
How Does Age Affect Injury Characteristics in Young Elite Footballers?—A Prospective Cohort Study of a German Youth Academy

 ,
,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Injury Monitoring
2.2. Exposure Monitoring
2.3. Data Analysis
3. Results
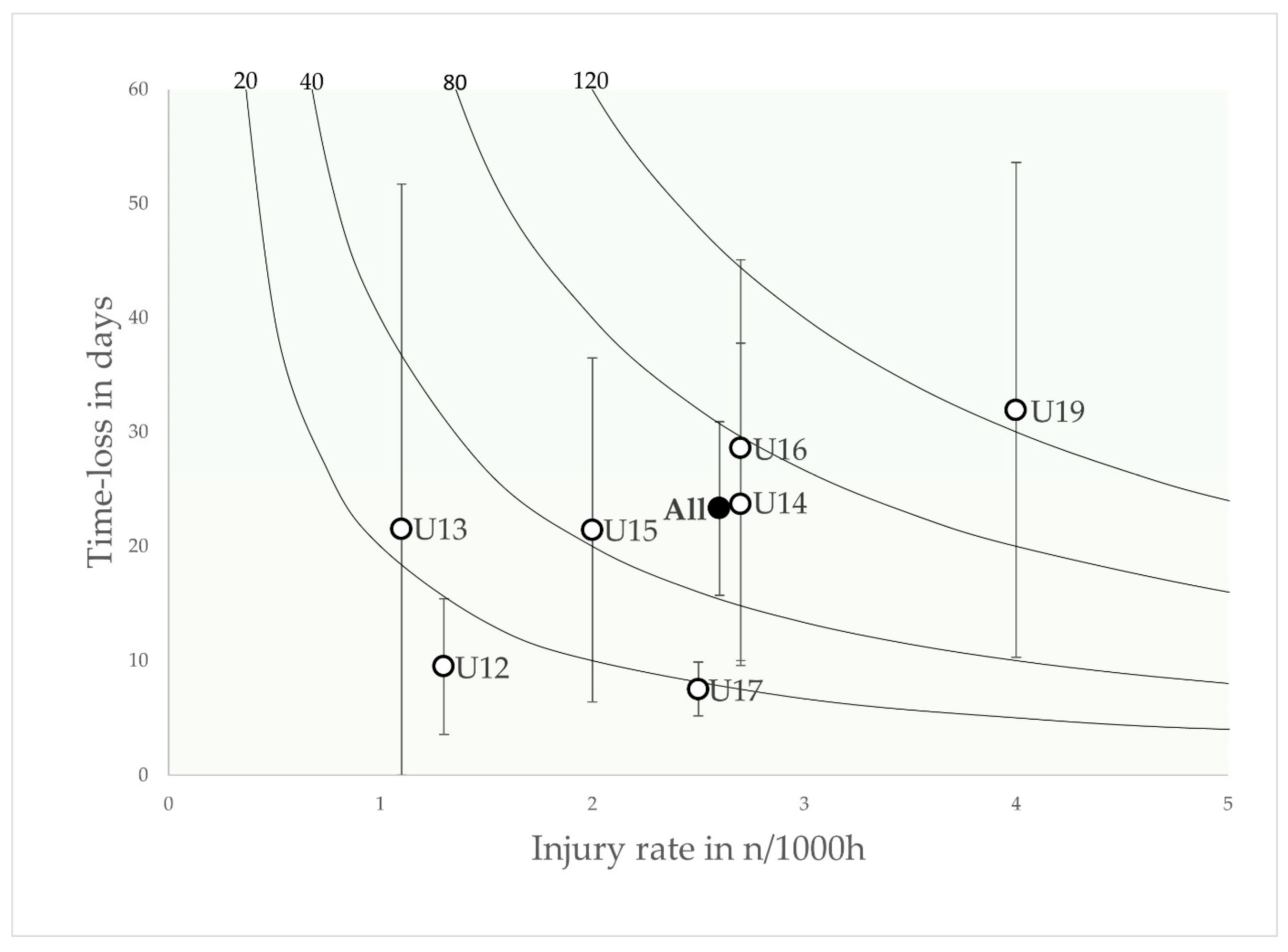
3.1. Main Injury Outcomes
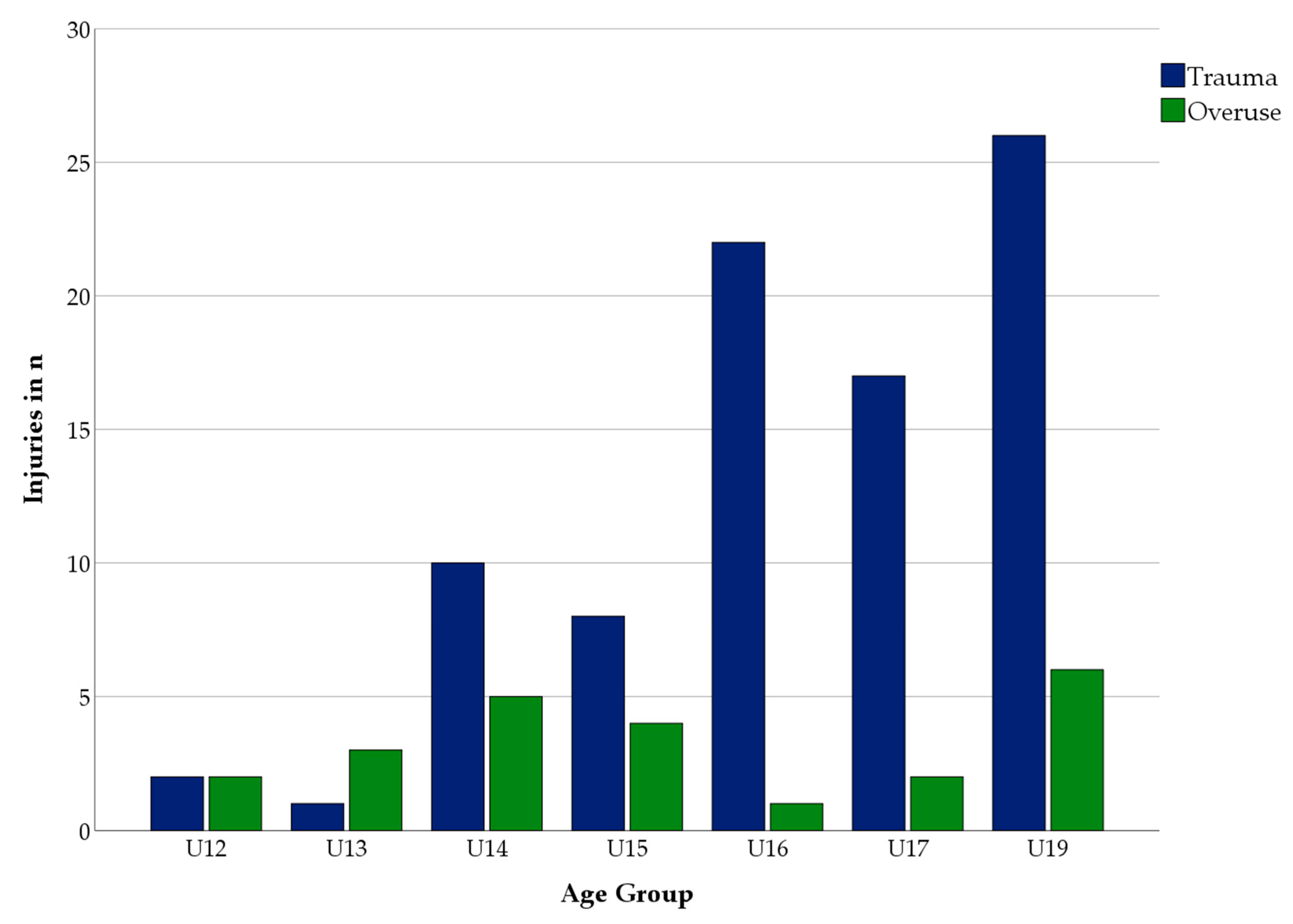
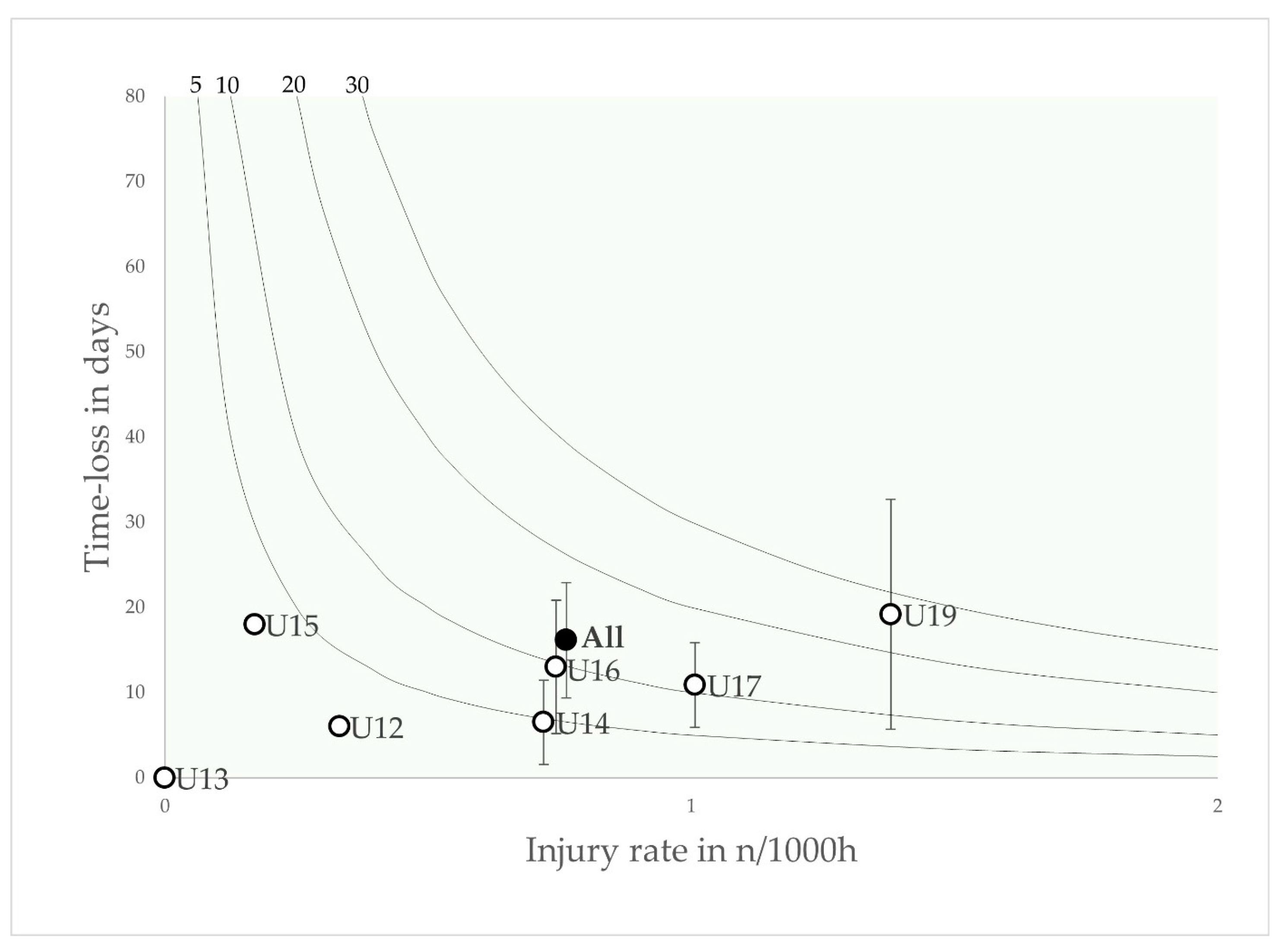
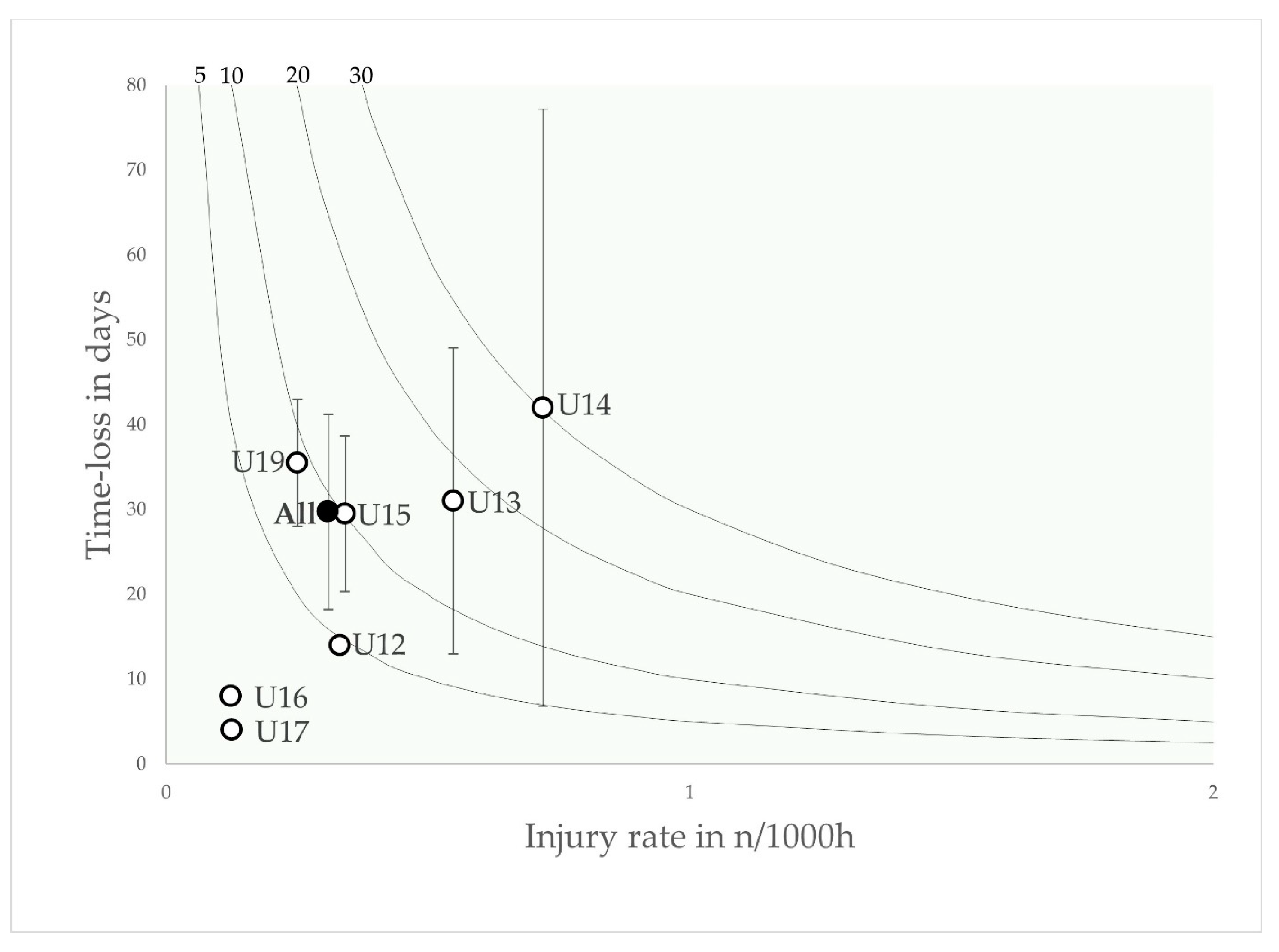
3.2. Injury Mechanism and Injury Type
3.3. Age Group Patterns
4. Discussion
4.1. Main Injury Outcomes
4.2. Onset Mechanism, Injury Type and Age Group Patterns
4.3. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jones, S.; Almousa, S.; Gibb, A.; Allamby, N.; Mullen, R.; Andersen, T.E.; Williams, M. Injury Incidence, Prevalence and Severity in High-Level Male Youth Football: A Systematic Review. Sports Med. 2019, 49, 1879–1899. [Google Scholar] [CrossRef]
- Finch, C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9, discussion 10. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, J.; Bergin, D.; Timpka, T.; Nyce, J.M.; Dahlström, Ö. Injuries in youth track and field are perceived to have multiple-level causes that call for ecological (holistic-developmental) interventions: A national sporting community perceptions and experiences. Scand. J. Med. Sci. Sports 2018, 28, 348–355. [Google Scholar] [CrossRef]
- Jaber, A.; Weishorn, J.; Berrsche, G.; Ott, H.; Bangert, Y. Injury Profile among Elite Youth Male Football Players in a German Academy. Int. J. Sports Med. 2021, 43, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, M.F.; Mountjoy, M.; Armstrong, N.; Chia, M.; Côté, J.; Emery, C.A.; Faigenbaum, A.; Gary Hall, J.; Kriemler, S.; Léglise, M.; et al. International Olympic Committee consensus statement on youth athletic development. Br. J. Sports Med. 2015, 49, 843–851. [Google Scholar] [CrossRef]
