

Technically Challenging Percutaneous Interventions of Chronic Total Occlusions Are Associated with Enhanced Platelet Activation

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Objectives
3. Patients and Methods
3.1. Patients
3.2. Blood Samples
3.3. Laboratory Analyses
3.3.1. Determination of Surface P-Selectin Expression on Platelets
3.3.2. Determination of Soluble P-Selectin Concentrations
3.3.3. RT-qPCR Analysis of Extracellular miRNAs
3.4. Statistical Analyses
3.5. Ethical Statement
4. Results
4.1. Baseline Characteristics of Patients
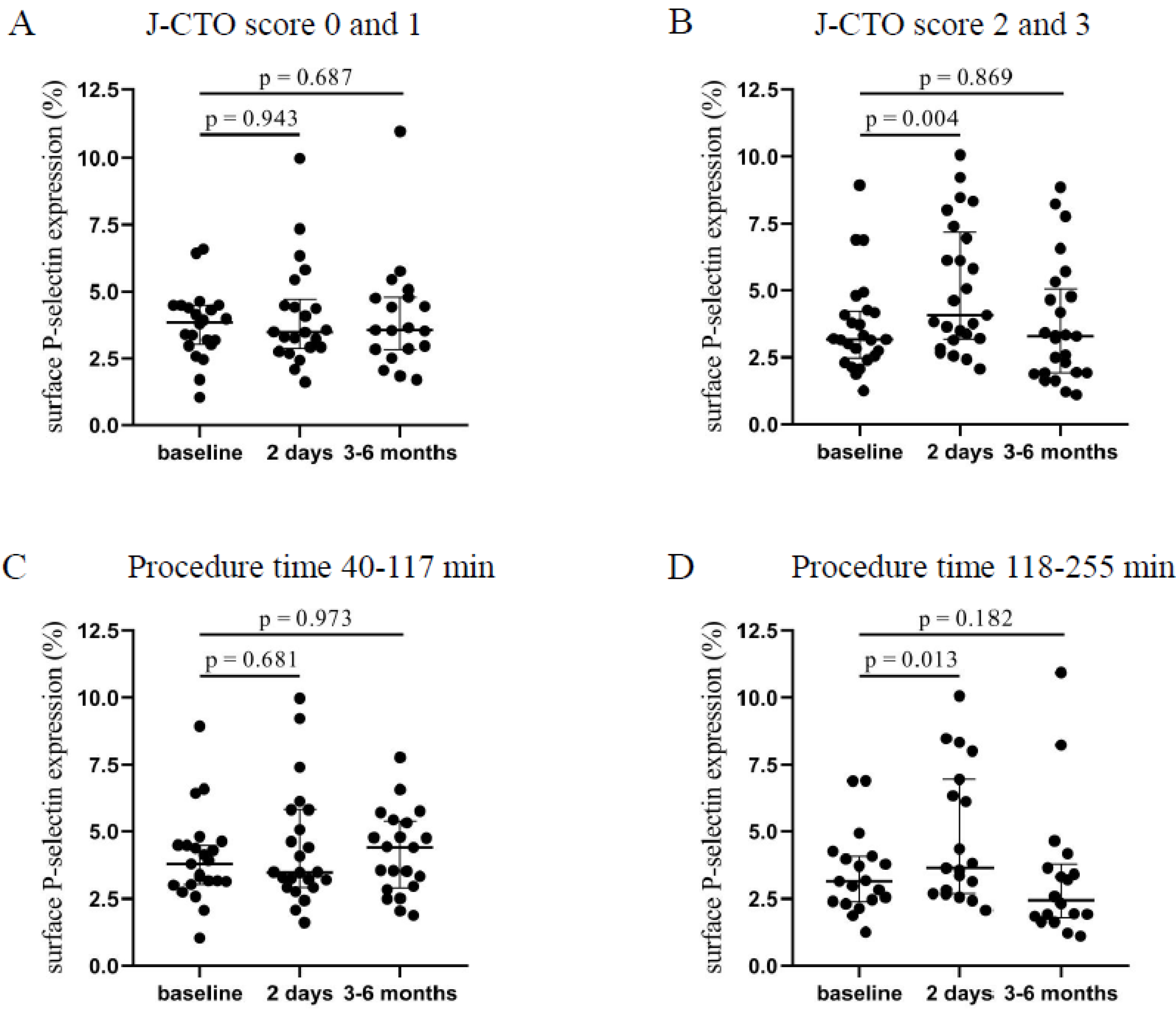
4.2. Induced Expression of Surface P-Selectin after Long, Complicated Interventions
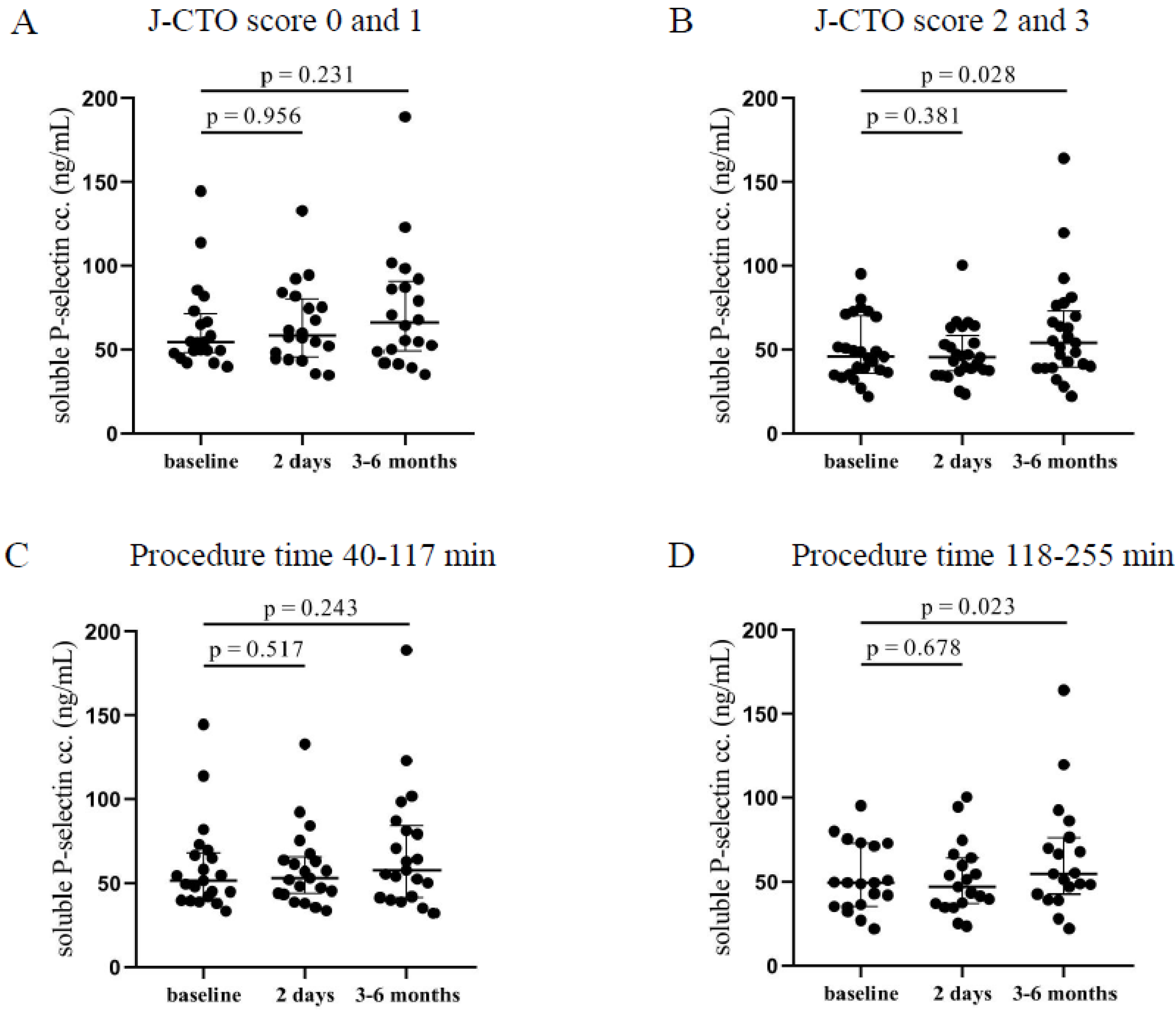
4.3. Elevated Post-PCI Soluble P-Selectin Concentrations at Higher J-CTO Scores and Longer PCI Duration
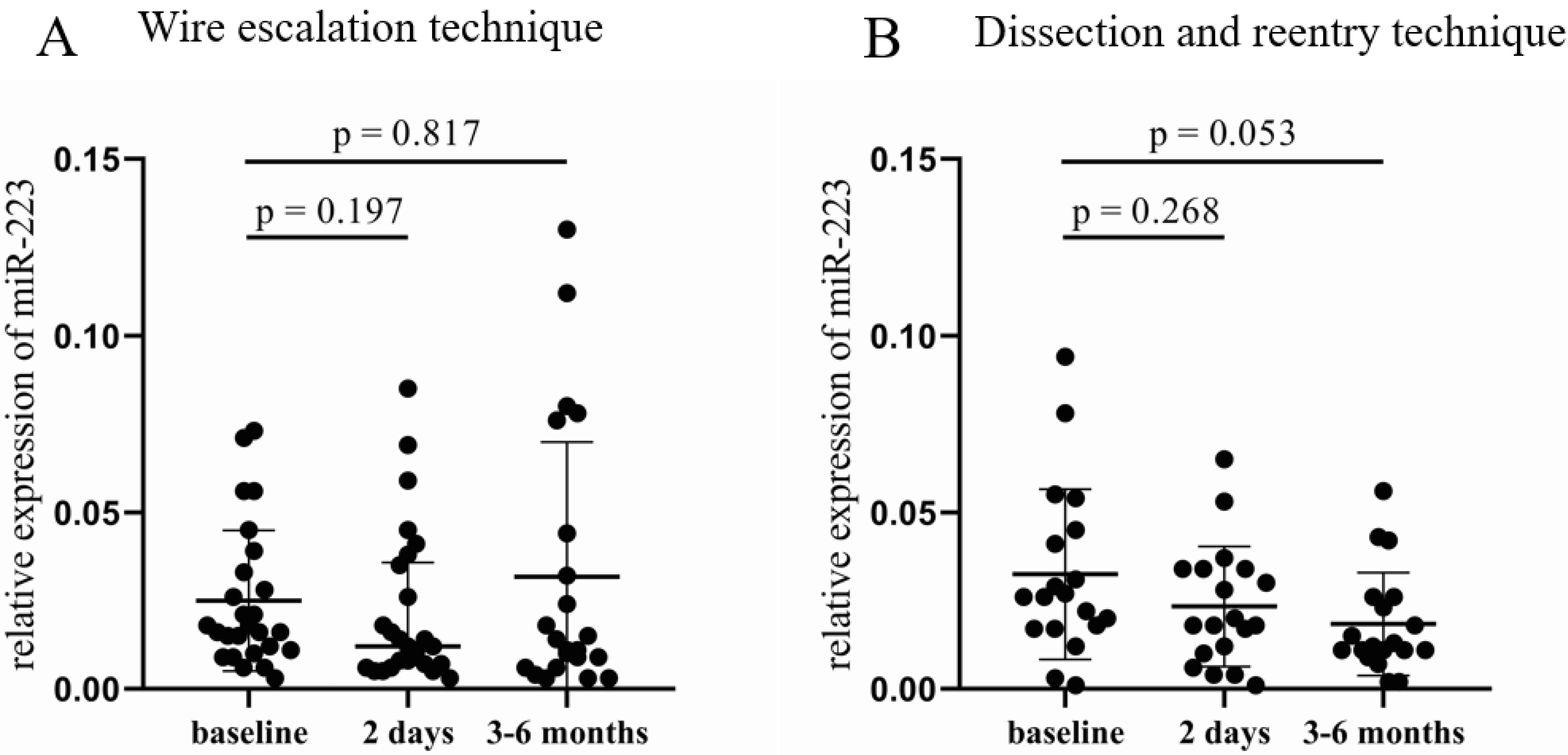
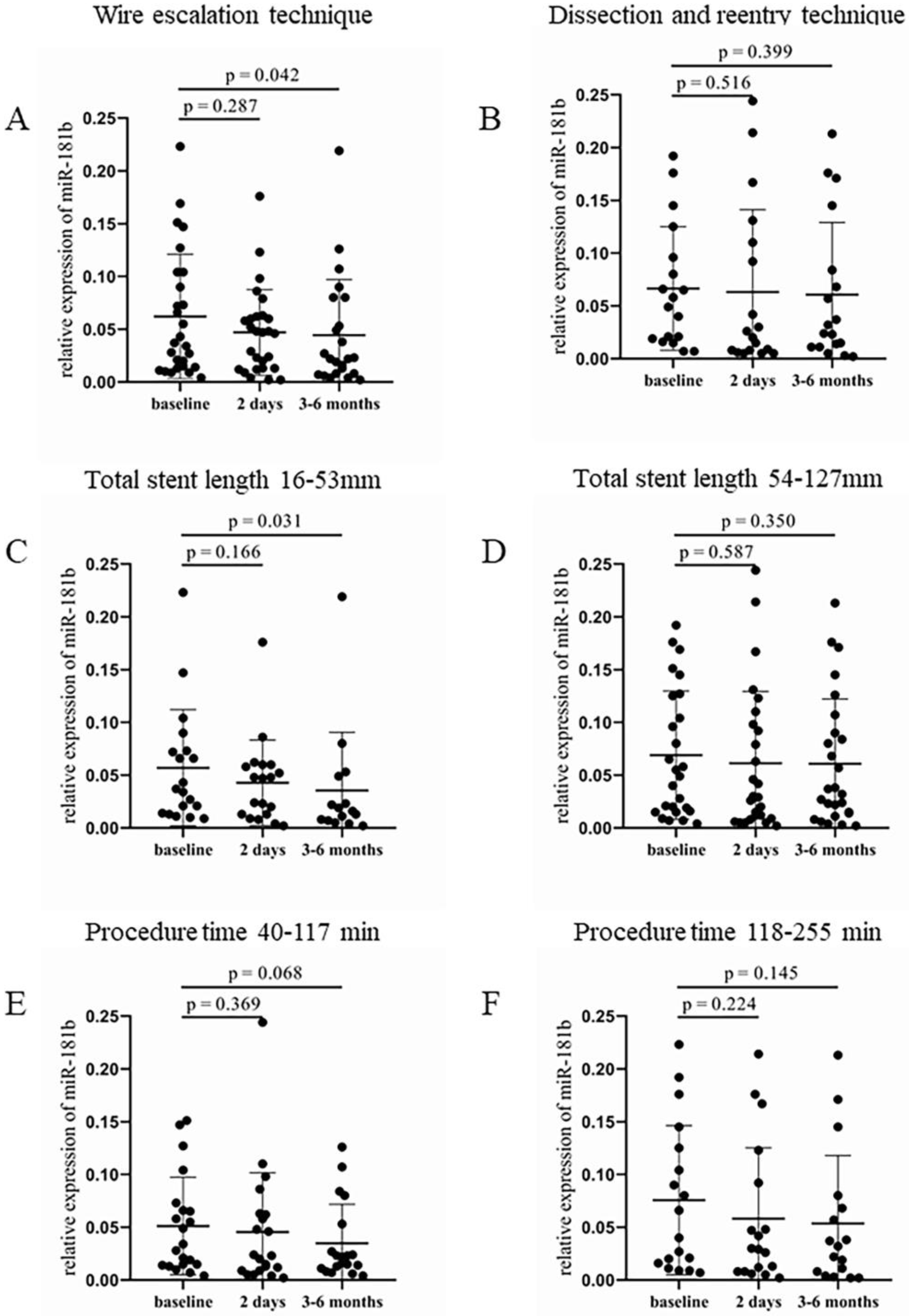
4.4. Altered Plasma microRNA Levels after CTO-PCI
4.5. Clinical Follow-Up of Patients
5. Discussion
6. Conclusions
7. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tajti, P.; Brilakis, E.S. Chronic Total Occlusion Percutaneous Coronary Intervention: Evidence and Controversies. J. Am. Heart Assoc. 2018, 7, e006732. [Google Scholar] [CrossRef]
- Fefer, P.; Knudtson, M.L.; Cheema, A.N.; Galbraith, P.D.; Osherov, A.B.; Yalonetsky, S.; Gannot, S.; Samuel, M.; Weisbrod, M.; Bierstone, D.; et al. Current Perspectives on Coronary Chronic Total Occlusions: The Canadian Multicenter Chronic Total Occlusions Registry. J. Am. Coll. Cardiol. 2012, 59, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Jeroudi, O.M.; Alomar, M.E.; Michael, T.T.; El Sabbagh, A.; Patel, V.G.; Mogabgab, O.; Fuh, E.; Sherbet, D.; Lo, N.; Roesle, M.; et al. Prevalence and management of coronary chronic total occlusions in a tertiary veterans affairs hospital. Catheter. Cardiovasc. Interv. 