
Association between Social Support and Depressive Symptoms in Informal Caregivers of Adult and Older Dependents: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
1. Introduction
- Is high perceived social support associated with fewer depressive symptoms?
- Is high received social support associated with fewer depressive symptoms?
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction and Synthesis
2.5. Ratings of Quality Assessment
2.6. Certainty Assessment
2.7. Analyses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author-Year) Country | N | Mean Age (SD) and Range | Percentage of Female (%) | Design | Recipients of Care | Type of Social Support | Measure of Social Support ** | Measuring Depressive Symptoms ** |
|---|---|---|---|---|---|---|---|---|
| Aggar 2010 [30] Australia | 93 | 65.8 (13.6) 37–95 | 59.1 | Cross-sectional | Frail older people | Perceived (global) | CRA | HADS |
| Ali 2016 [31] Pakistan | 90 | 34.9 (8.9) 20–45 | 84.4 | Cross-sectional | Stroke | Perceived (global) | MSPSS | DASS-42 |
| Amorin 2009 [32] Portugal | 46 | 35 (N/A) N/A | 80.4 | Cross-sectional | Cancer | Perceived (emotional) | ESSS | EADS-21 |
| Ar 2017 [33] Turkey | 190 | 51.4 (8.7) 26–77 | 89.5 | Cross-sectional | Dementia | Perceived (global) | MSPSS | BDI |
| Arevalo-Flechas 2014 [34] United States | 202 | 64.7(8.9) 47–83 * | 76.4 | Cross-sectional | Dementia | Perceived (global) | PRQ-85 | HADS |
| Asti 2006 [35] Turkey | 130 | 43.9 (8.52) 27–61 * | 81.5 | Cross-sectional | Dialysis | Perceived (global) | PSS | BDI |
| Au 2009 [36] China | 134 | 54.5 (13.2) 28–81 | 74.6 | Cross-sectional | Dementia | Perceived (global, emotional, and instrumental) | MSSS | CES-D |
| Azevedo 2017 [37] Brazil | 115 | 68 (N/A) 59–76 | 64.3 | Cross-sectional | Palliative care | Perceived (global) | MOS-SS | CES-D |
| Baillie 1988 [38] United States | 87 | 52.5 (13.9) 22–91 | 76 | Cross-sectional | Frail older people | Perceived (emotional) | Ad hoc | POMS |
| Ballard 1995 [39] United Kingdom | 109 | 64.3 (13.5) 37–91 * | 80.7 | Cross-sectional | Dementia | Perceived (global) | Ad hoc | Cornell |
| Bambara 2014 [40] United States | 42 | 51.6 (9.8) 32–71 * | 90.5 | Cross-sectional | Multiple sclerosis | Perceived (global) | SSSI | PHQ-9 |
| Bergman 1992 [41] United States | 94 | 70.2 (8.9) 52–88 * | 69.2 | Cross-sectional | Dementia | Perceived (global) | PRQ-85 | CES-D |
| Biggati 2011 [42] United States | 78 | 51.2 (12.6) 26–76 * | 0 | Cross-sectional | Cancer | Perceived (global) | ISEL | CES-D |
| Bonsu 2019 [43] Africa | 100 | 33.2 (8.9) 15–51 * | 79 | Cross-sectional | Severe burns injuries | Perceived (global) | MSPSS | BDI |
| Burgeois 1996 [44] United States | 100 | 71.9 (7.3) 57–87 * | 55 | Cross-sectional | Dementia | Perceived (global) | ISEL | CES-D |
| Burton 2008 [45] United States | 50 | 72.4 (10.2) 52–93 * | 80 | Cross-sectional | Palliative care | Perceived (global) | Ad hoc | CES-D |
| Butler 2001 [46] United States | 62 | 58 (N/A) 31–81 | 75.8 | Cross-sectional | Frail older people | Perceived (global) | Ad hoc | CES-D |