- van der Sluis, A.; Elferink-Gemser, M.T.; Brink, M.S.; Visscher, C. Importance of Peak Height Velocity Timing in Terms of Injuries in Talented Soccer Players. Int. J. Sports Med. 2015, 36, 327–332. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. An audit of injuries in six english professional soccer academies. J. Sports Sci. 2018, 36, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Price, R.J.; Hawkins, R.D.; Hulse, M.A.; Hodson, A. The Football Association medical research programme: An audit of injuries in academy youth football. Br. J. Sports Med. 2004, 38, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, F.; Carling, C.; Reilly, T.; Vandewalle, H.; Church, J.; Rochcongar, P. Incidence of injuries in elite French youth soccer players: A 10-season study. Am. J. Sports Med. 2006, 34, 928–938. [Google Scholar] [CrossRef]
- Hall, E.C.R.; Larruskain, J.; Gil, S.M.; Lekue, J.A.; Baumert, P.; Rienzi, E.; Moreno, S.; Tannure, M.; Murtagh, C.F.; Ade, J.D.; et al. An injury audit in high-level male youth soccer players from English, Spanish, Uruguayan and Brazilian academies. Phys. Ther. Sport 2020, 44, 53–60. [Google Scholar] [CrossRef]
- Bult, H.J.; Barendrecht, M.; Tak, I.J.R. Injury Risk and Injury Burden Are Related to Age Group and Peak Height Velocity Among Talented Male Youth Soccer Players. Orthop. J. Sports Med. 2018, 6, 2325967118811042. [Google Scholar] [CrossRef]
- Materne, O.; Chamari, K.; Farooq, A.; Weir, A.; Hölmich, P.; Bahr, R.; Greig, M.; McNaughton, L.R. Injury incidence and burden in a youth elite football academy: A four-season prospective study of 551 players aged from under 9 to under 19 years. Br. J. Sports Med. 2021, 55, 493–500. [Google Scholar] [CrossRef]
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, maturation, and physical activity, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Faulkner, R.A.; Davison, K.S.; Bailey, D.A.; Mirwald, R.L.; Baxter-Jones, A.D. Size-corrected BMD decreases during peak linear growth: Implications for fracture incidence during adolescence. J. Bone Miner. Res. 2006, 21, 1864–1870. [Google Scholar] [CrossRef] [PubMed]
- Weishorn, J.; Jaber, A.; Zietzschmann, S.; Spielmann, J.; Renkawitz, T.; Bangert, Y. Injury Patterns and Incidence in an Elite Youth Football Academy—A Prospective Cohort Study of 138 Male Athletes. J. Clin. Med. 2023, 12, 6138. [Google Scholar]
