


The Correlation between Retinal and Choroidal Thickness with Age-Related White Matter Hyperintensities in Progressive Supranuclear Palsy

 , , , ,
, , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Methods
2.2. Clinical and Instrumental Examination
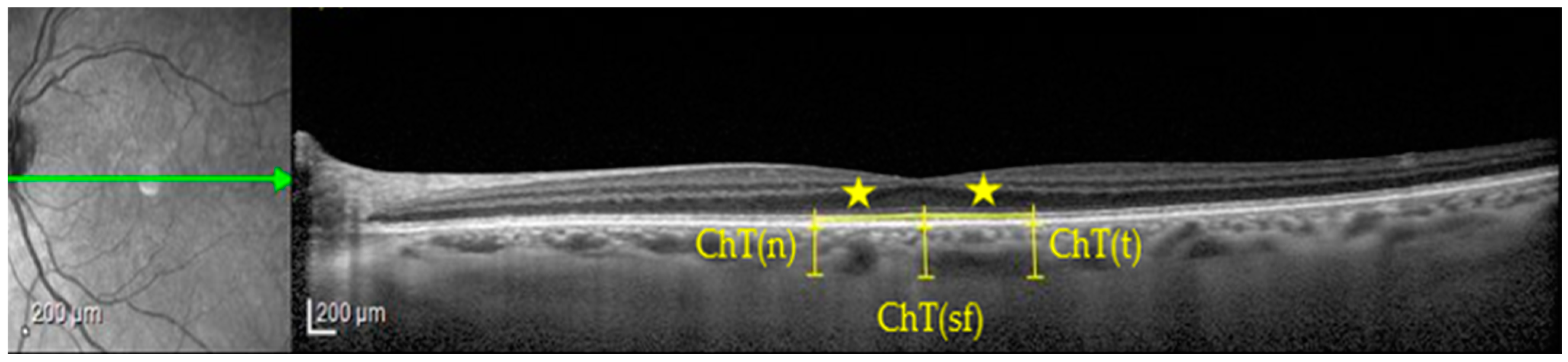
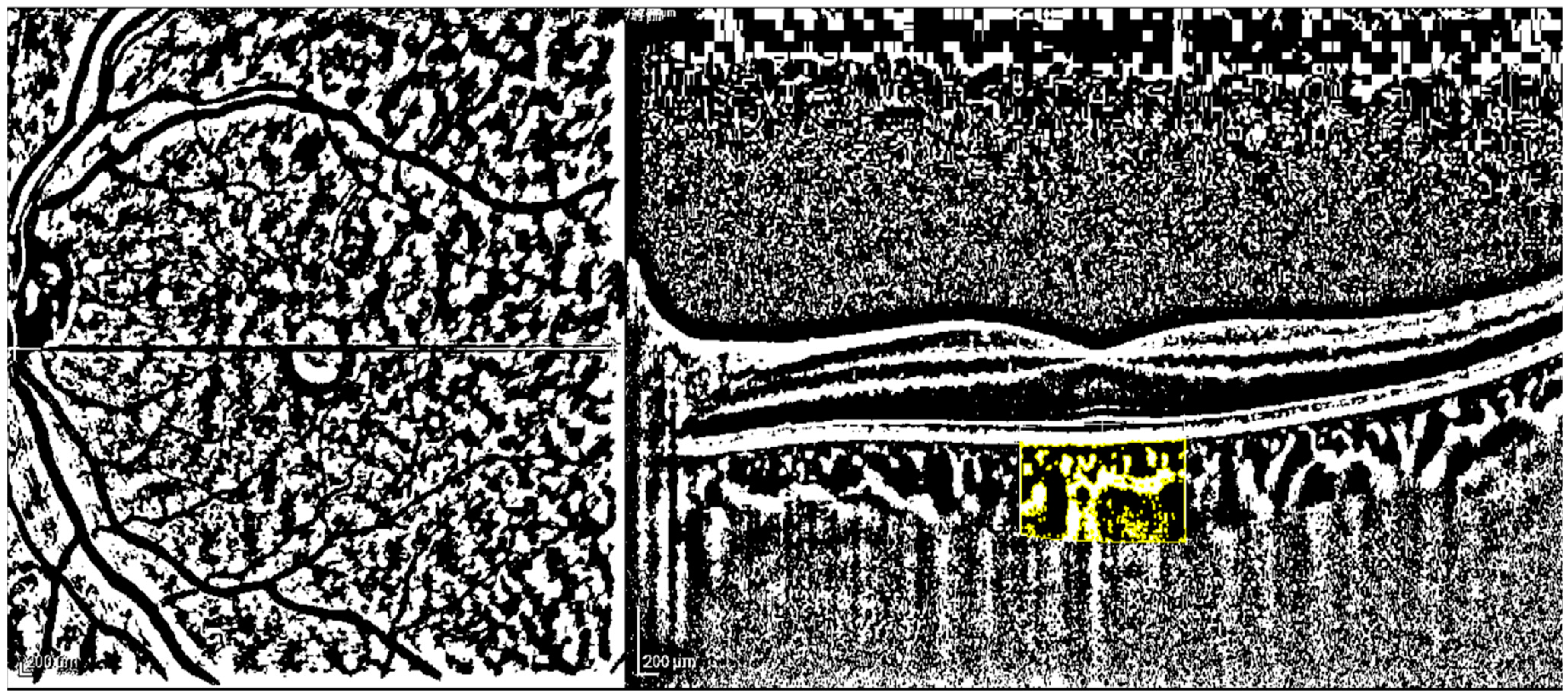
2.3. Imaging Protocol and Image Analysis
2.4. Brain MRI Protocol and Vascular Scoring
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Höglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Müller, U.; Nilsson, C.; Whitwell, J.L.; et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef]
- Boxer, A.L.; Yu, J.-T.; Golbe, L.I.; Litvan, I.; Lang, A.E.; Höglinger, G.U. New diagnostics and therapeutics for progressive supranuclear palsy. Lancet Neurol. 2017, 16, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [PubMed]
- Lukic, M.J.; Kurz, C.; Respondek, G.; Grau-Rivera, O.; Compta, Y.; Gelpi, E.; Troakes, C.; van Swieten, J.C.; Barcelona Brain Bank Collaborative Group; The MDS-Endorsed PSP Study Group; et al. Copathology in Progressive Supranuclear Palsy: Does It Matter? Mov. Disord. 2020, 35, 984–993. [Google Scholar] [CrossRef]
- Cheung, C.Y.; Chan, V.T.; Mok, V.C.; Chen, C.; Wong, T.Y. Potential retinal biomarkers for dementia: What is new? Curr. Opin. Neurol. 2019, 32, 82–91. [Google Scholar] [CrossRef]
- Stemplewitz, B.; Kromer, R.; Vettorazzi, E.; Hidding, U.; Frings, A.; Buhmann, C. Retinal degeneration in progressive supranuclear palsy measured by optical coherence tomography and scanning laser polarimetry. Sci. Rep. 2017, 7, 5357. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Ding, J.; Sen, P.; Rousselot, A.; Chan, A.; Nivison-Smith, L.; Wei, X.; Mahajan, S.; Kim, R.; Mishra, C.; et al. Exploring choroidal angioarchitecture in health and disease using choroidal vascularity index. Prog. Retin. Eye Res. 2020, 77, 100829. [Google Scholar] [CrossRef]
- Picillo, M.; Salerno, G.; Tepedino, M.F.; Abate, F.; Cuoco, S.; Gioia, M.; Coppola, A.; Erro, R.; Pellecchia, M.T.; Rosa, N.; et al. Retinal thinning in progressive supranuclear palsy: Differences with healthy controls and correlation with clinical variables. Neurol. Sci. 2022, 43, 4803–4809. [Google Scholar] [CrossRef]
- Picillo, M.; Tepedino, M.F.; Abate, F.; Erro, R.; Ponticorvo, S.; Tartaglione, S.; Volpe, G.; Frosini, D.; Cecchi, P.; Cosottini, M.; et al. Midbrain MRI assessments in progressive supranuclear palsy subtypes. J. Neurol. Neurosurg. Psychiatry 2020, 91, 98–103. [Google Scholar] [CrossRef]
