
Effects of Probiotics on Intermediate Cardiovascular Outcomes in Patients with Overweight or Obesity: A Systematic Review and Meta-Analysis


 and
and 
Abstract
1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
2.2. Search Methods
2.3. Outcomes
2.4. Selection and Data Collection of Studies
2.5. Data Extraction and Management
2.6. Assessment of Risk of Bias in Included Studies
2.7. Data Synthesis Methods
3. Results
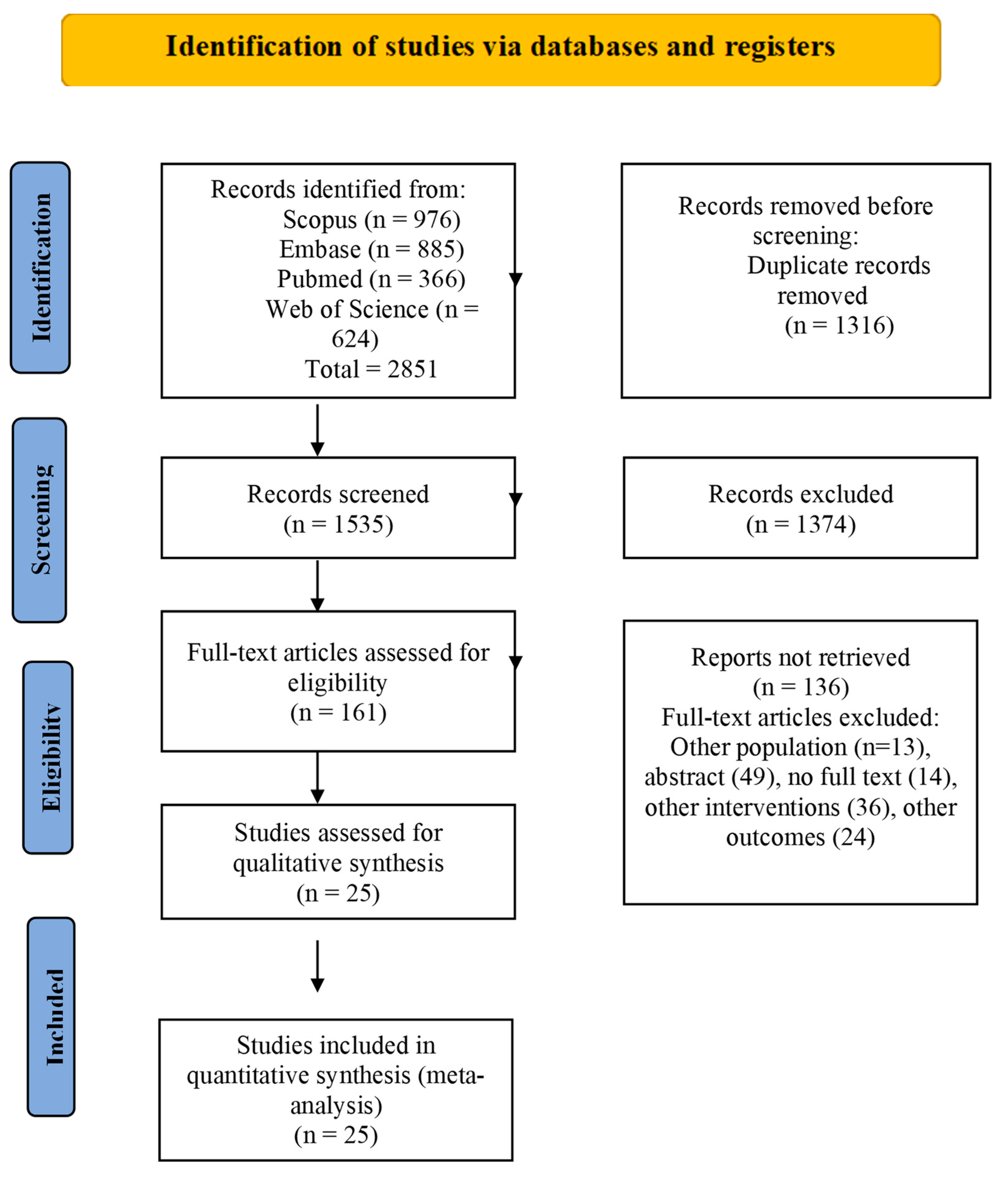
3.1. Selection of Studies
3.2. Characteristics of Included Trials
3.2.1. Risk of Bias and Quality of Evidence
3.2.2. Effect of Probiotics on Weight and Body Mass Index
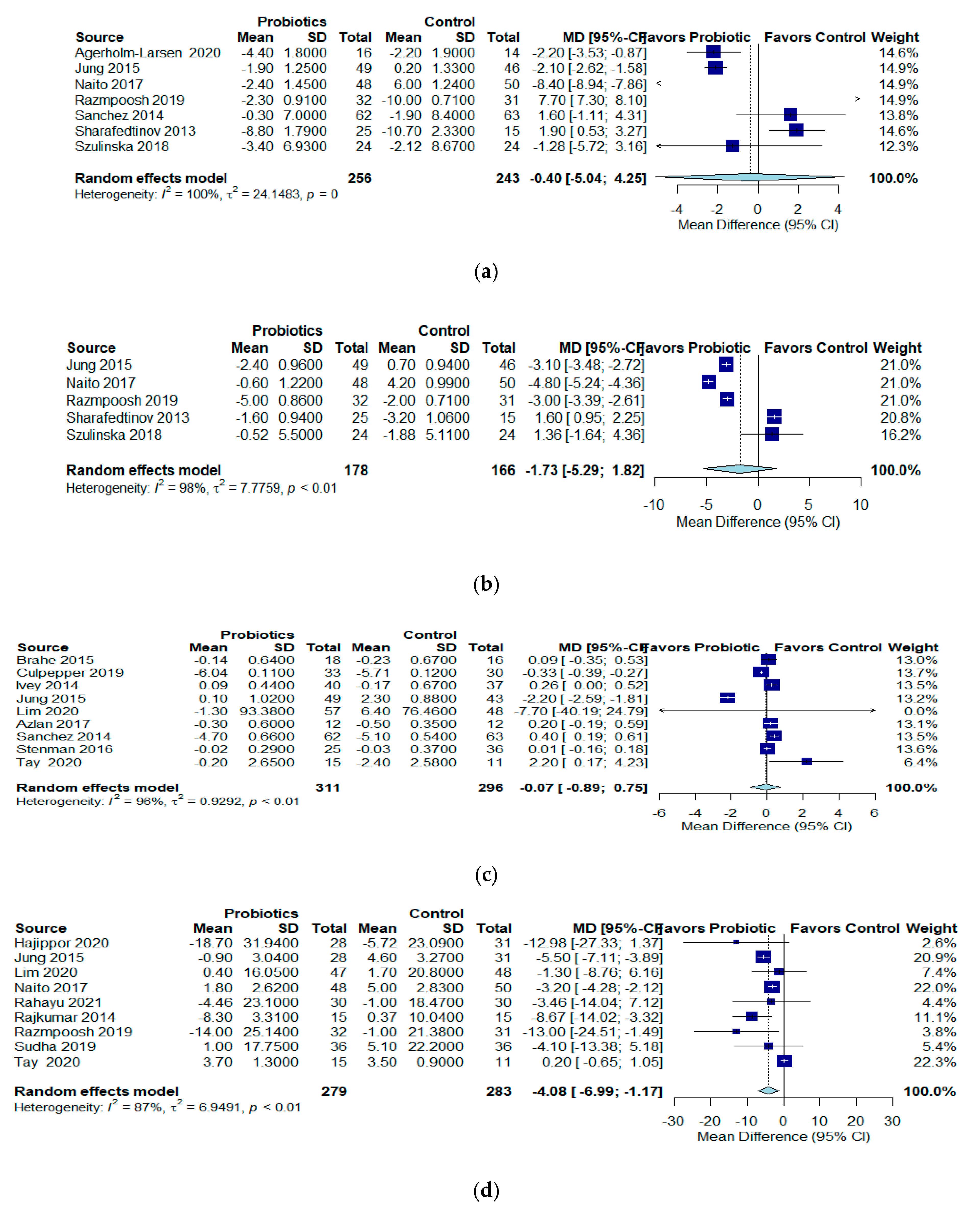
3.2.3. Effect of Probiotics on Blood Pressure
3.2.4. Effect of Probiotics on Glucose
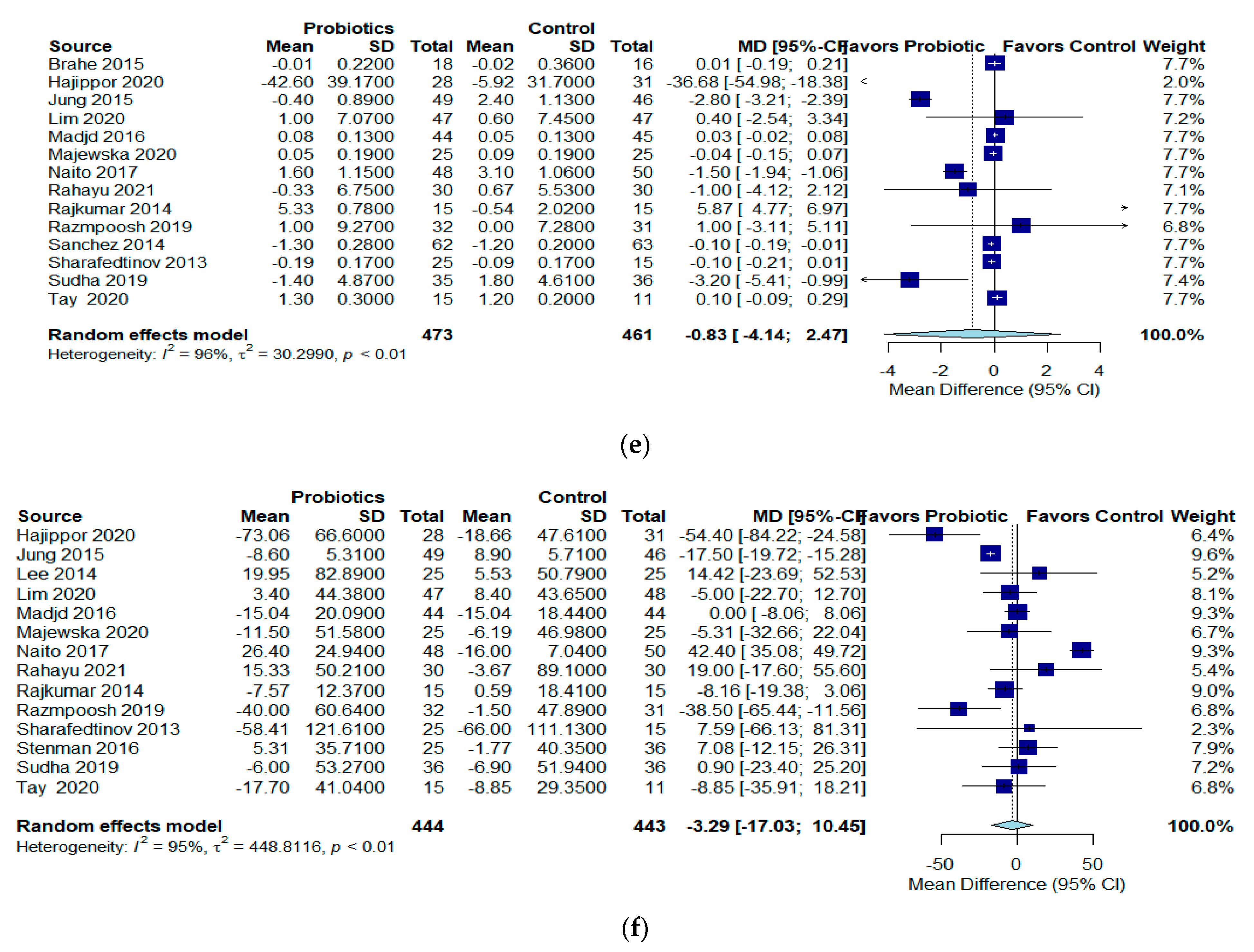
3.2.5. Effects of Probiotics on Lipids
3.3. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Marco, M.L.; Pavan, S.; Kleerebezem, M. Towards understanding molecular modes of probiotic action. Curr. Opin. Biotechnol. 2006, 17, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, A.S.; Larsen, N.; Pedersen-Skovsgaard, T.; Berg, R.M.; Møller, K.; Svendsen, K.D.; Jakobsen, M.; Pedersen, B.K. Effects of Lactobacillus acidophilus NCFM on insulin sensitivity and the systemic inflammatory response in human subjects. Br. J. Nutr. 2010, 104, 1831–1838. [Google Scholar] [CrossRef]
- Madsen, K.; Cornish, A.; Soper, P.; McKaigney, C.; Jijon, H.; Yachimec, C.; Doyle, J.; Jewell, L.; De Simone, C. Probiotic bacteria enhance murine and human intestinal epithelial barrier function. Gastroenterology 2001, 121, 580–591. [Google Scholar] [CrossRef]
- Cani, P.D.; Neyrinck, A.M.; Fava, F.; Knauf, C.; Burcelin, R.G.; Tuohy, K.M.; Gibson, G.R.; Delzenne, N.M. Selective increases of bifidobacteria in gut microflora improve high-fat-diet-induced diabetes in mice through a mechanism associated with endotoxaemia. Diabetologia 2007, 50, 2374–2383. [Google Scholar] [CrossRef]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef]
- Santacruz, A.; Collado, M.C.; García-Valdés, L.; Segura, M.T.; Martín-Lagos, J.A.; Anjos, T.; Martí-Romero, M.; Lopez, R.M.; Florido, J.; Campoy, C.; et al. Gut microbiota composition is associated with body weight, weight gain and biochemical parameters in pregnant women. Br. J. Nutr. 2010, 104, 83–92. [Google Scholar] [CrossRef]
- Million, M.; Lagier, J.C.; Yahav, D.; Paul, M. Gut bacterial microbiota and obesity. Clin. Microbiol. Infect. 2013, 19, 305–313. [Google Scholar] [CrossRef]
- Sanz, Y.; Santacruz, A.; Dalmau, J. Influencia del microbiota intestinal em la obesidad y las alteraciones del metabolismo. Acta Pediatr. Esp. 2009, 67, 437–442. [Google Scholar]
- Bernini, L.J.; Simão, A.N.; Alfieri, D.F.; Lozovoy, M.A.; Mari, N.L.; de Souza, C.H.; Dichi, I.; Costa, G.N. Beneficial effects of Bifidobacterium lactis on lipid profile and cytokines in patients with metabolic syndrome: A randomized trial. Effects of probiotics on metabolic syndrome. Nutrition 2016, 32, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.; Langan, D.; Salanti, G. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res. Synth. Methods 2016, 7, 55–79. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef]