2014, 84, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Morino, Y.; Abe, M.; Morimoto, T.; Kimura, T.; Hayashi, Y.; Muramatsu, T.; Ochiai, M.; Noguchi, Y.; Kato, K.; Shibata, Y.; et al. Predicting Successful Guidewire Crossing Through Chronic Total Occlusion of Native Coronary Lesions Within 30 Minutes: The J-CTO (Multicenter CTO Registry in Japan) Score as a Difficulty Grading and Time Assessment Tool. JACC Cardiovasc. Interv. 2011, 4, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Katoh, O.; Tsuchikane, E.; Nasu, K.; Kinoshita, Y.; Ehara, M.; Terashima, M.; Matsuo, H.; Matsubara, T.; Asakura, K.; et al. The Efficacy of a Bilateral Approach for Treating Lesions with Chronic Total Occlusions: The CART (Controlled Antegrade and Retrograde subintimal Tracking) Registry. JACC Cardiovasc. Interv. 2009, 2, 1135–1141. [Google Scholar] [CrossRef]
- Thompson, C.A.; Jayne, J.E.; Robb, J.F.; Friedman, B.J.; Kaplan, A.V.; Hettleman, B.D.; Niles, N.W.; Lombardi, W.L. Retrograde Techniques and the Impact of Operator Volume on Percutaneous Intervention for Coronary Chronic Total Occlusions: An Early U.S. Experience. JACC Cardiovasc. Interv. 2009, 2, 834–842. [Google Scholar] [CrossRef]
- Mitsudo, K.; Yamashita, T.; Asakura, Y.; Muramatsu, T.; Doi, O.; Shibata, Y.; Morino, Y. Recanalization strategy for chronic total occlusions with tapered and stiff-tip guidewire. The results of CTO new techniQUE for STandard procedure (CONQUEST) trial. J. Invasive Cardiol. 2008, 20, 571–577. [Google Scholar]