- De Bernardo, M.; Vitiello, L.; Battipaglia, M.; Mascolo, F.; Iovino, C.; Capasso, L.; Ciacci, C.; Rosa, N. Choroidal structural evaluation in celiac disease. Sci. Rep. 2021, 11, 16398. [Google Scholar] [CrossRef]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Uchino, E.; Kawano, H.; Yoshihara, N.; Terasaki, H.; Shirasawa, M.; Tomita, M.; Ishibashi, T. Luminal and Stromal Areas of Choroid Determined by Binarization Method of Optical Coherence Tomographic Images. Am. J. Ophthalmol. 2015, 159, 1123–1131. [Google Scholar] [CrossRef]
- Wahlund, L.O.; Barkhof, F.; Fazekas, F.; Bronge, L.; Augustin, M.; Sjögren, M.; Wallin, A.; Ader, H.; Leys, D.; Pantoni, L.; et al. A New Rating Scale for Age-Related White Matter Changes Applicable to MRI and CT. Stroke 2001, 32, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Cione, F.; Capasso, L.; Coppola, A.; Rosa, N. A formula to improve the reliability of optical axial length measurement in IOL power calculation. Sci. Rep. 2022, 12, 18845. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Wang, Y.; Li, T.; Lin, Y.; Ma, W.; Chen, X.; Lyu, C.; Li, Y.; Lu, L. Correlation of subfoveal choroidal thickness with axial length, refractive error, and age in adult highly myopic eyes. BMC Ophthalmol. 2018, 18, 127. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Dai, Y.; Shi, Y.; Russell, J.F.; Lyu, C.; Noorikolouri, J.; Feuer, W.J.; Chu, Z.; Zhang, Q.; de Sisternes, L.; et al. Age-Related Changes in Choroidal Thickness and the Volume of Vessels and Stroma Using Swept-Source OCT and Fully Automated Algorithms. Ophthalmol. Retin. 2020, 4, 204–215. [Google Scholar] [CrossRef]
- Gyawali, P.; Jnawali, A.; Kharal, A.; Subedi, M.; Kandel, S.; Puri, P.R.; Paudel, N. SubFoveal Choroidal Imaging in High Myopic Nepalese Cohort. J. Ophthalmol. 2023, 2023, 2209496. [Google Scholar] [CrossRef]
- Albrecht, P.; Müller, A.-K.; Südmeyer, M.; Ferrea, S.; Ringelstein, M.; Cohn, E.; Aktas, O.; Dietlein, T.; Lappas, A.; Foerster, A.; et al. Optical Coherence Tomography in Parkinsonian Syndromes. PLoS ONE 2012, 7, e34891. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Müller, H.-P.; Lauda, F.; Tumani, H.; Ludolph, A.C.; Kassubek, J.; Pinkhardt, E.H. Retinal single-layer analysis in Parkinsonian syndromes: An optical coherence tomography study. J. Neural Transm. 2014, 121, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.A.; Shin, J.Y.; Kim, H.; Ahn, J.; Jeon, B.; Lee, J.-Y. Peripapillary retinal nerve fiber layer thinning in patients with progressive supranuclear palsy. J. Neurol. 2022, 269, 3216–3225. [Google Scholar] [CrossRef]
