
Second Generation Long-Acting Injectable Antipsychotics in Schizophrenia: The Patient’s Subjective Quality of Life, Well-Being, and Satisfaction

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
- the constraints of rapid review methods (e.g., limited search) will provide sufficient information and be credible for end-users;
- the review has a narrow, well-defined scope (e.g., limited population, specific kind of drugs);
- the amount of evidence on the chosen topic is small;
- the evidence to summarize is limited in terms of years of interest;
- the outcome is relevant to clinicians and patients.
2.1. Setting the Research Question and Eligibility Criteria
2.2. Search Terms and Electronic Searches
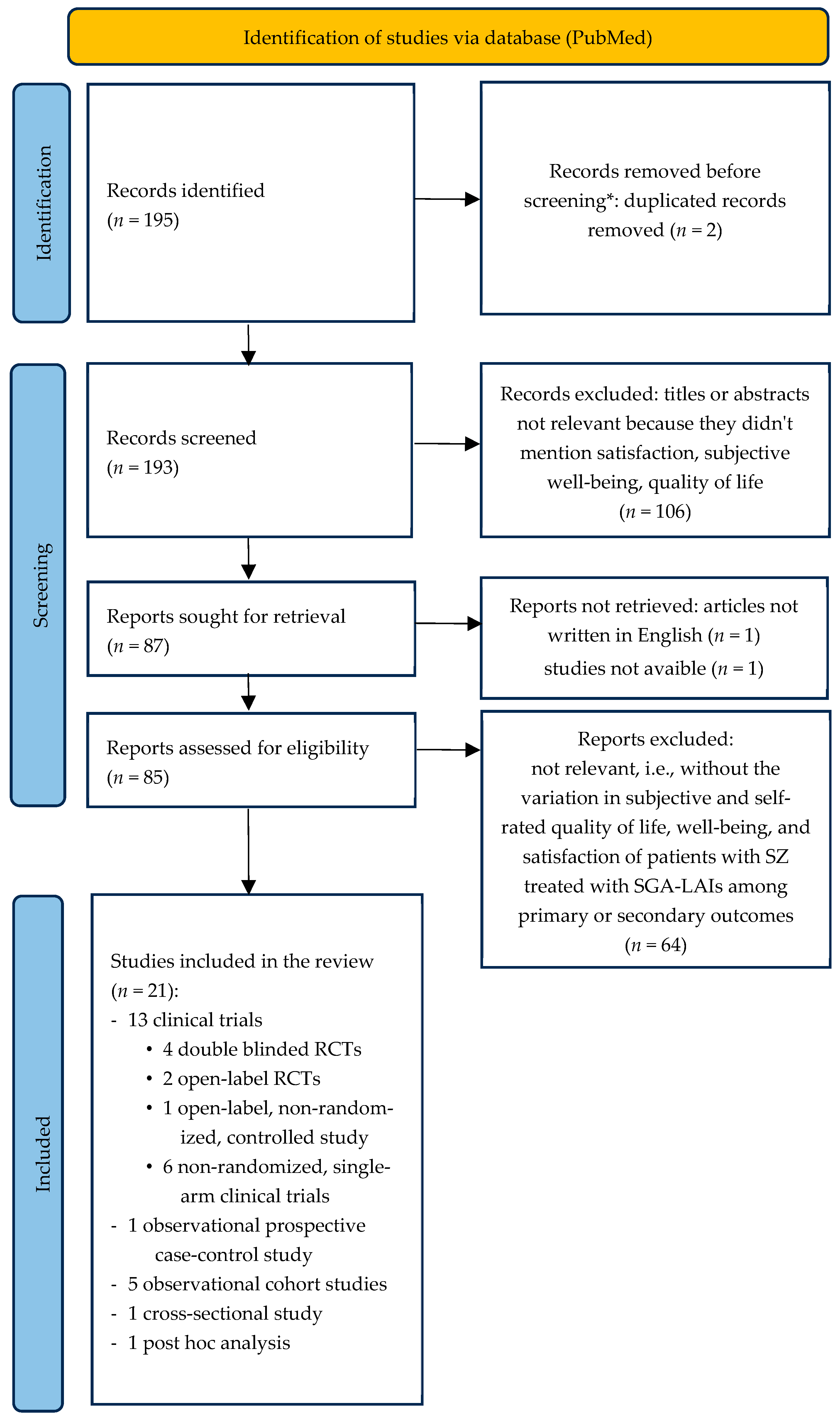
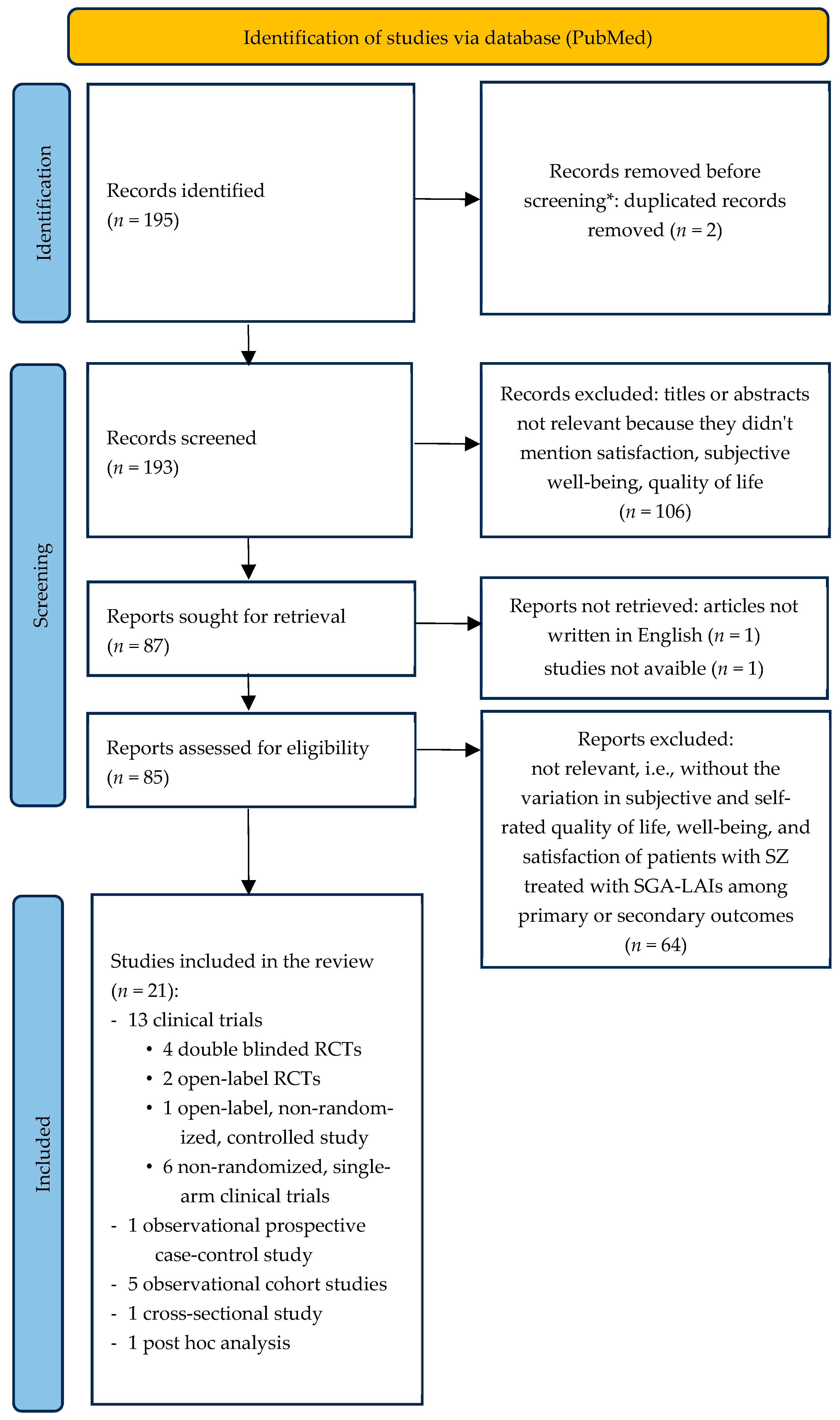
2.3. Screening and Selection Process
2.4. Data Extraction
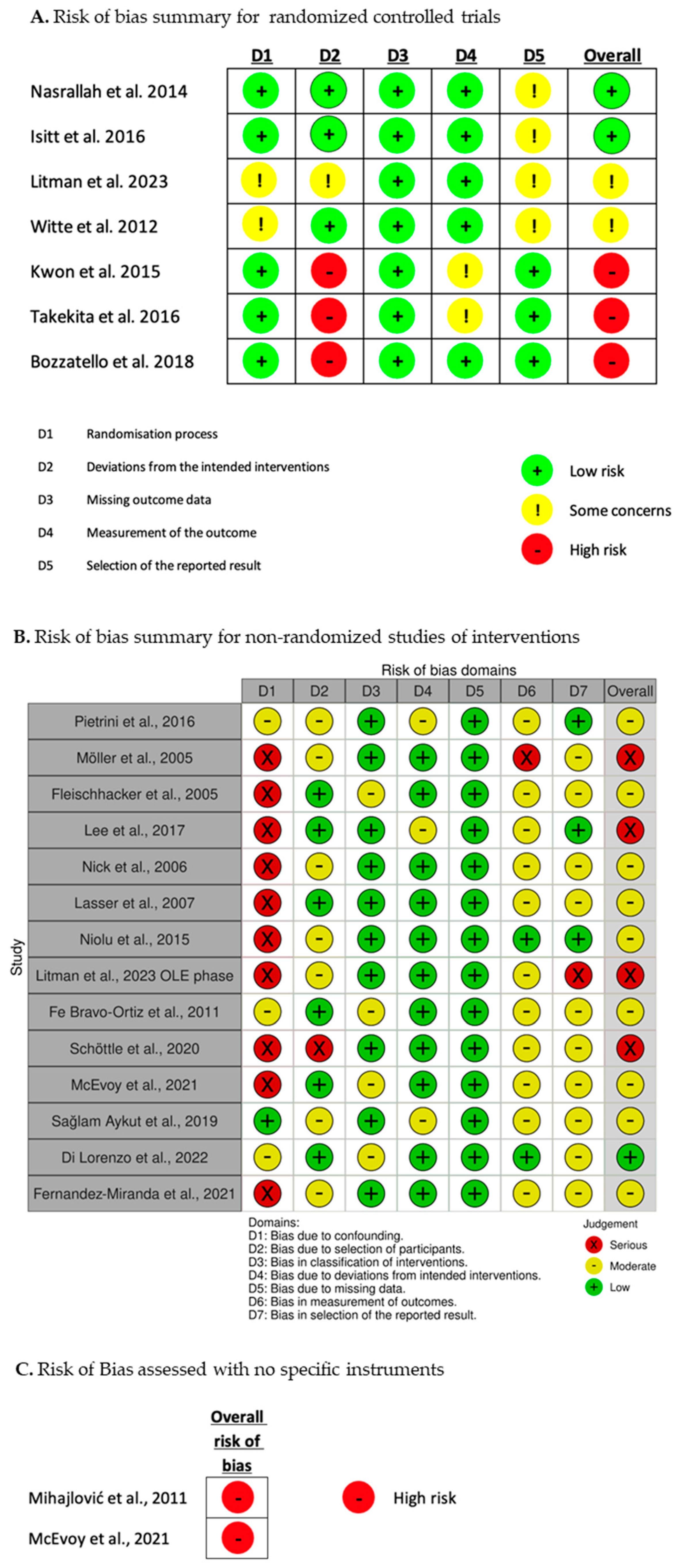
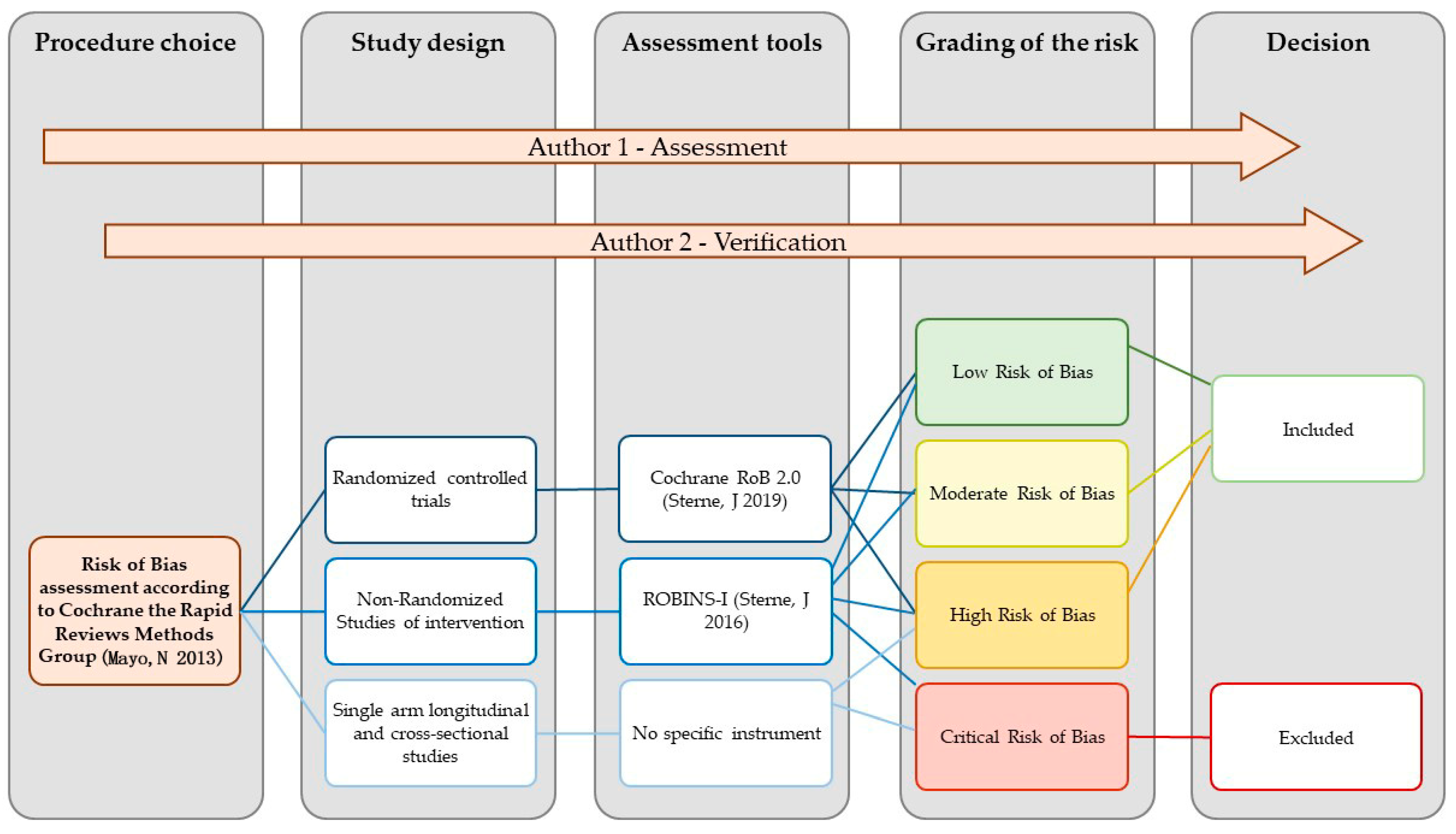
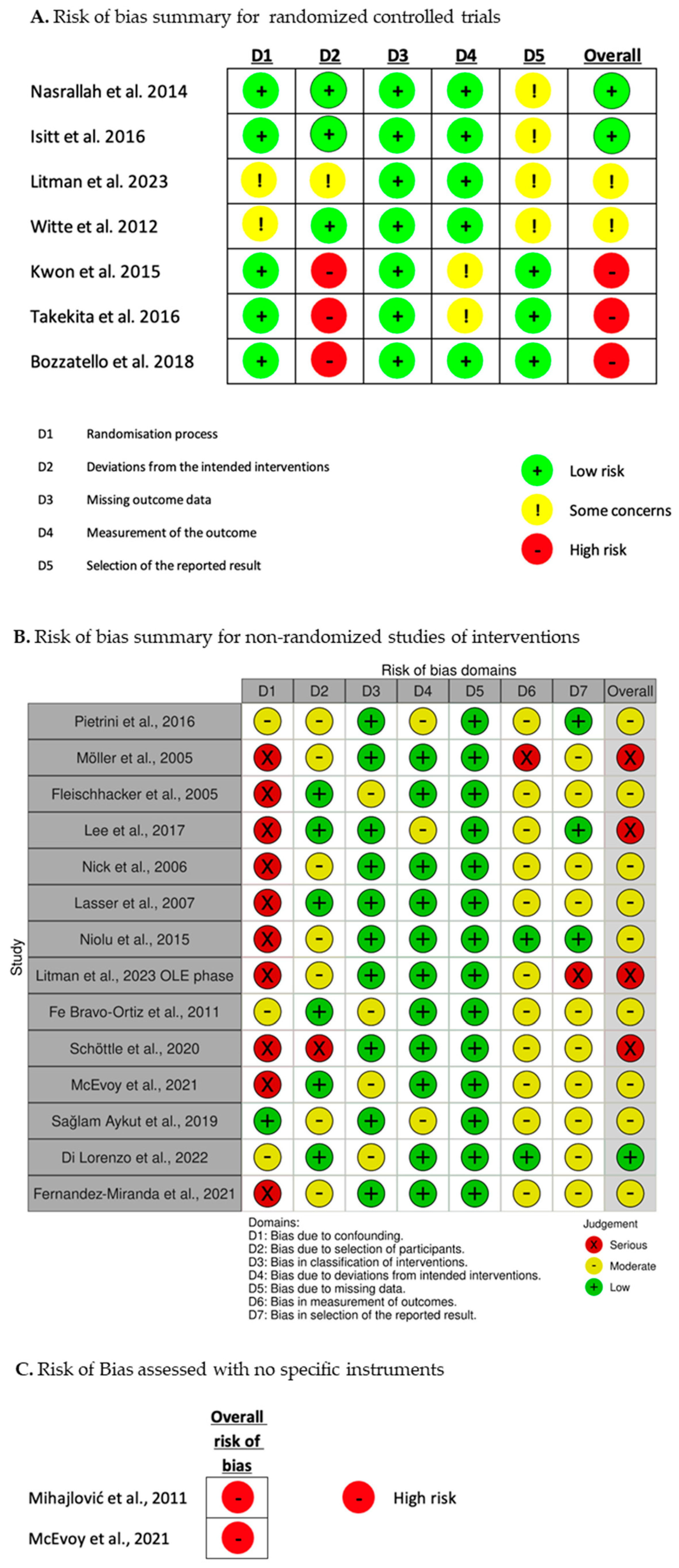
2.5. Risk of Bias Assessment
2.6. Synthesis and Discussion
3. Results
3.1. Scales for the Assessment of General and Health-Related Quality of Life
3.1.1. The World Health Organization Quality of Life Assessment Brief Form—WHOQoL-BREF
3.1.2. 36-Item Short Form Health Survey Questionnaire—SF-36
3.1.3. EuroQoL—EQ
3.1.4. Schizophrenia Quality of Life Scale—S-QoL
3.2. Scale for the Assessment of Well-Being
3.2.1. The WHO-5 Well-Being Index (WHO-5)
3.2.2. The Short form of the Subjective Well-Being under Neuroleptics Scale—SWNS
3.3. Scales for the Assessment of Satisfaction with Life and Medication
3.3.1. Satisfaction With Life Scale—SWLS
3.3.2. Treatment Satisfaction Questionnaire for Medication—TSQM
3.4. LAIs Versus Oral Antipsychotics in an Observational Case-Control Study
3.5. Risperidone Long-Acting Injectable (RLAI)
3.5.1. RLAI in Single-Arm Studies
3.5.2. Risperidone LAI vs. Placebo in Double-Blind, Randomized, Clinical Trials
3.5.3. Risperidone LAI vs. Other Antipsychotics in Observational Studies
3.6. Olanzapine LAI (OLAI)
Olanzapine LAI vs. Placebo in a Double-Blind, Randomized, Clinical Trial
3.7. Aripiprazole LAI Once a Month (AOM)
Aripiprazole LAI Once a Month in Single-Arm Studies
3.8. Paliperidone Palmitate LAI (PP)
3.8.1. Paliperidone LAI vs. Other Antipsychotics
Paliperidone LAI vs. Other Antipsychotics in Open-Label, Randomized Clinical Trials
Paliperidone LAI vs. Other Antipsychotics in Observational Studies
3.8.2. Paliperidone LAI vs. Oral Paliperidone in an Open-Label, Randomized Clinical Trial
3.8.3. PP3M vs. PP1M in an Observational Study
4. Discussion
4.1. Synthesis of the Reviewed Studies
4.2. Methodological Concerns about the Included Studies
4.2.1. Methodological Concerns Related to the Sample Selection
4.2.2. Methodological Concerns Related to the Study Design
4.2.3. Methodological Concerns Related to the Low Number of Studies for Each SGA-LAI
4.2.4. Methodological Concerns Related to the Outcome Measures
4.2.5. Possible Methodological Solutions for Further Studies on This Topic
4.3. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leucht, S.; Schneider-Thoma, J.; Burschinski, A.; Peter, N.; Wang, D.; Dong, S.; Huhn, M.; Nikolakopoulou, A.; Salanti, G.; Davis, J.M. Long-term Efficacy of Antipsychotic Drugs in Initially Acutely Ill Adults with Schizophrenia: Systematic Review and Network Meta-analysis. World Psychiatry 2023, 22, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Thompson-Leduc, P.; Ghelerter, I.; Nguyen, H.; Lafeuille, M.-H.; Benson, C.; Mavros, P.; Lefebvre, P. Real-World Evidence of the Clinical and Economic Impact of Long-Acting Injectable Versus Oral Antipsychotics among Patients with Schizophrenia in the United States: A Systematic Review and Meta-Analysis. CNS Drugs 2021, 35, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Fabrazzo, M.; Cipolla, S.; Camerlengo, A.; Perris, F.; Catapano, F. Second-Generation Antipsychotics’ Effectiveness and Tolerability: A Review of Real-World Studies in Patients with Schizophrenia and Related Disorders. J. Clin. Med. 2022, 11, 4530. [Google Scholar] [CrossRef] [PubMed]
- Faden, J.; Citrome, L. Schizophrenia: One Name, Many Different Manifestations. Med. Clin. N. Am. 2023, 107, 61–72. [Google Scholar] [CrossRef]
- MacEwan, J.P.; Forma, F.M.; Shafrin, J.; Hatch, A.; Lakdawalla, D.N.; Lindenmayer, J.-P. Patterns of Adherence to Oral Atypical Antipsychotics among Patients Diagnosed with Schizophrenia. J. Manag. Care Spec. Pharm. 2016, 22, 1349–1361. [Google Scholar] [CrossRef]
- Higashi, K.; Medic, G.; Littlewood, K.J.; Diez, T.; Granström, O.; De Hert, M. Medication Adherence in Schizophrenia: Factors Influencing Adherence and Consequences of Nonadherence, A Systematic Literature Review. Ther. Adv. Psychopharmacol. 2013, 3, 200–218. [Google Scholar] [CrossRef]
- Girardi, P.; Del Casale, A.; Rapinesi, C.; Kotzalidis, G.D.; Splendori, F.; Verzura, C.; Trovini, G.; Sorice, S.; Carrus, D.; Mancinelli, I.; et al. Predictive Factors of Overall Functioning Improvement in Patients with Chronic Schizophrenia and Schizoaffective Disorder Treated with Paliperidone Palmitate and Aripiprazole Monohydrate. Hum. Psychopharmacol. Clin. Exp. 2018, 33, e2658. [Google Scholar] [CrossRef]
- Kane, J.M.; McEvoy, J.P.; Correll, C.U.; Llorca, P.M. Controversies Surrounding the Use of Long-Acting Injectable Antipsychotic Medications for the Treatment of Patients with Schizophrenia. CNS Drugs 2021, 35, 1189–1205. [Google Scholar] [CrossRef]
