Abstract
Background: Pulse wave velocity (PWV) assessment represents a simple method to estimate arterial distensibility. At present, carotid-femoral PWV (cf-PWV) is considered the gold standard method in the non-invasive evaluation of the elastic properties of the aorta. On the other hand, the mechanical properties of muscular arteries can be evaluated on the axillo-brachial-radia axis by estimating the carotid-radial PWV (cr-PWV). While a number of studies have addressed these issues in adults, limited information is available on the respective features of cf-PWV and cr-PWV and on their modulating factors in children and adolescents at increased cardiovascular risk. Methods: The mechanical properties of the predominantly elastic (aorta) and muscular (axillo−brachial−radial axis) arteries were evaluated in a pediatric population characterized by either elevated blood pressure (BP) or excess body weight, and the main factors affecting cf-PWV and cr-PWV values in these individuals were investigated. Results: 443 children and adolescents (median age 11.5 years, 43.3% females) were enrolled; 25% had BP values >90th percentile and 81% were excess weight. The cf-PWV values were significantly lower than the cr-PWV values: median (Q1–Q3) = 4.8 m/s (4.3–5.5) and 5.8 m/s (5.0–6.5), respectively (p < 0.001). The pubertal development (p < 0.03), systolic BP and diastolic BP z-scores (p = 0.002), heart rate (p < 0.001), and waist-to-height ratio (p < 0.005) were significantly associated with cf-PWV values. No significant association was found between BMI z-score and cf-PWV. Predictors of high cf-PWV (>95th percentile) were the heart rate (OR 1.07, 95%CI 1.04–1.10, p < 0.001) and waist-to-height ratio (OR 1.06, 95%CI 1.0–1.13, p = 0.04). The variables significantly related with cr-PWV values were diastolic BP z-score (p = 0.001), heart rate (p < 0.01), and HOMA index (p < 0.02). No significant association was found between the cr-PWV and BMI z-score or waist-to-height ratio. Conclusions: Systolic and diastolic BP values and central obesity are associated with aortic stiffness in a population of children and adolescents at increased cardiovascular risk. In contrast, diastolic BP, heart rate, and levels of insulin resistance appear to be related to distensibility of the upper limb vascular district.
1. Introduction
Measurement of pulse wave velocity (PWV) represents a simple way to measure the stiffness of a specific arterial segment [1]. The pulse wave is transmitted through the arterial vessels, and its speed is inversely related to the viscoelastic properties of the wall itself; the higher the velocity, the less elastic the wall [2]. Carotid-femoral PWV (cf-PWV) investigates the viscoelastic properties of the aorta and is considered the non-invasive gold standard for estimating the degree of aortosclerosis in daily clinical practice [3,4]. In adults, high cf-PWV values represent an independent risk factor for cardiovascular events, as well as an important prognostic factor for cardiovascular mortality [3,5]. PWV can be modified both by structural and functional elements of the arterial wall [2].
Regarding the structural elements, the viscoelastic properties of the arterial wall in large arteries are guaranteed by the ratio between the elastin fibers and the collagen fibers in the tunica media [6,7,8]. This relationship can be altered by an increase in collagen fibers (as observed in arterial hypertension), as well as by a reduction in elastic fibers (as observed with aging) [4,9,10]. The aging process causes histological alterations in the arterial wall. Reduced elastin synthesis and increased elastase activity cause thinning and breakage of elastin fibers, and the result is a decrease in the elastin and collagen ratio. Starting from the first decades of life, there is a slow but progressive increase in aortic PWV values, with a rapid and exponential increase in adults and in the elderly population [11]. If the maintenance of the structural characteristics of the arterial wall represents an important element to guarantee the viscoelastic properties of the aorta and of the large elastic arteries, on the other hand the elastin−collagen ratio in the wall has a negligible impact on the mechanical properties of the muscular arteries.
Muscular arteries are mainly affected by functional factors, mostly related to the activity of the sympathetic nervous system [2,9]. Enhanced sympathetic activity results in an increase in heart rate, ventricular contractility, and peripheral vascular resistance, leading to a rise in mean arterial pressure. Concerning arterial vessels, the sympathetic system modulates the activity and the tone of the smooth muscle cells of the arterial wall. On the other hand, the impact of the sympathetic nervous system on the distensibility properties of the aorta is weak and it has been shown that the mechanical properties of the human aorta remain largely unaffected during sympathetic stimulation. The mechanical properties of predominantly muscular peripheral arteries can be assessed in the peripheral arterial districts of the lower limbs and upper limbs, by measuring the femoral-tibial PWV and carotid-radial PWV (cr-PWV), respectively. The latter provides an estimate of the viscoelastic properties of the axillo−brachial−radial arterial district. Several studies performed on the adult population have shown that elevated femoro-tibial and cr-PWV values have no prognostic or clinical significance [12,13]. Furthermore, while cf-PWV increases significantly with aging, cr-PWV does not change significantly with age [2]. Overall, PWV assessed at the upper limb likely reflects a functional condition of the arterial tree, which is closely related to the activation of the sympathetic system.
The relationship between PWV in the aorta and in upper limb muscular arteries has not yet been investigated in childhood and adolescence, and it is unclear what factors affect cf-PWV and cr-PWV at this age in the presence of cardiovascular risk factors. Thus, the aim of our study was to evaluate the main factors associated with cf-PWV and cr-PWV values in a pediatric population at increased cardiovascular risk.
2. Materials and Methods
2.1. Participants
We studied a cohort of children and adolescents, consecutively referred from May 2008 to September 2022 to the Unit for Cardiovascular Risk Assessment in Children of Istituto Auxologico Italiano, IRCCS (Milan, Italy) by their primary care pediatricians, for the clinical finding of excess weight or elevated blood pressure (BP) values.