- De Bernardo, M.; Altieri, V.; Coppola, A.; Gioia, M.; Rosa, N. Choroidal evaluation in patients under alpha-lytic therapy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2729–2736. [Google Scholar] [CrossRef]
- Vitiello, L.; De Bernardo, M.; Erra, L.; Della Rocca, F.; Rosa, N.; Ciacci, C. Optical Coherence Tomography Analysis of Retinal Layers in Celiac Disease. J. Clin. Med. 2022, 11, 4727. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Salerno, G.; Gioia, M.; Capasso, L.; Russillo, M.C.; Picillo, M.; Erro, R.; Amboni, M.; Barone, P.; Rosa, N.; et al. Intraocular pressure and choroidal thickness postural changes in multiple system atrophy and Parkinson’s disease. Sci. Rep. 2021, 11, 8936. [Google Scholar] [CrossRef] [PubMed]
- Sevim, D.G.; Unlu, M.; Gultekin, M.; Karaca, C.; Mirza, M.; Mirza, G.E. Evaluation of Retinal Changes in Progressive Supranuclear Palsy and Parkinson Disease. J. Neuro-Ophthalmol. 2018, 38, 151–155. [Google Scholar] [CrossRef]
- Kamata, Y.; Hara, N.; Satou, T.; Niida, T.; Mukuno, K. Investigation of the pathophysiology of the retina and choroid in Parkinson’s disease by optical coherence tomography. Int. Ophthalmol. 2022, 42, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Robbins, C.B.; Thompson, A.C.; Bhullar, P.K.; Koo, H.Y.; Agrawal, R.; Soundararajan, S.; Yoon, S.P.; Polascik, B.W.; Scott, B.L.; Grewal, D.S.; et al. Characterization of Retinal Microvascular and Choroidal Structural Changes in Parkinson Disease. JAMA Ophthalmol 2021, 139, 182–188. [Google Scholar] [CrossRef]
- Nguyen, T.-T.; Cheng, J.-S.; Chen, Y.-L.; Lin, Y.-C.; Tsai, C.-C.; Lu, C.-S.; Weng, Y.-H.; Wu, Y.-M.; Hoang, N.-T.; Wang, J.-J. Fixel-Based Analysis of White Matter Degeneration in Patients with Progressive Supranuclear Palsy or Multiple System Atrophy, as Compared to Parkinson’s Disease. Front. Aging Neurosci. 2021, 13, 625874. [Google Scholar] [CrossRef]
- Armstrong, R.; Kergoat, H. Oculo-visual changes and clinical considerations affecting older patients with dementia. Ophthalmic Physiol. Opt. 2015, 35, 352–376. [Google Scholar] [CrossRef]
- Fuhrmann, S. Eye morphogenesis and patterning of the optic vesicle. Curr. Top. Dev. Biol. 2010, 93, 61–84. [Google Scholar] [CrossRef]
- Blumenfeld, H. Areas of the CNS made up mainly of myelinated axons are called white matter. In Neuroanatomy through Clinical Cases, 2nd ed.; Sinauer Associates Inc.: Sunderland, MA, USA, 2010; p. 21. [Google Scholar]
