
Circus Activities as a Health Intervention for Children, Youth, and Adolescents: A Scoping Review
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
- What participant characteristics (skill, developmental stage, or biopsychosocial challenges) are being targeted by the circus interventions?
- What are the key elements of the circus interventions (activities being taught; frequency, length, total number of sessions, and settings utilised)?
- What health and well-being outcomes are reported in the literature investigating circus interventions?
- What are the gaps in the current literature and how do they, and the findings of this scoping review, inform the planning of further research?
2.1. Eligibility Criteria
2.2. Search Strategy & Study Selection
2.3. Data Extraction and Analysis
3. Results
3.1. Characteristics of Included Sources of Evidence
3.2. Characteristics of Participants Targeted by Circus Interventions
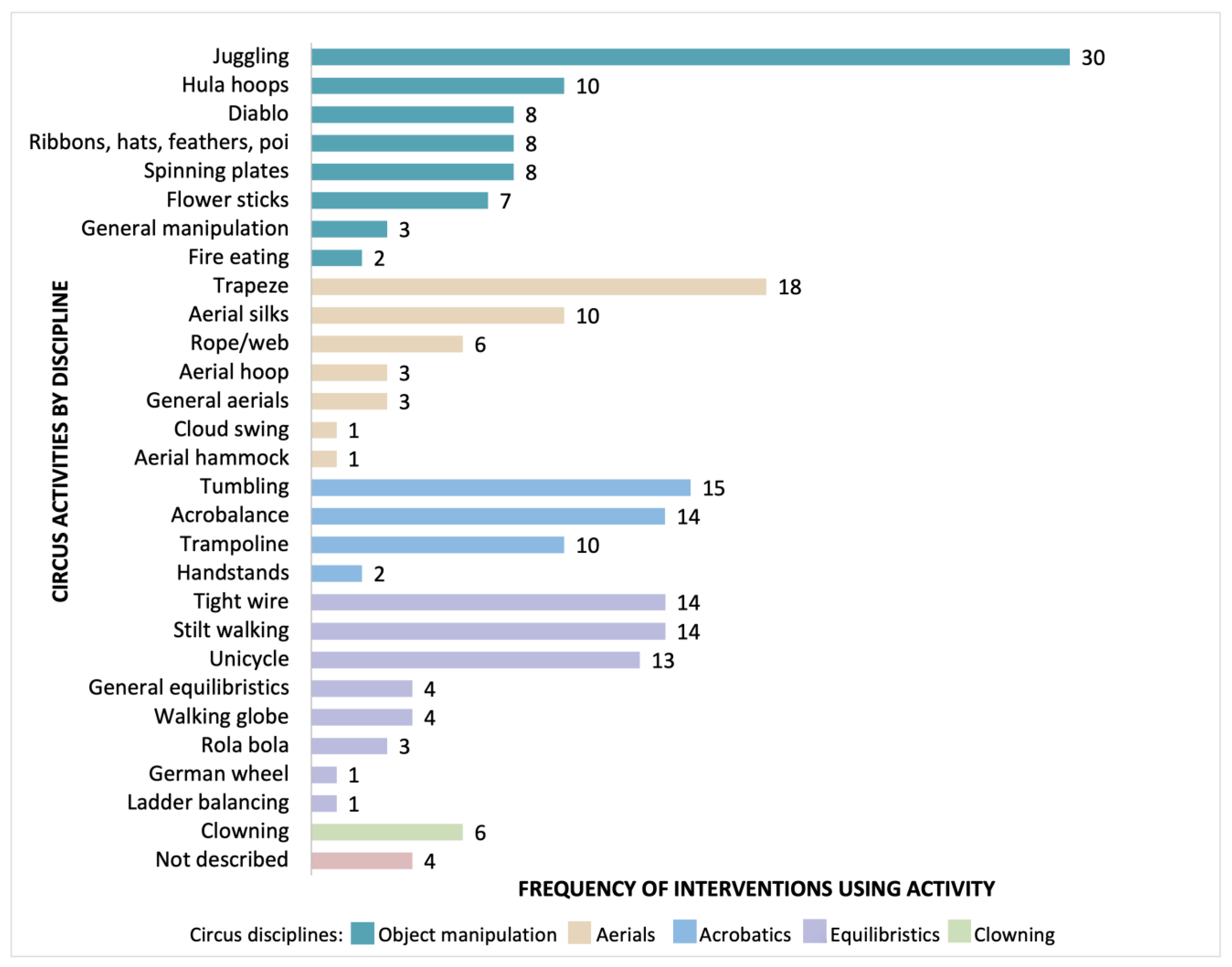
3.3. Key Elements of the Circus Interventions
3.4. Outcomes Relating to Health & Wellbeing
3.5. Physical Outcomes
3.6. Social-Emotional Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy Development

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population 1 | Concept 1 | Concept 2 | |
|---|---|---|---|
| As stated in research question | Children and youth | Circus activities | Health intervention |
| Alternate search terms for those concepts, using truncation * and wild cards # or? | paediatr*, preschool, kinder, kids, adolescent, infant, school-aged, young people | Social circus, community circus, recreational circus, youth circus, hula hoop, juggl*, acroba*, trapeze, tissu, silks | therap*, physiotherapy, occupational therapy, psychology*, program, exercise*, activit*, class, classes |
| Synonyms (alternate words) alternative spelling, language, etc. | Pre-school | Programmes, programme, programs | |
| Discarded after trialing in MEDLINE and CINAHL, with reasons | All population terms discarded due to scarcity of literature. | acroba*: no items returned relating to circus, many returned relating to gymnastics juggl*: first 50 citations screened related to “juggling work/life”, and none to circus trapeze: first 50 citations screened did not relate to circus tissu OR silks: first 50 citations screened did not relate to circus | |
| Indexed key words added after pilot search in MEDLINE and CINAHL | Nil | Nil | “social work” |
| Search | Query | Records Retrieved |
|---|---|---|
| #1 | circus OR hula hoop* OR hula-hoop* | 699 |
| #2 | therap* OR intervention* OR class OR classes OR program OR programme OR programs OR programmes OR activit* OR exercise OR exercises OR physiotherap* OR social work* OR psycholog* | 11,234,666 |
| #3 | #1 AND #2 | 276 |
| Limited to ‘human’ | 165 | |
Appendix B. Data Extraction Instrument
| Element for Extraction | Extracted Data |
|---|---|
| Citation: author/s, date | |
| Country of intervention delivery | |
| Literature type; Study design | |
| Sample size | |
| Participant details: (Aim 1) | |
| |
| |
| Intervention details (adapted from TIDieR checklist [3]): (Aim 2) | |
| |
| |
| |
| |
| |
| |
| Health/ wellbeing outcomes relating to circus intervention (Aim 3) |
Appendix C. Elements of the Circus Interventions
| Citations Grouped by Intervention | What (Circus Activities Only) | Where | When & How Much | For Whom |
|---|---|---|---|---|
| Agans et al., 2019 [17] | Tumbling, juggling, clowning, tight wire, trapeze | School, circus centre | Ongoing program, dosage not described | General population (circus school) |
| Barnett et al., 2020 [18]; Kiez, 2015 [36]; Kriellaars et al., 2019 [8]; Valentini et al., 2020 [74] | Juggling (balls, scarves), rola bola, stilt walking, unicycle, trampoline, flower sticks, trapeze, aerial rope, hula hoops, tight wire, German wheel, diabolo | School | One to three 50–60 min sessions per week for a school year | General population (primary school) |
| Biquet, 2014 [35] | Juggling, acrobalance (human pyramids), tumbling, general aerial skills, stilt walking | Circus centre | Once per week for 3 h in an ongoing program | “living in a warzone” |
| Bolton, 2004 [33] | Juggling, stilt walking, unicycle, acrobalance | School | 2 h per session for two weeks | General population (ex-pats & local community) |
| Bonk, 2019 [34] | Handstands, tumbling, juggling, unicycle, aerial silks, aerial hoop, and trapeze | Circus centre | One 1-h session | General population (circus school) |
| Boyd et al., 2010 [42]; Gilmore et al., 2010 [45]; Rodger & Kennedy-Behr, 2017 [32]; Sakzewski et al., 2012 [60]; Sakzewski, Provan, et al., 2015 [57]; Sakzewski, Ziviani, Abbott, et al., 2011a [54], 2011b [55], 2011c [61]; Sakzewski, Ziviani, & Boyd, 2011 [53]; Sakzewski, Ziviani & Poulsen, 2015 [16] | Ribbons, flower sticks, hula hoops, spinning plates, acrobalance, general aerials | Circus centre | Five 2-h sessions (in combination with 4 h of other tasks) for 2 weeks | Cerebral palsy: unilateral hemiplegia |
| Boyd et al., 2013 [41]; Miller et al., 2016 [48]; Sakzewski, Miller, et al., 2015 [56] | Ribbons, flower sticks, hula hoops, spinning plates, acrobalance, general aerials | Circus centre | Five 2-h sessions (within 4 h of other tasks) for 2 weeks | Cerebral palsy: unilateral hemiplegia |
| Cadwell & Rooney, 2013 [71] | Specific circus activities not described | Circus centre | Ongoing program, dosage not described | General population (circus school) |
| Caldwell, 1996 [75] | Juggling | School | Ongoing program, dosage not described | General population (circus school) |
| Candy, 2017 [20] | Juggling (scarves, balls, clubs, rings), balance feathers, spinning plates, diablo, unicycle, tightwire, hula hoops, rola bola, stilt walking, aerial silks, trapeze, rope | Circus centre | One or two 2.5 h sessions per week in an ongoing program | General population |
| Cohen, 2018 [43]; Smith et al., 2017 [70] | Specific circus activities not described | Not described | Between 30 and 489 contact hours depending on the program | General population (circus school) |
