
The Role of Electrocardiographic Markers for Predicting Atrial Fibrillation in Patients with Acute Ischemic Stroke: Data from the BIOSIGNAL Cohort Study
 , ,
, ,  , , and
, , and
Abstract
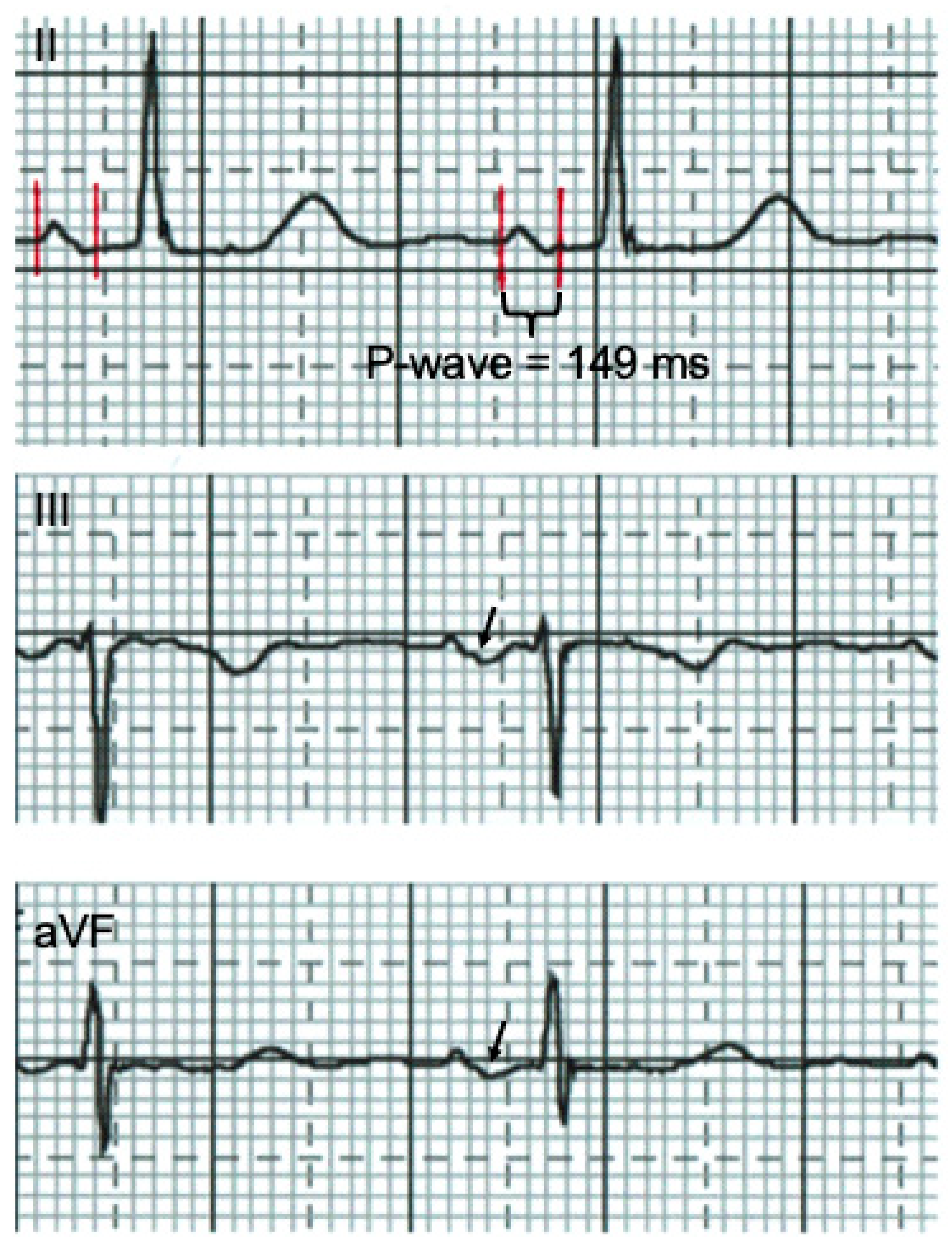
:- Advanced interatrial block (aIAB) and PR duration determined on 12-lead surface ECG in lead II are independently associated with newly diagnosed atrial fibrillation in patients with acute ischemic stroke.