- Christopoulos, G.; Karmpaliotis, D.; Alaswad, K.; Yeh, R.W.; Jaffer, F.A.; Wyman, R.M.; Lombardi, W.L.; Menon, R.V.; Grantham, J.A.; Kandzari, D.E.; et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int. J. Cardiol. 2015, 198, 222–228. [Google Scholar] [CrossRef]
- Hoebers, L.P.; Claessen, B.E.; Dangas, G.D.; Råmunddal, T.; Mehran, R.; Henriques, J.P.S. Contemporary overview and clinical perspectives of chronic total occlusions. Nat. Rev. Cardiol. 2014, 11, 458–469. [Google Scholar] [CrossRef]
- Srivatsa, S.; Edwards, W.D.; Boos, C.M.; Grill, D.E.; Sangiorgi, G.M.; Garratt, K.N.; Schwartz, R.S.; Holmes, D.R. Histologic Correlates of Angiographic Chronic Total Coronary Artery Occlusions: Influence of Occlusion Duration on Neovascular Channel Patterns and Intimal Plaque Composition. J. Am. Coll. Cardiol. 1997, 29, 955–963. [Google Scholar] [CrossRef]
- Brilakis, E.S.; Mashayekhi, K.; Tsuchikane, E.; Rafeh, N.A.; Alaswad, K.; Araya, M.; Avran, A.; Azzalini, L.; Babunashvili, A.M.; Bayani, B.; et al. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation 2019, 140, 420–433. [Google Scholar] [CrossRef]
- Brilakis, E.S.; Banerjee, S.; Karmpaliotis, D.; Lombardi, W.L.; Tsai, T.T.; Shunk, K.A.; Kennedy, K.F.; Spertus, J.A.; Holmes, D.R.; Grantham, J.A. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention. A Report From the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc. Interv. 2015, 8, 245–253. [Google Scholar] [CrossRef]
- Tekkesin, A.I. The first six-month clinical outcomes and risk factors associated with high on-treatment platelet reactivity of clopidogrel in patients undergoing coronary interventions. Anatol J. Cardiol. 2016, 16, 967–973. [Google Scholar] [CrossRef]