| Csuros, 2015 [44] | Juggling, tumbling and tightwire | Hospital | One session per week in an ongoing program | Children in psychiatric care: “conduct disorder, hyperactivity, attention deficit disorder (ADD), autism, spectrum disorders and psychiatric disorders requiring emergency care (crisis conditions, suicidal intensions or attempted suicide, self-destructive behaviour, sudden psychotic conditions), schizophrenia, mood disorders, anxiety disorders, post-traumatic disorder, emerging personality disorders, obsessive compulsive disorder, eating disorders, attachment disorders.” |
| Fernandez et al., 2018 [22] | Trapeze, aerial hoop, trampoline, tumbling | Circus centre | One 60 min session per week for 10 weeks | Children with developmental difficulties (without a specified medical condition or disability). |
| Fournier et al., 2014 [4] | Specific circus activities not described | Community centre (YWCA) | Two sessions per week for 3 months | Children in psychiatric care: mood disorders, anxiety disorders, relational or behavioural problems, attention deficit hyperactivity disorder (ADHD), psychotic disorders, eating disorders. |
| Heller & Taglialatela, 2018 [6] | Rola bola, hula hoops, aerial hammocks, trapeze, aerial web, aerial ring, tightwire | Circus centre | One 50–60 min session per week for 2 eight-week blocks | ADD, ADHD, anxiety, autism, behavioural challenges, impulse control challenges (sourced from personal communication with author). |
| Kinnunen et al., 2013 [69] | Hula hoops, aerial silks, trampoline, trapeze, unicycle, juggling, tight wire, acrobalance, diablo, handstands | School, rehabilitation centre, circus centre, retirement home, disability service centre | Varying dosages for different settings | Variety of populations, including “special needs” class (school); general population (school & pre-school); ADD/ ADHD, autism; children of families who use the child welfare services and are dealing with crises; children with visual impairment. |
| Kovalenko, 2018 [29] | Trampoline, juggling | Circus centre | Five 1.5–3-h sessions per week in an ongoing program | “at risk”: children from difficult family circumstances, adolescents who have committed an offence, children with disability. |
| Loiselle et al., 2019 [46] | Tumbling, trapeze, aerial silk, juggling, clowning, equilibristics | Circus centre | Two 2-h sessions per week for two 12-week blocks | Young people with physical disabilities including: cerebral palsy, leukodystrophy, Steiner’s syndrome, Childhood callosotomy sequelae for uncontrolled epilepsy, Friedrich’s ataxia, traumatic acquired brain injury (ABI), severe burns in infancy |
| Maglio & McKinstry, 2008 [9] | Tumbling, acrobalance, juggling, hula hoops, equilibristics | Circus centre, school | One 2-h session per week for 10–40 weeks | General population (school) |
| Mason, 2013 [72] | Juggling, tumbling | Circus centre, school, community centre | One session per day for 5 days | “living in a warzone” |
| McCaffery, 2011 [65] | Juggling, unicycle, stilt walking, flower sticks, poi, diabolo, spinning plates, hat manipulation | School | One 90–120 min session per week for 18 sessions | School students with moderate to severe learning difficulties |
| McCaffery, 2012 [64] | Juggling, unicycle, stilt walking, flower sticks, poi, diabolo, spinning plates, hat manipulation | Circus centre | One 90 min session per week for 18 sessions | Autism |
| McCaffery, 2014 [63] | Juggling, stilt walking, unicycle, general manipulation, general equilibristics | School | One 90 min session per week for 8 weeks | “at risk” school students: at-risk of disengagement, poor attendance or leaving school early. |
| McCutcheon, 2003 [37] | Unicycle, aerial silks, acrobalance, juggling, diabolo, stilt walking, tumbling, flower sticks, rola bola, clowning, ladder, trapeze, cloud swing, tightwire, trampoline | School | Varying dosages for different students | “at risk” school students |
| McGrath & Stevens, 2019 [47] | Stilt walking, trampoline, tumbling, trapeze, aerial silks | Circus centre | One 60 min session per week for 20 weeks | General population (circus school) |
| Momesso dos Santos et al., 2015 [49] | Tumbling, trampoline, stilt walking, trapeze | Circus centre | Two 60 min session per week for 38 sessions | Overweight |
| Neave et al., 2020 [50] | Acrobalance, aerial rope, unicycle, juggling | School | One 60 min session per week for 6 months | General population (school) |
| O’Donnell, n.d [66] | Stilt walking, tight wire, walking globe, tumbling, juggling, clowning, general manipulation | Schools, hospital | One 60 min session per week for ‘several weeks’ | “at-risk” due to socioeconomic status, single-parent homes, and/or a history of truancy and disruptive classroom behaviour at school; inpatient psychiatric unit. |
| Ott, 2005 [38] | Trapeze, tumbling, juggling, clowning, aerial web, tight wire, unicycle, fire-eating | Circus centre | Two 120 min session per week in an ongoing program | General population (circus school) |
| Pompe, 2021 [30] | Acrobalance, juggling, trampoline | Hospital | Ongoing program | Inpatient psychiatric unit |
| Rappaport, 2014 [73] | Acrobalance, juggling, tight wire, trapeze, aerial silks, clowning | School, hospital | (a) One 75 min session per week (b) Two 45 min sessions per week | Inpatient psychiatric unit: mood disorder, bipolar, depression; deaf, hard of hearing, or other communication difficulties. |
| Rivard et al., 2010 [51] | Acrobalance, juggling | Community centre | Once or twice per week in an ongoing program | Vulnerable young people in “difficult situations” |
| Sahli et al., 2013 [52] | Stilt walking, rola bola, walking globe, juggling and other manipulation, unicycle, hula hoops, tight wire | Circus centre | Two 2-h sessions per week in an ongoing program | General population (circus school) |
| Seay, 2004 [39] | Juggling, aerial silks, fire eating, trampoline, tumbling, trapeze | School | Two-week program | General population (school) |
| Seymour, 2012 [40] | Trapeze, juggling, tight wire, hula hoops, acrobalance | Circus centre, other various | Not described | Autism and other neurodiversities |
| Seymour & Wise, 2017 [58] | Trapeze, acrobalance, juggling, aerial silks | Circus centre, other various | Not described | Autism |
| Spiegel et al., 2015 [59] | Specific circus activities not described | Not described | Not described | Youth “living on the street” |