Children and adolescents with diabetes mellitus, secondary hypertension, hypertension under drug treatment, congenital cardiovascular disease, and kidney disease were excluded from the study. The presence of chronic disease involving habitual therapy was considered an exclusion criterion from the study.
The study protocol was approved by the local institutional ethics committee and conformed to the ethical guidelines of the 1975 Declaration of Helsinki. Informed consent was obtained from parents or legal representatives before the enrolment in the study.
2.2. Clinical Parameters
Height, weight, and waist circumference were measured. Waist circumference was measured by means of a flexible tape in a standing position. Body mass index (BMI) was calculated as weight/height2 (Kg/m2). The waist-to-height ratio (WtHr) was obtained dividing waist circumference by height, and expressed as percentage [14,15]. BMI z-scores were derived from the Centre for Disease and Control prevention charts [16]. All study participants were classified as normal weight, overweight, or obese according to the International Obesity Task Force classification [17]. The pubertal stage was assessed and children were divided into two categories, pre-pubertal and pubertal, according to Tanner [18,19], considering pre-pubertal boys with gonadal stage 1 and girls with breast stage 1.
2.3. Blood Pressure Measurement
BP measurements were performed after at least 5 min of rest, in a sitting position, using an oscillometric device validated in children (Omron 705IT; Omron Co., Kyoto, Japan) with an appropriate cuff for the upper-arm size. The BP measurement was performed 3 times (at intervals of 3 min) and the average of the last two measurements was considered. Systolic BP and diastolic BP percentiles and z-scores were calculated according to the nomograms of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents [20,21]. The children were classified as normotensive if both systolic and diastolic BP percentiles were <90th; high-normal if systolic BP and/or diastolic BP percentiles were ≥90th but <95th; and hypertensive if systolic BP and/or diastolic BP percentiles were ≥95th.
2.4. Biochemical Dosages
Fasting blood samples were taken in all study participants to measure serum glucose, insulin, uric acid, and creatinine. Commercial kits were employed for all analyses: enzymatic method with hexokinase Glucose HK Gen.3 Cobas Roche (F. Hoffmann-La Roche AG, Basel, Switzerland), for glucose assay; ElectroChemiLuminescence Elecsys Insulin Cobas Roche immunoassay was used for the insulin assay; colorimetric enzymatic test Uric Acid 2 Cobas Roche for the serum uric acid assay; and colorimetric kinetic test based on the Jaffé method Creatinine Jaffé Gen.2 Cobas Roche for creatinine assay. The homeostatic model assessment (HOMA) index was obtained by dividing the product of the serum insulin (mU/L) and serum glucose (mmol/L) by 22.5 [22]. The glomerular filtration rate was estimated (eGFR) using the Schwartz formula [23].
2.5. Arterial Stiffness Assessment
Measurements of arterial distensibility were obtained at a stable room temperature after 10 min of rest, by a validated ETT PulsePen tonometer [24] (DiaTecne srl, San Donato Milanese, Italy), as described in detail previously [25,26,27]. Briefly, PulsePen consists of a pocket size, high-fidelity applanation tonometer, and an integrated ECG unit. Aortic PWV was measured by recording carotid and femoral waveforms in rapid succession. cf-PWV was defined as 80% of the distance between the measuring sites divided by the time delay between the distal (femoral) pulse wave from the proximal (carotid) pulse wave, using the R wave of the ECG trace as the reference [11]. The R−R interval on the ECG recording was used to define the heart rate. The use of the PulsePen device in children had been validated in a previous study, which provided reference values according to gender and age for cf-PWV in children and adolescents [28].
2.6. Statistical Analysis
The characteristics of the cohort, overall and stratified according to sex, were described by median and interquartile range (Q1–Q3) if the variables were continuous and by frequencies and percentages if they were categorical. Univariate analyses to compare the characteristics of the two groups of children were conducted using the Mann−Whitney test in case of continuous variables, and through the Chi-Square test in case of categorical variables.
The univariate associations between cf-PWV (or cr-PWV) and systolic BP, diastolic BP and BMI z-score values, WtHr, uric acid, and HOMA index are represented in scatterplots, where 95% confidence interval on the Pearson correlation test and the p-value are displayed.
Multiple linear regression models were used to assess the impact of sex, pubertal status, systolic BP (or diastolic BP) z-score, BMI z-score (or WtHr), heart rate (detected at the time of measurement of cf-PWV), uric acid, HOMA index, and eGFR on cf-PWV. Multiple linear regression models were used to assess the impact of sex, pubertal status, systolic BP (or diastolic BP) z-score, BMI z-score (or WtHr), heart rate (detected at the time of measurement of cf-PWV), uric acid, HOMA index, and eGFR on cr-PWV. Multiple logistic regression models were used to assess the impact of sex, pubertal status, systolic BP (or diastolic BP) z-score, BMI z-score (or WtHr), heart rate, uric acid, HOMA index, and eGFR on having cf-PWV values equal to or greater than the 95th percentile according to gender and age [28]. As there were no reference nomograms for cr-PWV, only the multiple linear regression model was performed for this variable. Statistical analyses were performed with R (R Fundation for Statistical Computing, Vienna, Austria) 4.1.2 version (http://www.R-project.org) accessed on 1 November 2023. All p-values were 2-sided, with p-values < 0.05 considered to be statistically significant.
3. Results
3.1. Population
The study involved 443 children and adolescents referred to our clinic. Table 1 shows the characteristics of the population enrolled in the study. The median age was 11.5 years; 43.3% of children were female and 54% were prepubescent. Here, 25.5% (n = 113) had BP values greater than or equal to the 90th percentile. Furthermore, 80.8% (n = 358) were of excess weight, and 67.5% (n = 295) had WtHr >50%. The median cf-PWV value was 4.8 m/s, and 11.4% (n = 50) of the children had cf-PWV values equal to or greater than the 95th percentile [28]. The cr-PWV values were significantly higher (median value 5.8 m/s) than the cf-PWV values (p < 0.001), without differences between males and females.