- McCutcheon, R.A.; Keefe, R.S.E.; McGuire, P.K. Cognitive Impairment in Schizophrenia: Aetiology, Pathophysiology, and Treatment. Mol. Psychiatry 2023, 28, 1902–1918. [Google Scholar] [CrossRef]
- Okoli, C.T.C.; Kappi, A.; Wang, T.; Makowski, A.; Cooley, A.T. The Effect of Long-acting Injectable Antipsychotic Medications Compared with Oral Antipsychotic Medications among People with Schizophrenia: A Systematic Review and Meta-analysis. Int. J. Ment. Health Nurs. 2022, 31, 469–535. [Google Scholar] [CrossRef]
- Salzmann-Erikson, M.; Sjödin, M. A Narrative Meta-Synthesis of How People with Schizophrenia Experience Facilitators and Barriers in Using Antipsychotic Medication: Implications for Healthcare Professionals. Int. J. Nurs. Stud. 2018, 85, 7–18. [Google Scholar] [CrossRef]
- Velligan, D.I.; Sajatovic, M.; Hatch, A.; Kramata, P.; Docherty, J.P. Why Do Psychiatric Patients Stop Antipsychotic Medication? A Systematic Review of Reasons for Nonadherence to Medication in Patients with Serious Mental Illness. Patient Prefer. Adherence 2017, 11, 449–468. [Google Scholar] [CrossRef] [PubMed]
- Li, I.H.; Hsieh, W.L.; Liu, W.I. A Systematic Review and Meta-Analysis of the Effectiveness of Adherence Therapy and Its Treatment Duration in Patients with Schizophrenia Spectrum Disorders. Patient Prefer. Adherence 2023, 17, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, W.-L.; Li, I.-H.; Liu, W.-I. Effects of Empowerment-Based Illness Management on the Medication Adherence and Recovery of Persons with Schizophrenia: A Systematic Review and Meta-Analysis. Int. J. Ment. Health Nurs. 2023, 32, 1008–1024. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Mason, K. Partial Compliance with Long-Acting Paliperidone Palmitate and Impact on Hospitalization: A 6-Year Mirror-Image Study. Ther. Adv. Psychopharmacol. 2020, 10, 204512532092478. [Google Scholar] [CrossRef]
- Faden, J.; Citrome, L. How Would You Like to Take Your Medicine 2 Times a Year? Paliperidone Palmitate Every 6 Months for the Maintenance Treatment of Schizophrenia. Clin. Ther. 2022, 44, 476–479. [Google Scholar] [CrossRef]
- Stevens, G.L.; Dawson, G.; Zummo, J. Clinical Benefits and Impact of Early Use of Long-acting Injectable Antipsychotics for Schizophrenia. Early Interv. Psychiatry 2016, 10, 365–377. [Google Scholar] [CrossRef]
- Winter-van Rossum, I.; Weiser, M.; Galderisi, S.; Leucht, S.; Bitter, I.; Glenthøj, B.; Hasan, A.; Luykx, J.; Kupchik, M.; Psota, G.; et al. Efficacy of Oral versus Long-Acting Antipsychotic Treatment in Patients with Early-Phase Schizophrenia in Europe and Israel: A Large-Scale, Open-Label, Randomised Trial (EULAST). Lancet Psychiatry 2023, 10, 197–208. [Google Scholar] [CrossRef]
- Hahn, M.; Roll, S.C. The Relevance of Long-Acting Injectables in the Treatment of Schizophrenia. Lancet Psychiatry 2023, 10, 159–160. [Google Scholar] [CrossRef]
- Haddad, P.M.; Correll, C.U. Long-Acting Antipsychotics in the Treatment of Schizophrenia: Opportunities and Challenges. Expert. Opin. Pharmacother. 2023, 24, 473–493. [Google Scholar] [CrossRef]
- Keepers, G.A.; Fochtmann, L.J.; Anzia, J.M.; Benjamin, S.; Lyness, J.M.; Mojtabai, R.; Servis, M.; Walaszek, A.; Buckley, P.; Lenzenweger, M.F.; et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia. Am. J. Psychiatry 2020, 177, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Price, M.Z.; Price, R.L. The Use of Long-Acting Injectables in Early-Phase Schizophrenia. Lancet Psychiatry 2023, 10, 480. [Google Scholar] [CrossRef] [PubMed]
- Tiihonen, J. The Use of Long-Acting Injectables in Early-Phase Schizophrenia. Lancet Psychiatry 2023, 10, 481–482. [Google Scholar] [CrossRef]
- Lian, L.; Kim, D.D.; Procyshyn, R.M.; Fredrikson, D.H.; Cázares, D.; Honer, W.G.; Barr, A.M. Efficacy of Long-Acting Injectable versus Oral Antipsychotic Drugs in Early Psychosis: A Systematic Review and Meta-Analysis. Early Interv. Psychiatry 2022, 16, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, S.; Wolfgang Fleischhacker, W. The Use of Long-Acting Injectable Antipsychotics in Schizophrenia. Curr. Treat. Options Psychiatry 2017, 4, 117–126. [Google Scholar] [CrossRef]
- Jann, M.W.; Penzak, S.R. Long-Acting Injectable Second-Generation Antipsychotics: An Update and Comparison between Agents. CNS Drugs 2018, 32, 241–257. [Google Scholar] [CrossRef]
- Rauch, A.S.; Fleischhacker, W.W. Long-Acting Injectable Formulations of New-Generation Antipsychotics: A Review from a Clinical Perspective. CNS Drugs 2013, 27, 637–652. [Google Scholar] [CrossRef]
- Bozzatello, P.; Bellino, S.; Mancini, I.; Sandei, L.; Zanalda, E.; Rocca, P. Effects on Satisfaction and Service Engagement of Paliperidone Palmitate Compared with Oral Paliperidone in Patients with Schizophrenia: An Open Label Randomized Controlled Trial. Clin. Drug Investig. 2019, 39, 169–178. [Google Scholar] [CrossRef]
- Pietrini, F.; Spadafora, M.; Tatini, L.; Talamba, G.A.; Andrisano, C.; Boncompagni, G.; Manetti, M.; Ricca, V.; Ballerini, A. LAI versus Oral: A Case-Control Study on Subjective Experience of Antipsychotic Maintenance Treatment. Eur. Psychiatry 2016, 37, 35–42. [Google Scholar] [CrossRef]
- Haro, J.M.; Salvador-Carulla, L. The SOHO (Schizophrenia Outpatient Health Outcome) Study: Implications for the Treatment of Schizophrenia. CNS Drugs 2006, 20, 293–301. [Google Scholar] [CrossRef]
- Barbui, C.; Kikkert, M.; Mazzi, M.A.; Becker, T.; Bindman, J.; Schene, A.; Nosè, M.; Helm, H.; Thornicroft, G.; Tansella, M. Comparison of Patient and Clinician Perspectives in the Assessment of Antipsychotic Medication Adherence. Psychopathology 2009, 42, 311–317. [Google Scholar] [CrossRef]