- Wik, E.H.; Lolli, L.; Chamari, K.; Materne, O.; Salvo, V.D.; Gregson, W.; Bahr, R. Injury patterns differ with age in male youth football: A four-season prospective study of 1111 time-loss injuries in an elite national academy. Br. J. Sports Med. 2021, 55, 794–800. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Ekstrand, J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br. J. Sports Med. 2018, 52, 1018–1021. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Jeong, H.S.; Lee, S.Y. Injury Profiles in Korean Youth Soccer. Int. J. Environ. Res. Public Health 2020, 17, 5125. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br. J. Sports Med. 2006, 40, 193. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef]
- Fuller, C.W. Injury Risk (Burden), Risk Matrices and Risk Contours in Team Sports: A Review of Principles, Practices and Problems. Sports Med. 2018, 48, 1597–1606. [Google Scholar] [CrossRef]
- Ford, P.; De Ste Croix, M.; Lloyd, R.; Meyers, R.; Moosavi, M.; Oliver, J.; Till, K.; Williams, C. The long-term athlete development model: Physiological evidence and application. J. Sports Sci. 2011, 29, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Renshaw, A.; Goodwin, P.C. Injury incidence in a Premier League youth soccer academy using the consensus statement: A prospective cohort study. BMJ Open Sport Exerc. Med. 2016, 2, e000132. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Spreco, A.; Bengtsson, H.; Bahr, R. Injury rates decreased in men’s professional football: An 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br. J. Sports Med. 2021, 55, 1084–1091. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Ekstrand, J. Injuries in Swedish elite football--a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand. J. Med. Sci. Sports 2005, 15, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R. Demise of the fittest: Are we destroying our biggest talents? Br. J. Sports Med. 2014, 48, 1265–1267. [Google Scholar] [CrossRef]
- Martins, F.; França, C.; Marques, A.; Iglésias, B.; Sarmento, H.; Henriques, R.; Ihle, A.; Lopes, H.; Ornelas, R.T.; Gouveia, É.R. Sports Injuries of a Portuguese Professional Football Team during Three Consecutive Seasons. Int. J. Environ. Res. Public Health 2022, 19, 12582. [Google Scholar] [CrossRef] [PubMed]