| Cabral 2014 [47] Portugal | 104 | 52 (N/A) 22–77 | 62.5 | Cross-sectional | Mental health | Perceived (global) | ESSS | EADS-21 |
| Calvete 2011 [48] Spain | 223 | 49.9 (12.6) 20–77 | 72.2 | Cross-sectional | Traumatic brain injury | Perceived (global, emotional, instrumental) | FNQ | CES-D |
| Cardenas 2014 [49] United States | 264 | 57.5 (13) 21.5–84 * | 100 | Cross-sectional | Dementia | Perceived (global) | ISSB | CES-D |
| Chai 2018 [50] Asia | 165 | 45 (14.6) 16–74 * | 54.4 | Cross-sectional | Mental health | Perceived (global) | MSPSS | QIDS-SR 16 |
| Chou 2010 [51] China | 350 | 66.6 (7.7) 55–87 | 44.9 | Cross-sectional | Intellectual disability | Perceived (global) | SSS | CES-D |
| Chow 2012 [52] China | 158 | 75.6 (6.8) 55–90 | 61.4 | Cross-sectional | Frail older people | Perceived (global) | SSSQ | GDS |
| Clyburn 2000 [53] Canada | 613 | 58.8 (13.5) 32–86 * | 71 | Cross-sectional | Dementia | Received (global) | Ad hoc | CES-D |
| Crespo 2005 [54] Spain | 108 | 57.2 (11.5) 34–78 * | 82.2 | Cross-sectional | Frail older people | Received and perceived (global) | SSSQ | BDI |
| Cumming 2008 [55] Australia | 116 | 66.9 (13.3) 32–92 | 71 | Cross-sectional | Stroke | Perceived (global) | MOS-SS | IDA Scale |
| Decker 1989 [56] United States | 67 | 55.9 (N/A) 17–75 | 88 | Cross-sectional | Spinal cord injury | Perceived (global) | Ad hoc | CES-D |
| Del Pino Casado 2022 [57] Spain | 81 | 57.6 (12.5) 28–89 | 87.3 | Longitudinal (repeated measures) | Frail older people | Perceived (global) | Duke-UNC | Goldberg |
| Durkin 2010 [58] United States | 130 | 63.4 (15) 20–87 | 84 | Longitudinal (repeated measures) | Frail older people | Perceived (global) | ISEL | CES-D |
| Faber 2005 [59] United States | 310 | 38.9 (7.3) 22–62 | 100 | Cross-sectional | Cancer | Perceived (global) | ISEL | CES-D |
| Gibson 2013 [60] United States | 1218 | 62.2 (13.2) 36–89 * | 82 | Cross-sectional | Dementia | Received (global) | K & B-C | CES-D |
| Giovannetti 2015 [61] Italy | 129 | 52.8 (13.1) 27–79* | 68.2 | Cross-sectional | Disorders of consciousness | Perceived (global) | MOS-SS | BDI-II |
| Grant 2000 [62] United States | 52 | 53.7 (16) 22–81 | 82.7 | Cross-sectional | Stroke | Perceived (global, emotional, instrumental) | ISEL | CES-D |
| Grant 2001 [63] United States | 40 | 53.3 (N/A) 22–81 | 85 | Cross-sectional | Stroke | Perceived (global) | ISEL | CES-D |
| Graven 2020 [64] United States | 530 | 41.4 (10.4) 21–62 * | 49.1 | Cross-sectional | Heart failure | Perceived (global) | ISEL | CES-D |
| Haley 1987 [65] United States | 54 | 56.1 (16.3) 20–87 | 80 | Cross-sectional | Dementia | Perceived (global) | HDLS | BDI |
| Han 2014 [66] China | 301 | 46.7 (14) 19–75 * | 63 | Cross-sectional | Cancer | Perceived (global) | MSPSS | CESD-10 |
| Harwood 2000 [67] United States | 64 | 63.8 (14.9) 27–90 | 70 | Cross-sectional | Dementia | Perceived (global) | PESS | CES-D |