- Serrano, C.V.; Ramires, J.A.F.; Venturinelli, M.; Arie, S.; D’amico, E.; Zweier, J.L.; Pileggi, F.; da Luz, P.L. Coronary Angioplasty Results in Leukocyte and Platelet Activation with Adhesion Molecule Expression: Evidence of Inflammatory Responses in Coronary Angioplasty. J. Am. Coll. Cardiol. 1997, 29, 1276–1283. [Google Scholar] [CrossRef] [PubMed]
- Gregorini, L.; Marco, J.; Fajadet, J.; Bernies, M.; Cassagneau, B.; Brunel, P.; Bossi, I.M.; Mannucci, P.M. Ticlopidine and Aspirin Pretreatment Reduces Coagulation and Platelet Activation During Coronary Dilation Procedures. J. Am. Coll. Cardiol. 1997, 29, 13–20. [Google Scholar] [CrossRef]
- EPIC Investigators. Use of a Monoclonal Antibody Directed against the Platelet Glycoprotein IIb/IIIa Receptor in High-Risk Coronary Angioplasty. N. Engl. J. Med. 1994, 330, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.; Popma, J.J.; Ellis, S.G.; Hacker, J.A.; Topol, E.J. Abrupt vessel closure complicating coronary angioplasty: Clinical, angiographic and therapeutic profile. J. Am. Coll. Cardiol. 1992, 19, 926–935. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.-I.; Watanabe, N.; Nakazawa, K.; Suzuki, J.; Tsushima, K.; Tamatani, T.; Sakamoto, S.; Isobe, M. Roles of P-selectin in inflammation, neointimal formation, and vascular remodeling in balloon-injured rat carotid arteries. Circulation 2000, 102, 1710–1717. [Google Scholar] [CrossRef]
- Chan, M.Y.; Weitz, J.I.; Merhi, Y.; Harrington, R.A.; Becker, R.C. Catheter thrombosis and percutaneous coronary intervention: Fundamental perspectives on blood, artificial surfaces and antithrombotic drugs. J. Thromb. Thrombolysis 2009, 28, 366–380. [Google Scholar] [CrossRef]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef]
