
Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment
2.3. Protocol
2.4. Measures
- Does the user read attentional cues well?: At the top of the screen, the following sentence appears ‘find attentional cues’.
- Attentional cues search: Indicate if the user can find the orange spheres that appear around the arena.
- Does the user use the button to make them disappear?: The user has to use the joypad (the button ‘A’) to make attentional cues disappear.
- Does the user read the sentence well?: A message appears ‘find the guideline’.
- Guideline search: Indicate if the user uses the line to reach the object.
- 3dRudder rotation to find the object: Indicate if the user turns the 3dRudder correctly to find the object.
- Does the user see the object well?: Indicate whether the user sees the object well.
- Advancement with the 3dRudder to reach the object: Indicate if the user easily uses the 3dRudder to reach and pick the object.
- Does the user read the 3D map well?: On the screen, the user can see a map with cardinal points indicating their direction and the landmarks’ locations.
- Object relocation: The user has to relocate the object four times using the 3dRudder to reach the correct point.
- Does the user use the button to relocate?: The user has to use the joypad (button ‘A’) to put the object in the preferred location.
- Does the user read the relocation feedback well?: A message is shown on the screen ‘congratulations’ if the position is right or ‘try again’ if it is wrong.
- Does the user see the position marker well?: The user has to go to the exact location of the item looking for a white circle on the ground that indicates the correct location.
3. Results
3.1. Quantitative Measures
3.2. Qualitative Measures
“I don’t see any objects”.(ID 3)
“I’m towards the Northwest, I don’t read well”.(ID 1)
“It’s too fast! I didn’t read it in time!”.(ID 1)
“I have to do some practice”.(ID 2)
“It seemed like an easy game, once you understand how you have to move there is no problem”.(ID 3)
“It’s the first time I’ve used the platform and the joystick, I’m not skilled”.(ID 8)
“Then I liked it”.(ID 4)
“I liked it”.(ID 6)
“I don’t really like games”.(ID 8)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [PubMed]
- Facal, D.; Guàrdia-Olmos, J.; Juncos-Rabadán, O. Diagnostic transitions in mild cognitive impairment by the use of simple Markov models. Int. J. Geriatr. Psychiatry 2015, 30, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current Concepts in Mild Cognitive Impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Coughlan, G.; Laczó, J.; Hort, J.; Minihane, A.-M.; Hornberger, M. Spatial navigation deficits—Overlooked cognitive marker for preclinical Alzheimer disease? Nat. Rev. Neurol. 2018, 14, 496–506. [Google Scholar] [CrossRef]
- Tuena, C.; Mancuso, V.; Stramba-Badiale, C.; Pedroli, E.; Stramba-Badiale, M.; Riva, G.; Repetto, C. Egocentric and Allocentric Spatial Memory in Mild Cognitive Impairment with Real-World and Virtual Navigation Tasks: A Systematic Review. J. Alzheimer’s Dis. 2020, 79, 95–116. [Google Scholar] [CrossRef]