- Elshazzly, M.; Lopez, M.J.; Reddy, V.; Caban, O. Embryology, Central Nervous System; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Saint-Geniez, M.; D’Amore, P.A. Development and pathology of the hyaloid, choroidal and retinal vasculature. Int. J. Dev. Biol. 2004, 48, 1045–1058. [Google Scholar] [CrossRef]
- Patton, N.; Aslam, T.; MacGillivray, T.; Pattie, A.; Deary, I.J.; Dhillon, B. Retinal vascular image analysis as a potential screening tool for cerebrovascular disease: A rationale based on homology between cerebral and retinal microvasculatures. J. Anat. 2005, 206, 319–348. [Google Scholar] [CrossRef]
- Geerling, C.F.; Terheyden, J.H.; Langner, S.M.; Kindler, C.; Keil, V.C.; Turski, C.A.; Turski, G.N.; Wintergerst, M.W.M.; Petzold, G.C.; Finger, R.P. Changes of the retinal and choroidal vasculature in cerebral small vessel disease. Sci. Rep. 2022, 12, 3660. [Google Scholar] [CrossRef]
- La Marca, A.; Biondino, D.; Gioia, M. Comment on Naranjo-Bonilla et al. Retinal and Choroidal Effects of Continuous Positive Airway Pressure as Treatment for Sleep Apnea: Results at 12 Months. Int. J. Environ. Res. Public Health 2022, 19, 12637, Erratum in Int. J. Environ. Res. Public Health2023, 20, 1139. [Google Scholar] [CrossRef]
- Li, X.Q.; Larsen, M.; Munch, I.C. Subfoveal Choroidal Thickness in Relation to Sex and Axial Length in 93 Danish University Students. Investig. Opthalmology Vis. Sci. 2011, 52, 8438–8441. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-A.; Oh, S.Y. Choroidal Thickness in Healthy Children. Retina 2013, 33, 1971–1976. [Google Scholar] [CrossRef] [PubMed]
- Bidaut-Garnier, M.; Schwartz, C.; Puyraveau, M.M.; Montard, M.; Delbosc, B.; Saleh, M. Choroidal thickness measurement in children using optical coherence tomography. Retina 2014, 34, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Mirzania, D.; Thompson, A.C.; Robbins, C.B.; Soundararajan, S.; Lee, J.M.; Agrawal, R.; Liu, A.J.; Johnson, K.G.; Grewal, D.S.; Fekrat, S. Retinal and Choroidal Changes in Men Compared with Women with Alzheimer’s Disease: A Case-Control Study. Ophthalmol. Sci. 2021, 2, 100098. [Google Scholar] [CrossRef]
- Mori, Y.; Miyake, M.; Hosoda, Y.; Uji, A.; Nakano, E.; Takahashi, A.; Muraoka, Y.; Miyata, M.; Tamura, H.; Ooto, S.; et al. Distribution of Choroidal Thickness and Choroidal Vessel Dilation in Healthy Japanese Individuals: The Nagahama Study. Ophthalmol. Sci. 2021, 1, 100033. [Google Scholar] [CrossRef] [PubMed]