| Stevens et al., 2019 [14] | Stilt walking, trampoline, tumbling, trapeze, aerial silks | Circus centre | General population (circus school) | |
| Taylor & Taylor, 2004 [62] | Juggling (scarves, bean bags, balls), flower sticks, spinning plates, diabolo, poi, stilt walking, unicycle | School | Three 60 min sessions per week in an ongoing program | Range of intellectual and/or physical disabilities (mild to severe) |
| Trotman, 2013a [67] | Spinning plates, diabolo, tight wire, walking globe, hula hoops, tumbling, acrobalance | School | One 90 min session per week for 8 weeks | General population (school) |
| Trotman, 2013b [68] | Juggling, equilibristics | Circus centre | One 60 min session per week in an ongoing program | General population (circus school) |
| Van Es et al., 2021 [21] | Tumbling, trapeze, juggling, spinning plates, tight wire, walking globe | Community centre | Two 5-h session per week for 8 weeks | Refugee youth/ children and youth with traumatic war experiences. |
Appendix D. Sources of Evidence Included
| Citations | Type of Literature | Study Design | Sample Size | Age Range (Mean) |
|---|---|---|---|---|
| Agans et al., 2019 [17] | Peer-reviewed: journal article | Cross-sectional design | 111 | 10–21 y (15 y 9 m) |
| Barnett et al., 2020 [18] | Peer-reviewed: journal article | Concept paper | N/A | 9–12 y (10 y 0 m) |
| Biquet, 2014 [35] | Peer-reviewed: masters thesis | Case study | 15 | 11–20 y |
| Bolton, 2004 [33] | Peer-reviewed: PhD thesis | Not described | 30 | Kindergarten-Year 10 |
| Bonk, 2019 [34] | Peer-reviewed: masters thesis | Case study | 1 | 10 y |
| Boyd et al., 2010 [42] | Peer-reviewed: journal article | Randomised comparison trial protocol | N/A | N/A |
| Boyd et al., 2013 [41] | Peer-reviewed: journal article | Randomised comparison trial protocol | N/A | N/A |
| Cadwell & Rooney, 2013 [71] | Grey literature: conference proceedings | Not described | 33 | 5–20 y |
| Caldwell, 1996 [75] | Grey literature: newspaper article | N/A | Not described | 6–11 y |
| Candy, 2017 [20] | Peer-reviewed: masters thesis | N/A | 11 children 18 parents | “school-aged children” |
| Cohen, 2018 [43] | Peer-reviewed: journal article | Not described | Not described | “youth” |
| Csuros, 2015 [44] | Peer-reviewed: journal article | Not described | 10–15 | 4–18 y |
| Fernandez et al., 2018 [22] | Peer-reviewed: journal article | Qualitative | 20 | 5–10 y |
| Fournier et al., 2014 [4] | Peer-reviewed: journal article | Mixed-methods | 15 patients 9 non-patients | 14–24 y |
| Gilmore et al., 2010 [45] | Peer-reviewed: journal article | Qualitative | 32 | 9–11 y (10 y 1 m) |
| Heller & Taglialatela, 2018 [6] | Peer-reviewed: journal article | Pre-post survey design | 15 | 4–12 y (6 y 6 m) |
| Kiez, 2015 [36] | Peer-reviewed: masters thesis | Prospective, clustered, quasi-experimental design | 211 | 9–12 y (10 y 0 m) |
| Kinnunen et al., 2013 [69] | Grey literature: report | Mixed-methods | Not described | 2–3 y, “babies”, “primary and high-school aged children”, 7–13 y |
| Kriellaars et al., 2019 [8] | Peer-reviewed: journal article | Prospective, clustered, quasi-experimental design | 211 | 9–12 y (10 y 0 m) |
| Kovalenko, 2018 [29] | Peer-reviewed: bachelors thesis | Qualitative | 7 | “children & adolescents” |
| Loiselle et al., 2019 [46] | Peer-reviewed: journal article | Qualitative | 11 | 18–22 y (20 y 0 m) |
| Maglio & McKinstry, 2008 [9] | Peer-reviewed: journal article | Process evaluation | Not described | 6–18 y |
| Mason, 2013 [72] | Grey literature: conference proceedings | Not described | Authors have educated over 2000 children in circus arts | “children” |
| McCaffery, 2011 [65] | Grey literature: report | Mixed-methods | 20 | 3–19 y |
| McCaffery, 2012 [64] | Grey literature: report | Mixed-methods | 12 | “young people under 24 years” (personal communication) |
| McCaffery, 2014 [63] | Grey literature: report | Mixed-methods | 11 | “Year 10 students” |
| McCutcheon, 2003 [37] | Peer-reviewed: masters thesis | Case studies | Case 1: 60 Case 2: 300 Case 3: not described Case 4: various Case 5: 100 | “school-aged children” |
| McGrath & Stevens, 2019 [47] | Peer-reviewed: journal article | Mixed-methods | Surveys: 23 Focus group: 54 | 8–14 y (10 y 0 m) |
| Miller et al., 2016 [48] | Peer-reviewed: journal article | Exploratory study imbedded in larger prospective, clustered, quasi-experimental design | 26 | 5–16 y (8 y 2 m) |
| Momesso dos Santos et al., 2015 [49] | Peer-reviewed: journal article | Not described | 60 | 9–11 y (10 y 0 m) |
| Neave et al., 2020 [50] | Peer-reviewed: journal article | Between subjects repeated measures design | 89 | 9–12 y (10 y 0 m) |
| O’Donnell, n.d. [66] | Grey literature: report | Pre-post survey design | 125 | 5–17 y |
| Ott, 2005 [38] | Peer-reviewed: PhD thesis | Qualitative | 11 | 8–18 y (13 y 4 m) |
| Pompe, 2021 [30] | Peer-reviewed: bachelors thesis | Case study | Not described | 7–12 y, 13–18 y, 18–24 y |
| Rappaport, 2014 [73] | Grey literature: conference poster | Qualitative | Group 1: 6 Group 2: 68 | 12–17 y |
| Rivard et al., 2010 [51] | Peer-reviewed: journal article | Case study | Not described | 10–19 y |
| Rodger & Kennedy-Behr, 2017 [32] | Peer-reviewed: book | Review of the literature | Not described | ‘children’ |
| Sahli et al., 2013 [52] | Peer-reviewed: journal article | Not described | 24 | 5–6 y |
| Sakzewski, Ziviani, & Boyd, 2011 [53] | Peer-reviewed: journal article | Secondary analysis of single-blind matched-pairs randomized comparison trial | 61 | 5–16 y (10 y 2 m) |
| Sakzewski, Ziviani, Abbott, et al., 2011a [54] | Peer-reviewed: journal article | Single-blind matched-pairs randomized comparison trial | 62 | 5–16 y (10 y 2 m) |
| Sakzewski, Ziviani, Abbott, et al., 2011b [55] | Peer-reviewed: journal article | Single-blind matched-pairs randomized comparison trial | 62 | 5–16 y (10 y 2 m) |
| Sakzewski, Miller, et al., 2015 [56] | Peer-reviewed: journal article | Matched-pairs randomized comparison trial | 25 | 5–16 y (8 y) |
| Sakzewski, Provan, et al., 2015 [57] | Peer-reviewed: journal article | Secondary analysis of two single-blind matched-pairs randomized comparison trials | 82 | 5–16 y (Group 1: 10.2 y, Group 2: 8.7 y) |