Table 1.
Anthropometric and clinical characteristics according to sex.
3.2. Factors Affecting Arterial Stiffness
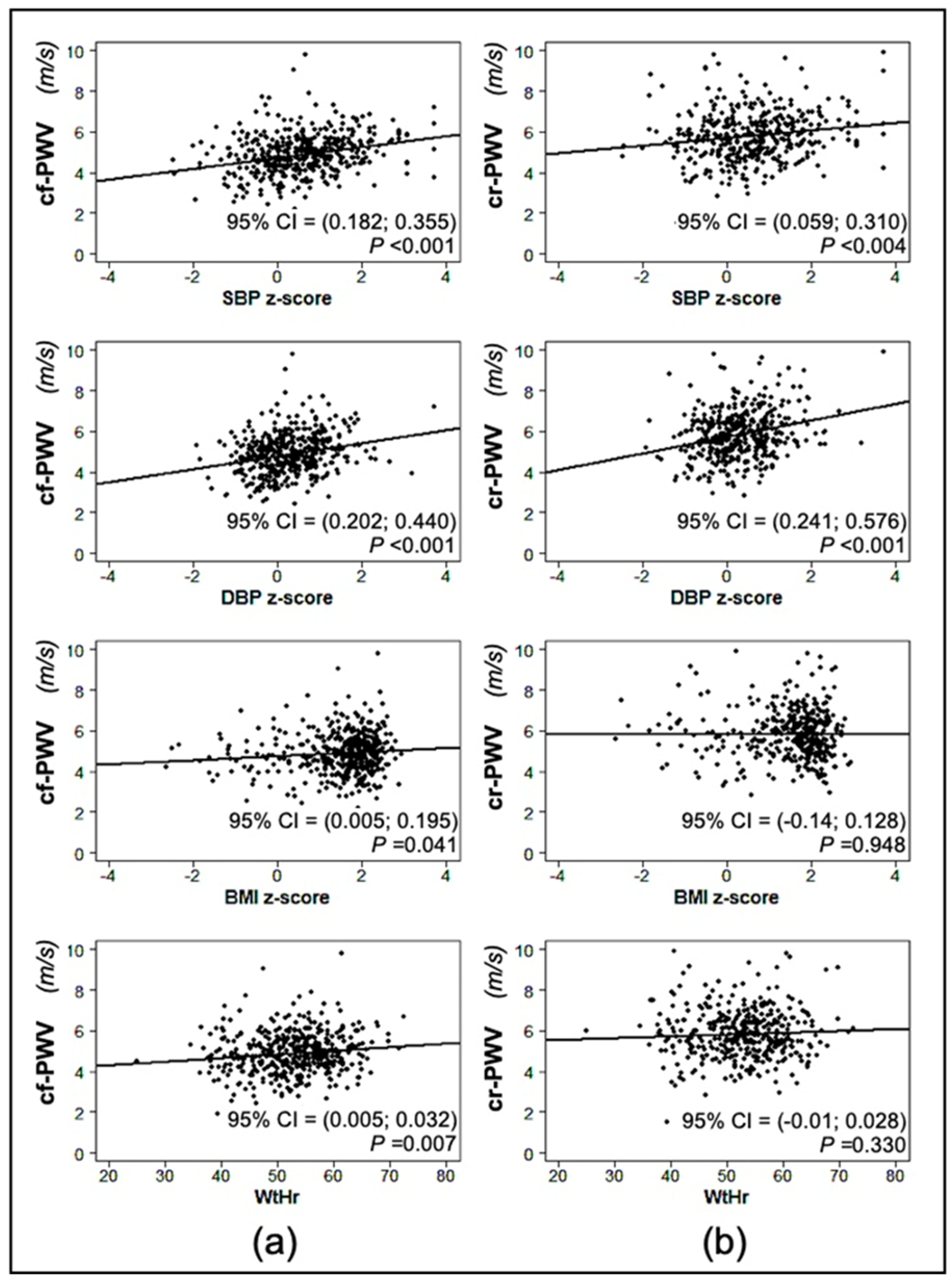
Figure 1 shows the linear regression between cf-PWV/cr-PWV values and systolic BP, diastolic BP and BMI z-scores, and WtHr. The systolic BP z-score was significantly correlated with both cf-PWV (p < 0.01) and cr-PWV values (p < 0.01). The same was true for the correlation of diastolic BP z-scores with both cf-PWV (p < 0.001) and cr-PWV (p < 0.001) values. BMI z-score and WtHr were associated with cf-PWV values (p = 0.041 and p = 0.007, respectively), but not with cr-PWV values. Both serum uric acid and HOMA index values were correlated with cf-PWV (p < 0.001), while only HOMA index but not serum uric acid was associated with cr-PWV (p = 0.005) (Figure 2).

Figure 1.
Linear regression between carotid-femoral pulse wave velocity (cf-PWV) (a) and carotid-radial pulse wave velocity (cr-PWV) (b) and systolic (SBP), diastolic blood pressure (DBP) z-score, body mass index (BMI) z-score, and waist-to-height ratio (WtHr).