- Mohamed, S.; Rosenheck, R.; McEvoy, J.; Swartz, M.; Stroup, S.; Lieberman, J.A. Cross-Sectional and Longitudinal Relationships between Insight and Attitudes toward Medication and Clinical Outcomes in Chronic Schizophrenia. Schizophr. Bull. 2009, 35, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Skar-Fröding, R.; Clausen, H.K.; Šaltytė Benth, J.; Ruud, T.; Slade, M.; Sverdvik Heiervang, K. Relationship between Satisfaction with Mental Health Services, Personal Recovery and Quality of Life among Service Users with Psychosis: A Cross-Sectional Study. BMC Health Serv. Res. 2021, 21, 439. [Google Scholar] [CrossRef]
- Gharabawi, G.M.; Greenspan, A.; Rupnow, M.F.T.; Kosik-Gonzalez, C.; Bossie, C.A.; Zhu, Y.; Kalali, A.H.; Awad, A.G. Reduction in Psychotic Symptoms as a Predictor of Patient Satisfaction with Antipsychotic Medication in Schizophrenia: Data from a Randomized Double-Blind Trial. BMC Psychiatry 2006, 6, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ram, D.; Gowdappa, B. Trust and Expectation on Psychiatrist and Its Correlation with Satisfaction and Adherence in Patients with Mental Illness. Arch. Clin. Psychiatry 2015, 42, 13–17. [Google Scholar] [CrossRef]
- Whoqol Group. The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 Health Survey Questionnaire: New Outcome Measure for Primary Care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef]
- Dong, M.; Lu, L.; Zhang, L.; Zhang, Y.-S.; Ng, C.H.; Ungvari, G.S.; Li, G.; Meng, X.; Wang, G.; Xiang, Y.-T. Quality of Life in Schizophrenia: A Meta-Analysis of Comparative Studies. Psychiatr. Q. 2019, 90, 519–532. [Google Scholar] [CrossRef]
- Alptekin, K.; Akvardar, Y.; Akdede, B.B.K.; Dumlu, K.; Işık, D.; Pirinçci, F.; Yahssin, S.; Kitiş, A. Is Quality of Life Associated with Cognitive Impairment in Schizophrenia? Prog. Neuropsychopharmacol. Biol. Psychiatry 2005, 29, 239–244. [Google Scholar] [CrossRef]
- Rosenheck, R.; Leslie, D.; Keefe, R.; McEvoy, J.; Swartz, M.; Perkins, D.; Stroup, S.; Hsiao, J.K.; Lieberman, J. Barriers to Employment for People with Schizophrenia. Am. J. Psychiatry 2006, 163, 411–417. [Google Scholar] [CrossRef]
- Sibitz, I.; Amering, M.; Unger, A.; Seyringer, M.E.; Bachmann, A.; Schrank, B.; Benesch, T.; Schulze, B.; Woppmann, A. The Impact of the Social Network, Stigma and Empowerment on the Quality of Life in Patients with Schizophrenia. Eur. Psychiatry 2011, 26, 28–33. [Google Scholar] [CrossRef]
- Stubbs, B.; Firth, J.; Berry, A.; Schuch, F.B.; Rosenbaum, S.; Gaughran, F.; Veronesse, N.; Williams, J.; Craig, T.; Yung, A.R.; et al. How Much Physical Activity Do People with Schizophrenia Engage in? A Systematic Review, Comparative Meta-Analysis and Meta-Regression. Schizophr. Res. 2016, 176, 431–440. [Google Scholar] [CrossRef]
- Awad, A.G.; Voruganti, L.N. Quality of Life and New Antipsychotics in Schizophrenia. Are Patients Better Off? Int. J. Soc. Psychiatry 1999, 45, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Alptekin, K.; Akdede, B.B.; Akvardar, Y.; Çelikgün, S.; Dilşen, N.S.; Durak, G.; Türk, A.; Fidaner, H. Quality of Life Assessment in Turkish Patients with Schizophrenia and Their Relatives. Psychol. Rep. 2004, 95, 197–206. [Google Scholar] [CrossRef] [PubMed]
- DE Hert, M.; Schreurs, V.; Vancampfort, D.; Van Winkel, R. Metabolic Syndrome in People with Schizophrenia: A Review. World Psychiatry 2009, 8, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Kim-Prieto, C.; Diener, E.; Tamir, M.; Scollon, C.; Diener, M. Integrating the Diverse Definitions of Happiness: A Time-Sequential Framework of Subjective Well-Being. J. Happiness Stud. 2005, 6, 261–300. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective Well-Being: Three Decades of Progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Aunjitsakul, W.; Teetharatkul, T.; Vitayanont, A.; Liabsuetrakul, T. Does the Psychiatrist’s Use of Subjective Well-Being Measurement in People with Schizophrenia Provide a Better Alignment with the Patient’s Well-Being Perception than Clinical Judgement Alone? Adm. Policy Ment. Health Ment. Health Serv. Res. 2021, 48, 768–779. [Google Scholar] [CrossRef]
- Vothknecht, S.; Schoevers, R.A.; de Haan, L. Subjective Well-Being in Schizophrenia as Measured with the Subjective Well-Being under Neuroleptic Treatment Scale: A Review. Aust. N. Z. J. Psychiatry 2011, 45, 182–192. [Google Scholar] [CrossRef]
- He, Y.; Tanaka, A.; Kishi, T.; Li, Y.; Matsunaga, M.; Tanihara, S.; Iwata, N.; Ota, A. Recent Findings on Subjective Well-Being and Physical, Psychiatric, and Social Comorbidities in Individuals with Schizophrenia: A Literature Review. Neuropsychopharmacol. Rep. 2022, 42, 430–436. [Google Scholar] [CrossRef]
- Citrome, L.; Mychaskiw, M.A.; Cortez, A.; Opler, M.; Sopina, L.; Kotak, S. Clinical Outcome Assessment Instruments in Schizophrenia: A Scoping Literature Review with a Focus on the Potential of Patient-Reported Outcomes. Innov. Clin. Neurosci. 2023, 20, 14–33. [Google Scholar]
- Ponce-Correa, F.; Caqueo-Urízar, A.; Berrios, R.; Escobar-Soler, C. Defining Recovery in Schizophrenia: A Review of Outcome Studies. Psychiatry Res. 2023, 322, 115134. [Google Scholar] [CrossRef] [PubMed]
- Vita, A.; Barlati, S. Recovery from Schizophrenia. Curr. Opin. Psychiatry 2018, 31, 246–255. [Google Scholar] [CrossRef]