- Weishorn, J.; Spielmann, J.; Kern, R.; Mayer, J.; Friedmann-Bette, B.; Renkawitz, T.; Bangert, Y. Neue Therapieverfahren im Wettkampfsport. Die Orthopädie 2023, 52, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Rommers, N.; Rössler, R.; Goossens, L.; Vaeyens, R.; Lenoir, M.; Witvrouw, E.; D’Hondt, E. Risk of acute and overuse injuries in youth elite soccer players: Body size and growth matter. J. Sci. Med. Sport 2020, 23, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med 2016, 50, 731–737. [Google Scholar] [CrossRef]
- Gurau, T.V.; Gurau, G.; Musat, C.L.; Voinescu, D.C.; Anghel, L.; Onose, G.; Munteanu, C.; Onu, I.; Iordan, D.A. Epidemiology of Injuries in Professional and Amateur Football Men (Part II). J. Clin. Med. 2023, 12, 6293. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Rosado-Portillo, A.; Chamorro-Moriana, G.; Gonzalez-Medina, G.; Perez-Cabezas, V. Acute Hamstring Injury Prevention Programs in Eleven-a-Side Football Players Based on Physical Exercises: Systematic Review. J. Clin. Med. 2021, 10, 2029. [Google Scholar] [CrossRef]
- Al Attar, W.S.A.; Soomro, N.; Sinclair, P.J.; Pappas, E.; Sanders, R.H. Effect of Injury Prevention Programs that Include the Nordic Hamstring Exercise on Hamstring Injury Rates in Soccer Players: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 907–916. [Google Scholar] [CrossRef]
- O’Brien, J.; Finch, C.F. A systematic review of core implementation components in team ball sport injury prevention trials. Inj. Prev. 2014, 20, 357–362. [Google Scholar] [CrossRef]
- Barnes, C.; Archer, D.T.; Hogg, B.; Bush, M.; Bradley, P.S. The evolution of physical and technical performance parameters in the English Premier League. Int. J. Sports Med. 2014, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Mendez-Villanueva, A. Effects of age, maturity and body dimensions on match running performance in highly trained under-15 soccer players. J. Sports Sci. 2014, 32, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Kucera, K.L.; Marshall, S.W.; Kirkendall, D.T.; Marchak, P.M.; Garrett, W.E., Jr. Injury history as a risk factor for incident injury in youth soccer. Br. J. Sports Med. 2005, 39, 462. [Google Scholar] [CrossRef]