- Balsbem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Ytter, Y.F.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Agerholm-Larsen, L.; Raben, A.; Haulrik, N.; Hansen, A.S.; Manders, M.; Astrup, A. Effect of 8 week intake of probiotic milk products on risk factors for cardiovascular diseases. Eur. J. Clin. Nutr. 2000, 54, 288–297. [Google Scholar] [CrossRef]
- Banach, K.; Glibowski, P.; Jedut, P. The Effect of Probiotic Yogurt Containing Lactobacillus Acidophilus LA-5 and Bifidobacterium Lactis BB-12 on Selected Anthropometric Parameters in Obese Individuals on an Energy-Restricted Diet: A Randomized, Controlled Trial. Appl. Sci. 2020, 10, 5830. [Google Scholar] [CrossRef]
- Brahe, L.K.; Le Chatelier, E.; Prifti, E.; Pons, N.; Kennedy, S.; Blædel, T.; Håkansson, J.; Dalsgaard, T.K.; Hansen, T.; Pedersen, O.; et al. Dietary modulation of the gut microbiota—A randomised controlled trial in obese postmenopausal women. Br. J. Nutr. 2015, 114, 406–417. [Google Scholar] [CrossRef]
- Culpepper, T.; Rowe, C.C.; Rusch, C.T.; Burns, A.M.; Federico, A.P.; Girard, S.A.; Tompkins, T.A.; Nieves, C., Jr.; Dennis-Wall, J.C.; Christman, M.C.; et al. Three probiotic strains exert different effects on plasma bile acid profiles in healthy obese adults: Randomised, double-blind placebo-controlled crossover study. Benef. Microbes 2019, 10, 497–509. [Google Scholar] [CrossRef]
- Hajipoor, S.; Hekmatdoost, A.; Rezaei, M.; Nachvak, S.M.; Alipour, M.; Eskandari, S.; Mostafai, R.; Sobhiyeh, M.R.; Mohammadi, R.; Pasdar, Y. The effect of yogurt co-fortified with probiotic and vitamin D on lipid profile, anthropometric indices and serum 25-hydroxi vitamin D in obese adult: A Double-Blind Randomized-Controlled Trial. Food Sci. Nutr. 2020, 9, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Ivey, K.L.; Hodgson, J.M.; Kerr, D.A.; Lewis, J.R.; Thompson, P.L.; Prince, R.L. The effects of probiotic bacteria on glycaemic control in overweight men and women: A randomised controlled trial. Eur. J. Clin. Nutr. 2014, 68, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Lee, Y.J.; Kim, M.; Kim, M.; Kwak, J.H.; Lee, J.-W.; Ahn, Y.-T.; Sim, J.-H.; Lee, J.H. Supplementation with two probiotic strains, Lactobacillus curvatus HY7601 and Lactobacillus plantarum KY1032, reduced body adiposity and Lp-PLA2 activity in overweight subjects. J. Funct. Foods 2015, 19, 744–752. [Google Scholar] [CrossRef]
- Kim, M.; Kim, M.; Kang, M.; Yoo, H.J.; Kim, M.S.; Ahn, Y.T.; Sim, J.H.; Jee, S.H.; Lee, J.H. Effects of weight loss using supplementation with Lactobacillus strains on body fat and medium-chain acylcarnitines in overweight individuals. Food Funct. 2017, 8, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Bose, S.; Seo, J.G.; Chung, W.S.; Lim, C.Y.; Kim, H. The effects of co-administration of probiotics with herbal medicine on obesity, metabolic endotoxemia and dysbiosis: A randomized double-blind controlled clinical trial. Clin. Nutr. 2014, 33, 973–981. [Google Scholar] [CrossRef]