- Fabian, M.R.; Sonenberg, N.; Filipowicz, W. Regulation of mRNA Translation and Stability by microRNAs. Annu. Rev. Biochem. 2010, 79, 351–379. [Google Scholar] [CrossRef] [PubMed]
- Landry, P.; Plante, I.; Ouellet, D.L.; Perron, M.P.; Rousseau, G.; Provost, P. Existence of a microRNA pathway in anucleate platelets. Nat. Struct. Mol. Biol. 2009, 16, 961–966. [Google Scholar] [CrossRef]
- Kaudewitz, D.; Skroblin, P.; Bender, L.H.; Barwari, T.; Willeit, P.; Pechlaner, R.; Sunderland, N.P.; Willeit, K.; Morton, A.C.; Armstrong, P.C.; et al. Association of MicroRNAs and YRNAs With Platelet Function. Circ. Res. 2016, 118, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Qu, M.-J.; Pan, J.-J.; Shi, X.-J.; Zhang, Z.-J.; Tang, Y.-H.; Yang, G.-Y. MicroRNA-126 is a prospective target for vascular disease. Neuroimmunol. Neuroinflammation 2018, 5, 105. [Google Scholar] [CrossRef]
- Harris, T.A.; Yamakuchi, M.; Ferlito, M.; Mendell, J.T.; Lowenstein, C.J. MicroRNA-126 regulates endothelial expression of vascular cell adhesion molecule 1. Proc. Natl. Acad. Sci. USA 2008, 105, 1516–1521. [Google Scholar] [CrossRef] [PubMed]
- Fejes, Z.; Czimmerer, Z.; Szük, T.; Póliska, S.; Horváth, A.; Balogh, E.; Jeney, V.; Váradi, J.; Fenyvesi, F.; Balla, G.; et al. Endothelial cell activation is attenuated by everolimus via transcriptional and post-transcriptional regulatory mechanisms after drug-eluting coronary stenting. PLoS ONE 2018, 13, e0197890. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; He, S.; Sun, X.; Franck, G.; Deng, Y.; Yang, D.; Haemmig, S.; Wara, A.K.M.; Icli, B.; Li, D.; et al. MicroRNA-181b inhibits thrombin-mediated endothelial activation and arterial thrombosis by targeting caspase recruitment domain family member 10. FASEB J. 2016, 30, 3216–3226. [Google Scholar] [CrossRef]