- Wik, E.H. Growth, maturation and injuries in high-level youth football (soccer): A mini review. Front. Sports Act. Living 2022, 4, 975900. [Google Scholar] [CrossRef]
- Monasterio, X.; Gil, S.M.; Bidaurrazaga-Letona, I.; Lekue, J.A.; Santisteban, J.; Diaz-Beitia, G.; Martin-Garetxana, I.; Bikandi, E.; Larruskain, J. Injuries according to the percentage of adult height in an elite soccer academy. J. Sci. Med. Sport 2021, 24, 218–223. [Google Scholar] [CrossRef]
- Elferink-Gemser, M.T.; Huijgen, B.C.; Coelho-e-Silva, M.; Lemmink, K.A.; Visscher, C. The changing characteristics of talented soccer players--a decade of work in Groningen. J. Sports Sci. 2012, 30, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Materne, O.; Chamari, K.; Farooq, A.; Tabben, M.; Weir, A.; Holmich, P.; Bahr, R.; Greig, M.; McNaughton, L.R. Shedding light on incidence and burden of physeal injuries in a youth elite football academy: A 4-season prospective study. Scand. J. Med. Sci. Sports 2022, 32, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Materne, O.; Chamari, K.; Farooq, A.; Weir, A.; Hölmich, P.; Bahr, R.; Greig, M.; McNaughton, L.R. Association of Skeletal Maturity and Injury Risk in Elite Youth Soccer Players: A 4-Season Prospective Study with Survival Analysis. Orthop. J. Sports Med. 2021, 9, 2325967121999113. [Google Scholar] [CrossRef] [PubMed]
- Weishorn, J.; Bumberger, A.; Niemeyer, P.; Tischer, T.; Mueller-Rath, R.; Renkawitz, T.; Bangert, Y. The first decade of the DGOU’s cartilage register-insights for clinical practice. Orthopadie 2023, 52, 455–462. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Definition |
|---|---|
| Player season | A player who participated in a particular season. |
| Time-loss injury | A physical condition or symptom experienced by a player that requires the medical staff to restrict, in whole or in part, the player’s participation in a future football team training session or match [20]. |