- Lim, S.; Moon, J.H.; Shin, C.M.; Jeong, D.; Kim, B. Effect of Lactobacillus sakei, a Probiotic Derived from Kimchi, on Body Fat in Koreans with Obesity: A Randomized Controlled Study. Endocrinol. Metab. 2020, 35, 425–434. [Google Scholar] [CrossRef]
- Madjd, A.; Taylor, M.A.; Mousavi, N.; Delavari, A.; Malekzadeh, R.; Macdonald, I.A.; Farshchi, H.R. Comparison of the effect of daily consumption of probiotic compared with low-fat conventional yogurt on weight loss in healthy obese women following an energy-restricted diet: A randomized controlled trial. Am. J. Clin. Nutr. 2016, 103, 323–329. [Google Scholar] [CrossRef]
- Azlan, D.; Shyam, S.; Barua, A.; Krishnappa, P.; Ramamurthy, S. Effect of Probiotic Microbial Cell Preparation (MCP) on Fasting Blood Glucose, Body Weight, Waist Circumference, and Faecal Short Chain Fatty Acids among Overweight Malaysian Adults: A Pilot Randomised Controlled Trial of 4 Weeks. Mal. J. Nutr. 2017, 23, 329–341. [Google Scholar]
- Majewska, K.; Kręgielska-Narożna, M.; Jakubowski, H.; Szulińska, M.; Bogdański, P. The Multispecies Probiotic Effectively Reduces Homocysteine Concentration in Obese Women: A Randomized Double-Blind Placebo-Controlled Study. J. Clin. Med. 2020, 9, 998. [Google Scholar] [CrossRef]
- Naito, E.; Yoshida, Y.; Kunihiro, S.; Makino, K.; Kasahara, K.; Kounoshi, Y.; Aida, M.; Hoshi, R.; Watanabe, O.; Igarashi, T.; et al. Effect of Lactobacillus casei strain Shirota-fermented milk on metabolic abnormalities in obese prediabetic Japanese men: A randomised, double-blind, placebo-controlled trial. Biosci. Microbiota Food Health 2018, 37, 9–18. [Google Scholar] [CrossRef]
- Narmaki, E.; Borazjani, M.; Ataie-Jafari, A.; Hariri, N.; Doost, A.H.; Qorbani, M.; Saidpour, A. The combined effects of probiotics and restricted calorie diet on the anthropometric indices, eating behavior, and hormone levels of obese women with food addiction: A randomized clinical trial. Nutr. Neurosci. 2022, 25, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Rahayu, E.S.; Mariyatun, M.; Manurung, N.E.P.; Hasan, P.N.; Therdtatha, P.; Mishima, R.; Komalasari, H.; Mahfuzah, N.A.; Pamungkaningtyas, F.H.; Yoga, W.K.; et al. Effect of probiotic Lactobacillus plantarum Dad-13 powder consumption on the gut microbiota and intestinal health of overweight adults. World J. Gastroenterol. 2021, 27, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, H.; Mahmood, N.; Kumar, M.; Varikuti, S.R.; Challa, H.R.; Myakala, S.P. Effect of probiotic (VSL#3) and omega-3 on lipid profile, insulin sensitivity, inflammatory markers, and gut colonization in overweight adults: A randomized, controlled trial. Mediat. Inflamm. 2014, 2014, 348959. [Google Scholar]