| Sakzewski, Ziviani, et al., 2015 [16] | Peer-reviewed: book chapter | N/A | N/A | “Children” |
| Sakzewski et al., 2012 [60] | Peer-reviewed: journal article | Single-blind matched-pairs randomized comparison trial | 63 | 5–16 y (10 y 2 m) |
| Sakzewski, Ziviani, Abbott, et al., 2011c [61] | Peer-reviewed: journal article | Single-blind matched-pairs randomized comparison trial | 57 | 5–16 y (10 y 2 m) |
| Seay, 2004 [39] | Peer-reviewed: masters thesis | Not described | 157 | 6th–8th Grade |
| Seymour, 2012 [40] | Peer-reviewed: masters thesis | Qualitative | Not described | “children” |
| Seymour & Wise, 2017 [58] | Peer-reviewed: journal article | Not described | Not described | 3–5 y |
| Smith et al., 2017 [70] | Grey literature: report | Mixed-methods | 11 circus programs | 6–18 y |
| Spiegel et al., 2015 [59] | Peer-reviewed: journal article | Mixed methods case study | Not described | “youth and children” |
| Stevens et al., 2019 [14] | Peer-reviewed: journal article | Qualitative | 55 | 8–14 y (10 y 0 m) |
| Taylor & Taylor, 2004 [62] | Peer-reviewed: journal article | Case study | 20 | 12–18 y |
| Trotman, 2013a [67] | Grey literature: report | Mixed-methods | 28 | 8–10 y |
| Trotman, 2013b [68] | Grey literature: report | Qualitative | 13 | 0–4 y |
| Valentini et al., 2020 [74] | Grey literature: conference proceeding | Qualitative | 211 | 9–12 y (10 y 0 m) |
| Van Es et al., 2021 [21] | Peer-reviewed: journal article | Qualitative | 11 | 5–20 y |
Appendix E. Extracted Outcome Data
| Citations | For Whom | Outcome Measures & Time Point | Health & Wellbeing Outcomes Reported |
|---|---|---|---|
| Agans et al., 2019 [17] | General population (circus school) | Single timepoint in an ongoing program: quantitative survey.
|
|
| Barnett et al., 2020 [18] | General population (primary school) | Timepoint not described: literature review |
|
| Biquet, 2014 [35] | “living in a warzone” | Single timepoint in an ongoing program: participant observations, semi-structured interviews. |
|
| Bolton, 2004 [33] | General population (ex-pats & local community) | Timepoint not described: custom survey, interviews, observations. |
|
| Bonk, 2019 [34] | General population (circus school) | Single timepoint immediately following intervention: Body map artwork & participant interview. |
|
| Boyd et al., 2010 [42] | Cerebral palsy: unilateral hemiplegia | Protocol: Data to be collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
| Protocol only (no outcomes described) |
| Boyd et al., 2013 [41] | Cerebral palsy: unilateral hemiplegia | Protocol: Data to be collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
| Protocol only (no outcomes described) |
| Cadwell & Rooney, 2013 [71] | General population (circus school) | Single timepoint in an ongoing program: self-reporting questionnaires, panel discussion & survey ‘game’ |
|
| Caldwell, 1996 [75] | General population (circus school) | Timepoint not described: observation. |
|
| Candy, 2017 [20] | General population | Single timepoint in an ongoing program: custom quantitative surveys. |
|
| Cohen, 2018 [43] | General population (circus school) | Data collected at 3 timepoints (no further description provided): results from Smith, 2017 | Large positive change in individual youths’ social-emotional behavioural skills (emotion management, teamwork, initiative, empathy, responsibility, problem solving) |
| Csuros, 2015 [44] | Children in psychiatric care: “conduct disorder, hyperactivity, attention deficit disorder (ADD), autism, spectrum disorders and psychiatric disorders requiring emergency care (crisis conditions, suicidal intensions or attempted suicide, self-destructive behaviour, sudden psychotic conditions), schizophrenia, mood disorders, anxiety disorders, post-traumatic disorder, emerging personality disorders, mood disorders, obsessive compulsive disorder, eating disorders, attachment disorders.” | Timepoint not described: observations. |
|
| Fernandez et al., 2018 [22] | Children with developmental difficulties (without a specified medical condition or disability). | Single timepoint, immediately following intervention:
|
|
| Fournier et al., 2014 [4] | Children in psychiatric care: mood disorders, anxiety disorders, relational or behavioural problems, attention deficit hyperactivity disorder (ADHD), psychotic disorders, eating disorders. | Data collected at 3 timepoints: prior to, immediately following and 3-months after intervention.
|
|
| Gilmore et al., 2010 [45] | Cerebral palsy | Single timepoint during intervention: Semi-structured interviews, video footage and recall diary. |
|
| Heller & Taglialatela, 2018 [6] | ADD, ADHD, anxiety, autism, behavioural challenges, impulse control challenges (sourced from personal communication with author). | Data collected at 3 timepoints: prior to intervention, end of first intervention block, end of second intervention block. Parental report using custom online surveys. |
|
| Kiez, 2015 [36] | General population (primary school) | Data collected at 2 timepoints: prior to and on completion of intervention.
|
|
| Kinnunen et al., 2013 [69] | Variety of populations, including “special needs” class (school); general population (school & pre-school); ADD/ ADHD, autism; children of families who use the child welfare services and are dealing with crises; children with visual impairment. | Single timepoint in an ongoing program: surveys and interviews. |
|
| Kriellaars et al., 2019 [8] | General population (primary school) | Data collected at 2 timepoints: prior to and on completion of intervention.
|
|
| Kovalenko, 2018 [29] | “at risk”: children from difficult family circumstances, adolescents who have committed an offence, children with disability. | Data collected over a 12-month period in an ongoing program: observation and interviews. |
|
| Loiselle et al., 2019 [46] | Young people with physical disabilities including: cerebral palsy, leukodystrophy, Steiner’s syndrome, Childhood callosotomy sequelae for uncontrolled epilepsy, Friedrich’s ataxia, traumatic acquired brain injury (ABI), severe burns in infancy | Data collected at 3 timepoints: prior to, mid-point and on completion of intervention.