- Nedelska, Z.; Laczo, J.; Uller, M.; Vyhnalek, M.; Fripp, J.; Vlcek, K.; Parizkova, M.; Hort, J. Dementia with lewy bodies: Severe impairment of real-space navigation skills examined with human analogue of morris water maze and their structural underpinnings. J. Neurol. Sci. 2017, 381, 83–84. [Google Scholar] [CrossRef]
- Uc, E.Y.; Rizzo, M.; Anderson, S.W.; Sparks, J.D.; Rodnitzky, R.L.; Dawson, J.D. Impaired navigation in drivers with Parkinson’s disease. Brain 2007, 130, 2433–2440. [Google Scholar] [CrossRef]
- Lowry, E.; Puthusseryppady, V.; Coughlan, G.; Jeffs, S.; Hornberger, M. Path Integration Changes as a Cognitive Marker for Vascular Cognitive Impairment?—A Pilot Study. Front. Hum. Neurosci. 2020, 14, 131. [Google Scholar] [CrossRef]
- Tu, S.; Spiers, H.J.; Hodges, J.R.; Piguet, O.; Hornberger, M. Egocentric versus Allocentric Spatial Memory in Behavioral Variant Frontotemporal Dementia and Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 59, 883–892. [Google Scholar] [CrossRef]
- Tuena, C.; Serino, S.; Pedroli, E.; Stramba-Badiale, M.; Riva, G.; Repetto, C. Building Embodied Spaces for Spatial Memory Neurorehabilitation with Virtual Reality in Normal and Pathological Aging. Brain Sci. 2021, 11, 1067. [Google Scholar] [CrossRef]
- Lester, A.W.; Moffat, S.D.; Wiener, J.M.; Barnes, C.A.; Wolbers, T. The Aging Navigational System. Neuron 2017, 95, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- VandenBos, G.R. APA Dictionary of Psychology; American Psychological Association: Washington, DC, USA, 2007. [Google Scholar]
- Burgess, N. Spatial Cognition and the Brain. Ann. N. Y. Acad. Sci. 2008, 1124, 77–97. [Google Scholar] [CrossRef] [PubMed]
- Chrastil, E.R.; Warren, W.H. Active and passive spatial learning in human navigation: Acquisition of graph knowledge. J. Exp. Psychol. Learn. Mem. Cogn. 2015, 41, 1162–1178. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, E.; Perez-Lopez, M.B.; Diersch, N.; Döhler, J.; Wolbers, T.; Riemer, M. Embodiment in the aging mind. Neurosci. Biobehav. Rev. 2018, 86, 207–225. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Mancuso, V.; Cavedoni, S.; Stramba-Badiale, C. Virtual reality in neurorehabilitation: A review of its effects on multiple cognitive domains. Expert Rev. Med. Devices 2020, 17, 1035–1061. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K.; Mantovani, F. Neuroscience of Virtual Reality: From Virtual Exposure to Embodied Medicine. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 82–96. [Google Scholar] [CrossRef]
- Tuena, C.; Serino, S.; Dutriaux, L.; Riva, G.; Piolino, P. Virtual Enactment Effect on Memory in Young and Aged Populations: A Systematic Review. J. Clin. Med. 2019, 8, 620. [Google Scholar] [CrossRef]
- Plancher, G.; Tirard, A.; Gyselinck, V.; Nicolas, S.; Piolino, P. Using virtual reality to characterize episodic memory profiles in amnestic mild cognitive impairment and Alzheimer’s disease: Influence of active and passive encoding. Neuropsychologia 2012, 50, 592–602. [Google Scholar] [CrossRef]