| Injury incidence | The frequency of time-loss injuries per 1000 player hours [20]. |
| Season incidence proportion | Percentage of players with at least one time-loss injury recorded for the season studied [16]. |
| Injury burden | A measure of the impact of injury as a product of frequency (how often) and severity (duration), calculated as the total number of days lost per 1000 player hours [21]. |
| Training exposure | Team and individual physical activities under the control of the team’s coaching or fitness staff, designed to maintain or improve football skills or physical condition. Team exposure is measured in hours [20]. |
| Match exposure | Match between teams from different clubs or academies. Player exposure is measured in hours [22]. |
| U12 | U13 | U14 | U15 | U16 | U17 | U19 | |
|---|---|---|---|---|---|---|---|
| Players (n) | 15 | 18 | 20 | 21 | 22 | 21 | 21 |
| Age (y, SD) | 11.8 (0.4) | 12.7 (0.5) | 13.5 (0.5) | 14.6 (0.5) | 15.7 (0.5) | 16.6 (0.5) | 18.0 (0.8) |
| Stature (cm, SD) | 148.1 (7,1) | 156.7 (7.2) | 161.4 (7.0) | 168.5 (7.3) | 173.8 (6.4) | 176.7 (5.2) | 181.7 (7.8) |
| Body mass (kg, SD) | 42.1 (5.5) | 44.7 (6.1) | 48.3 (5.9) | 55.4 (6.1) | 62.5 (6.2) | 69.8 (6.7) | 75.1 (7.5) |
| Time-loss injuries (n) | 4 | 4 | 15 | 12 | 22 | 20 | 32 |
| Total time-loss (days) | 38 | 86 | 356 | 257 | 629 | 148 | 1022 |
| Overall Injury incidence | 1.3 | 1.1 | 2.7 | 2.0 | 2.7 | 2.5 | 4.0 |
| Training injury incidence | 1.3 | 1.1 | 2.1 | 2.2 | 1.8 | 1.8 | 2.7 |
| Match injury incidence | 1.5 | 1.2 | 6.6 | 1.2 | 13.9 | 9.2 | 14.5 |
| Mean days lost per injury (95%-CI) | 9.5 (3.6–15.4) | 21.5 (0–51.7) | 23.7 (9.6–37.8) | 21.4 (6.4–36.5) | 28.6 (10–45.1) | 7.5 (5.2–9.9) | 31.9 (10.3–53.6) |
| Injury burden (95%-CI) | 12.4 (4.7–20) | 23.7 (0–56.9) | 64 (25.9–102.1) | 42.8 (12.8–73) | 77.2 (27–121.8) | 18.8 (13–24.8) | 127.6 (41.2–214.4) |
| Body Part | Injuries Incidence Rate | Median Time-Loss | Burden | |
|---|---|---|---|---|
| Diagnosis | n | Injuries Per 1000 h | Days (IQ 25th–75th) | Time Loss Days Per 1000 h (95% CI) |
| Head and Neck | 5 | 0.12 | 10 (4.5–12.5) | 1.1 (0.4 to 1.7) |