- Razmpoosh, E.; Zare, S.; Fallahzadeh, H.; Safi, S.; Nadjarzadeh, A. Effect of a low energy diet, containing a high protein, probiotic condensed yogurt, on biochemical and anthropometric measurements among women with overweight/obesity: A randomised controlled trial. Clin. Nutr. 2020, 35, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, M.; Darimont, C.; Panahi, S.; Drapeau, V.; Marette, A.; Taylor, V.H.; Doré, J.; Tremblay, A. Effects of a Diet-Based Weight-Reducing Program with Probiotic Supplementation on Satiety Efficiency, Eating Behaviour Traits, and Psychosocial Behaviours in Obese Individuals. Nutrients 2017, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Sharafedtinov, K.K.; Plotnikova, O.A.; Alexeeva, R.I.; Sentsova, T.B.; Songisepp, E.; Stsepetova, J.; Smidt, I.; Mikelsaar, M. Hypocaloric diet supplemented with probiotic cheese improves body mass index and blood pressure indices of obese hypertensive patients--a randomized double-blind placebo-controlled pilot study. Nutr. J. 2013, 12, 138. [Google Scholar] [CrossRef]
- Stenman, L.K.; Lehtinen, M.J.; Meland, N.; Christensen, J.E.; Yeung, N.; Saarinen, M.T.; Courtney, M.; Burcelin, R.; Lähdeaho, M.L.; Linros, J.; et al. Probiotic With or Without Fiber Controls Body Fat Mass, Associated With Serum Zonulin, in Overweight and Obese Adults-Randomized Controlled Trial. EBioMedicine 2016, 13, 190–200. [Google Scholar] [CrossRef]
- Sudha, M.R.; Ahire, J.J.; Jayanthi, N.; Tripathi, A.; Nanal, S. Effect of multi-strain probiotic (UB0316) in weight management in overweight/obese adults: A 12-week double blind, randomised, placebo-controlled study. Benef. Microbes 2019, 10, 855–866. [Google Scholar] [CrossRef]
- Szulińska, M.; Łoniewski, I.; Skrypnik, K.; Sobieska, M.; Korybalska, K.; Suliburska, J.; Bogdański, P. Multispecies Probiotic Supplementation Favorably Affects Vascular Function and Reduces Arterial Stiffness in Obese Postmenopausal Women-A 12-Week Placebo-Controlled and Randomized Clinical Study. Nutrients 2018, 10, 1672. [Google Scholar] [CrossRef]
- Tay, A.; Pringle, H.; Penning, E.; Plank, L.D.; Murphy, R. PROFAST: A Randomized Trial Assessing the Effects of Intermittent Fasting and Lacticaseibacillus rhamnosus Probiotic among People with Prediabetes. Nutrients 2020, 12, 3530. [Google Scholar] [CrossRef]
- Zarrati, M.; Raji Lahiji, M.; Salehi, E.; Yazdani, B.; Razmpoosh, E.; Shokouhi Shoormasti, R.; Shidfar, F. Effects of Probiotic Yogurt on Serum Omentin-1, Adropin, and Nesfatin-1 Concentrations in Overweight and Obese Participants Under Low-Calorie Diet. Probiotics Antimicrob. Proteins 2019, 11, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- van Dis, I.; Kromhout, D.; Geleijnse, J.M.; Boer, J.M.; Verschuren, W.M. Body mass index and waist circumference predict both 10-year nonfatal and fatal cardiovascular disease risk: Study conducted in 20,000 Dutch men and women aged 20–65 years. Eur. J. Cardiovasc. Prev. Cardiol. 2009, 16, 729–734. [Google Scholar]
- Jung, S.P.; Lee, K.M.; Kang, J.H.; Yun, S.I.; Park, H.O.; Moon, Y.; Kim, J.Y. Effect of Lactobacillus gasseri BNR17 on Overweight and Obese Adults: A Randomized, Double-Blind Clinical Trial. Korean J. Fam. Med. 2013, 34, 80–89. [Google Scholar] [CrossRef]