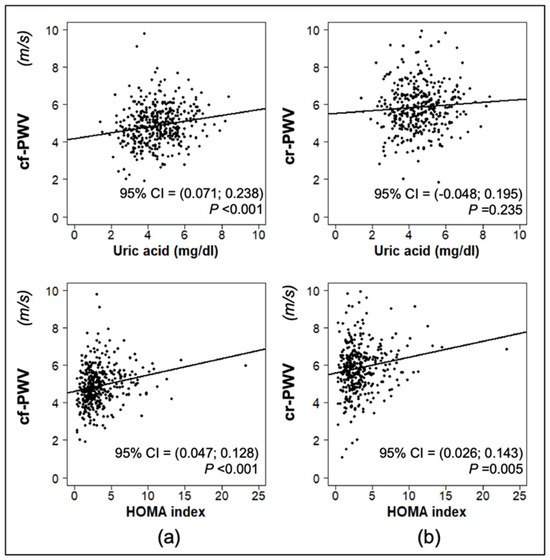
Figure 2.
Linear regression between carotid-femoral pulse wave velocity (cf-PWV) (a) and carotid-radial pulse wave velocity (cr-PWV) (b) and serum uric acid and homeostatic model assessment (HOMA) index.
Multiple linear regression analysis (Table 2) showed that the variables significantly associated with cf-PWV values were the presence of pubertal development (p < 0.03), systolic BP and diastolic BP z-scores (p = 0.002), and heart rate (p < 0.001). A correlation between HOMA index and cf-PWV was evident when the model was adjusted for diastolic BP z-score (p = 0.039). The estimated glomerular filtration rate (eGFR) was inversely related with cf-PWV (p = 0.020). No significant association was evident between BMI z-score and cf-PWV. In contrast, when WtHr was entered into the model instead of BMI z-score, a significant correlation was shown between WtHr and cf-PWV (p < 0.05). All of the results of the previous model were confirmed, except for the HOMA index, which was no longer associated with cf-PWV. If the HOMA index was removed from the regressors, the association between WtHr and cf-PWV became stronger (p < 0.01), while the other results remained unchanged.
Table 2.
Results of multiple linear regression analysis with carotid-femoral pulse wave velocity (m/s) as dependent variables in the entire sample.
The multiple logistic regression model exploring factors significantly associated with the presence of cf-PWV values equal to or greater than the 95th percentile for sex and age, adjusted for systolic BP z-score (Table 3), showed a direct association with heart rate (OR 1.07 95%CI 1.04–1.10, p < 001) and an inverse association with eGFR (OR 0.98 95% CI 0.97–0.99, p = 0.025) (Table 4). The results were similar when the diastolic BP z-score was included in the model. When the BMI z-score was substituted for WtHr in the model adjusted for systolic BP z-score, the OR was 1.07 (95%CI 1.04–1.10, p < 0.001) for heart rate and 0.98 (95%CI 0.97–0.99, p = 0.018) for eGFR. Interestingly, in the latter model, WtHr was also significantly associated with the presence of cf-PWV values equal to or greater than the 95th percentile (OR 1.06 95%CI 1.0–1.13, p = 0.040). Similar results were obtained for the model adjusted for diastolic BP z-score. The results did not change when the HOMA index was removed from the model.
Table 3.
Results of multiple regression model with carotid-femoral pulse wave velocity values equal to or greater than the 95th percentile as dependent variables.
Table 4.
Results of multiple linear regression analysis with carotid-radial pulse wave velocity (m/s) as dependent variables in the entire sample.
Variables significantly related to cr-PWV were heart rate (p < 0.01) and HOMA index (p < 0.02), diastolic BP z-score (p = 0.001), but not systolic BP z-score. There was an inverse correlation between cr-PWV and eGFR (p = 0.035). No significant association was evident between BMI z-score and cr-PWV. When WtHr was included in the model instead of BMI z-score, the results were essentially unchanged and WtHr was not associated with cr-PWV (Table 4). The results did not change when the HOMA index was removed from the model.
4. Discussion
To our knowledge, this is the first study comparing parameters estimating the viscoelastic properties of the aorta and upper limb muscular arteries in a pediatric cohort with cardiovascular risk factors. As a main and innovative contribution, the present study highlights how, in this population, the factors significantly associated with upper limb arterial distensibility (estimated by cr-PWV) are somewhat different from those associated with aortic distensibility (estimated by cf-PWV). If the viscoelastic properties of muscular arteries in the upper limbs appear to be mediated by tonic levels of sympathetic activity, aortic distensibility appears, instead, to be more affected by blood pressure, heart rate, and WtHr. Interesting, a significant and inverse correlation with eGFR was found with both cf-PWV and cr-PWV values.
4.1. Aortic Pulse Wave Velocity
Aortic PWV depends on structural elements and transient functional changes in the arterial wall. The structural factors are stable and closely related to the relationship between elastin and collagen fibers in the tunica media of the arterial wall. The tunica media of the aorta has a typical lamellar arrangement, characterized by an orderly arrangement and interrelationship between elastic fibers and collagen fibers. Elastic fibers are characterized by an accentuated viscoelastic property and collagen fibers are mainly responsible for a structural containment function.
The characteristically different adult patterns of elastin and collagen composition of thoracic and abdominal aortic segments are already present to some degree at birth [6]. The number of lamellar units present at birth remains almost constant in the first decade of life, then increases progressively in adulthood, doubling in the thoracic aorta (from 25–30 units to approximately 56 units in the adult), while it increases less (from 15–20 units to approximately 28 units in the adult) in the abdominal aorta [29]. BP level may be an important mechanical factor influencing the relative degree of lamellar growth during the first years of life and in childhood [29,30]. Collagen is continuously degraded and deposited in a process of homeostatic regulation [31]. An increase in BP, directly or indirectly, provides the stimulus for the elaboration of fibrous collagen proteins in the arterial wall [29], in order to counterbalance the resulting transmural pressure increase [2]. The higher synthesis of collagen fibers induced by high BP values, therefore, causes an imbalance in the elastin−collagen ratio of the arterial wall, determining a condition of aortic stiffening. This action of BP on the viscoelastic properties of the aorta explains how, in our population of children and adolescents with cardiovascular risk factors, the indexed values (z-scores) of systolic and diastolic BP and heart rate were independently associated with aortic stiffness, confirming what is already widely known in the youth [32,33] and in adult population [3,11].