| Concussion | 2 | 0.05 | 10.5 (10–10.5) | 0.5 (0.2 to 0.8) |
| Nasal bone fracture | 2 | 0.05 | 9 (4–9) | 0.5 (0.2 to 0.8) |
| Cut | 1 | 0.2 | 5 (5–5) | 1 (1 to 1) |
| Upper Limb | 10 | 0.24 | 7 (4.75–31.75) | 5.4 (0.2 to 11.0) |
| AC-contusion | 1 | 0.02 | 4 (4–4) | 0.1 (0.1 to 0.1) |
| Shoulder contusion | 1 | 0.02 | 5 (5–5) | 0.1 (0.1 to 0.1) |
| Ellbow contusion | 1 | 0.02 | 8 (8–8) | 0.2 (0.2 to 0.2) |
| Forearm contusion | 1 | 0.02 | 7 (7–7) | 0.1 (0.1 to 0.1) |
| Forearm fracture | 2 | 0.05 | 45.5 (45–46) | 2.3 (1.4 to 3.7) |
| Hand contusion | 2 | 0.05 | 5.5 (5–6) | 0.3 (0.2 to 1.2) |
| Hand/finger sprain | 1 | 0.02 | 6 (6–6) | 0.1 (0.1 to 0.1) |
| Hand/finger fracture | 1 | 0.02 | 93 (93–93) | 1.9 (1.9 to 1.9) |
| Trunk | 3 | 0.07 | 11 (5.0–11) | 1.0 (0.4 to 1.8) |
| Overuse unspecific pathology | 2 | 0.05 | 18.5 (11–18.5) | 0.9 (0.6 to 1.3) |
| Functional muscle disorder | 1 | 0.02 | 5 (5–5) | 0.1 (0.1 to 0.1) |
| Hip and Pelvis | 5 | 0.12 | 36 (13.5–58.5) | 4.3 (1.0 to 7.7) |
| Physeal injury (avulsion) | 2 | 0.05 | 34 (12–34) | 1.7 (0.6 to 2.8) |
| Physeal injury (apophysitis) | 2 | 0.05 | 48.5 (36–48.5) | 2.4 (1.8 to 3.1) |
| Gluteal strain | 1 | 0.02 | 15 (15–15) | 0.3 (0.3 to 0.3) |
| Thigh | 26 | 0.62 | 6.0 (4–32.5) | 7.6 (4.6 to 10.5) |
| Torn hamstrings | 5 | 0.12 | 23.0 (13–44) | 3.4 (1.1 to 5.6) |
| Torn quadriceps | 1 | 0.02 | 15 (15–15) | 0.3 (0.3 to 0.3) |
| Thigh contusion | 3 | 0.07 | 5 (4–5) | 0.4 (0.2 to 0.5) |
| Adductor strain | 5 | 0.12 | 11 (5.0–17.5) | 1.3 (0.2 to 2.5) |
| Hamstring strain | 4 | 0.1 | 4 (4–4.75) | 0.4 (0.3 to 0.5) |
| Quadriceps strain | 8 | 0.19 | 6 (4–13) | 1.8 (0.4 to 3.1) |
| Knee | 21 | 0.5 | 14 (7.5–38) | 22.1 (4.2 to 40) |
| Knee sprain/ligament | 9 | 0.21 | 10 (4–16) | 2.4 (1.2 to 3.6) |
| Meniscus and cartilage damaged | 3 | 0.07 | 48 (33–48) | 6.2 (2.9 to 9.5) |
| Knee physeal injury | 7 | 0.17 | 14 (8–28) | 3.2 (1.1 to 5.3) |
| Patellar dislocation | 1 | 0.02 | 90 (90–90) | 1.8 (1.8 to 1.8) |
| Torn ACL | 1 | 0.02 | 339 (339–339) | 6.8 (6.8 to 6.8) |
| Lower Leg and Calf | 6 | 0.14 | 7.5 (5.75–9.75) | 1.1 (0.7 to 1.5) |