- Ghibaudi, L.; Cook, J.; Farley, C.; van Heek, M.; Hwa, J.J. Fat intake affects adiposity, comorbidity factors, and energy metabolism of sprague-dawley rats. Obes. Res. 2002, 10, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.H.; Lobley, G.E.; Holtrop, G.; Ince, J.; Johnstone, A.M.; Louis, P.; Flint, H.J. Human colonic microbiota associated with diet, obesity and weight loss. Int. J. Obes. 2008, 32, 1720–1724. [Google Scholar] [CrossRef]
- Kovatcheva-Datchary, P.; Arora, T. Nutrition, the gut microbiome and the metabolic syndrome. Best Pract. Res. Clin. Gastroenterol. 2013, 27, 59–72. [Google Scholar] [CrossRef]
- Grembi, J.A.; Nguyen, L.H.; Haggerty, T.D.; Gardner, C.D.; Holmes, S.P.; Parsonnet, J. Gut microbiota plasticity is correlated with sustained weight loss on a low-carb or low-fat dietary intervention. Sci. Rep. 2020, 10, 1405. [Google Scholar] [CrossRef]
- Jones, M.L.; Martoni, C.J.; Parent, M.; Prakash, S. Cholesterol-lowering efficacy of a microencapsulated bile salt hydrolase-active Lactobacillus reuteri NCIMB 30242 yoghurt formulation in hypercholesterolaemic adults. Br. J. Nutr. 2012, 107, 1505–1513. [Google Scholar] [CrossRef]
- Kumar, M.; Rakesh, S.; Nagpal, R.; Hemalatha, R.; Ramakrishna, A.; Sudarshan, V.; Ramagoni, R.; Shujauddin, M.; Verma, V.; Kumar, A.; et al. Probiotic Lactobacillus rhamnosus GG and Aloe vera gel improve lipid profiles in hypercholesterolemic rats. Nutrition 2013, 29, 574–579. [Google Scholar] [CrossRef]
- Park, S.; Bae, J.H. Probiotics for weight loss: A systematic review and meta-analysis. Nutr. Res. 2015, 35, 566–575. [Google Scholar] [CrossRef]
- Borgeraas, H.; Johnson, L.K.; Skattebu, J.; Hertel, J.K.; Hjelmesaeth, J. Effects of probiotics on body weight, body mass index, fat mass and fat percentage in subjects with overweight or obesity: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2018, 19, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Nikbakht, E.; Khalesi, S.; Singh, I.; Williams, L.T.; West, N.P.; Colson, N. Effect of probiotics and synbiotics on blood glucose: A systematic review and meta-analysis of controlled trials. Eur. J. Nutr. 2018, 57, 95–106. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Sample Size | Population | Age | Intervention | Control | Outcomes | Follow-Up (Month) |
|---|---|---|---|---|---|---|---|---|
| Agerholm-Larsen et al., 2020 [18] | Denmark | 70 | Overweight 10% and Obese 90% | 38.6 ± 2.1 | Enterococcus faecium (human species) and two strains of Streptococcus thermophilus. The subjects attended the department 3 days a week (mornings or afternoons) to consume 300 mL yogurt or one placebo tablet and to collect products for consumption at home. | The placebo milk product was of identical composition as the other milk products, but chemically fermented with an organic acid (delta-acid-lactone) instead of a living bacterial culture. | SBP | 2 |