A condition of aortic stiffness has been described even in metabolic diseases such as diabetes [34], fatty liver disease [35,36,37], kidney failure [12,38,39], and alterations in calcium metabolism [40,41]. Some metabolic disorders can be accompanied by an increase in oxidative stress, arterial medial calcifications, and by inflammation of the arterial wall [42]. Inflammation causes both arterial stiffening and endothelial dysfunction [43]. There is no agreement in the literature regarding the relationship between BMI and vascular stiffness in children and adolescents. Some data suggest that there is no influence of excess weight on cf-PWV [33,44], while others go in the opposite direction [45,46]. Some authors have also suggested that in obese adolescents, there is an inverse correlation between cf-PWV and BMI values. On the other hand, several studies show a close relationship between insulin resistance and arterial stiffness in children and adolescents [44,47,48,49], and this suggests that excess weight and visceral fat (related to insulin resistance) may be associated with different effects on arterial viscoelasticity, although not all authors agree on this point [50]. Our study did not show an association between cf-PWV and BMI. However, we found a significant relationship between cf-PWV and WtHr. This result is interesting, because it suggests that, for the same weight class, a greater quantity of visceral fat could lead to a more severe clinical picture, presumably related to the production of cytokines, which would induce endothelial dysfunction through an increase in oxidative stress and trigger an inflammatory process that would lead to early vascular damage [51,52]. As there is a strong relationship between central obesity and insulin resistance already in childhood [53] and the cytokines produced by visceral fat can influence BP values in children [54], it is difficult to distinguish the role of insulin resistance and/or visceral obesity when determining the viscoelastic properties of the aorta.
4.2. Upper Limb Pulse Wave Velocity
Along the arterial tree there is a functional diversification that corresponds to a progressive change in the composition of the arterial wall. The aorta and large elastic arteries have the characteristic lamellar structure with layers of elastin interdigitated by layers of collagen and vascular smooth muscle. These arteries contribute to the buffering function and ensure the Windkessel effect. Progressing towards the periphery of the vascular system, the arteries lose their lamellar elastic structure and evolve into muscular-type arteries with a decrease in elastin and a predominance of smooth muscle cells.
This distinction between elastic and muscular vessels is particularly important from a clinical point of view, as, if high cf-PWV values are correlated with a high cardiovascular risk, no relationship between cr-PWV and the incidence of cardiovascular disease has been demonstrated [12,13].
In healthy young subjects, the autonomic nervous system does not have a pressure-independent role in the regulation of the large elastic central arteries [55], which are little or not at all innervated by the sympathetic system [56]. On the contrary, the distal segments of the arterial tree (“muscular” arteries) are more muscular [57] and densely innervated [58,59], thus being particularly sensitive to the activity of the sympathetic system [60]. Thus, the stiffness of muscular arteries appears to be mediated by tonic levels of sympathetic activity [61]. The results of our study are in agreement with these pathophysiological premises, as upper limb PWV was independently associated with z-score of diastolic BP and heart rate, resulting from a condition of sympathetic activation.
In agreement with other studies in humans [62,63], the HOMA index (indicative of insulin resistance) also had a significant association with cr-PWV. Given the condition of sympathetic activation associated with insulin resistance, this finding also appears likely to be induced by sympathetic activity. The interpretation of data on the relationship between insulin resistance and PWV in the two vascular districts is complex. From our results, it would appear that insulin resistance has a greater role in determining carotid-radial stiffness than carotid-femoral stiffness, which, conversely, would be more influenced by central obesity. However, these findings should be interpreted with due caution and would need to be confirmed by additional studies.
4.3. Arterial Stiffness and Glomerular Filtration Rate
Arterial stiffness is increased in children with chronic kidney disease [64]. All children and adolescents in our study population had normal renal function. However, there was a strong inverse association between eGFR values and both cf-PWV and cr-PWV. This finding may suggest that, despite the absence of renal disease, a higher filtration rate leads to better vascular compliance. We can only speculate on the possible mechanisms behind these findings. One possibility could be that children with a higher eGFR have a smaller intravascular volume and that this may contribute to an increased vascular stiffness. Further studies are needed to test this hypothesis.
4.4. Study Limitations and Strenghts
While our results are supported by the consistent number of children and adolescents at increased cardiovascular risk that we were able to include in our paper, we have to acknowledge a limitation of our study, related to the fact that we were able to collect only cross-sectional data. Indeed, our hypotheses on the mechanisms behind our findings would need longitudinal data to be tested and confirmed. However, we believe that our results are, nevertheless, important, because they pave the way for such future longitudinal evaluations.
5. Conclusions
PWVs of the aorta and upper limb have different regulatory mechanisms and clinical significance. If the viscoelastic properties of the aorta are linked to blood pressure, heart rate and visceral fat, on the other hand the distensibility of the muscular arteries of the upper limbs seems to be mainly influenced by the sympathetic system in our population of children at increased cardiovascular risk.
Further longitudinal studies are needed to clarify the prognostic significance of elevated cf-PWV and cr-PWV values in childhood and adolescence, as well as their possible role in the pathogenesis of arterial hypertension.
Author Contributions
Conceptualization, S.G. and P.S.; methodology, S.G. and P.S.; data collection, G.L., A.O., M.G. and I.P.; data analysis, E.T., L.A., S.G., P.S. and G.P.; formal analysis, E.T. and L.A.; investigation, G.L., A.O., M.G. and I.P; writing—original draft preparation, S.G., P.S. and G.P.; writing—review and editing, S.G., P.S. and G.P.; supervision, S.G., P.S. and G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Italian Ministry of Health (“Ricerca corrente”).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Local Institutional Ethics Committee (CPP Est III 15 December 2006).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy concerns.