- Cogné, M.; Auriacombe, S.; Vasa, L.; Tison, F.; Klinger, E.; Sauzéon, H.; Joseph, P.-A.; N′kaoua, B. Are visual cues helpful for virtual spatial navigation and spatial memory in patients with mild cognitive impairment or Alzheimer’s disease? Neuropsychology 2018, 32, 385–400. [Google Scholar] [CrossRef]
- Tuena, C.; Pedroli, E.; Trimarchi, P.D.; Gallucci, A.; Chiappini, M.; Goulene, K.; Gaggioli, A.; Riva, G.; Lattanzio, F.; Giunco, F.; et al. Usability Issues of Clinical and Research Applications of Virtual Reality in Older People: A Systematic Review. Front. Hum. Neurosci. 2020, 14, 93. [Google Scholar] [CrossRef]
- Mondellini, M.; Arlati, S.; Gapeyeva, H.; Lees, K.; Märitz, I.; Pizzagalli, S.L.; Otto, T.; Sacco, M.; Teder-Braschinsky, A. User Experience during an Immersive Virtual Reality-Based Cognitive Task: A Comparison between Estonian and Italian Older Adults with MCI. Sensors 2022, 22, 8249. [Google Scholar] [CrossRef] [PubMed]
- Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Mouzakidis, C.; Karathanasi, E.M.; Petridou, N.; Tsolaki, M.; Zikas, P.; Evangelou, G.; et al. A Virtual Reality App for Physical and Cognitive Training of Older People With Mild Cognitive Impairment: Mixed Methods Feasibility Study. JMIR Serious Games 2021, 9, e24170. [Google Scholar] [CrossRef] [PubMed]
- Arlati, S.; Di Santo, S.G.; Franchini, F.; Mondellini, M.; Filiputti, B.; Luchi, M.; Ratto, F.; Ferrigno, G.; Sacco, M.; Greci, L. Acceptance and Usability of Immersive Virtual Reality in Older Adults with Objective and Subjective Cognitive Decline. J. Alzheimer’s Dis. 2021, 80, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.M.; Cassels, A.K. The World Report on Ageing and Health. Gerontologist 2016, 56, S163–S166. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Somoza, L.M.; Irazoki, E.; Toribio-Guzmán, J.M.; de la Torre-Díez, I.; Diaz-Baquero, A.A.; Parra-Vidales, E.; Perea-Bartolomé, M.V.; Franco-Martín, M.Á. Usability and User Experience of Cognitive Intervention Technologies for Elderly People With MCI or Dementia: A Systematic Review. Front. Psychol. 2021, 12, 636116. [Google Scholar] [CrossRef]
- Pedroli, E.; Cipresso, P.; Greci, L.; Arlati, S.; Boilini, L.; Stefanelli, L.; Rossi, M.; Goulene, K.; Sacco, M.; Stramba-Badiale, M.; et al. An Immersive Motor Protocol for Frailty Rehabilitation. Front. Neurol. 2019, 10, 1078. [Google Scholar] [CrossRef]
- Muratore, M.; Tuena, C.; Pedroli, E.; Cipresso, P.; Riva, G. Virtual Reality as a Possible Tool for the Assessment of Self-Awareness. Front. Behav. Neurosci. 2019, 13, 62. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-Mental State Examination: A normative study in Italian elderly population. Eur. J. Neurol. 1996, 3, 198–202. [Google Scholar] [CrossRef]
- Tuena, C.; Serino, S.; Pedroli, E.; Cipresso, P.; Stramba-Badiale, M.; Riva, G.; Repetto, C. ANTaging: A Research Protocol for Active Navigation Training with Virtual Reality in Mild Cognitive Impairment. Annu. Rev. CyberTherapy Telemed. 2022, 20, 115–119. [Google Scholar]