|
|
| Maglio & McKinstry, 2008 [9] | General population (school) | Single timepoint immediately following intervention:
|
|
| Mason, 2013 [72] | “living in a warzone” | Timepoint not described: observation |
|
| McCaffery, 2011 [65] | School students with moderate to severe learning difficulties | Single timepoint immediately following intervention:
|
|
| McCaffery, 2012 [64] | Autism | Single timepoint immediately following intervention:
|
|
| McCaffery, 2014 [63] | “at risk” school students: at-risk of disengagement, poor attendance or leaving school early. | Single timepoint immediately following intervention:
|
|
| McCutcheon, 2003 [37] | “at risk” school students | Single timepoint in ongoing programs:
|
|
| McGrath & Stevens, 2019 [47] | General population (circus school) | Data collected pre- and post-intervention:
|
|
| Miller et al., 2016 [48] | Cerebral palsy: unilateral hemiplegia | Single timepoint: mid-intervention
| Children in circus group were more motivated and engaged |
| Momesso dos Santos et al., 2015 [49] | Overweight | Single timepoint: Blood sample (lymphocyte, plasma glucose & insulin concentration, plasma inflammatory markers) |
|
| Neave et al., 2020 [50] | General population (school) | Data collected pre- and post-intervention:
| Circus participants had fewer emotional problems (SDQ) (psychosomatic illness, worries, unhappiness, nervousness, lack of confidence and fearfulness), no other significant differences |
| O’Donnell, n.d. [66] | “at-risk” due to socioeconomic status, single-parent homes, and/or a history of truancy and disruptive classroom behaviour at school; inpatient psychiatric unit. | Data collected pre- and post-intervention:
|
|
| Ott, 2005 [38] | General population (circus school) | Data collected over a 5-month period and then followed up 4 and 5 years later: semi-structured interviews & observation |
|
| Pompe, 2021 [30] | Inpatient psychiatric unit | Timepoint not described: observations & case studies |
|
| Rappaport, 2014 [73] | Inpatient psychiatric unit: mood disorder, bipolar, depression; deaf, hard of hearing, or othercommunication difficulties. | Timepoint not described: thematic analysis of program evaluations |
|
| Rivard et al., 2010 [51] | Vulnerable young people in “difficult situations”. | Single timepoint in an ongoing program: observation and interviews |
|
| Rodger & Kennedy-Behr, 2017 [32] | Cerebral palsy | Timepoint not described: literature review drawing on results from Sakzewski et al. 2011 a [54], b [55], c [61] |
|
| Sahli et al., 2013 [52] | General population (circus school) | Single timepoint in an ongoing program: force platform centre of pressure excursions for:
|
|
| Sakzewski, Ziviani, & Boyd, 2011 [53] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
|
|
| Sakzewski, Ziviani, Abbott, et al., 2011a [54] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
| Significant improvements in bi-manual performance following intervention. Small difference between training approaches (both including circus), with one approach (BIM) showing retained gains at 26 weeks, and the other (CIMT) showing additional improvements in unimanual capacity |
| Sakzewski, Ziviani, Abbott, et al., 2011b [55] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
|
|
| Sakzewski, Miller, et al., 2015 [56] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
|
|
| Sakzewski, Provan, et al., 2015 [57] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
|
|
| Sakzewski, Ziviani, et al., 2015 [16] | Cerebral palsy: unilateral hemiplegia | Literature review in book chapter | Circus activities can support psychological need satisfaction |
| Sakzewski et al., 2012 [60] | Cerebral palsy: unilateral hemiplegia | Data collected at 3 timepoints: prior to, on completion, and 26 weeks post- intervention.
| Both groups improved quality of life, and these changes were retained at 3-months |
| Sakzewski, Ziviani, Abbott, et al., 2011c [61] | Cerebral palsy: unilateral hemiplegia | 52-week follow-up (single time point)
| Gains in unimanual capacity, bimanual performance and individual outcomes are retained at 1-year |
| Seay, 2004 [39] | General population (school) | Data collected at 3 timepoints: prior to, on completion, and 3-month post- intervention.
|
|
| Seymour, 2012 [40] | Autism and other neurodiversities | Timepoint not described
| Participants develop trust and community, physical development and personal confidence, improvements in day-to-day tasks, improvements in muscle tone and motor coordination; improvement in posture; improved attention; improved ability to participate in a group and confidence in social interactions; improved self-perception and motivation; improved coordination, and attention regulation |
| Seymour & Wise, 2017 [58] | Autism | Timepoint not described
| Circus builds trust & connection, belonging, coordination, spatial awareness, joy, develops body awareness and fitness, improves confidence and trust in physical capabilities |
| Smith et al., 2017 [70] | General population (circus school) | Data collected at baseline & completion of 3 programs over 3 timepoints:
| Participants demonstrated positive and substantial social-emotional behavioural skill growth |
| Spiegel et al., 2015 [59] | Youth “living on the street” | Protocol—timepoint not described:
| From included literature review: circus promotes creativity and building perseverance, team building, social engagement, and social inclusion |
| Stevens et al., 2019 [14] | General population (circus school) | Single timepoint in ongoing program: focus group |
|
| Taylor & Taylor, 2004 [62] | Range of intellectual and/or physical disabilities (mild to severe) | Timepoint not described: observation of videos of practice & performance |
|
| Trotman, 2013a [67] | General population (school) | Single timepoint following intervention:
|
|
| Trotman, 2013b [68] | General population (circus school) | Single timepoint in ongoing program: interviews and custom survey. |
|
| Valentini et al., 2020 [74] | General population (primary school) | Timepoint not described: literature review |
|
| Van Es et al., 2021 [21] | Refugee youth/ children and youth with traumatic war experiences. | Single timepoint during intervention: Semi-structured interviews and participant observations |
|
References
- World Health Organisation [WHO]. International Classification of Health Interventions (ICHI). Available online: http://www.who.int/classifications/ichi/en/ (accessed on 18 July 2020).
- Fortune, N.; Madden, R.; Almborg, A.H. Use of a new international classification of health interventions for capturing information on health interventions relevant to people with disabilities. Int. J. Environ. Res. Public Health 2018, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Fournier, C.; Drouin, M.A.; Marcoux, J.; Garel, P.; Bochud, E.; Théberge, J.; Aubertin, P.; Favreau, G.; Fleet, R. Cirque du Monde as a health intervention: Perceptions of medical students and social circus experts. Can. Fam. Physician 2014, 60, e548–e553. [Google Scholar] [PubMed]
- Baumgold, J. Exploring the experiences of adults participating in community circus classes: The synergistic relationship between circus and occupational therapy. Master’s Thesis, Utica College, Utica, NY, USA, 2017. [Google Scholar]
- Heller, C.; Taglialatela, L.A. Circus Arts Therapy® fitness and play therapy program shows positive clinical results. Int. J. Play Ther. 2018, 27, 69–77. [Google Scholar] [CrossRef]
- Spiegel, J.B.; Breilh, M.C.; Campana, A.; Marcuse, J.; Yassi, A. Social circus and health equity: Exploring the national social circus program in Ecuador. Arts Health 2015, 7, 65–74. [Google Scholar] [CrossRef]
- Kriellaars, D.J.; Cairney, J.; Bortoleto, M.A.C.; Kiez, T.K.M.; Dudley, D.; Aubertin, P. The impact of circus arts instruction in physical education on the physical literacy of children in Grades 4 and 5. J. Teach. Phys. Educ. 2019, 38, 162–170. [Google Scholar] [CrossRef]
- Maglio, J.; McKinstry, C. Occupational therapy and circus: Potential partners in enhancing the health and well-being of today’s youth. Aust. Occup. Ther. J. 2008, 55, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Woodhead, P. To Study In-School Circus Programmes with Emphasis on Management and Teaching Practices, and Efficacy of the Visited Programmes in Terms of Student Welfare, Performance and Physical Education Opportunities. Churchill Trust. 2002, pp. 1–16. Available online: https://www.churchilltrust.com.au/fellow/paul-woodhead-nsw-2002 (accessed on 9 February 2022).
- Sugarman, R.J. Circus for Everyone: Circus Learning around the World; Mountainside Press: Laguna Woods, CA, USA, 2001. [Google Scholar]
- Imms, C.; Granlund, M.; Wilson, P.H.; Steenbergen, B.; Rosenbaum, P.L.; Gordon, A.M. Participation, both a means and an end: A conceptual analysis of processes and outcomes in childhood disability. Dev. Med. Child Neurol. 2017, 59, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Cadwell, S.J. Falling together: An examination of trust-building in youth and social circus training. Theatre Danc. Perform. Train. 2018, 9, 19–35. [Google Scholar] [CrossRef]
- Stevens, K.; McGrath, R.; Ward, E. Identifying the influence of leisure-based social circus on the health and well-being of young people in Australia. Ann. Leis. Res. 2019, 22, 305–322. [Google Scholar] [CrossRef]
- Trotman, R. Building Character and Community, Community Circus: A Literature Review. Lotteries Community Research Fund. 2012, pp. 1–54. Available online: https://docplayer.net/35082073-April-building-character-and-community-community-circus-a-literature-review.html (accessed on 28 July 2020).