- aIAB significantly improved risk stratification beyond established risk factors.
- aIAB is an easily measurable ECG marker and has a high inter-rater reliability.
- Therefore, aIAB may help refine diagnostic work-up to search for atrial fibrillation in patients with acute ischemic stroke.
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. ECG Parameters
2.3. Echocardiographic Parameters
2.4. Biomarker Measurement
2.5. Outcome Variable
2.6. Inter-Rater Reliability of the ECG Markers
2.7. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Inter-Rater Reliability for ECG Parameters
3.3. Association of PTFV1 and PR Interval with NDAF
3.4. Association of aIAB with NDAF
3.5. Association of MR-proANP and LAESD with NDAF
4. Discussion
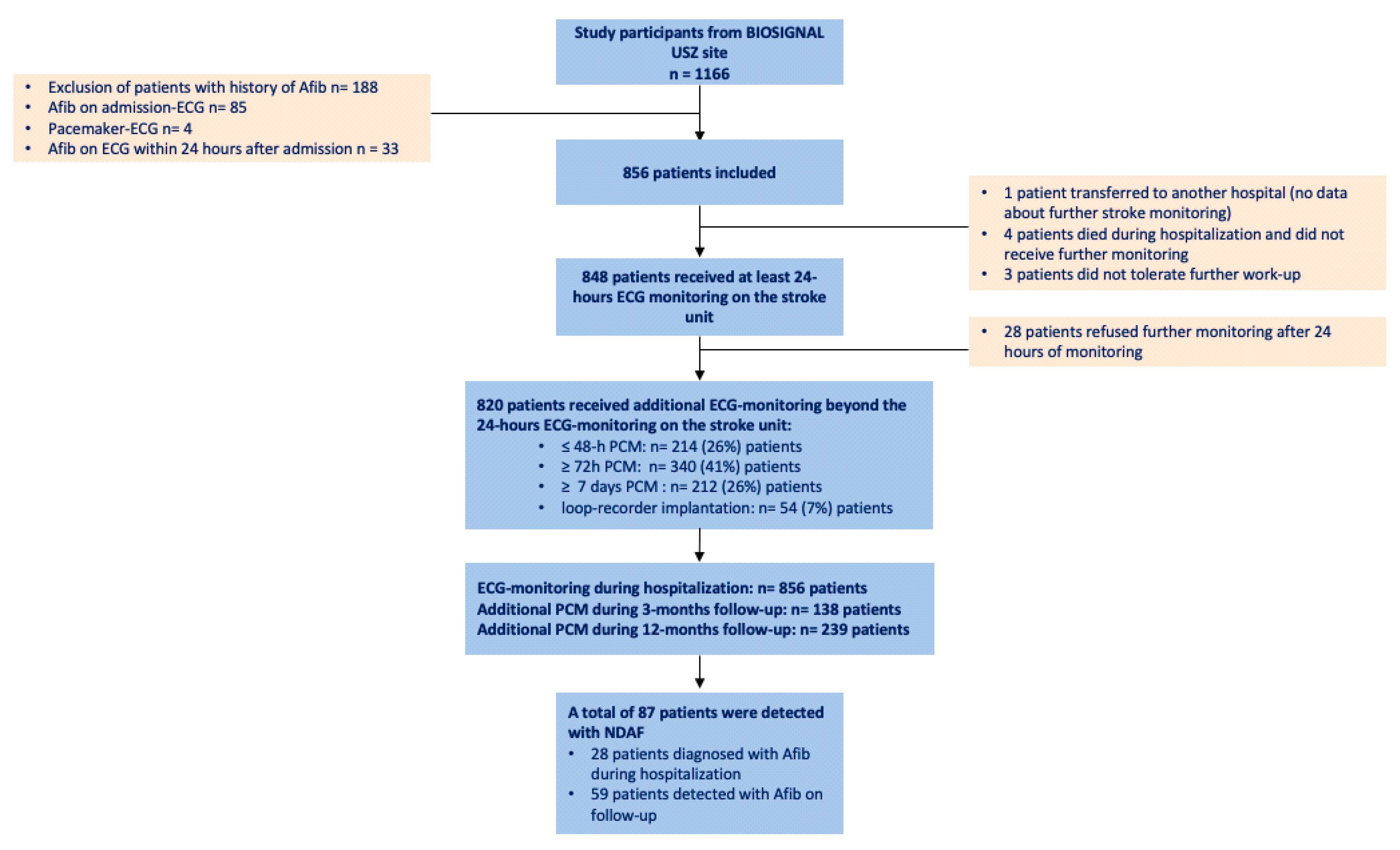
- NDAF was detected in 10% during follow-up after the index AIS. This finding is similar to other studies in the field, such as Find AF and CRYSTAL AF, with 5–12% within one year of follow-up, depending on the electrocardiographic monitoring method [24,25]. However, Find AF did not include patients with severe ipsilateral carotid or intracranial artery stenosis, and Crystal AF only included cryptogenic strokes compared to our cohort of unselected stroke patients, suggesting that the rate of NDAF is likely independent of initial stroke etiology.