Conflicts of Interest
P.S. has been involved as a consultant and expert witness in DiaTecne S.R.L. The other authors declare no conflict of interest.
References
- Bramwell, J.C.; Hill, A.V. Velocity of transmission of the pulse-wave and elasticity of the arteries. Lancet 1922, 1, 891–892. [Google Scholar] [CrossRef]
- Salvi, P. Pulse waves. In How Vascular Hemodynamics Affects Blood Pressure, 2nd ed.; Springer Nature: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [PubMed]
- Segers, P.; Chirinos, J.A. Arterial wall stiffness: Basic principles and methods of measurement in vivo. In Textbook of Arterial Stiffness and Pulsatile Hemodynamics in Health and Disease; Chirinos, J.A., Ed.; Academic Press: London, UK, 2022; Volume 1, pp. 111–124. [Google Scholar]
- Chirinos, J.A.; Segers, P.; Hughes, T.; Townsend, R. Large-Artery Stiffness in Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1237–1263. [Google Scholar] [CrossRef] [PubMed]
- Wahart, A.; Bennasroune, A.; Schmelzer, C.E.H.; Laffargue, M.; Blaise, S.; Romier-Crouzet, B.; Sartelet, H.; Martiny, L.; Gillery, P.; Jaisson, S.; et al. Role of elastin and elastin-derived peptides in arterial stiffness: From synthesis to potential therapeutic interventions. In Hemodynamic Determinants of Myocardial Oxygen Demand and Supply; Chirinos, J.A., Ed.; Elsevier: Amsterdam, The Netherlands; Academic Press: London, UK, 2022; Volume 1, pp. 299–314. [Google Scholar]
- Giudici, A.; Wilkinson, I.B.; Khir, A.W. Review of the Techniques Used for Investigating the Role Elastin and Collagen Play in Arterial Wall Mechanics. IEEE Rev. Biomed. Eng. 2021, 14, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Cocciolone, A.J.; Hawes, J.Z.; Staiculescu, M.C.; Johnson, E.O.; Murshed, M.; Wagenseil, J.E. Elastin, arterial mechanics, and cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H189–H205. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.W.; O’Rourke, M.; Edelman, E.R.; Vlachopoulos, C. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles, 7th ed.; CRC Press: Boca Raton, FL, USA, 2022. [Google Scholar]
- Wahart, A.; Hocine, T.; Albrecht, C.; Henry, A.; Sarazin, T.; Martiny, L.; El Btaouri, H.; Maurice, P.; Bennasroune, A.; Romier-Crouzet, B.; et al. Role of elastin peptides and elastin receptor complex in metabolic and cardiovascular diseases. FEBS J. 2019, 286, 2980–2993. [Google Scholar] [CrossRef] [PubMed]
- Reference Values for Arterial Stiffness, C. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: ‘establishing normal and reference values’. Eur. Heart J. 2010, 31, 2338–2350. [Google Scholar] [CrossRef]
- Pannier, B.; Guerin, A.P.; Marchais, S.J.; Safar, M.E.; London, G.M. Stiffness of capacitive and conduit arteries: Prognostic significance for end-stage renal disease patients. Hypertension 2005, 45, 592–596. [Google Scholar] [CrossRef]
- Van Sloten, T.T.; Schram, M.T.; van den Hurk, K.; Dekker, J.M.; Nijpels, G.; Henry, R.M.; Stehouwer, C.D. Local stiffness of the carotid and femoral artery is associated with incident cardiovascular events and all-cause mortality: The Hoorn study. J. Am. Coll. Cardiol. 2014, 63, 1739–1747. [Google Scholar] [CrossRef]
- Ashwell, M.; Gibson, S. Waist-to-height ratio as an indicator of ‘early health risk’: Simpler and more predictive than using a ‘matrix’ based on BMI and waist circumference. BMJ Open 2016, 6, e010159. [Google Scholar] [CrossRef]
- Peterson, K.; Savoie Roskos, M. Weight Bias: A Narrative Review of the Evidence, Assumptions, Assessment, and Recommendations for Weight Bias in Health Care. Health Educ. Behav. 2023, 50, 517–528. [Google Scholar] [CrossRef] [PubMed]
- CDC. Centers for Disease Control and Prevention. Clinical Growth Charts. Available online: https://www.cdc.gov/growthcharts/clinical_charts.htm (accessed on 20 June 2023).