- Szilágyi, B.; Fejes, Z.; Póliska, S.; Pócsi, M.; Czimmerer, Z.; Patsalos, A.; Fenyvesi, F.; Rusznyák, Á.; Nagy, G.; Kerekes, G.; et al. Reduced miR-26b Expression in Megakaryocytes and Platelets Contributes to Elevated Level of Platelet Activation Status in Sepsis. Int. J. Mol. Sci. 2020, 21, 866. [Google Scholar] [CrossRef]
- Szilágyi, B.; Fejes, Z.; Pócsi, M.; Kappelmayer, J.; Nagy, B., Jr. Role of sepsis modulated circulating microRNAs. EJIFCC 2019, 30, 128–145. [Google Scholar]
- Czimmerer, Z.; Hulvely, J.; Simandi, Z.; Varallyay, E.; Havelda, Z.; Szabo, E.; Varga, A.; Dezso, B.; Balogh, M.; Horvath, A.; et al. A Versatile Method to Design Stem-Loop Primer-Based Quantitative PCR Assays for Detecting Small Regulatory RNA Molecules. PLoS ONE 2013, 8, e55168. [Google Scholar] [CrossRef]
- Shah, P.B. Management of Coronary Chronic Total Occlusion. Circulation 2011, 123, 1780–1784. [Google Scholar] [CrossRef]
- Cinar, T.; Hayiroğlu, M.; Çiçek, V.; Asal, S.; Atmaca, M.M.; Keser, N.; Orhan, A.L. Predictors of left atrial thrombus in acute ischemic stroke patients without atrial fibrillation: A single-center cross-sectional study. Rev. Da Assoc. Médica Bras. 2020, 66, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Hoshi, K.; Fujito, T.; Sakai, Y.; Morooka, S.; Sohma, R. Early detection of platelet activation after coronary angioplasty. Coron. Artery Dis. 1996, 7, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Sohma, R.; Miyazaki, T.; Iwasaki, Y.; Yaguchi, I.; Morooka, S. Comparison of activation process of platelets and neutrophils after coronary stent implantation versus balloon angioplasty for stable angina pectoris. Am. J. Cardiol. 