- The presence of aIAB, an easy-to-measure and robust 12-lead ECG parameter reflecting atrial electrical activation delay, performed best from all electrocardiographic P-wave markers and was independently associated with NDAF in multivariable analysis. Adding aIAB to the regression model, including known risk factors and LAESD, improved the discriminatory accuracy of the model to predict NDAF.
4.1. Previous Literature on aIAB
4.2. Previous Literature on PR Interval and PTFV1
4.3. Manual Measurement of P-Wave Indices in the Era of Artificial Intelligence (AI)
4.4. Clinical Consequences of Detecting AF in Patients with AIS during Follow-Up
4.5. Previous Literature on MR-proANP
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendieta, G.; Guasch, E.; Weir, D.; Aristizabal, D.; Escobar-Robledo, L.A.; Llull, L.; Mont, L.; Bayes de Luna, A.; Sitges, M. Advanced interatrial block: A predictor of covert atrial fibrillation in embolic stroke of undetermined source. J. Electrocardiol. 2020, 58, 113–118. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, W.T.; Kamel, H.; Zhang, Z.M.; Chen, L.Y.; Alonso, A.; Soliman, E.Z. Advanced interatrial block and ischemic stroke: The Atherosclerosis Risk in Communities Study. Neurology 2016, 87, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Soliman, E.Z.; Prineas, R.J.; Case, L.D.; Zhang, Z.M.; Goff, D.C., Jr. Ethnic distribution of ECG predictors of atrial fibrillation and its impact on understanding the ethnic distribution of ischemic stroke in the Atherosclerosis Risk in Communities (ARIC) study. Stroke 2009, 40, 1204–1211. [Google Scholar] [CrossRef]
- Kamel, H.; Bartz, T.M.; Elkind, M.S.V.; Okin, P.M.; Thacker, E.L.; Patton, K.K.; Stein, P.K.; deFilippi, C.R.; Gottesman, R.F.; Heckbert, S.R.; et al. Atrial Cardiopathy and the Risk of Ischemic Stroke in the CHS (Cardiovascular Health Study). Stroke 2018, 49, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Selles, M.; Elosua, R.; Ibarrola, M.; de Andres, M.; Diez-Villanueva, P.; Bayes-Genis, A.; Baranchuk, A.; Bayes-de-Luna, A.; Investigators, B.R. Advanced interatrial block and P-wave duration are associated with atrial fibrillation and stroke in older adults with heart disease: The BAYES registry. Europace 2020, 22, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Acampa, M.; Lazzerini, P.E.; Guideri, F.; Tassi, R.; Lo Monaco, A.; Martini, G. Inflammation and Atrial Electrical Remodelling in Patients With Embolic Strokes of Undetermined Source. Heart Lung Circ. 2019, 28, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Kamel, H.; O’Neal, W.T.; Okin, P.M.; Loehr, L.R.; Alonso, A.; Soliman, E.Z. Electrocardiographic left atrial abnormality and stroke subtype in the atherosclerosis risk in communities study. Ann. Neurol. 2015, 78, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Thijs, V.N.; Brachmann, J.; Morillo, C.A.; Passman, R.S.; Sanna, T.; Bernstein, R.A.; Diener, H.C.; Di Lazzaro, V.; Rymer, M.M.; Hogge, L.; et al. Predictors for atrial fibrillation detection after cryptogenic stroke: Results from CRYSTAL AF. Neurology 2016, 86, 261–269. [Google Scholar] [CrossRef]