- Van Eck, R.M.; Burger, T.J.; Vellinga, A.; Schirmbeck, F.; de Haan, L. The Relationship between Clinical and Personal Recovery in Patients with Schizophrenia Spectrum Disorders: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2018, 44, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Gründer, G.; Heinze, M.; Cordes, J.; Mühlbauer, B.; Juckel, G.; Schulz, C.; Rüther, E.; Timm, J. Effects of First-Generation Antipsychotics versus Second-Generation Antipsychotics on Quality of Life in Schizophrenia: A Double-Blind, Randomised Study. Lancet Psychiatry 2016, 3, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Rocca, P.; Montemagni, C.; Frieri, T. Second-Generation Long-Acting Injectable Antipsychotics in Schizophrenia: Patient Functioning and Quality of Life. Neuropsychiatr. Dis. Treat. 2016, 12, 917–929. [Google Scholar] [CrossRef]
- Kisely, S.; Sawyer, E.; Robinson, G.; Siskind, D. A Systematic Review and Meta-Analysis of the Effect of Depot Antipsychotic Frequency on Compliance and Outcome. Schizophr. Res. 2015, 166, 178–186. [Google Scholar] [CrossRef]
- Swainston Harrison, T.; Goa, K.L.; Beauclair, L. Long-Acting Risperidone A Review of Its Use in Schizophrenia. CNS Drugs 2004, 18, 113–132. [Google Scholar] [CrossRef]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group Offers Evidence-Informed Guidance to Conduct Rapid Reviews. J. Clin. Epidemiol. 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Hamel, C.; Michaud, A.; Thuku, M.; Skidmore, B.; Stevens, A.; Nussbaumer-Streit, B.; Garritty, C. Defining Rapid Reviews: A Systematic Scoping Review and Thematic Analysis of Definitions and Defining Characteristics of Rapid Reviews. J. Clin. Epidemiol. 2021, 129, 74–85. [Google Scholar] [CrossRef]
- Featherstone, R.M.; Dryden, D.M.; Foisy, M.; Guise, J.-M.; Mitchell, M.D.; Paynter, R.A.; Robinson, K.A.; Umscheid, C.A.; Hartling, L. Advancing Knowledge of Rapid Reviews: An Analysis of Results, Conclusions and Recommendations from Published Review Articles Examining Rapid Reviews. Syst. Rev. 2015, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Guise, J.-M.; Hempel, S.; Featherstone, R.; Mitchell, M.D.; Motu’apuaka, M.L.; Robinson, K.A.; Schoelles, K.; Totten, A.; Whitlock, E.; et al. Fit for Purpose: Perspectives on Rapid Reviews from End-User Interviews. Syst. Rev. 2017, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Plüddemann, A.; Aronson, J.K.; Onakpoya, I.; Heneghan, C.; Mahtani, K.R. Redefining Rapid Reviews: A Flexible Framework for Restricted Systematic Reviews. BMJ Evid. Based Med. 2018, 23, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Mayo, N.; Asano, M.; Barbic, S. When Is a Research Question Not a Research Question? J. Rehabil. Med. 2013, 45, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, P.; Petrisor, B.A.; Farrokhyar, F.; Bhandari, M. Practical Tips for Surgical Research: Research Questions, Hypotheses and Objectives. Can. J. Surg. 2010, 53, 278–281. [Google Scholar]
- Durbin, C.G. How to Come Up with a Good Research Question: Framing the Hypothesis Introduction the Research Process Devising and Improving a Hypothesis an Example of Moving from a Broad Hypothesis to a Manageable Research Question Determining What Type of Controls to Use Deciding Exactly What Data to Collect Novice Researchers Should Find and Use a Research Mentor. Respir. Care 2004, 49, 1195–1198. [Google Scholar]
- Thabane, L.; Thomas, T.; Ye, C.; Paul, J. Posing the Research Question: Not so Simple. Can. J. Anesth./J. Can. D’anesthésie 2009, 56, 71–79. [Google Scholar] [CrossRef]
- Rios, L.P.; Ye, C.; Thabane, L. Association between Framing of the Research Question Using the PICOT Format and Reporting Quality of Randomized Controlled Trials. BMC Med. Res. Methodol. 2010, 10, 11. [Google Scholar] [CrossRef]
- Fandino, W. Formulating a Good Research Question: Pearls and Pitfalls. Indian J. Anaesth. 2019, 63, 611. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Sommer, I.; Hamel, C.; Devane, D.; Noel-Storr, A.; Puljak, L.; Trivella, M.; Gartlehner, G. Rapid Reviews Methods Series: Guidance on Team Considerations, Study Selection, Data Extraction and Risk of Bias Assessment. BMJ Evid. Based Med. 2023, 1–6. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Möller, H.-J.; Llorca, P.-M.; Sacchetti, E.; Martin, S.D.; Medori, R.; Parellada, E.; StoRMi Study Group. Efficacy and Safety of Direct Transition to Risperidone Long-Acting Injectable in Patients Treated with Various Antipsychotic Therapies. Int. Clin. Psychopharmacol. 2005, 20, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Fleischhacker, W.W.; Rabinowitz, J.; Kemmler, G.; Eerdekens, M.; Mehnert, A. Perceived Functioning, Well-Being and Psychiatric Symptoms in Patients with Stable Schizophrenia Treated with Long-Acting Risperidone for 1 Year. Br. J. Psychiatry 2005, 187, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-S.; Ko, Y.-H.; Lee, S.-H.; Seo, Y.-J.; Kim, S.-H.; Joe, S.-H.; Han, C.-S.; Lee, J.-H.; Jung, I.-K. Long-Term Treatment with Long-Acting Risperidone in Korean Patients with Schizophrenia. Hum. Psychopharmacol. 2006, 21, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Nick, B.; Vauth, R.; Braendle, D.; Riecher-Rössler, A.; The Swiss StoRMi Investigators Group. Symptom Control, Functioning and Satisfaction among Swiss Patients Treated with Risperidone Long-Acting Injectable. Int. J. Psychiatry Clin. Pract. 2006, 10, 174–181. [Google Scholar] [CrossRef]