2000, 86, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Nagy, B.; Szűk, T.; Debreceni, I.B.; Kappelmayer, J. Platelet-derived microparticle levels are significantly elevated in patients treated by elective stenting compared to subjects with diagnostic catheterization alone. Platelets 2010, 21, 147–151. [Google Scholar] [CrossRef]
- Inoue, T.; Hoshi, K.; Yaguchi, I.; Iwasaki, Y.; Takayanagi, K.; Morooka, S. Serum Levels of Circulating Adhesion Molecules after Coronary Angioplasty. Cardiology 1999, 91, 236–242. [Google Scholar] [CrossRef]
- Dai, G.-H.; Ma, P.-Z.; Song, X.-B.; Liu, N.; Zhang, T.; Wu, B. MicroRNA-223-3p Inhibits the Angiogenesis of Ischemic Cardiac Microvascular Endothelial Cells via Affecting RPS6KB1/hif-1a Signal Pathway. PLoS ONE 2014, 9, e108468. [Google Scholar] [CrossRef]
- Sun, X.; Icli, B.; Wara, A.K.; Belkin, N.; He, S.; Kobzik, L.; Hunninghake, G.M.; Vera, M.P.; Blackwell, T.S.; Baron, R.M.; et al. MicroRNA-181b regulates NF-κB–mediated vascular inflammation. J. Clin. Investig. 2012, 122, 1973–1990. [Google Scholar] [CrossRef]
- Illési, Á.; Debreceni, I.B.; Fejes, Z.; Nagy, B.; Hodosi, K.; Kappelmayer, J.; Csanádi, Z.; Szük, T.I. Effect of invasive therapeutic coronary interventions on endothelial cell activation and thrombin generation in patients with chronic total coronary occlusion. Thromb. Res. 2022, 217, 64–72. [Google Scholar] [CrossRef]
- Simon, T.; Verstuyft, C.; Mary-Krause, M.; Quteineh, L.; Drouet, E.; Méneveau, N.; Steg, P.G.; Ferrières, J.; Danchin, N.; Becquemont, L. Genetic Determinants of Response to Clopidogrel and Cardiovascular Events. N. Engl. J. Med. 2009, 360, 363–375. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 61.78 ± 8.72 |
| Male, n (%) | 30 (60) |
| Hypertension, n (%) | 42 (84) |