- Baranchuk, A.; Torner, P.; de Luna, A.B. Bayes Syndrome: What Is It? Circulation 2018, 137, 200–202. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, X.; Jing, J.; Meng, X.; Li, Z.; Pan, Y.; Jiang, Y.; Yan, H.; Huang, X.; Liu, L.; et al. Prognostic significance of atrial cardiopathy in patients with acute ischemic stroke. Eur. Stroke J. 2023, 8, 183–190. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the Management of Atrial Fibrillation Developed in Collaboration With EACTS. Rev. Esp. Cardiol. (Engl. Ed.) 2017, 70, 50. [Google Scholar] [CrossRef] [PubMed]
- Uphaus, T.; Weber-Kruger, M.; Grond, M.; Toenges, G.; Jahn-Eimermacher, A.; Jauss, M.; Kirchhof, P.; Wachter, R.; Groschel, K. Development and validation of a score to detect paroxysmal atrial fibrillation after stroke. Neurology 2019, 92, e115–e124. [Google Scholar] [CrossRef] [PubMed]
- Hatano, S. Experience from a multicentre stroke register: A preliminary report. Bull. World Health Organ. 1976, 54, 541–553. [Google Scholar]
- Goldstein, L.B.; Samsa, G.P.; Matchar, D.B.; Horner, R.D. Charlson Index comorbidity adjustment for ischemic stroke outcome studies. Stroke 2004, 35, 1941–1945. [Google Scholar] [CrossRef] [PubMed]
- Bayes de Luna, A.; Platonov, P.; Cosio, F.G.; Cygankiewicz, I.; Pastore, C.; Baranowski, R.; Bayes-Genis, A.; Guindo, J.; Vinolas, X.; Garcia-Niebla, J.; et al. Interatrial blocks. A separate entity from left atrial enlargement: A consensus report. J. Electrocardiol. 2012, 45, 445–451. [Google Scholar] [CrossRef]
- Acampa, M.; Lazzerini, P.E.; Guideri, F.; Tassi, R.; Andreini, I.; Domenichelli, C.; Cartocci, A.; Martini, G. Electrocardiographic Predictors of Silent Atrial Fibrillation in Cryptogenic Stroke. Heart Lung Circ. 2019, 28, 1664–1669. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Struck, J.; Thomas, B.; Bergmann, A. Immunoluminometric assay for the midregion of pro-atrial natriuretic peptide in human plasma. Clin. Chem. 2004, 50, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, J.; Arnold, M.; Konig, I.R.; Bicvic, A.; Westphal, L.P.; Schutz, V.; Inauen, C.; Scherrer, N.; Luft, A.; Galovic, M.; et al. Measurement of Midregional Pro-Atrial Natriuretic Peptide to Discover Atrial Fibrillation in Patients With Ischemic Stroke. J. Am. Coll. Cardiol. 2022, 79, 1369–1381. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Weber-Kruger, M.; Gelbrich, G.; Stahrenberg, R.; Liman, J.; Kermer, P.; Hamann, G.F.; Seegers, J.; Groschel, K.; Wachter, R.; Find, A.F.i. Finding atrial fibrillation in stroke patients: Randomized evaluation of enhanced and prolonged Holter monitoring--Find-AF(RANDOMISED)—Rationale and design. Am. Heart J. 2014, 168, 438–445.e1. [Google Scholar] [CrossRef] [PubMed]
- Sanna, T.; Diener, H.-C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.A.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic Stroke and Underlying Atrial Fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef] [PubMed]