- Lasser, R.A.; Bossie, C.A.; Zhu, Y.; Locklear, J.C.; Kane, J.M. Long-Acting Risperidone in Young Adults with Early Schizophrenia or Schizoaffective Illness. Ann. Clin. Psychiatry 2007, 19, 65–71. [Google Scholar] [CrossRef]
- Niolu, C.; Bianciardi, E.; Di Lorenzo, G.; Marchetta, C.; Barone, Y.; Sterbini, N.; Ribolsi, M.; Reggiardo, G.; Siracusano, A. Enhancing Adherence, Subjective Well-Being and Quality of Life in Patients with Schizophrenia: Which Role for Long-Acting Risperidone? Ther. Adv. Psychopharmacol. 2015, 5, 278–288. [Google Scholar] [CrossRef]
- Nasrallah, H.A.; Duchesne, I.; Mehnert, A.; Janagap, C.; Eerdekens, M. Health-Related Quality of Life in Patients with Schizophrenia during Treatment with Long-Acting, Injectable Risperidone. J. Clin. Psychiatry 2004, 65, 531–536. [Google Scholar] [CrossRef]
- Isitt, J.J.; Nadipelli, V.R.; Kouassi, A.; Fava, M.; Heidbreder, C. Health-Related Quality of Life in Acute Schizophrenia Patients Treated with RBP-7000 Once Monthly Risperidone: An 8-Week, Randomized, Double-Blind, Placebo-Controlled, Multicenter Phase 3 Study. Schizophr. Res. 2016, 174, 126–131. [Google Scholar] [CrossRef]
- Litman, R.; Naber, D.; Anta, L.; Martínez, J.; Filts, Y.; Correll, C.U. Personal and Social Functioning and Health-Related Quality of Life in Patients with Schizophrenia Treated with the Long-Acting Injectable Antipsychotic Risperidone ISM. Neuropsychiatr. Dis. Treat. 2023, 19, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Mihajlović, G.; Jovanović-Mihajlović, N.; Radmanović, B.; Radonjić, K.; Djukić-Dejanović, S.; Janković, S.; Janjić, V.; Milovanović, N.; Petrović, D.; Tomić, K. Quality of Life of Schizophrenic Patients Treated with Haloperidol Depot and Injection Preparation of Long-Lasting Risperidone. Srp. Arh. Celok. Lek. 2011, 139 (Suppl. S1), 36–40. [Google Scholar] [CrossRef] [PubMed]
- Fe Bravo-Ortiz, M.; Gutiérrez-Casares, J.R.; Rodríguez-Morales, A.; García, M.A.P.; Hidalgo-Borrajo, R. Influence of Type of Treatment on the Well-Being of Spanish Patients with Schizophrenia and Their Caregivers. Int. J. Psychiatry Clin. Pract. 2011, 15, 286–295. [Google Scholar] [CrossRef]
- Witte, M.M.; Case, M.G.; Schuh, K.J.; Ascher-Svanum, H. Effects of Olanzapine Long-Acting Injection on Levels of Functioning among Acutely Ill Patients with Schizophrenia. Curr. Med. Res. Opin. 2012, 28, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Schöttle, D.; Janetzky, W.; Luedecke, D.; Beck, E.; Correll, C.U.; Wiedemann, K. The Use of Long-Acting Aripiprazole in a Multi-Center, Prospective, Uncontrolled, Open-Label, Cohort Study in Germany: A Report on Global Assessment of Functioning and the WHO Wellbeing Index. BMC Psychiatry 2020, 20, 77. [Google Scholar] [CrossRef]
- McEvoy, J.P.; Weiden, P.J.; Lysaker, P.H.; Sun, X.; O’Sullivan, A.K. Long-Term Effect of Aripiprazole Lauroxil on Health-Related Quality of Life in Patients with Schizophrenia. BMC Psychiatry 2021, 21, 164. [Google Scholar] [CrossRef]
- Kwon, J.S.; Kim, S.N.; Han, J.; Lee, S.I.; Chang, J.S.; Choi, J.-S.; Lee, H.-J.; Cho, S.J.; Jun, T.-Y.; Lee, S.-H.; et al. Satisfaction of Immediate or Delayed Switch to Paliperidone Palmitate in Patients Unsatisfied with Current Oral Atypical Antipsychotics. Int. Clin. Psychopharmacol. 2015, 30, 320–328. [Google Scholar] [CrossRef]
- Takekita, Y.; Koshikawa, Y.; Fabbri, C.; Sakai, S.; Sunada, N.; Onohara, A.; Nishida, K.; Yoshimura, M.; Kato, M.; Serretti, A.; et al. Cognitive Function and Risperidone Long-Acting Injection vs. Paliperidone Palmitate in Schizophrenia: A 6-Month, Open-Label, Randomized, Pilot Trial. BMC Psychiatry 2016, 16, 172. [Google Scholar] [CrossRef]
- Sağlam Aykut, D. Comparison of Paliperidone Palmitate and Second-Generation Oral Antipsychotics in Terms of Medication Adherence, Side Effects, and Quality of Life. J. Clin. Psychopharmacol. 2019, 39, 57–62. [Google Scholar] [CrossRef]
- Di Lorenzo, R.; Iorio, A.; Pinelli, M.; Magarini, F.; Marchi, M.; Sacchetti, A.; Calogero, C.; Galeazzi, G.M.; Ferri, P.; Rovesti, S.; et al. Effectiveness and Quality of Life with Paliperidone Palmitate 3-Monthly in Comparison with Other Long-Acting Drugs. Neuropsychiatr. Dis. Treat. 2022, 18, 829–846. [Google Scholar] [CrossRef]
- Fernández-Miranda, J.J.; Díaz-Fernández, S.; De Berardis, D.; López-Muñoz, F. Paliperidone Palmitate Every Three Months (PP3M) 2-Year Treatment Compliance, Effectiveness and Satisfaction Compared with Paliperidone Palmitate-Monthly (PP1M) in People with Severe Schizophrenia. J. Clin. Med. 2021, 10, 1408. [Google Scholar] [CrossRef]
- Group, W. Development of the WHOQOL: Rationale and Current Status. Int. J. Ment. Health 1994, 23, 24–56. [Google Scholar] [CrossRef]
- WHOQoL Group. The Development of the World Health Organization Quality of Life Assessment Instrument (the WHOQOL). In Proceedings of the Quality of Life Assessment: International Perspectives: Proceedings of the Joint-Meeting Organized by the World Health Organization and the Fondation IPSEN, Paris, France, 2–3 July 1993; Springer: Berlin/Heidelberg, Germany, 1994; pp. 41–57. [Google Scholar]
- The WHOQoL Group. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. SF-36 Health Survey. Manual and Interpretation Guide; The Health Institute: Boston, MA, USA, 1993; pp. 1–6. [Google Scholar]