| Hyperlipidemia, n (%) | 48 (96) |
| Obesity, n (%) | 45 (90) |
| AMI in anamnesis, n (%) | 22 (44) |
| DM in anamnesis, n (%) | 19 (38) |
| J-CTO score | 1.52 ± 0.95 |
| ACEi/ARB, n (%) | 44 (88) |
| BB, n (%) | 45 (90) |
| Nitrates, n (%) | 21 (42) |
| Statin, n (%) | 42 (84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Illési, Á.; Fejes, Z.; Pócsi, M.; Debreceni, I.B.; Hodosi, K.; Nagy Jr., B.; Kappelmayer, J.; Kőszegi, Z.; Csanádi, Z.; Szük, T. Technically Challenging Percutaneous Interventions of Chronic Total Occlusions Are Associated with Enhanced Platelet Activation. J. Clin. Med. 2023, 12, 6829. https://doi.org/10.3390/jcm12216829
Illési Á, Fejes Z, Pócsi M, Debreceni IB, Hodosi K, Nagy Jr. B, Kappelmayer J, Kőszegi Z, Csanádi Z, Szük T. Technically Challenging Percutaneous Interventions of Chronic Total Occlusions Are Associated with Enhanced Platelet Activation. Journal of Clinical Medicine. 2023; 12(21):6829. https://doi.org/10.3390/jcm12216829
Chicago/Turabian StyleIllési, Ádám, Zsolt Fejes, Marianna Pócsi, Ildikó Beke Debreceni, Katalin Hodosi, Béla Nagy Jr., János Kappelmayer, Zsolt Kőszegi, Zoltán Csanádi, and Tibor Szük. 2023. "Technically Challenging Percutaneous Interventions of Chronic Total Occlusions Are Associated with Enhanced Platelet Activation" Journal of Clinical Medicine 12, no. 21: 6829. https://doi.org/10.3390/jcm12216829
APA StyleIllési, Á., Fejes, Z., Pócsi, M., Debreceni, I. B., Hodosi, K., Nagy Jr., B., Kappelmayer, J., Kőszegi, Z., Csanádi, Z., & Szük, T. (2023). Technically Challenging Percutaneous Interventions of Chronic Total Occlusions Are Associated with Enhanced Platelet Activation. Journal of Clinical Medicine, 12(21), 6829. https://doi.org/10.3390/jcm12216829