- Benito, E.M.; De Luna, A.B.; Baranchuk, A.; Mont, L. Extensive atrial fibrosis assessed by late gadolinium enhancement cardiovascular magnetic resonance associated with advanced interatrial block electrocardiogram pattern. Europace 2017, 19, 377. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Josephson, M.E.; Hauser, T.H.; O’Halloran, T.D.; Agarwal, A.; Manning, W.J.; Yeon, S.B. Accuracy of electrocardiographic criteria for atrial enlargement: Validation with cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2008, 10, 7. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Longstreth, W.T., Jr.; Elkind, M.S.; Soliman, E.Z. Atrial cardiopathy: A broadened concept of left atrial thromboembolism beyond atrial fibrillation. Future Cardiol. 2015, 11, 323–331. [Google Scholar] [CrossRef]
- Kamel, H.; Okin, P.M.; Elkind, M.S.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke: Time for a New Model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef]
- Lebek, S.; Wester, M.; Pec, J.; Poschenrieder, F.; Tafelmeier, M.; Fisser, C.; Provaznik, Z.; Schopka, S.; Debl, K.; Schmid, C.; et al. Abnormal P-wave terminal force in lead V1 is a marker for atrial electrical dysfunction but not structural remodelling. ESC Heart Fail. 2021, 8, 4055–4066. [Google Scholar] [CrossRef]
- Maheshwari, A.; Norby, F.L.; Roetker, N.S.; Soliman, E.Z.; Koene, R.J.; Rooney, M.R.; O’Neal, W.T.; Shah, A.M.; Claggett, B.L.; Solomon, S.D.; et al. Refining Prediction of Atrial Fibrillation-Related Stroke Using the P2-CHA2DS2-VASc Score. Circulation 2019, 139, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J.; et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Glotzer, T.V.; Daoud, E.G.; Wyse, D.G.; Singer, D.E.; Ezekowitz, M.D.; Hilker, C.; Miller, C.; Qi, D.; Ziegler, P.D. The relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: The TRENDS study. Circ. Arrhythm. Electrophysiol. 2009, 2, 474–480. [Google Scholar] [CrossRef]
- Turakhia, M.P.; Ziegler, P.D.; Schmitt, S.K.; Chang, Y.; Fan, J.; Than, C.T.; Keung, E.K.; Singer, D.E. Atrial Fibrillation Burden and Short-Term Risk of Stroke: Case-Crossover Analysis of Continuously Recorded Heart Rhythm from Cardiac Electronic Implanted Devices. Circ. Arrhythm. Electrophysiol. 2015, 8, 1040–1047. [Google Scholar] [CrossRef]
- Sposato, L.A.; Chaturvedi, S.; Hsieh, C.Y.; Morillo, C.A.; Kamel, H. Atrial Fibrillation Detected After Stroke and Transient Ischemic Attack: A Novel Clinical Concept Challenging Current Views. Stroke 2022, 53, e94–e103. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Fluri, F.; Schuetz, P.; Morgenthaler, N.G.; Zweifel, C.; Bingisser, R.; Kappos, L.; Steck, A.; Engelter, S.T.; Muller, B.; et al. Midregional pro-atrial natriuretic peptide and outcome in patients with acute ischemic stroke. J. Am. Coll. Cardiol. 2010, 56, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Moon, Y.; von Eckardstein, A.; Spanaus, K.; DeRosa, J.; Gutierrez, J.; DeCarli, C.; Wright, C.; Sacco, R.; Elkind, M. Procalcitonin and Midregional Proatrial Natriuretic Peptide as Biomarkers of Subclinical Cerebrovascular Damage: The Northern Manhattan Study. Stroke 2017, 48, 604–610. [Google Scholar] [CrossRef]