| Banach et al., 2020 [19] | Poland | 54 | Obese | 34.8 ± 9.2 | Lactobacillus acidophilus LA-5 and Bifidobacterium lactis BB-12 strains | Hypocaloric diet without deliberates | BMI | 3 |
| Brahe et al., 2015 [20] | Denmark | 58 | Obese | 61.4 ± 6.5 | L. paracasei F19 | Maltodextrin | Glucose, HDL | 1.5 |
| Culpepper et al., 2019 [21] | USA | 103 | Obese | 51.2 ± 1.4 | Bacillus subtilis R0179, Lactobacillus plantarum HA-119, Bifidobacterium animalis subsp. lactis B94 | Placebo (potato starch) | Glucose | 4.5 |
| Hajippor et al., 2020 [22] | Iran | 140 | Obese | 40.9 ± 6.7 | Lactobacillus Acidophilus La-B5 and Bifidobacterium lactis Bb-12 (at levels of colony-forming 4 × 107) | Vitamin D | Cholesterol, HDL, LDL, Triglycerides. | 2.5 |
| Ivey et al., 2014 [23] | New Zeland | 156 | Overweight | 68.4 ± 7.8 | Lactobacillus acidophilus La5 and Bifidobacterium animalis subsp lactis Bb12 | Control milk (prepared by Harvey Fresh, Harvey, WA, Australia) | Glucose | 1.5 |
| Jung et al., 2015 [24] | Korea | 95 | Overwight | 40.1 ± 1.4 | L. curvatus HY7601 and L. plantarum KY1032 | The same amountof powder that did not contain any probiotics. | BMI, glucose, SBP, DBP, cholesterol, LDL, HDL and triglycerides | 3 |
| Kim et al., 2017 [25] | Korea | 60 | Obese | 37.9 | Lactobacillus curvatus (L. curvatus) HY7601 and Lactobacillus plantarum (L. plantarum) KY1032 | Placebo | BMI, weight | 3 |
| Lee et al., 2014 [26] | Korea | 50 | Obese | Streptococcus thermophiles (KCTC 11870BP), Lactobacillus plantarum (KCTC 10782BP), Lactobacillus acidophilus (KCTC 11906BP), Lactobacillus rhamnosus (KCTC 12202BP), Bifidobacterium lactis (KCTC 11904BP), Bifidobacterium longum (KCTC 12200BP), and Bifidobacterium breve (KCTC 12201BP). | Placebo | BMI, weight, cholesterol, triglycerides | 2 | |
| Lim et al., 2020 [27] | Korea | 95 | Obese | 46.4 ± 12.2 | L. sakei CJLS03 | Placebo | BMI, weight, glucose, cholesterol, HDL, LDL, triglycerides | 3 |
| Madjd et al., 2016 [28] | Iran | 89 | Obese | 32.2 ± 6.9 | Lactobacillus acidophilus LA5) and bifidobacteria (Bifidobacterium lactis BB12) | Simple yogurt | BMI, weight, HDL, triglycerides | 3 |
| Azlan et al., 2017 [29] | Malaysia | 24 | Overweight | 28.0 ± 8.3 | Lactobacillus acidophilus, Lactobacillus lactis, Lactobacillus casei, Bifi dobacterium longum, Bifi dobacterium bifi dum, and Bifi dobacterium infantis | Hexbio® B-Crobes Laboratory Sdn Bhd. Ipoh, Malaysia provided the MCP supplement and placebo samples. | Weight, glucose, | 1 |
| Majewska et al., 2020 [30] | Poland | 50 | Obese | 55.2 ± 6.9 | Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Bifidobacterium lactis W52, Lactobacillus acidophilus W37, Lactobacillus brevis W63, Lactobacillus casei W56, Lactobacillus salivarius W24, Lactococcus lactis W19, and Lactococcus lactis W58 | Placebo | HDL, triglycerides | 3 |
| Naito et al., 2017 [31] | Japan | 248 | Obese | 46.6 ± 1.1 | Lactobacillus casei strain Shirota (LcS) | Placebo milk | BMI, weight, SBP, DBP, cholesterol, LDL, HDL, triglycerides | 3 |