- Prieto, L.; Sacristán, J.A.; Hormaechea, J.A.; Casado, A.; Badia, X.; Gómez, J.C. Psychometric Validation of a Generic Health-Related Quality of Life Measure (EQ-5D) in a Sample of Schizophrenic Patients. Curr. Med. Res. Opin. 2004, 20, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Auquier, P.; Simeoni, M.C.; Sapin, C.; Reine, G.; Aghababian, V.; Cramer, J.; Lançon, C. Development and Validation of a Patient-Based Health-Related Quality of Life Questionnaire in Schizophrenia: The S-QoL. Schizophr. Res. 2003, 63, 137–149. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Naber, D. A Self-Rating to Measure Subjective Effects of Neuroleptic Drugs, Relationships to Objective Psychopathology, Quality of Life, Compliance and Other Clinical Variables. Int. Clin. Psychopharmacol. 1995, 10, 133–138. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Atkinson, M.J.; Sinha, A.; Hass, S.L.; Colman, S.S.; Kumar, R.N.; Brod, M.; Rowland, C.R. Validation of a General Measure of Treatment Satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), Using a National Panel Study of Chronic Disease. Health Qual. Life Outcomes 2004, 2, 12. [Google Scholar] [CrossRef]
- Vernon, M.K.; Revicki, D.A.; Awad, A.G.; Dirani, R.; Panish, J.; Canuso, C.M.; Grinspan, A.; Mannix, S.; Kalali, A.H. Psychometric Evaluation of the Medication Satisfaction Questionnaire (MSQ) to Assess Satisfaction with Antipsychotic Medication among Schizophrenia Patients. Schizophr. Res. 2010, 118, 271–278. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Acronym | Extended Name | Items Number | Subscales, Components, Items | Single Item Scoring |
|---|---|---|---|---|
| WHOQoL-BREF WHOQOL group, 1998 [94] | World Health Organization Quality of Life Assessment Brief Form | 24 | Subscales: physical health (PH; 7 items); psychological well-being (PS; 6 items); social relationships (SR; 3 items); environment health (EH; 8 items) | 1 to 5 |
| SF-36 Ware et al., 1993 [95] | 36-Item Short Form Health Survey questionnaire | 36 | Subscales: physical functioning (PF); physical role (RP); bodily pain (BP); general health (GH); vitality (VT); social functioning (SF); emotional role (RE); mental health (MH) Components: physical component summary (PCS); mental component summary (MCS) | Depending on the item |
| EQ Kind, 1996 [96] | EuroQoL | 5 | EQ 5 dimensions (EQ-5D): mobility, self-care, usual activities, pain/discomfort, and anxiety/depression; EQ visual analog scale (EQ-VAS); EQ Index (EQ-I) | 1 to 3 |
| S-QoL Auquier et al., 2003 [97] | Schizophrenia Quality of Life Scale | 41 | Subscales: psychological well-being, self-esteem, family relationships, relationship with friends, resilience, physical well-being, autonomy, and sentimental life | 1 to 5 |
| WHO-5 Topp et al., 2015 [98] | WHO-5 Well-Being Index | 5 | Five positive questions about the time spent in a state of psychological well-being | 0 to 5 |
| SWNS Naber et al., 1995 [99] | Short Form of the Subjective Well-Being under Neuroleptics Scale | 20 | Emotional Regulation (ER); Mental Functioning (MF); Physical Functioning (PF); Self-Control (SC); Social Integration (SI) | 1 to 6 |
| SWLS Diener et al., 1985 [100] | Satisfaction With Life Scale | 5 | Items: in most ways, my life is close to my ideal; the conditions of my life are excellent; I am satisfied with my life; so far, I have gotten the important things I want in life; if I could live my life over, I would change almost nothing | 1 to 7 |
| TSQM Atkinson et al., 2004 [101] | Treatment Satisfaction Questionnaire for Medication | 12 | Subscales: effectiveness; side effects; convenience; global satisfaction | 1 to 5 |
| Study | Study Design | Drugs | Comparator Group(s) | Sample Size | Age | Sample Characteristics | Diagnosis | Assessment of QoL/SWB/Sat | Outcome | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Change in QoL/SWB/Sat | Effect | ||||||||||
| Pietrini et al., 2016 [29] | Observational case–control longitudinal study | LAI group (OLA 300–405 mg/month and PP 100–150 mg/month) | Oral group (OLA 10–15 mg/d or PAL 9–12 mg/d) | 40 | LAI group: 40.55 (11.00) Oral group: 45.10 (10.68) | Patients in full remission, treated with a single antipsychotic (olanzapine or paliperidone) for over 4 weeks, eligible for a switch to the equivalent LAI maintenance regimen of the same antipsychotic. | SZ | SWNS, SF-36 | Primary Outcome: change in SWNS and SF-36 at month 6 | ↑ vs. oral group in single domains of SF-36 and SWNS | LAI group vs. oral group: SWNS significant improvement in single domains: ER p < 0.05 SC, PF, SI p < 0.01 MF p < 0.001 LAI group vs. baseline: SF-36 significant improvement in single domains: RF p < 0.05 SF, VT, RE, MH p < 0.01 GH p < 0.001 Oral group vs. baseline: SF-36 significant worsening in single domains: SF, RE p < 0.05 |
| Study | Study Design | Drugs | Comparator Group(s) | Sample Size | Age | Sample Characteristics | Diagnosis | Assessment of QoL/SWB/Sat | Outcome | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Change in QoL/SWB/Sat | Effect | ||||||||||
| Möller et al., 2005 [73] | Non-randomized, single-arm study | RLAI-TM 25–50 mg | N/A | 1876 | 39.8 (12.1) | Symptomatically stable, requiring a therapy change | SZ | SF-36 5-point scale for satisfaction with treatment | Improvements in PANSS, CGI-S, GAF, SF-36, ESRS | ↑ SF-36 and Sat with treatment vs. baseline | ↑ vs. baseline for all SF-36 domains; > 5 pts difference for RP, BP, GH, SF, RE, and MH domains of SF-36 ↑ Sat. with treatment (p < 0.001) |
| Fleischhacker et al., 2005 [74] | Open-label, single arm, non-controlled multicenter trial | RLAI-TM 25–75 mg | N/A | 400 | 42 (15.0) | Symptomatically stable | SZ | SF-36 | Primary: PANSS; Secondary: SF-36 | ↑ SF-36 vs. baseline | ↑ vs. baseline for SF-36 MHC (p < 0.08) |