- Sakzewski, L.; Ziviani, J.; Poulsen, A. The Allure of the Circus: Embedding Goals in a Naturalistic Leisure Setting. In Goal Setting and Motivation in Therapy: Engaging Children and Parents; Poulsen, A., Ziviani, J., Cuskelly, M., Eds.; Jessica Kingsley Publishers: London, UK, 2015; pp. 89–99. [Google Scholar]
- Agans, J.P.; Davis, J.L.; Vazou, S.; Jarus, T. Self-determination through circus arts: Exploring youth development in a novel activity context. J. Youth Dev. 2019, 14, 110–129. [Google Scholar] [CrossRef]
- Barnett, L.M.; Dennis, R.; Hunter, K.; Cairney, J.; Keegan, R.J.; Essiet, I.A.; Dudley, D.A. Art meets sport: What can actor training bring to physical literacy programs? Int. J. Environ. Res. Public Health 2020, 17, 4497. [Google Scholar] [CrossRef] [PubMed]
- Bolton, R. Circus as education. Australas. Drama Stud. 1999, 35, 9–18. [Google Scholar]
- Candy, N. Stretching and Strengthening Circus Teaching in Iceland. Master’s Thesis, Iceland Academy of the Arts, Reykjavik, Iceland, 2017. [Google Scholar]
- Van Es, V.; Rommes, E.; De Kwaadsteniet, L. Building resilience by becoming a circus artist. J. Refug. Stud. 2021, 34, 760–786. [Google Scholar] [CrossRef]
- Fernandez, Y.; Ziviani, J.; Cuskelly, M.; Colquhoun, R.; Jones, F. Participation in community leisure programs: Experiences and perspectives of children with developmental difficulties and their parents. Leis. Sci. 2018, 40, 110–130. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.M.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Khalil, H.; Peters, M.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Parker, D. An evidence-based approach to scoping reviews. Worldviews Evid.-Based Nurs. 2016, 13, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Coulston, F.; Cameron, K.L.; Spittle, A.; Sellick, K.; Toovey, R. Circus activities as a health intervention for children, youth, and adolescents: A scoping review protocol. JBI Evid. Synth. 2021, 20, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Youth. United Nations. Available online: https://www.un.org/en/sections/issues-depth/youth-0/ (accessed on 3 August 2020).
- UN General Assembly. The Convention on the Rights of the Child; United Nations: New York, NY, USA, 1989; Volume 1577.
- Kovalenko, D. Social Circus as a New Form of Solidarity in Russia: Case Study of a Socio-Cultural Project. Bachelor’s Thesis, Saint Petersburg State University, Saint Petersburg, Russia, 2018. [Google Scholar]
- Pompe, V. Circus therapy: Research into the Use of Circus as a Therapeutic Medium in Child and Adolescent Psychiatry. Bachelor’s Thesis, De Artevelde University of Applied Sciences, Ghent, Belgium, 2021. [Google Scholar]
- Gmelig Meyling, C.; Verschuren, O.; Rentinck, I.R.; Engelbert, R.H.H.; Gorter, J.W. Physical rehabilitation interventions in children with acquired brain injury: A scoping review. Dev. Med. Child Neurol. 2022, 64, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Rodger, S.; Kennedy-Behr, A. (Eds.) Occupation-Centred Practice with Children: A Practical Guide for Occupational Therapists, 2nd ed.; John Wiley & Sons: Oxford, UK, 2017. [Google Scholar]
- Bolton, R. Why Circus Works: How the Values and Structures of Circus Make It a Significant Developmental Experience for Young People. Ph.D. Thesis, Murdoch University, Perth, Australia, 2004. [Google Scholar]
- Bonk, R. The Role of Circus Arts in Art Therapy. Master’s Thesis, Saint Mary-of-the-Woods College, St. Mary’s, IN, USA, 2019. [Google Scholar]
- Biquet, D. Performing Arts as Vehicle for Youth Empowerment: The Case of the Palestinian Circus School. Master’s Thesis, Ghent University, Ghent, Belgium, 2014. [Google Scholar]
- Kiez, T.K.M. The Impact of Circus Arts Instruction on the Physical Literacy of Children in Grades 4 and 5. Master’s Thesis, The University of Manitoba, Winnipeg, MB, Canada, 2015. [Google Scholar]
- McCutcheon, S. Negotiating Identity through Risk: A Community Circus Model for Evoking Change and Empowering Youth. Master’s Thesis, Charles Sturt University, Bathurst, Australia, 2003. [Google Scholar]
- Ott, D. A Phenomenology of Youth Circus Training at Fern Street Circus. Ph.D. Thesis, Arizona State University, Tempe, AZ, USA, 2005. [Google Scholar]
- Seay, A. The Effects of a Circus of the Kids Program on the Psychosocial Functioning of Middle School Youth. Master’s Thesis, University of South Alabama, Mobile, AL, USA, 2004. [Google Scholar]
- Seymour, K. How Circus Training Can Enhance the Well-Being of Children with Autism and Their Families. Master’s Thesis, Griffith University, Brisbane, Australia, 2012. [Google Scholar]
- Boyd, R.N.; Ziviani, J.; Sakzewski, L.; Miller, L.; Bowden, J.; Cunnington, R.; Ware, R.; Guzzetta, A.; Al Macdonell, R.; Jackson, G.D.; et al. COMBIT: Protocol of a randomised comparison trial of COMbined modified constraint induced movement therapy and bimanual intensive training with distributed model of standard upper limb rehabilitation in children with congenital hemiplegia. BMC Neurol. 2013, 13, 68. [Google Scholar] [CrossRef] [PubMed]
- Boyd, R.; Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Badawy, R.; Gilmore, R.; Provan, K.; Tournier, J.D.; Macdonell, R.A.; Jackson, G.D. INCITE: A randomised trial comparing constraint induced movement therapy and bimanual training in children with congenital hemiplegia. BMC Neurol. 2010, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A. Social circus: Developing structures for program efficacy in the United States. Perform. Matters 2018, 4, 134–140. [Google Scholar]
- Csuros, D. Circus workshops in the child psychiatry. Arteterapia 2015, 10, 269–280. [Google Scholar]
- Gilmore, R.; Ziviani, J.; Sakzewski, L.; Shields, N.; Boyd, R. A balancing act: Children’s experience of modified constraint-induced movement therapy. Dev. Neurorehabilit. 2010, 13, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Loiselle, F.; Rochette, A.; Tétreault, S.; Lafortune, M.; Bastien, J. Social circus program (Cirque du Soleil) promoting social participation of young people living with physical disabilities in transition to adulthood: A qualitative pilot study. Dev. Neurorehabilit. 2019, 22, 250–259. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.; Stevens, K. Forecasting the social return on investment associated with children’s participation in circus-arts training on their mental health and well-being. Int. J. Sociol. Leis. 2019, 2, 163–193. [Google Scholar] [CrossRef]
- Miller, L.; Ziviani, J.; Ware, R.S.; Boyd, R.N. Does context matter? Mastery motivation and therapy engagement of children with cerebral palsy. Phys. Occup. Ther. Pediatr. 2016, 36, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Momesso dos Santos, C.M.; Sato, F.T.; Cury-Boaventura, M.F.; Guirado-Rodrigues, S.H.; Cacula, K.G.; Goncalves Santos, C.C.; Hatanaka, E.; de Oliveira, H.H.; Santos, V.C.; Murata, G.; et al. Effect of regular circus physical exercises on lymphocytes in overweight children. PLoS ONE 2015, 10, e0120262. [Google Scholar] [CrossRef] [PubMed]
- Neave, N.; Johnson, A.; Whelan, K.; McKenzie, K. The psychological benefits of circus skills training (CST) in schoolchildren. Theatre Danc. Perform. Train. 2020, 11, 488–497. [Google Scholar] [CrossRef]