- Brooke, J. SUS: A ‘Quick and Dirty’ Usability Scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, A.L., Eds.; Taylor and Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Lessiter, J.; Freeman, J.; Keogh, E.; Davidoff, J. A Cross-Media Presence Questionnaire: The ITC-Sense of Presence Inventory. Presence Teleoperators Virtual Environ. 2001, 10, 282–297. [Google Scholar] [CrossRef]
- Lewis, C. Using the “thinking Aloud” Method in Cognitive Interface Design. In Proceedings of the IBM Research Report, RC-9265; TJ Watson Research Center: Yorktown Heights, NY, USA, 1982. [Google Scholar]
- Riva, G.; Castelnuovo, G.; Mantovani, F. Transformation of flow in rehabilitation: The role of advanced communication technologies. Behav. Res. Methods 2006, 38, 237–244. [Google Scholar] [CrossRef]
- Pedroli, E.; Greci, L.; Colombo, D.; Serino, S.; Cipresso, P.; Arlati, S.; Mondellini, M.; Boilini, L.; Giussani, V.; Goulene, K.; et al. Characteristics, Usability, and Users Experience of a System Combining Cognitive and Physical Therapy in a Virtual Environment: Positive Bike. Sensors 2018, 18, 2343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Item | Scores |
|---|---|
| PC experience | |
| None (N) | 3 |
| Sufficient (N) | 3 |
| Good (N) | 1 |
| Great (N) | 1 |
| VG experience | |
| Never (N) | 7 |
| Occasionally (N) | 1 |
| Often (less than 50% of the days) (N) | 0 |
| More than 50% of the days (N) | 0 |
| Everyday (N) | 0 |
| VR experience | |
| Yes (N) | 3 |
| No (N) | 5 |
| VR knowledge | |
| None (N) | 5 |
| Sufficient (N) | 2 |
| Good (N) | 1 |
| Great (N) | 0 |
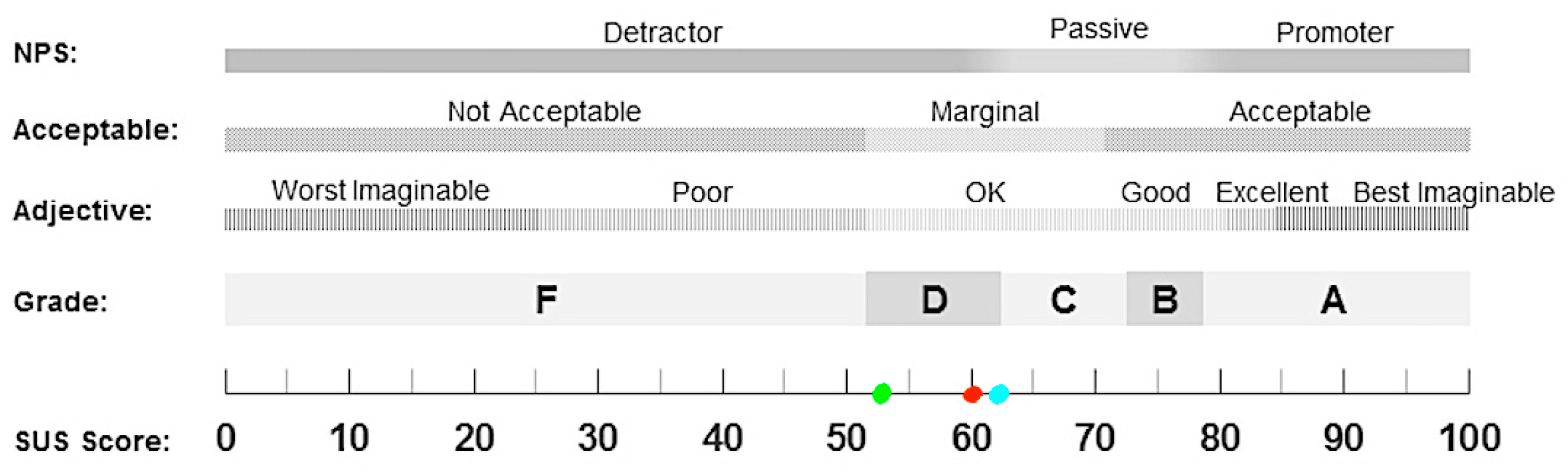
| SUS | 60 (SD = 15.05) |
| Females | 53.75 (SD = 8.75) |
| Males | 62.08 (SD = 16.10) |
| Cybersickness (ITC-SOPI) | 1.23 (SD = 0.31) |
| Spatial presence (ITC-SOPI) | 2.93 (SD = 0.75) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuena, C.; Serino, S.; Stramba-Badiale, C.; Pedroli, E.; Goulene, K.M.; Stramba-Badiale, M.; Riva, G. Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment. J. Clin. Med. 2023, 12, 1949. https://doi.org/10.3390/jcm12051949
Tuena C, Serino S, Stramba-Badiale C, Pedroli E, Goulene KM, Stramba-Badiale M, Riva G. Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment. Journal of Clinical Medicine. 2023; 12(5):1949. https://doi.org/10.3390/jcm12051949
Chicago/Turabian StyleTuena, Cosimo, Silvia Serino, Chiara Stramba-Badiale, Elisa Pedroli, Karine Marie Goulene, Marco Stramba-Badiale, and Giuseppe Riva. 2023. "Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment" Journal of Clinical Medicine 12, no. 5: 1949. https://doi.org/10.3390/jcm12051949
APA StyleTuena, C., Serino, S., Stramba-Badiale, C., Pedroli, E., Goulene, K. M., Stramba-Badiale, M., & Riva, G. (2023). Usability of an Embodied CAVE System for Spatial Navigation Training in Mild Cognitive Impairment. Journal of Clinical Medicine, 12(5), 1949. https://doi.org/10.3390/jcm12051949