- Mihara, N.; Sonoda, S.; Terasaki, H.; Shiihara, H.; Sakono, T.; Funatsu, R.; Sakamoto, T. Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes. J. Clin. Med. 2023, 12, 1505. [Google Scholar] [CrossRef]
- Wang, L.; Wang, W.; Zhou, Z.; Wang, H.; Chakravarthy, U.; Peto, T.; Casalino, G.; Wang, K.; Li, S. Quantitative Assessment of Choroidal Thickness and Choroidal Vascular Features in Healthy Eyes Based on Image Binarization of EDI-OCT: A Single-Center Cross-Sectional Analysis in Chinese Population. J. Clin. Med. 2023, 12, 1911. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total PSP Patients | HC | p | ||
|---|---|---|---|---|
| n. | 26 | 26 | 0.043 | |
| M/W | 13/13 | 6/20 | ||
| Age | Mean ± SD | 69.89 ± 6.71 | 71.39 ± 7.56 | 0.284 |
| Median | 72.25 | 73.91 | ||
| min–max | 53.08–82.25 | 48.17–83.25 | ||
| AL | Mean ± SD | 23.29 ± 0.82 | 23.27 ± 0.83 | 0.923 |
| Median | 23.41 | 23.36 | ||
| min–max | 22.03–25.34 | 22.06–25.43 | ||
| PSP Patients (26) | HC (26) | p | ||
|---|---|---|---|---|
| ChT subfoveal (µm) | Mean ± SD | 243.15 ± 70 | 214.58 ± 50.26 | 0.097 |
| Range | 123–416 | 125–339 | ||
| ChT nasal (µm) | Mean ± SD | 230.77 ± 70.71 | 199.38 ± 58.78 | 0.088 |
| Range | 121–403 | 99–327 | ||
| ChT temporal (µm) | Mean ± SD | 238.12 ± 67.73 | 207.19 ± 53.12 | 0.073 |
| Range | 124–372 | 130–334 | ||
| TCA (mm2) | Mean ± SD | 2.04 ± 0.51 | 1.86 ± 0.46 | 0.200 |
| Range | 1.34–3.19 | 1.12–2.66 | ||
| LCA (mm2) | Mean ± SD | 1.36 ± 0.33 | 1.23 ± 0.31 | 0.145 |
| Range | 0.91–2.06 | 0.69–1.78 | ||
| SCA (mm2) | Mean ± SD | 0.67 ± 0.21 | 0.63 ± 0.16 | 0.621 |
| Range | 0.35–1.13 | 0.39–0.94 | ||
| CVI | Mean ± SD | 67.3% ± 5% | 66.1% ± 3.3% | 0.308 |
| Range | 50.1–75.6% | 60%–73.1% |
| PSP Patients (16) | |||
|---|---|---|---|
| Fovea (1 mm Diameter) | Mean ± SD | Range | |
| Thickness (Mt) (μm) | Photoreceptors (Bruch-OLM) | 87 ± 5.45 | 79–98 |
| IRL (OLM-ILM) | 182.19 ± 26.74 | 148–236 | |
| RPE (Bruch-RPE) | 15 ± 1.63 | 12–17 | |
| ONL | 87.69 ± 10.98 | 67–108 | |
| OPL | 24.19 ± 6.66 | 14–35 | |
| ONL/OPL | 3.96 ± 1.42 | 1.97–7.71 | |
| All layers | 269.19 ± 25.4 | 231–321 | |
| Volume (Mv) (μm2) | Photoreceptors (median) | 0.07 | 0.06–0.08 |
| IRL thickness | 0.14 ± 0.022 | 0.12–0.19 | |
| RPE | 0.01 | ||
| ONL (median) | 0.07 | 0.05–0.08 | |
| OPL (median) | 0.02 | 0.01–0.03 | |
| Macular volume (median) | 0.21 | 0.18–0.25 | |
| 5 central regions (3 mm) | Mean ± SD | Range | |
| Thickness (Meant) (μm) | Photoreceptors | 82.71 ± 3.65 | 76.2–89.8 |
| IRL (median) | 225.50 | 205.6–264.8 | |
| RPE | 14.53 ± 1.34 | 12.8–17.4 | |