- Truong, Q.A.; Siegel, E.; Karakas, M.; Januzzi, J.L., Jr.; Bamberg, F.; Mahabadi, A.A.; Dasdemir, S.; Brady, T.J.; Bergmann, A.; Kunde, J.; et al. Relation of natriuretic peptides and midregional proadrenomedullin to cardiac chamber volumes by computed tomography in patients without heart failure: From the ROMICAT Trial. Clin. Chem. 2010, 56, 651–660. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Leip, E.P.; Omland, T.; Wolf, P.A.; Vasan, R.S. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N. Engl. J. Med. 2004, 350, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Perera, K.S.; Vanassche, T.; Bosch, J.; Swaminathan, B.; Mundl, H.; Giruparajah, M.; Barboza, M.A.; O’Donnell, M.J.; Gomez-Schneider, M.; Hankey, G.J.; et al. Global Survey of the Frequency of Atrial Fibrillation-Associated Stroke: Embolic Stroke of Undetermined Source Global Registry. Stroke 2016, 47, 2197–2202. [Google Scholar] [CrossRef] [PubMed]
- Mor-Avi, V.; Yodwut, C.; Jenkins, C.; Kuhl, H.; Nesser, H.J.; Marwick, T.H.; Franke, A.; Weinert, L.; Niel, J.; Steringer-Mascherbauer, R.; et al. Real-time 3D echocardiographic quantification of left atrial volume: Multicenter study for validation with CMR. JACC Cardiovasc. Imaging 2012, 5, 769–777. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total | No Atrial Fibrillation | NDAF | p-Value ** | |
|---|---|---|---|---|
| No. (%) | 856 | 769 | 87 | |
| Demographic data | ||||
| Age, median (IQR) | 70 (59–80) | 69 (57–79) | 77 (69–84) | <0.001 ** |
| Female sex, n (%) | 345 (40%) | 299 (39%) | 46 (53%) | 0.012 |
| Medical history | ||||
| Hypertension, n (%) | 593 (69%) | 531 (69%) | 62 (71%) | 0.67 |
| Smoking, n (%) | 249 (29%) | 231 (30%) | 18 (21%) | 0.074 |
| Diabetes mellitus, n (%) | 124 (14%) | 114 (15%) | 10 (11%) | 0.40 |
| Alcohol abuse, n (%) | 54 (6%) | 51 (7%) | 3 (4%) | 0.26 |
| Coronary heart disease, n (%) | 160 (19%) | 145 (19%) | 15 (17%) | 0.71 |
| Cardiac heart failure, n (%) | 24 (3%) | 20 (3%) | 4 (5%) | 0.28 |
| Dyslipidemia, n (%) | 621 (73%) | 555 (72%) | 66 (76%) | 0.46 |
| Family history of CV disease, n (%) | 122 (15%) | 109 (15%) | 13 (16%) | 0.74 |
| BMI > 30, n (%) | 127 (15%) | 112 (15%) | 15 (18%) | 0.50 |
| Previous stroke/TIA, n (%) | 121 (14%) | 111 (14%) | 10 (11%) | 0.46 |
| Peripheral vascular disease, n (%) | 125 (15%) | 115 (15%) | 10 (11%) | 0.39 |
| Stroke severity, n (%) | ||||
| Mild stroke (NIHSS ≤ 8) | 595 (70%) | 537 (70%) | 58 (67%) | 0.54 |
| Moderate stroke (NIHSS 9–15) | 161 (19%) | 146 (19%) | 15 (17%) | 0.69 |
| Severe stroke (NIHSS ≥ 16) | 100 (12%) | 86 (11%) | 14 (16%) | 0.18 |
| Stroke size (DWI), n (%) * | ||||
| Large Lesion | 93 (12%) | 81 (12%) | 12 (16%) | 0.31 |
| Medium Lesion | 309 (41%) | 274 (40%) | 35 (47%) | 0.30 |
| Small Lesion | 350 (47%) | 322 (48%) | 28 (37%) | 0.092 |
| Etiology (TOAST), n (%) | ||||
| Large artery atherosclerosis | 166 (19%) | 162 (21%) | 4 (5%) | <0.001 ** |
| Cardioembolism † | 103 (12%) | 79 (10%) | 24 (28%) | 0.31 |
| Small vessel disease | 123 (14%) | 119 (15%) | 4 (5%) | 0.006 |
| Other etiology | 76 (9%) | 73 (9%) | 3 (3%) | 0.060 |
| Unknown etiology | 389 (45%) | 337 (44%) | 52 (60%) | <0.005 |
| Scores | ||||
| AS5F | 67.5 (58.0–75.9) | 67.1 (57.3–75.4) | 73.6 (66.0–79.4) | <0.001 ** |
| CHADS-VASc-Score, median (IQR) | 2.0 (1.0–3.0) | 2.0 (1.0–3.0) | 2.0 (1.0–2.0) | 0.86 |
| ECG-Markers | ||||
| P-terminal force in V1 (µVxms), median (IQR) * | 3354 (2135–5015) | 3314 (2108–5006) | 3728 (2256–5166) | 0.29 |
| logP-terminal force in V1, median (IQR) | 3.5 (3.3–3.7) | 3.5 (3.3–3.7) | 3.6 (3.4–3.7) | 0.29 |
| PR interval, median (IQR) | 178 (162–198) | 177 (161–195) | 191 (175–212) | <0.001 ** |