| Lee et al., 2007 [75] | Non-randomized, open-label, single-center trial | RLAI-TM 25–50 mg | N/A | 40 | 37 (10.5) | Symptomatically stable | SZ, SZA | SF-36 SWNS | Improvements in CGI-S, PANSS, GAF | SF-36 ↔ vs. baseline SWNS ↔ vs. baseline | Patient-rated perceived functioning and well-being did not change from baseline |
| Nick et al., 2006 [76] | Open-label, single-arm study | RLAI-TM 25–50 mg | N/A | 60 | 40.5 (12.0) | Symptomatically stable and considered to require a treatment change | SZ, SZA | SF-36 5-point scale for satisfaction with treatment | Primary outcome: change in PANSS total score Secondary outcome: change in CGI-S, GAF, SF-36, and treatment satisfaction | ↔ vs. baseline for SF-36 ↑ vs. baseline for the 5-point treatment satisfaction questionnaire | Treatment satisfaction improvement (p < 0.001). The proportion of patients rating their satisfaction as “very good” increased from 4.3% at baseline to 37.0% at endpoint |
| Lasser 2007 [77] | Open-label trial | RLAI-TM 25–50 mg | N/A | 66 | 23.3 (3.3) | Men aged 18–25 years and women aged 18–30 years | SZ | SF-36 | Improvements in PANSS, CGI–S, SF-36, DAI | ↑ of SF-36 vs. baseline | Improvements in all SF subscales except BP; improvements > 5 pts on the SF, RE, PF, and RP subscales |
| Niolu et al., 2015 [78] | Open-label, single-arm study | RLAI-TM 25–50 mg | N/A | 27 | 36.1 (NA) | Patients with frequent episodes of recurrence with hospital admission because of poor adherence to treatment | SZ, SZA | S-QoL SWN | Change from baseline after 30 months in SANS, SAPS, S-QoL, SWN | ↑ vs. baseline for SWN | S-QoL p < 0.01 SWN p < 0.0001 |
| Nasrallah et al., 2004 [79] | Double-blinded RCT | RLAI-TM 25–75 mg | Placebo | 369 | 25 mg: 38.9 (1.0); 50 mg: 36 (1.0); 75 mg: 39 (1.1) placebo: 38.2 (0.9) | PANSS total score between 60 and 120 pts | SZ | SF-36 | Primary outcome: change after 12 weeks in single domains of SF-36 | ↑ vs. placebo for SF-36 | RLAI total group vs. placebo: p < 0.05 in SF-36 RS, BP, GH, SF, RE, MH RLAI 50 mg vs. placebo: p < 0.05 in SF-36 BP, MH RLAI 75 mg vs. placebo: p < 0.05 in SF-36 BP, RS, FE |
| Isitt et al., 2016 [80] | Randomized, double-blind, placebo-controlled, multicenter phase 3 study | RLAI-OM 90 or 120 mg RBP-700, Sbc | Placebo | 337 | 18–55, median 43 | PANSS between 80 and 120 pts | SZ | SWNS MSQ | Primary outcome: change in EQ SWNS MSQ | ↑ vs. placebo for SWNS, EQ-VAS, MSQ | RBP-7000 120 mg vs. placebo: EQ-VAS (p = 0.0212), SWNS-PF (p = 0.0093), SI (p = 0.0368), and total score (p = 0.0395). MSQ with RBP-7000 vs. placebo (90 mg p = 0.0009, 120 mg p = 0.0006) RBP-7000 preferred over the previous medication (90 mg p = 0.0001, 120 mg p = 0.0619). |
| Litman et al., 2023 [81] | DB RCT + OLE | RLAI-OM 75 or 100 mg ISM, IM | Placebo | DB phase: Patients n = 433 OLE phase: Patients n = 215 | DB phase: RLAI: 42.7 (10.89) placebo: 40.6 (11.23) OLE phase: RLAI 39.3 (10.84) | DB phase: patients with acute exacerbation of SZ OLE phase: patients who completed the DB phase, divided into three groups—stable, stabilized, unstable patients. | SZ | SWNS | Primary outcome: change in PSP and SWNS scale for both DB phase and OLE phase | DB phase: ↑ vs. placebo in single items of SWNS OLE phase: ↑ vs. baseline in single items of SWNS | DB phase: RLAI-ISM vs. placebo: SWNS-PF p < 0.006 at day 29. Any other single item change was not significant (p < 0.01) OLE phase: RLAI-ISM vs. baseline: SWNS-SI changes were significant at weeks 24 and 52 only for unstable patients (p < 0.01) SWNS total changes were significant at week 24 only for unstable patients (p < 0.01) |
| Mihajlović et al., 2011 [82] | Cross-sectional study | RLAI-TM 25–50 mg | HLAI-OM 50 mg | 60 | RLAI: 35.33 (7.02) HLAI: 50.97 (11.44) | SZ patients in treatment with HLAI 50 mg or RLAI 25–50 mg for longer than one year | SZ | SWLS, WHOQoL-BREF | Primary outcome: change in SFS, SWLS, WHO-QoL-Brief | ↑ RLAI vs. ALO | WHOQoL-BREF: greater inclination to actively engage in everyday activities and leisure (p < 0.05) SWLS: higher satisfaction with life, living conditions, and self-image (p < 0.05) |
| Fe Bravo-Ortiz M et al., 2011 [83] | Observational longitudinal study | RLAI (dosage not specified) | Other AP: oral FGA, oral SGA, FGA-LAI | 1865 | <25 years: 193 (10.3%) 25–45 years: 1091 (58.5%) >45 years: 579 (31.0%) Not recorded: 2 (0.1%) | Patients initiating new antipsychotic treatment recruited by public mental health units and private clinics throughout Spain. | SZ, SZA, SZF | EQ-5D | Primary outcome: change in EQ-5D at months 3 and 6 Secondary outcome: change in PANSS total score and CGI-S at month 3 and 6 | ↑ vs. other LAI in improving EQ-5D | RIS LAI vs. other AP: higher percentage of patients (39.8%) with positive EQ-5D scores (in the past 3 months compared to other AP (p < 0.0018) |
| Study | Study Design | Drugs | Comparator Group(s) | Sample | Age | Sample Characteristics | Diagnosis | Assessment of QoL/SWB/Sat | Outcome | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Change in QoL/SWB/Sat | Effect | ||||||||||
| Witte et al., 2012 [84] | Randomized, double-blind, placebo-controlled trial | OLAI-TM 210 mg; OLAI-TM 300 mg; OLAI-OM 405 mg | Placebo | 404 | 210 mg: 39.8 (10.8); 300 mg: 41.5 (11.1); 405 mg: 39.5 (11.4); placebo: 42.6 (11.2) | BPRS ≥ 30 moderate-to-high level of symptom severity | SZ | SF-36 | QLS, SF-36 | ↑ SF-36 vs. placebo | Combined group: better SF-36 MCS (p = 0.007), MH (p = 0.003), SF (p = 0.0149). MH significant (p < 0.005) in all OLAI doses, SC significant in 300 mg and 405 mg OLAI groups |
