | 1810 | 5 (0.9%) | 17 (1.4%) | 0.80 [0.32, 2.00] | 0.14 | 0% |
| LADRH vs. ODRH | 6 | 594 | 6 (3.6%) | 4 (0.94%) | 2.56 [0.73, 9.05] | 0.62 | 0% |
| Peak AST | 18 | 3030 | 226.0 ± 104.6 | 219.2 ± 121.1 | 10.83 [−12.57, 34.23] | 0.36 | 96% |
| PLDRH vs. ODRH | 11 | 2366 | 220.4 ± 82.9 | 211.3 ± 107.8 | 13.43 [−15.69, 42.56] | 0.37 | 98% |
| LADRH vs. ODRH | 7 | 664 | 250.1 ± 166.8 | 245.0 ± 154.3 | 0.39 [−26.86, 27.65] | 0.98 | 44% |
| PSM | 5 | 1060 | 214.1 ± 80.9 | 219.2 ± 77.0 | −16.97 [−59.34, 25.40] | 0.43 | 98% |
| Peak ALT | 18 | 3050 | 234.5 ± 112.5 | 225.7 ± 135.0 | 18.92 [−10.26, 48.10] | 0.2 | 96% |
| PLDRH vs. ODRH | 11 | 2366 | 226.8 ± 94.4 | 216.4 ± 123.4 | 21.07 [−15.99, 58.12] | 0.27 | 97% |
| LADRH vs. ODRH | 7 | 684 | 264.3 ± 161.9 | 255.9 ± 163.7 | 9.67 [−26.24, 45.57] | 0.6 | 56% |
| PSM | 5 | 1060 | 226.1 ± 93.2 | 234.4 ± 93.0 | −23.43 [−75.74, 28.89] | 0.38 | 99% |
| Peak TB | 17 | 3010 | 3.1 ± 1.6 | 3.1 ± 1.6 | −0.08 [−0.26, 0.09] | 0.36 | 83% |
| PLDRH vs. ODRH | 11 | 2366 | 3.2 ± 1.6 | 3.0 ± 1.6 | −0.04 [−0.25, 0.18] | 0.73 | 88% |
| LADRH vs. ODRH | 6 | 644 | 2.6 ± 1.4 | 3.2 ± 1.6 | −0.21 [−0.42, −0.00] | 0.05 | 0% |
| PSM | 5 | 1060 | 3.3 ± 1.5 | 5.4 ± 12.2 | 0.08 [−0.38, 0.53] | 0.74 | 96% |
| Bile leak | 17 | 2958 | 37 (3.9%) | 56 (2.8%) | 1.28 [0.84, 1.97] | 0.26 | 15% |
| PLDRH vs. ODRH | 12 | 2346 | 29 (3.8%) | 38 (2.4%) | 1.46 [0.88, 2.46] | 0.14 | 21% |
| LADRH vs. ODRH | 5 | 612 | 8 (4.7%) | 18 (4.1%) | 0.90 [0.38, 2.11] | 0.81 | 5% |
| PSM | 5 | 823 | 12 (3.0%) | 10 (2.3%) | 1.32 [0.57, 3.08] | 0.52 | 0% |
| Clavien–Dindo grade ≥ III | 18 | 2904 | 47 (4.8%) | 89 (4.6%) | 1.06 [0.71, 2.24] | 0.93 | 0% |
| PLDRH vs. ODRH | 13 | 2260 | 36 (4.5%) | 58 (3.9%) | 1.07 [0.67, 1.72] | 0.77 | 0% |
| LADRH vs. ODRH | 6 | 644 | 11 (5.7%) | 31 (6.9%) | 1.04 [0.48, 2.24] | 0.93 | 0% |
| PSM | 6 | 1165 | 32 (5.7%) | 29 (4.8%) | 1.14 [0.68, 1.91] | 0.63 | 0% |
| Re-hospital | 7 | 1340 | 21 (6.5%) | 39 (3.8%) | 1.18 [0.68, 2.04] | 0.56 | 0% |
| PLDRH vs. ODRH | 5 | 902 | 14 (5.9%) | 27 (4.1%) | 1.16 [0.60, 2.25] | 0.66 | 0% |
| LADRH vs. ODRH | 2 | 438 | 7 (8.1%) | 12 (3.4%) | 1.21 [0.45, 3.25] | 0.71 | 0% |
| PSM | 3 | 332 | 12 (7.7%) | 15 (8.5%) | 0.87 [0.40, 1.93] | 0.74 | 0% |
| Reoperation | 13 | 2143 | 22 (3%) | 27(1.92%) | 1.43 [0.79, 2.57] | 0.23 | 0% |
| PLDRH vs. ODRH | 8 | 1531 | 15 (2.6%) | 17 (1.7%) | 1.47 [0.72, 2.99] | 0.29 | 1% |
| LADRH vs. ODRH | 5 | 612 | 7 (4.0%) | 10 (2.3%) | 1.33 [0.47, 3.78] | 0.59 | 0% |
| PSM | 3 | 322 | 5(3.1%) | 3 (1.9%) | 1.59 [0.41, 6.20] | 0.50 | 0% |
| Biliary stricture | 6 | 1467 | 8 (1.5%) | 5 (0.5%) | 2.38 [0.81, 7.04] | 0.12 | 0% |
| PLDRH vs. ODRH | 5 | 1317 | 7 (1.5%) | 5 (0.5%) | 2.18 [0.69, 6.90] | 0.19 | 1% |
| LADRH vs. ODRH | 1 | 150 | 1 (1.6%) | 0 (0.0%) | 4.56 [0.18, 113.89] | 0.36 | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mu, C.; Chen, C.; Wan, J.; Chen, G.; Hu, J.; Wen, T. Minimally Invasive Donors Right Hepatectomy versus Open Donors Right Hepatectomy: A Meta-Analysis. J. Clin. Med. 2023, 12, 2904. https://doi.org/10.3390/jcm12082904
Mu C, Chen C, Wan J, Chen G, Hu J, Wen T. Minimally Invasive Donors Right Hepatectomy versus Open Donors Right Hepatectomy: A Meta-Analysis. Journal of Clinical Medicine. 2023; 12(8):2904. https://doi.org/10.3390/jcm12082904
Chicago/Turabian StyleMu, Chunyang, Chuwen Chen, Jianghong Wan, Guoxin Chen, Jing Hu, and Tianfu Wen. 2023. "Minimally Invasive Donors Right Hepatectomy versus Open Donors Right Hepatectomy: A Meta-Analysis" Journal of Clinical Medicine 12, no. 8: 2904. https://doi.org/10.3390/jcm12082904
APA StyleMu, C., Chen, C., Wan, J., Chen, G., Hu, J., & Wen, T. (2023). Minimally Invasive Donors Right Hepatectomy versus Open Donors Right Hepatectomy: A Meta-Analysis. Journal of Clinical Medicine, 12(8), 2904. https://doi.org/10.3390/jcm12082904