| Advanced interatrial block, n (%) * | 222 (29%) | 172 (25%) | 50 (60%) | <0.001 ** |
| Echocardiographic parameters | ||||
| LAESD (cm), median (IQR) * | 3.8 (3.4–4.2) | 3.8 (3.3–4.1) | 4.1 (3.7–4.5) | <0.001 ** |
| LVEF in %, median (IQR) | 60 (56–64) | 60 (56–64) | 60 (56–63) | 0.59 |
| Laboratory values, median (IQR) | ||||
| MR-proANP (pmol/L) | 110.5 (70.4–182.6) | 106.5 (68.2–172.9) | 176.4 (106.2–262.6) | <0.001 ** |
| Univariate Analysis | ||
|---|---|---|
| Variables | OR | 95%-CI |
| aIAB (binary variable) | 4.45 | 2.78–7.12 |
| Model 1 | ||
| aIAB (binary variable) | 3.71 | 2.29–6.00 |
| AS5F per points | 1.01 | 0.99–1.04 |
| logMR-proANP (pmol/L) | 4.69 | 1.92–11.50 |
| Model 2 ‡ | ||
| aIAB (binary variable) | 3.81 | 2.33–6.23 |
| AS5F per points | 1.02 | 1.00–1.04 |
| logMR-proANP (pmol/L) | 3.99 | 1.57–10.15 |
| LAESD per cm | 1.63 | 1.06–2.50 |
| Large vessel stroke | 0.14 | 0.05–0.40 |
| Predictors | AUC | CI 95% | p-Value (LR-TEST) | cNRI |
|---|---|---|---|---|
| Model 1 without aIAB | 0.69 | (0.63–0.75) | - | - |
| Model 1 + aIAB | 0.76 | (0.71–0.81) | *** | 0.69 *** |
| Model 2 ‡ without aIAB | 0.78 | (0.77–0.80) | - | - |
| Model 2 ‡ + aIAB | 0.81 | (0.80–0.83) | *** | 0.66 *** |
| Model 1 + aIAB | 0.73 | (0.68–0.79) | - | - |
| Model 2 ‡ + aIAB | 0.82 | (0.80–0.83) | - | - |
| MR-proANP Cut Point | Sensitivity | Specificity | CC | LR + | LR − |
|---|---|---|---|---|---|
| ≥156 pmol/L | 56.32% | 70.89% | 69.40% | 1.93 | 0.61 |
| ≥200 pmol/L | 42.53% | 81.46% | 77.49% | 2.29 | 0.71 |
| ≥255 pmol/L | 26.44% | 89.16% | 82.77% | 2.44 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schütz, V.; Dougoud, S.; Bracher, K.; Arnold, M.; Schweizer, J.; Nakas, C.; Westphal, L.P.; Inauen, C.; Pokorny, T.; Duru, F.; et al. The Role of Electrocardiographic Markers for Predicting Atrial Fibrillation in Patients with Acute Ischemic Stroke: Data from the BIOSIGNAL Cohort Study. J. Clin. Med. 2023, 12, 6830. https://doi.org/10.3390/jcm12216830
Schütz V, Dougoud S, Bracher K, Arnold M, Schweizer J, Nakas C, Westphal LP, Inauen C, Pokorny T, Duru F, et al. The Role of Electrocardiographic Markers for Predicting Atrial Fibrillation in Patients with Acute Ischemic Stroke: Data from the BIOSIGNAL Cohort Study. Journal of Clinical Medicine. 2023; 12(21):6830. https://doi.org/10.3390/jcm12216830
Chicago/Turabian StyleSchütz, Valerie, Svetlana Dougoud, Katja Bracher, Markus Arnold, Juliane Schweizer, Christos Nakas, Laura P. Westphal, Corinne Inauen, Thomas Pokorny, Firat Duru, and et al. 2023. "The Role of Electrocardiographic Markers for Predicting Atrial Fibrillation in Patients with Acute Ischemic Stroke: Data from the BIOSIGNAL Cohort Study" Journal of Clinical Medicine 12, no. 21: 6830. https://doi.org/10.3390/jcm12216830
APA StyleSchütz, V., Dougoud, S., Bracher, K., Arnold, M., Schweizer, J., Nakas, C., Westphal, L. P., Inauen, C., Pokorny, T., Duru, F., Steffel, J., Luft, A., Spanaus, K., Saguner, A. M., & Katan, M. (2023). The Role of Electrocardiographic Markers for Predicting Atrial Fibrillation in Patients with Acute Ischemic Stroke: Data from the BIOSIGNAL Cohort Study. Journal of Clinical Medicine, 12(21), 6830. https://doi.org/10.3390/jcm12216830