| Study | Study Design | Drugs | Comparator Group(s) | Sample Size | Age | Sample Characteristics | Diagnosis | Assessment of QoL/SWB/Sat | Outcome | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Change in QoL/SWB/Sat | Effect | ||||||||||
| Schöttle et al., 2020 [85] | Observational longitudinal study | AOM 400 mg | N/A | 242 | 43.1 (15.1) | Stable patients who switched their treatment to AOM after 9.7 (±22.3) months of oral treatment. | SZ | WHO-5 Index | Primary outcome: change from baseline at month 6 in BPRS, CGI, WHO-5, GAF | ↑ vs. baseline in WHO-5 Index | At month 6, well-being significantly improved, with a 4.8-point increase on the WHO-5 index (p < 0.001). Initial progress was most prominent in the first 4 weeks |
| McEvoy et al., 2021 [86] | Post hoc analysis | AOM 400 mg | N/A | 291 | Age 18–70; median 38.6 | Clinically stable patients | SZ | SF-36 | Primary outcome: change in SF-36 mental component summary (MCS) and physical component summary (PCS) scores from baseline to 124 weeks | ↑ of SF-36 vs. baseline | SF-36 MCS ↑ vs. baseline (p < 0.05); SF-36 PCS ↔ vs. baseline |
| Study | Study Design | Drugs | Comparator Group(s) | Sample Size | Age | Sample Characteristics | Diagnosis | Assessment of QoL/SWB/Sat | Outcome | Results | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Change in QoL/SWB/Sat | Effect | ||||||||||
| Kwon et al., 2015 [87] | Randomized, open-label comparative study | PP1M | Oral SGA | 134 | 34.3 (9.7) | Patients unsatisfied with the current treatment with atypical antipsychotics. | SZ | MSQ, TSQM | MSQ, TSQM, PANSS, PSP | ↑ MSQ from baseline greater in PP1M; ↑ TSQM from baseline greater in PP1M | ↑ MSQ (p < 0.0001) ↑ TSQM (p < 0.0001) |
| Takekita et al., 2016 [88] | Randomized, open-label, clinical trial | PP1M | RLAI-TM | 30 | PP1M; 43.5 (11.8) RLAI: 46.4 (10.4) | Non-acute phase; PANSS ≤ 120; RLAI for 2 months or longer | SZ, SZA | SWNS | Primary: BACS; Secondary: SWNS, PANSS, DIEPSS | ↔ SWNS between groups | No between-group differences in SWNS |
| Sağlam Aykut, 2019 [89] | Observational longitudinal study | PP1M 100–150 mg | Oral SGA: quetiapine 600–1200 mg/d olanzapine 15–30 mg/d paliperidone 6–9 mg/d aripiprazole 15–30 mg/d risperidone 4–8 mg/d amisulpride 400–1200 mg/d clozapine 300–600 mg/d | 84 | PP1M: 36.91 (9.02) SGA oral: 37.24 (9.67) | Patients receiving treatment with either paliperidone palmitate or second-generation oral antipsychotics for at least six months | SZ | SF-36 | Primary outcome: change at month 6 in PANSS, CGI, ESRS, UKU-SERS, SF-36, MMAS, SACTI | ↑ vs. SGA oral in a single item of the SF-36 | PAL LAI vs. oral SGA: SF-36, higher scores in the General Health subscale (p < 0.001). No significant differences were found in the other subscales |
| Di Lorenzo et al., 2022 [90] | Observational cohort study | PP1M, PP3M | HLAI | 90 | PP1M: 50.6 (13.4) PP3M: 51.4 (13.0) HLAI: 55.9 (11.7) | LAI therapy for at least 6 months. | SZ, SZA | WHOQOL-BREF | WHOQOL-BREF, GAF, CGI-S | ↑ in WHOQOL-BREF vs. baseline within each group ↔ in WHOQOL-BREF between groups | ↑ in WHOQOL-BREF vs. baseline for all groups (p < 0.006) No statistical difference between groups |
| Bozzatello et al., 2018 [28] | Open-label, randomized, controlled trial | PP1M | ER oral paliperidone | 65 | NA | Diagnosis of stable but symptomatic schizophrenia; previous unsuccessful treatment with an oral antipsychotic | SZ | TSQM, SWNS, SES | Primary: TSQM, SWNS, SES; Secondary: CGI-SCH, PSP | ↑ TSMQ total and convenience subscale in the PP1M vs. oral paliperidone | ↑ TSMQ total score (p = 0.001) ↑ TSMQ convenience (p = 0.037) |
| Fernández-Miranda et al., 2021 [91] | Observational longitudinal study | PP3M | PP1M | 84 | 42.1 (7.6) | Patients with severe symptoms and impairment (GCI-S score ≥ 5) treated with PP3M after at least 2 years of stabilization with PP1M | SZ | TSQM, VAS-S | Primary outcome: change from baseline at month 24 in TSQM and VAS-S score | ↑ TSQM and VAS-S in PP3M vs. PP1M | TSQM: p < 0.01 VAS-S: p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brasso, C.; Bellino, S.; Bozzatello, P.; Montemagni, C.; Nobili, M.G.A.; Sgro, R.; Rocca, P. Second Generation Long-Acting Injectable Antipsychotics in Schizophrenia: The Patient’s Subjective Quality of Life, Well-Being, and Satisfaction. J. Clin. Med. 2023, 12, 6985. https://doi.org/10.3390/jcm12226985
Brasso C, Bellino S, Bozzatello P, Montemagni C, Nobili MGA, Sgro R, Rocca P. Second Generation Long-Acting Injectable Antipsychotics in Schizophrenia: The Patient’s Subjective Quality of Life, Well-Being, and Satisfaction. Journal of Clinical Medicine. 2023; 12(22):6985. https://doi.org/10.3390/jcm12226985
Chicago/Turabian StyleBrasso, Claudio, Silvio Bellino, Paola Bozzatello, Cristiana Montemagni, Marco Giuseppe Alberto Nobili, Rodolfo Sgro, and Paola Rocca. 2023. "Second Generation Long-Acting Injectable Antipsychotics in Schizophrenia: The Patient’s Subjective Quality of Life, Well-Being, and Satisfaction" Journal of Clinical Medicine 12, no. 22: 6985. https://doi.org/10.3390/jcm12226985
APA StyleBrasso, C., Bellino, S., Bozzatello, P., Montemagni, C., Nobili, M. G. A., Sgro, R., & Rocca, P. (2023). Second Generation Long-Acting Injectable Antipsychotics in Schizophrenia: The Patient’s Subjective Quality of Life, Well-Being, and Satisfaction. Journal of Clinical Medicine, 12(22), 6985. https://doi.org/10.3390/jcm12226985