| Hasson-Ohayon 2010 [68] Israel | 150 | 56.2 (11) 34–78 * | 100 | Cross-sectional | Cancer | Received (global) | CPASS | BSI |
| Hobbs 1997 [69] United States | 100 | 65.6 (8.12) 55–86 | 100 | Cross-sectional | Mental health | Perceived (global) | PESS | CES-D |
| Hwang 2011 [70] United States | 35 | 51.7 (12.9) 18–71 | 60 | Cross-sectional | Pulmonary hypertension | Perceived (global) | MOS-SS | PHQ-9 |
| Jeong 2017 [71] Korea | 39 | 45 (12.8) 19–71 * | 72.2 | Cross-sectional | Cancer | Perceived (global) | Duke-UNC | HADS |
| Khusaifan 2017 [72] Saudi Arabia | 122 | N/A | 78.7 | Cross-sectional | Dementia | Perceived (global) | MSPSS | HDRS |
| Kiral 2017 [73] Turkey | 141 | 59.7 (12.7) 32–85 * | 77 | Cross-sectional | Dementia | Perceived (global) | MSPSS | BDI |
| Koerner 2010 [74] United States | 61 | 56.7(13.2) 30–83 * | 73 | Cross-sectional | Frail older people | Perceived (global) | Walen & Lanchman | HSC |
| Kruithof 2016 [75] Netherlands | 183 | 62.5 (10.9) 41–84 * | 78.7 | Longitudinal (repeated measures) | Stroke | Received (global) | SSL-12-I | HADS |
| Kusku 2009 [76] Turkey | 51 | 42.2 (11.1) 20–64 * | 84.3 | Cross-sectional | Cancer | Perceived (global) | MSPSS | BDI |
| Lakey 2002 [77] United States | 100 | 49 (N/A) N/A | 100 | Cross-sectional | Dementia | Perceived (emotional) | QRI | CES-D |
| Lee 2003 [78] China | 69 | 53 (14.4) 23–82 | 84 | Cross-sectional | Dementia | Perceived (global) | PRQ-85 | CES-D |
| Leibach 2013 [79] United States | 81 | 43.4 (15.3) 13–74 * | 66.7 | Cross-sectional | Multiple sclerosis | Perceived (global) | ISEL | PHQ-9 |
| Li 1997 [80] United States | 252 | 65.4 (8.3) 49–82 * | 100 | Cross-sectional | Frail older people | Received (global, emotional, instrumental) | Ad hoc | CES-D |
| Li 2019 [81] China | 557 | 57 (6.7) 44–70 * | 47.2 | Cross-sectional | Frail older people | Perceived (global) | MSPSS | CES-D |
| Losada 2010 [82] Spain | 334 | 58.6 (12.9) 28–85 | 77.8 | Cross-sectional | Dementia | Received (global) | PSQ | CES-D |
| Luchsinger 2015 [83] United States | 139 | 59.3 (10.4) 39–80 * | 85.7 | Cross-sectional | Dementia | Perceived (global) | SSNL | GDS |
| Majerovitz 2007 [84] United States | 103 | 56 (N/A) N/A | 74 | Cross-sectional | People living in nursing homes | Perceived (global) | SSSQ | CES-D |
| MaloneBeach 1995 [85] United States | 57 | 58.3 (11.1) 22–83 | 100 | Cross-sectional | Dementia | Received (global, emotional, instrumental) | Ad hoc | CES-D |
| Manso Martínez 2013 [86] Spain | 88 | 56.6 (12.2) 32–81 * | 84.1 | Cross-sectional | Frail older people | Perceived (global) | Duke-UNC | HADS |
| Moral Serrano 2003 [87] Spain | 215 | 55.3 (14.6) 26–85 * | 87 | Cross-sectional | Older people hospitalized at home | Perceived (global) | Duke-UNC | Goldberg |
| Neri 2012 [88] Brazil | 176 | 71.8 (4.9) 68–90 | 70.7 | Cross-sectional | Frail older people | Perceived (global) | ISEL | GDS |
| Nuwamanya 2023 [11] Africa | 336 | 39.2 (11.5) 16–62 * | 60.4 | Cross-sectional | Cancer | Perceived (global) | MSPSS | PHQ-9 |