| ONL | 72.25 ± 7.71 | 52.4–85.6 | |
| OPL | 30.88 ± 3.42 | 25.6–36.2 | |
| ONL/OPL | 2.38 ± 0.40 | 1.45–2.81 | |
| INL | 37.05 ± 3.80 | 31–46 | |
| IPL | 33.25 ± 4.30 | 25–45.6 | |
| GCL | 37.63 ± 6.24 | 23–45.6 | |
| RNFL | 19.03 ± 2.09 | 16.4–25 | |
| Macular thickness | 312.34 ± 13.91 | 285.6–343.2 | |
| Volume (Meanv) (μm2) | Photoreceptors (median) | 0.12 | 0.108–0.126 |
| IRL (median) | 0.33 | 0.3–0.378 | |
| RPE (mean ± SD) | 0.02 ± 0.002 | 0.018–0.024 | |
| ONL (mean ± SD) | 0.10 ± 0.011 | 0.122–0.072 | |
| OPL (median) | 0.04 | 0.054–0.036 | |
| INL (median) | 0.06 | 0.064–0.044 | |
| IPL (median) | 0.05 | 0.036–0.178 | |
| GCL (median) | 0.06 | 0.036–0.066 | |
| RNFL (median) | 0.03 | 0.024–0.038 | |
| Macular volume (median) | 0.45 | 0.414–0.49 | |
| ARWMC Scale | |||
|---|---|---|---|
| Mean ± SD | Median | Range | |
| Frontal | 0.5 ± 0.65 | 0 | 0–2 |
| Parietal | 0.16 ± 0.38 | 0 | 0–1 |
| Temporal | 0.06 ± 0.25 | 0 | 0–1 |
| Occipital | 0.13 ± 0.34 | 0 | 0–1 |
| Basal ganglia | 0 | ||
| Total | 1.81 ± 2.56 | 0 | 0–8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bernardo, M.; Diana, F.; Gioia, M.; De Luca, M.; Tepedino, M.F.; Pellecchia, M.T.; Rosa, N.; Barone, P.; Picillo, M. The Correlation between Retinal and Choroidal Thickness with Age-Related White Matter Hyperintensities in Progressive Supranuclear Palsy. J. Clin. Med. 2023, 12, 6671. https://doi.org/10.3390/jcm12206671
De Bernardo M, Diana F, Gioia M, De Luca M, Tepedino MF, Pellecchia MT, Rosa N, Barone P, Picillo M. The Correlation between Retinal and Choroidal Thickness with Age-Related White Matter Hyperintensities in Progressive Supranuclear Palsy. Journal of Clinical Medicine. 2023; 12(20):6671. https://doi.org/10.3390/jcm12206671
Chicago/Turabian StyleDe Bernardo, Maddalena, Francesco Diana, Marco Gioia, Martina De Luca, Maria Francesca Tepedino, Maria Teresa Pellecchia, Nicola Rosa, Paolo Barone, and Marina Picillo. 2023. "The Correlation between Retinal and Choroidal Thickness with Age-Related White Matter Hyperintensities in Progressive Supranuclear Palsy" Journal of Clinical Medicine 12, no. 20: 6671. https://doi.org/10.3390/jcm12206671
APA StyleDe Bernardo, M., Diana, F., Gioia, M., De Luca, M., Tepedino, M. F., Pellecchia, M. T., Rosa, N., Barone, P., & Picillo, M. (2023). The Correlation between Retinal and Choroidal Thickness with Age-Related White Matter Hyperintensities in Progressive Supranuclear Palsy. Journal of Clinical Medicine, 12(20), 6671. https://doi.org/10.3390/jcm12206671