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in the pattern of pubertal changes in boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in, C. Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar] [CrossRef]
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Haycock, G.B.; Edelmann, C.M., Jr.; Spitzer, A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 1976, 58, 259–263. [Google Scholar] [CrossRef]
- Salvi, P.; Safar, M.E.; Parati, G. Arterial applanation tonometry: Technical aspects relevant for its daily clinical use. J. Hypertens. 2013, 31, 469–471. [Google Scholar] [CrossRef]
- Salvi, P.; Lio, G.; Labat, C.; Ricci, E.; Pannier, B.; Benetos, A. Validation of a new non-invasive portable tonometer for determining arterial pressure wave and pulse wave velocity: The PulsePen device. J. Hypertens. 2004, 22, 2285–2293. [Google Scholar] [CrossRef]
- Salvi, P.; Scalise, F.; Rovina, M.; Moretti, F.; Salvi, L.; Grillo, A.; Gao, L.; Baldi, C.; Faini, A.; Furlanis, G.; et al. Noninvasive Estimation of Aortic Stiffness Through Different Approaches. Hypertension 2019, 74, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Joly, L.; Perret-Guillaume, C.; Kearney-Schwartz, A.; Salvi, P.; Mandry, D.; Marie, P.Y.; Karcher, G.; Rossignol, P.; Zannad, F.; Benetos, A. Pulse wave velocity assessment by external noninvasive devices and phase-contrast magnetic resonance imaging in the obese. Hypertension 2009, 54, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Reusz, G.S.; Cseprekal, O.; Temmar, M.; Kis, E.; Cherif, A.B.; Thaleb, A.; Fekete, A.; Szabo, A.J.; Benetos, A.; Salvi, P. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension 2010, 56, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Wolinsky, H. Comparison of medial growth of human thoracic and abdominal aortas. Circ. Res. 1970, 27, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Naeye, R.L. Arterial changes during the perinatal period. Arch. Pathol. 1961, 71, 121–128. [Google Scholar] [PubMed]
- Humphrey, J.D. Vascular adaptation and mechanical homeostasis at tissue, cellular, and sub-cellular levels. Cell. Biochem. Biophys. 2008, 50, 53–78. [Google Scholar] [CrossRef] [PubMed]
- Lurbe, E.; Torro, I.; Garcia-Vicent, C.; Alvarez, J.; Fernandez-Fornoso, J.A.; Redon, J. Blood pressure and obesity exert independent influences on pulse wave velocity in youth. Hypertension 2012, 60, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Salvi, P.; Nava, E.; Tassistro, E.; Giussani, M.; Desimone, I.; Orlando, A.; Battaglino, M.; Lieti, G.; Montemerlo, M.; et al. Blood Pressure and Body Weight Have Different Effects on Pulse Wave Velocity and Cardiac Mass in Children. J. Clin. Med. 2020, 9, 2954. [Google Scholar] [CrossRef]
- Christoforidis, A.; Georeli, I.; Dimitriadou, M.; Galli-Tsinopoulou, A.; Stabouli, S. Arterial stiffness indices in children and adolescents with type 1 diabetes mellitus: A meta-analysis. Diabetes Metab. Res. Rev. 2022, 38, e3555. [Google Scholar] [CrossRef]
- Salvi, P.; Ruffini, R.; Agnoletti, D.; Magnani, E.; Pagliarani, G.; Comandini, G.; Pratico, A.; Borghi, C.; Benetos, A.; Pazzi, P. Increased arterial stiffness in nonalcoholic fatty liver disease: The Cardio-GOOSE study. J. Hypertens 2010, 28, 1699–1707. [Google Scholar] [CrossRef]
- Jaruvongvanich, V.; Chenbhanich, J.; Sanguankeo, A.; Rattanawong, P.; Wijarnpreecha, K.; Upala, S. Increased arterial stiffness in nonalcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2017, 29, e28–e35. [Google Scholar] [CrossRef] [PubMed]
- Sunbul, M.; Agirbasli, M.; Durmus, E.; Kivrak, T.; Akin, H.; Aydin, Y.; Ergelen, R.; Yilmaz, Y. Arterial stiffness in patients with non-alcoholic fatty liver disease is related to fibrosis stage and epicardial adipose tissue thickness. Atherosclerosis 2014, 237, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Kouis, P.; Kousios, A.; Kanari, A.; Kleopa, D.; Papatheodorou, S.I.; Panayiotou, A.G. Association of non-invasive measures of subclinical atherosclerosis and arterial stiffness with mortality and major cardiovascular events in chronic kidney disease: Systematic review and meta-analysis of cohort studies. Clin. Kidney J. 2020, 13, 842–854. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R.; Anderson, A.H.; Chirinos, J.A.; Feldman, H.I.; Grunwald, J.E.; Nessel, L.; Roy, J.; Weir, M.R.; Wright, J.T., Jr.; Bansal, N.; et al. Association of Pulse Wave Velocity with Chronic Kidney Disease Progression and Mortality: Findings from the CRIC Study (Chronic Renal Insufficiency Cohort). Hypertension 2018, 71, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Bellasi, A.; Raggi, P. Vascular calcification in chronic kidney disease: Usefulness of a marker of vascular damage. J. Nephrol. 2011, 24 (Suppl. 18), S11–S15. [Google Scholar] [CrossRef] [PubMed]
- Raggi, P.; Bellasi, A.; Ferramosca, E.; Islam, T.; Muntner, P.; Block, G.A. Association of pulse wave velocity with vascular and valvular calcification in hemodialysis patients. Kidney Int. 2007, 71, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Sequi-Dominguez, I.; Cavero-Redondo, I.; Alvarez-Bueno, C.; Saz-Lara, A.; Mesas, A.E.; Martinez-Vizcaino, V. Association between arterial stiffness and the clustering of metabolic syndrome risk factors: A systematic review and meta-analysis. J. Hypertens. 2021, 39, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.M.; Reesink, K.D.; Ghiadoni, L. Advances in the non-invasive assessment of vascular dysfunction in metabolic syndrome and diabetes: Focus on endothelium, carotid mechanics and renal vessels. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 121–128. [Google Scholar] [CrossRef]