- Rivard, J.; Bourgeault, G.; Mercier, C. Cirque du Monde in Mexico City: Breathing new life into action for young people in difficult situations. Int. Soc. Sci. J. 2010, 61, 181–194. [Google Scholar] [CrossRef]
- Sahli, S.; Ghroubi, S.; Rebai, H.; Chaabane, M.; Yahia, A.; Pérennou, D.; Elleuch, M.H. The effect of circus activity training on postural control of 5–6-year-old children. Sci. Sports 2013, 28, 11–16. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Boyd, R.N. Best responders after intensive upper-limb training for children with unilateral cerebral palsy. Arch. Phys. Med. Rehabil. 2011, 92, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Macdonell, R.A.L.; Jackson, G.D.; Boyd, R.N. Randomized trial of constraint-induced movement therapy and bimanual training on activity outcomes for children with congenital hemiplegia. Dev. Med. Child Neurol. 2011, 53, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Macdonell, R.A.L.; Jackson, G.D.; Boyd, R.N. Participation outcomes in a randomized trial of 2 models of upper-limb rehabilitation for children with congenital hemiplegia. Arch. Phys. Med. Rehabil. 2011, 92, 531–539. [Google Scholar] [CrossRef]
- Sakzewski, L.; Miller, L.; Ziviani, J.; Abbott, D.F.; Rose, S.; Macdonell, R.A.; Boyd, R.N. Randomized comparison trial of density and context of upper limb intensive group versus individualized occupational therapy for children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 539–547. [Google Scholar] [CrossRef]
- Sakzewski, L.; Provan, K.; Ziviani, J.; Boyd, R.N. Comparison of dosage of intensive upper limb therapy for children with unilateral cerebral palsy: How big should the therapy pill be? Res. Dev. Disabil. 2015, 37, 9–16. [Google Scholar] [CrossRef]
- Seymour, K.; Wise, P. Circus training for autistic children: Difference, creativity, and community. New Theatre Q. 2017, 33, 78–90. [Google Scholar] [CrossRef]
- Spiegel, J.B.; Breilh, J.; Yassi, A. Why language matters: Insights and challenges in applying a social determination of health approach in a North-South collaborative research program. Glob. Health 2015, 11, 9. [Google Scholar] [CrossRef]
- Sakzewski, L.; Carlon, S.; Shields, N.; Ziviani, J.; Ware, R.S.; Boyd, R.N. Impact of intensive upper limb rehabilitation on quality of life: A randomized trial in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Macdonell, R.A.L.; Jackson, G.D.; Boyd, R.N. Equivalent retention of gains at 1 year after training with constraint-induced or bimanual therapy in children with unilateral cerebral palsy. Neurorehabilit. Neural Repair 2011, 25, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Taylor, C. Circus ‘C’: An innovative approach to leisure for people with disabilities. Ann. Leis. Res. 2004, 7, 127–142. [Google Scholar] [CrossRef]
- McCaffery, N. Malone College Project Evaluation; Streetwise Community Circus CIC: Belfast, UK, 2014; pp. 1–37. [Google Scholar]
- McCaffery, N. National Autistic Society Project Evaluation; Streetwise Community Circus CIC: Belfast, UK, 2012; pp. 1–24. [Google Scholar]
- McCaffery, N. Knockavoe School Evaluation; Streetwise Community Circus CIC: Belfast, UK, 2011; pp. 1–43. [Google Scholar]
- O’Donnell, J. Circus Mojo Evaluation Report; C.A.R.E. Consultancy, n.d. pp. 1–26. Available online: https://circusmojo.com/circus-mojo-evaluation-report/ (accessed on 21 January 2022).
- Trotman, R. Evaluation of a Community Circus Skills Programme at Dargaville Primary School; Lotteries Community Sector Research Fund: Dargaville, New Zealand, 2013; pp. 1–24. Available online: http://www.bibliotheque.enc.qc.ca/Record.htm?Record=19143236124919614189 (accessed on 4 February 2021).
- Trotman, R. Evaluation of the SKIP Community Circus Programme in Dargaville; Lotteries Community Sector Research Fund: Dargaville, New Zealand, 2013; pp. 1–16. Available online: http://www.bibliotheque.enc.qc.ca/Record.htm?record=19143209124919614819 (accessed on 4 February 2021).
- Kinnunen, R.; Lidman, J.; Kakko, S.C.; Kekäläinen, K. “They’re Smiling from Ear to Ear”: Wellbeing Effects from Social Circus; Centre for Practice as Research in Theatre, University of Tampere: Tampere, Finland, 2013; pp. 1–68. [Google Scholar]
- Smith, C.; Roy, L.; Peck, S.; MacLeod, C. Evaluation of Program Quality and Social and Emotional Learning in American Youth Circus Organization Social Circus Programs; The David P. Weikart Center for Youth Program Quality: Ypsilanti, MI, USA, 2017; pp. 1–33. [Google Scholar]
- Cadwell, S.; Rooney, B. Measuring happiness: Assessing the intrinsic value of youth circus. In Effective Circus Project, Proceedings of the Culture Has an Impact! Seminar, Tampere, Finland, 12–15 December 2013; Kekäläinen, K., Ed.; University of Tampere: Tampere, Finland, 2013; pp. 52–60. [Google Scholar]
- Mason, D. Social circus in a warzone. In Effective Circus Project, Proceedings of the Culture Has an Impact! Seminar, Tampere, Finland, 12–15 December 2013; Kekäläinen, K., Ed.; University of Tampere: Tampere, Finland, 2013; pp. 14–26. [Google Scholar]
- Rappaport, S. Circus arts & occupational therapy: Gaining great performance. Conference unknown. Br. J. Occup. Ther. 2014, 77, 23–24. [Google Scholar]
- Valentini, M.; Cesauri, A.; Schembri, R.; Federici, A. Circus-mobility: The value of a circus laboratory at school. J. Hum. Sport Exerc. 2020, 15, S1081–S1092. [Google Scholar]
- Caldwell, M.L. Juggling to learn. Teaching Pre K-8 1996, 27, 47. [Google Scholar]
- Sakzewski, L.; Ziviani, J.; Boyd, R.N. Efficacy of upper limb therapies for unilateral cerebral palsy: A meta-analysis. Pediatrics 2014, 133, e175–e204. [Google Scholar] [CrossRef]
- Bessone, I. Social circus as an organised cultural encounter: Embodied knowledge, trust and creativity at play. J. Intercult. Stud. 2017, 38, 651–664. [Google Scholar] [CrossRef]
- Spiegel, J.B. Singular Bodies, Collective dreams: Socially engaged circus arts and the “Quebec Spring”. In Cirque Global; Leroux, L.P., Batson, C., Eds.; McGill-Queen’s University Press: Montreal, QC, Canada, 2016; pp. 266–283. [Google Scholar]
- Bungay, H.; Vella-Burrows, T. The effects of participating in creative activities on the health and well-being of children and young people: A rapid review of the literature. Perspect. Public Health 2013, 133, 44–52. [Google Scholar] [CrossRef]
- Davies, C.; Knuiman, M.; Rosenberg, M. The art of being mentally healthy: A study to quantify the relationship between recreational arts engagement and mental well-being in the general population. BMC Public Health 2016, 16, 15. [Google Scholar] [CrossRef]
- Zarobe, L.; Bungay, H. The role of arts activities in developing resilience and mental wellbeing in children and young people a rapid review of the literature. Perspect. Public Health 2017, 137, 337–347. [Google Scholar] [CrossRef]
- Ryan, R.; Deci, E. Self-determination theory. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Anaby, D.; Hand, C.; Bradley, L.; DiRezze, B.; Forhan, M.; DiGiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]. International Classification of Functioning, Disability and Health: Children and Youth Version: ICF-CY. 2007. Available online: https://apps.who.int/iris/handle/10665/43737 (accessed on 19 May 2021).