| Functional muscle disorder | 1 | 0.02 | 12 (12–12) | 0.2 (0.2 to 0.2) |
| Torn calf muscle | 1 | 0.02 | 8 (8–8) | 0.2 (0.2 to 0.2) |
| Calf muscle strain | 3 | 0.07 | 6 (5–6) | 0.5 (0.1 to 0.8) |
| Calf cut | 1 | 0.02 | 7 (7–7) | 0.1 (0.1 to 0.1) |
| Foot and Ankle | 33 | 0.79 | 14 (5–31) | 18.0 (11.3 to 24.7) |
| Ankle sprain/ligament | 19 | 0.45 | 13.0 (7–19) | 7.0 (3.5 to 10.4) |
| Ankle contusion | 1 | 0.02 | 4 (4–4) | 0.1 (0.1 to 0.1) |
| Ankle fracture | 1 | 0.02 | 57 (57–57) | 1.1 (1.1 to 1.1) |
| Ankle stress injury | 1 | 0.02 | 5 (5–5) | 0.1 (0.1 to 0.1) |
| Physeal injury | 2 | 0.05 | 44 (39–44) | 2.2 (2.0 to 2.5) |
| Foot/toe fracture | 4 | 0.1 | 56 (17–65.8) | 4.6 (0.2 to 9.0) |
| Foot contusion | 3 | 0.07 | 4 (4–4) | 2.2 (0.3 to 4.2) |
| Foot sprain | 2 | 0.05 | 11 (4–11) | 0.6 (0.2 to 0.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weishorn, J.; Jaber, A.; Trefzer, R.; Zietzschmann, S.; Kern, R.; Spielmann, J.; Renkawitz, T.; Bangert, Y. How Does Age Affect Injury Characteristics in Young Elite Footballers?—A Prospective Cohort Study of a German Youth Academy. J. Clin. Med. 2023, 12, 6938. https://doi.org/10.3390/jcm12216938
Weishorn J, Jaber A, Trefzer R, Zietzschmann S, Kern R, Spielmann J, Renkawitz T, Bangert Y. How Does Age Affect Injury Characteristics in Young Elite Footballers?—A Prospective Cohort Study of a German Youth Academy. Journal of Clinical Medicine. 2023; 12(21):6938. https://doi.org/10.3390/jcm12216938
Chicago/Turabian StyleWeishorn, Johannes, Ayham Jaber, Raphael Trefzer, Severin Zietzschmann, Ralph Kern, Jan Spielmann, Tobias Renkawitz, and Yannic Bangert. 2023. "How Does Age Affect Injury Characteristics in Young Elite Footballers?—A Prospective Cohort Study of a German Youth Academy" Journal of Clinical Medicine 12, no. 21: 6938. https://doi.org/10.3390/jcm12216938
APA StyleWeishorn, J., Jaber, A., Trefzer, R., Zietzschmann, S., Kern, R., Spielmann, J., Renkawitz, T., & Bangert, Y. (2023). How Does Age Affect Injury Characteristics in Young Elite Footballers?—A Prospective Cohort Study of a German Youth Academy. Journal of Clinical Medicine, 12(21), 6938. https://doi.org/10.3390/jcm12216938