- Pucci, G.; Martina, M.R.; Bianchini, E.; D’Abbondanza, M.; Curcio, R.; Battista, F.; Anastasio, F.; Crapa, M.E.; Sanesi, L.; Gemignani, V.; et al. Relationship between measures of adiposity, blood pressure and arterial stiffness in adolescents. The MACISTE study. J. Hypertens 2023, 41, 1100–1107. [Google Scholar] [CrossRef]
- Urbina, E.M.; Kimball, T.R.; Khoury, P.R.; Daniels, S.R.; Dolan, L.M. Increased arterial stiffness is found in adolescents with obesity or obesity-related type 2 diabetes mellitus. J. Hypertens 2010, 28, 1692–1698. [Google Scholar] [CrossRef]
- Koopman, L.P.; McCrindle, B.W.; Slorach, C.; Chahal, N.; Hui, W.; Sarkola, T.; Manlhiot, C.; Jaeggi, E.T.; Bradley, T.J.; Mertens, L. Interaction between myocardial and vascular changes in obese children: A pilot study. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2012, 25, 401–410.e401. [Google Scholar] [CrossRef]
- Correia-Costa, A.; Correia-Costa, L.; Caldas Afonso, A.; Schaefer, F.; Guerra, A.; Moura, C.; Mota, C.; Barros, H.; Areias, J.C.; Azevedo, A. Determinants of carotid-femoral pulse wave velocity in prepubertal children. Int. J. Cardiol. 2016, 218, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Moreno, M.I.; Vilches-Perez, A.; Gallardo-Escribano, C.; Vargas-Candela, A.; Lopez-Carmona, M.D.; Perez-Belmonte, L.M.; Ruiz-Moreno, A.; Gomez-Huelgas, R.; Bernal-Lopez, M.R. Metabolically Healthy Obesity: Presence of Arterial Stiffness in the Prepubescent Population. Int. J. Environ. Res. Public Health 2020, 17, 96995. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Montelisciani, L.; Viazzi, F.; Giussani, M.; Lieti, G.; Patti, I.; Orlando, A.; Antolini, L.; Salvi, P.; Parati, G. Uric acid and arterial stiffness in children and adolescents: Role of insulin resistance and blood pressure. Front. Cardiovasc. Med. 2022, 9, 978366. [Google Scholar] [CrossRef] [PubMed]
- Hvidt, K.N.; Olsen, M.H.; Holm, J.C.; Ibsen, H. Obese children and adolescents have elevated nighttime blood pressure independent of insulin resistance and arterial stiffness. Am. J. Hypertens. 2014, 27, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Lorincz, H.; Somodi, S.; Ratku, B.; Harangi, M.; Paragh, G. Crucial Regulatory Role of Organokines in Relation to Metabolic Changes in Non-Diabetic Obesity. Metabolites 2023, 13, 270. [Google Scholar] [CrossRef] [PubMed]
- Dangardt, F.; Charakida, M.; Georgiopoulos, G.; Chiesa, S.T.; Rapala, A.; Wade, K.H.; Hughes, A.D.; Timpson, N.J.; Pateras, K.; Finer, N.; et al. Association between fat mass through adolescence and arterial stiffness: A population-based study from The Avon Longitudinal Study of Parents and Children. Lancet Child. Adolesc. Health 2019, 3, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Brambilla, P.; Giussani, M.; Galbiati, S.; Mastriani, S.; Pieruzzi, F.; Stella, A.; Valsecchi, M.G.; Antolini, L. Insulin resistance, prehypertension, hypertension and blood pressure values in paediatric age. J. Hypertens 2012, 30, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Antolini, L.; Street, M.E.; Giussani, M.; Galbiati, S.; Valsecchi, M.G.; Stella, A.; Zuccotti, G.V.; Bernasconi, S.; Genovesi, S. Adiponectin and hypertension in normal-weight and obese children. Am. J. Hypertens. 2013, 26, 257–264. [Google Scholar] [CrossRef]
- Maki-Petaja, K.M.; Barrett, S.M.; Evans, S.V.; Cheriyan, J.; McEniery, C.M.; Wilkinson, I.B. The Role of the Autonomic Nervous System in the Regulation of Aortic Stiffness. Hypertension 2016, 68, 1290–1297. [Google Scholar] [CrossRef]
- Grassi, G.; Giannattasio, C.; Failla, M.; Pesenti, A.; Peretti, G.; Marinoni, E.; Fraschini, N.; Vailati, S.; Mancia, G. Sympathetic modulation of radial artery compliance in congestive heart failure. Hypertension 1995, 26, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Shadwick, R.E. Mechanical design in arteries. J. Exp. Biol. 1999, 202, 3305–3313. [Google Scholar] [CrossRef] [PubMed]
- Kienecker, E.W.; Knoche, H. Sympathetic innervation of the pulmonary artery, ascending aorta, and coronar glomera of the rabbit. A fluorescence microscopic study. Cell Tissue Res. 1978, 188, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Tebbs, B.T. The Sympathetic Innervation of the Aorta and Intercostal Arteries. J. Anat. Physiol. 1898, 32, 308–311. [Google Scholar] [PubMed]
- Peterson, L.H. Regulation of blood vessels. Circulation 1960, 21, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Failla, M.; Grappiolo, A.; Emanuelli, G.; Vitale, G.; Fraschini, N.; Bigoni, M.; Grieco, N.; Denti, M.; Giannattasio, C.; Mancia, G. Sympathetic tone restrains arterial distensibility of healthy and atherosclerotic subjects. J. Hypertens 1999, 17, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Webb, D.R.; Khunti, K.; Silverman, R.; Gray, L.J.; Srinivasan, B.; Lacy, P.S.; Williams, B.; Davies, M.J. Impact of metabolic indices on central artery stiffness: Independent association of insulin resistance and glucose with aortic pulse wave velocity. Diabetologia 2010, 53, 1190–1198. [Google Scholar] [CrossRef]
- Emoto, M.; Nishizawa, Y.; Kawagishi, T.; Maekawa, K.; Hiura, Y.; Kanda, H.; Izumotani, K.; Shoji, T.; Ishimura, E.; Inaba, M.; et al. Stiffness indexes beta of the common carotid and femoral arteries are associated with insulin resistance in NIDDM. Diabetes Care 1998, 21, 1178–1182. [Google Scholar] [CrossRef]
- Azukaitis, K.; Kirchner, M.; Doyon, A.; Litwin, M.; Bayazit, A.; Duzova, A.; Canpolat, N.; Jankauskiene, A.; Shroff, R.; Melk, A.; et al. Arterial Stiffness and Chronic Kidney Disease Progression in Children. Clin. J. Am. Soc. Nephrol. 2022, 17, 1467–1476. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).