| Narmaki et al., 2020 [32] | Iran | 62 | Obese | 35.2 ± 5.7 | Lactobacillus acidophilus (1.8 × 109 CFU/capsule), Bifidobacterium bifidum (1.8 × 109 CFU/capsule), Bifidobacterium lactis (1.8 × 109 CFU/capsule), Bifidobacterium longum (1.8 × 109 FU/capsule), Lactobacillus rhamnosus (1 × 109 CFU/capsule), Lactobacillus reuteri (1 × 109 CFU/capsule) | Magnesium stearate, and maltodextrin | BMI, weight | 3 |
| Rahayu et al., 2021 [33] | Indonesia | 60 | Overweight | 44.0 ± 6.2 | Lactobacillus plantarum Dad-13 | Skim milk obtained from a local supermarket was used in the placebo group. | BMI, weight, cholesterol, HDL, LDL, triglycerides | 3 |
| Rajkumar et al., 2014 [34] | India | 60 | Overweight | 49(40–60) | Bifidobacteria (Bifidobacterium longum, Bifidobacterium infantis, and Bifidobacterium breve), four strains of lactobacilli (Lactobacillus acidophilus, Lactobacillus paracasei, Lactobacillus delbrueckii subsp. bulgaricus, and Lactobacillus plantarum), and one strain of Streptococcus salivarius subsp. thermophilus. | Omega 3 | Cholesterol, HDL, LDL, triglycerides | 1.5 |
| Razmpoosh et al., 2019 [35] | Iran | 70 | Overweight | 35.0 ± 10.0 | L. acidophilus La5 and 1.79 106 CFU/g of B. lactis Bb12 | Low energy diet | BMI, weight, SBP, DBP, cholesterol, HDL, LDL, triglycerides | 2 |
| Sanchez et al., 2014 [36] | Canada | 153 | Obese | 37.0 ± 10.0 | Lactobacillus rhamnosus CGMCC1.3724 | Oligofructose and inulin | BMI, weight, glusoce, SBP, HDL | 6 |
| Sharafedtinov et al., 2013 [37] | Russia | 40 | Obese | L. plantarum TENSIA | Cheese | BMI, weight, SBP, DBP, HDL, triglycerides | 1 | |
| Stenman et al., 2016 [38] | Finland | 172 | Obese | 48.8 ± 10.5 | Bifidobacterium animalis ssp. Lactis | Microcrystalline cellulose | BMI, weight, glucose, triglycerides | 6 |
| Sudha et al., 2019 [39] | India | 92 | Overweight | 43.5 | Lactobacillus salivarius UBLS-22, Lactobacillus casei UBLC-42, Lactobacillus plantarum, UBLP-40, Lactobacillus acidophilus UBLA-34, Bifidobacterium breve UBBr-01, and Bacillus coagulans | Maltodextrin | BMI, weight, cholesterol, LDL, HDL, triglycerides | 3 |
| Szulinska et al., 2018 [40] | 110 | Obese | 55.1 ± 6.8 | Bifidobacterium bifidum W23, Bifidobacterium lactis W51, Bifidobacterium lactis W52, Lactobacillus acidophilus W37, Lactobacillus brevis W63, Lactobacillus casei W56, Lactobacillus salivarius W24, Lactococcus lactis W19, and Lactococcus lactis W58 | Maize starch and maltodextrins | BMI, SBP, DBP | 3 | |
| Tay et al., 2020 [41] | New Zeland | 59 | Obese | 52.9 ± 8.7 | Lacticaseibacillus rhamnosus | Microcrystalline cellulose and dextrose anhydrate | BMI, weight, glucose, cholesterol, LDL, HDL, triglycerides | 3 |
| Zarrati et al., 2018 [42] | Iran | 60 | Obese | 36 ± 8.4 | Lactobacillus acidophilus La5, Bifidobacterium BB12, and Lactobacillus casei | Conventional yogurts | BMI, weight | 2 |
| Outcomes | Anticipated Absolute Effects * (95% CI) | No of Participants (Studies) | Certainty of the Evidence (Grade) | |
|---|---|---|---|---|