- Rosenbaum, P.; Gorter, J.W. The “F-words” in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]
- World Health Organisation [WHO]. Health Equity. Available online: https://www.who.int/health-topics/health-equity (accessed on 20 August 2022).
- Mills, I.S.; Doyle, L.W.; Cheong, J.L.; Roberts, G. Rates of early intervention services in children born extremely preterm/ extremely low birthweight. J. Paediatr. Child Health 2018, 54, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Roberts, G.; Howard, K.; Spittle, A.J.; Brown, N.C.; Anderson, P.J.; Doyle, L.W. Rates of early intervention services in very preterm children with developmental disabilities at age 2 years. J. Paediatr. Child Health 2008, 44, 276–280. [Google Scholar] [CrossRef]
- Malik, J.; Stemplewski, R.; Maciaszek, J. The effect of juggling as dual-task activity on human neuroplasticity: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 7102. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, T.; Nakahara, K.; Uehara, M.; Koyama, K.I.; Li, K.; Harada, T.; Yasuhara, D.; Taguchi, H.; Kojima, S.; Sagiyama, K.I.; et al. Effect of juggling therapy on anxiety disorders in female patients. BioPsychoSocial Med. 2007, 1, 10. [Google Scholar] [CrossRef]





| Intervention Elements | Circus Disciplines | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Citations Grouped by Intervention | Sessions per Week (Number) | Total Sessions (Number) | Duration per Session (Hours) | Total Dosage (Hours) | Aerials | Acrobatics | Object Manipulation | Equilibristics | Clowning |
| Agans et al., 2019 [17] | Not described | X 1 | X | X | X | X | |||
| Barnett et al., 2020 [18]; Kiez, 2015 [36]; Kriellaars et al., 2019 [8]; Valentini et al., 2020 [74] | 1–4 | 10–84 | 1 | 10–84 | X | X | X | X | |
| Biquet, 2014 [35] | 1 | ongoing program | 3 | X | X | X | X | ||
| Bolton, 2004 [33] | 2 | - | X | X | X | ||||
| Bonk, 2019 [34] | 1 | 1 | 1 | 1 | X | X | X | X | |
| Boyd et al., 2010 [42]; Gilmore et al., 2010 [45]; Rodger & Kennedy-Behr, 2017 [32]; Sakzewski et al., 2012 [60]; Sakzewski, Provan, et al., 2015 [57]; Sakzewski, Ziviani, Abbott, et al., 2011a [54], 2011b [55], 2011c [61]; Sakzewski, Ziviani, & Boyd, 2011 [53]; Sakzewski, Ziviani & Poulsen, 2015 [16]; | 5 | 10 | 2 (in addition to 4 h of other activities) | 20 (of circus activities) | X | X | X | ||
| Boyd et al., 2013 [41]; Miller et al., 2016 [48]; Sakzewski, Miller, et al., 2015 [56] | 5 | 10 | 2 | 20 | X | X | X | ||
| Cadwell & Rooney, 2013 [71] | ongoing program | Specific circus activities not described | |||||||
| Caldwell, 1996 [75] | Not described | X | |||||||
| Candy, 2017 [20] | 1 or 2 | ongoing program | 2.5 | X | X | X | |||
| Cohen, 2018 [43]; Smith et al., 2017 [70] | ongoing programs | Specific circus activities not described | |||||||
| Csuros, 2015 [44] | 1 | ongoing program | X | X | X | ||||
| Fernandez et al., 2018 [22] | 1 | 10 | 1 | 10 | X | X | |||
| Fournier et al., 2014 [4] | 2 | 24 | Specific circus activities not described | ||||||
| Heller & Taglialatela, 2018 [6] | 1 | 16 | 1 | 16 | X | X | X | ||
| Kinnunen et al., 2013 [69] | ongoing program | X | X | X | X | ||||
| Kovalenko, 2018 [29] | 5 | ongoing program | 1.5–3 | X | X | ||||
| Loiselle et al., 2019 [46] | 2 | 48 | 2 | 96 | X | X | X | X | X |
| Maglio & McKinstry, 2008 [9] | 1 | 10–40 | 1 | 10–40 | X | X | X | ||
| Mason, 2013 [72] | 5 | 5 | X | X | |||||
| McCaffery, 2011 [65] | 1 | 18 | 1.5–2 | 27–36 | X | X | |||
| McCaffery, 2012 [64] | 18 | 1.5 | 27 | X | X | ||||
| McCaffery, 2014 [63] | 1 | 8 | 1.5 | 12 | X | X | |||
| McCutcheon, 2003 [37] | ongoing programs | X | X | X | X | X | |||
| McGrath & Stevens, 2019 [47] | 1 | 20 | 1 | 20 | X | X | X | ||
| Momesso dos Santos et al., 2015 [49] | 2 | 38 | 1 | 38 | X | X | X | ||
| Neave et al., 2020 [50] | 1 | 18 | 1 | 18 | X | X | X | X | |
| O’Donnell, n.d. [66] | 1 | 1 | X | X | X | X | |||
| Ott, 2005 [38] | 2 | ongoing program | 2 | X | X | X | X | X | |
| Pompe, 2021 [30] | ongoing program | X | X | ||||||
| Rappaport, 2014 [73] | 1–2 | 0.75–1.25 | X | X | X | X | X | ||
| Rivard et al., 2010 [51] | 1–2 | ongoing program | X | X | |||||
| Sahli et al., 2013 [52] | 2 | ongoing program | 2 | X | X | ||||
| Seay, 2004 [39] | Not described | X | X | X | |||||
| Seymour, 2012 [40] | 1 | ongoing program | X | X | X | X | |||
| Seymour & Wise, 2017 [58] | 1 | X | X | X | |||||
| Spiegel et al., 2015 [59] | Not described | Specific circus activities not described | |||||||
| Stevens et al., 2019 [14] | ongoing program | X | X | X | |||||
| Taylor & Taylor, 2004 [62] | 3 | ongoing program | 1 | X | X | ||||
| Trotman, 2013a [67] | 1 | 8 | 1.5 | 12 | X | X | X | ||
| Trotman, 2013b [68] | 1 | ongoing program | 1 | X | X | ||||
| Van Es et al., 2021 [21] | 2 | 16 | 5 | 80 | X | X | X | X | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coulston, F.; Cameron, K.L.; Sellick, K.; Cavallaro, M.; Spittle, A.; Toovey, R. Circus Activities as a Health Intervention for Children, Youth, and Adolescents: A Scoping Review. J. Clin. Med. 2023, 12, 2046. https://doi.org/10.3390/jcm12052046
Coulston F, Cameron KL, Sellick K, Cavallaro M, Spittle A, Toovey R. Circus Activities as a Health Intervention for Children, Youth, and Adolescents: A Scoping Review. Journal of Clinical Medicine. 2023; 12(5):2046. https://doi.org/10.3390/jcm12052046
Chicago/Turabian StyleCoulston, Free, Kate L. Cameron, Kath Sellick, Madeline Cavallaro, Alicia Spittle, and Rachel Toovey. 2023. "Circus Activities as a Health Intervention for Children, Youth, and Adolescents: A Scoping Review" Journal of Clinical Medicine 12, no. 5: 2046. https://doi.org/10.3390/jcm12052046
APA StyleCoulston, F., Cameron, K. L., Sellick, K., Cavallaro, M., Spittle, A., & Toovey, R. (2023). Circus Activities as a Health Intervention for Children, Youth, and Adolescents: A Scoping Review. Journal of Clinical Medicine, 12(5), 2046. https://doi.org/10.3390/jcm12052046