| Risk with Control | Risk with Probiotics | |||
| Body mass index follow-up: range 2 months to 6 months | The mean body mass index was 0.73 kg/m2. | MD 0.27 kg/m2 lower (0.35 lower to 0.19 lower) | 1169 (17 RCTs) | ⨁⨁⨁◯ Moderate a |
| Weight follow-up: range 2 months to 6 months | The mean weight was −1.07 Kg. | MD 0.61 Kg lower (0.89 lower to 0.34 lower) | 998 (15 RCTs) | ⨁⨁⨁◯ Moderate b |
| Systolic blood pressure follow-up: range 2 months to 6 months | The mean systolic blood pressure was −2.96 mmHg. | MD 0.4 mmHg lower (5.04 lower to 4.25 higher) | 499 (7 RCTs) | ⨁◯◯◯ Very low c,d,e |
| Diastolic blood pressure follow-up: range 2 months to 6 months | The mean diastolic blood pressure was −0.43 mmHg. | MD 1.73 mmHg lower (5.29 lower to 1.82 higher) | 344 (5 RCTs) | ⨁◯◯◯ Very Low f,g,h |
| Glucose follow-up: range 2 to 6 months | The mean glucose was −0.60 mg/dL. | MD 0.07 mg/dL lower (0.89 lower to 0.75 higher) | 607 (9 RCTs) | ⨁◯◯◯ Very Low i,j,k |
| Low-density lipoprotein follow-up: range 2 months to 6 months | The mean low-density lipoprotein was 1.39 mg/dL. | MD 4.08 mg/dL lower (6.99 lower to 1.17 lower) | 562 (9 RCTs) | ⨁⨁◯◯ Low l,m |
| High-density lipoprotein follow-up: range 2 months to 6 months | The mean high-density lipoprotein was 0.15 mg/dL. | MD 0.83 mg/dL lower (4.14 lower to 2.47 higher) | 934 (14 RCTs) | ⨁◯◯◯ Very low n,o,p |
| Triglycerides follow-up: range 2 months to 6 months | The mean triglycerides was −8.65 mg/dL. | MD 3.29 mg/dL lower (17.03 lower to 10.45 higher) | 887 (14 RCTs) | ⨁◯◯◯ Very low q,r,s |
| * The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). The crosses are symbols marked according to GRADE methodology. CI: confidence interval; MD: mean difference | ||||
| GRADE working group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of the effect. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayta-Tovalino, F.; Diaz-Arocutipa, C.; Piscoya, A.; Hernandez, A.V. Effects of Probiotics on Intermediate Cardiovascular Outcomes in Patients with Overweight or Obesity: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2554. https://doi.org/10.3390/jcm12072554
Mayta-Tovalino F, Diaz-Arocutipa C, Piscoya A, Hernandez AV. Effects of Probiotics on Intermediate Cardiovascular Outcomes in Patients with Overweight or Obesity: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(7):2554. https://doi.org/10.3390/jcm12072554
Chicago/Turabian StyleMayta-Tovalino, Frank, Carlos Diaz-Arocutipa, Alejandro Piscoya, and Adrian V. Hernandez. 2023. "Effects of Probiotics on Intermediate Cardiovascular Outcomes in Patients with Overweight or Obesity: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 7: 2554. https://doi.org/10.3390/jcm12072554
APA StyleMayta-Tovalino, F., Diaz-Arocutipa, C., Piscoya, A., & Hernandez, A. V. (2023). Effects of Probiotics on Intermediate Cardiovascular Outcomes in Patients with Overweight or Obesity: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(7), 2554. https://doi.org/10.3390/jcm12072554