| Pagel 1987 [89] United States | 68 | 65 (9) 35–85 | 63.2 | Cross-sectional | Dementia | Perceived (global) | GSS | BDI |
| Pagnini 2010 [90] Italy | 40 | 55.6 (12.3) 51–80 * | 70 | Cross-sectional | Amyotrophic lateral sclerosis | Perceived (global) | MG-SS | BDI-II |
| Pearce 2006 [91] United States | 162 | 51 (13.3) 24–78 * | 73 | Cross-sectional | Terminal cancer | Perceived (global) | ISEL | DSM-IV |
| Raad 2020 [14] United States | 558 | 46.1 (14.1) 18–74 * | 58 | Cross-sectional | Traumatic brain injury | Perceived (global) | TBI-CareQOL | TBI-CareQOL |
| Rapp 1998 [92] United States | 65 | 61.3 (14.4) 33–90 * | 76.8 | Cross-sectional | Dementia | Perceived (global) | MOS-SS | CES-D |
| Rauktis 1995 [93] United States | 106 | 59 (N/A) 30–84 | 86 | Cross-sectional | Mental health | Perceived (global) | PSI | CES-D |
| Rivera 1991 [94] Africa | 165 | 58.6 (10.9) 30–85 | 100 | Cross-sectional | Frail older people | Perceived (global) | ASSIS | SADS |
| Riverra–Navarro 2018 [95] Spain | 326 | 60.1 (14.5) 31–89 * | 67.2 | Cross-sectional | Dementia | Perceived (global) | Duke-UNC | HADS |
| Robinson 1989 [96] United States | 78 | 65 (N/A) 47–85 | 100 | Cross-sectional | Dementia | Received (global) | ISSB | CES-D |
| Robinson 1994 [97] United States | 40 | 65 (N/A) 52–80 | 100 | Cross-sectional | Dementia | Perceived and Received (global) | GSS/SNL | CES-D |
| Rodakowski 2013 [98] United States | 173 | 53 (15) 23–83 * | 76 | Cross-sectional | Spinal cord injury | Received | REACH trial | CES-D |
| Rodi 2015 [99] United States, United Kingdom and Australia | 87 | N/A (N/A) 18–74 | 86.2 | Cross-sectional | Cancer | Perceived (global) | MOS-SS | BDI-II |
| Sahin 2012 [100] Turkey | 60 | 54.7 (N/A) N/A | 18 | Cross-sectional | Cancer | Perceived (global) | PSS-Fa | BDI |
| Sandoval 2019 [101] Chile | 377 | 51.7 (15.4) 15–87 | 85.1 | Cross-sectional | Frail older people | Perceived (global) | Duke-UNC | CES-D |
| Schulz 1991 [102] United States | 172 | 57.8 (N/A) N/A | 18 | Repeated measures with cross-sectional correlations | Dementia | Perceived (global) | ISEL | CES-D |
| Schumacher 1993 [103] United States | 75 | 43.8 (14.7) 18–75 | 51 | Cross-sectional | Cancer | Perceived (global) | Ad hoc | POMS |
| Schwarz 2000 [104] United States | 100 | 64.7 (13.4) 29–88 | 74 | Repeated measures with cross-sectional correlations | Frail older people | Received (global) | MISSB | CES-D |
| Scicolone 2018 [105] United States | 249 | 64.3 (11.1) 30–89 | 92.5 | Cross-sectional | Frail older people | Perceived (global) | MOS-SS | CES-D |
| Serrani 2014 [106] Argentina | 100 | 48.2 (3.4) 51–55 * | 91 | Cross-sectional | Greater | Perceived (global) | Duke-UNC | CES-D |
| Serrano-Ortega 2017 [107] Spain | 177 | 58.5 (12.9) 20–89 | 88 | Longitudinal (repeated measures) | Frail older people | Perceived (global) | Duke-UNC | Goldberg |
| Shaughnessy 2011 [108] Canada | 30 | 73.7 (6.9) 57–86 | 63.3 | Cross-sectional | Dementia | Perceived (global) | MOS-SS | CES-D |
| Shukri 2020 [109] Malaysia | 340 | 46 (15.2) 20–70 | 54.4 | Cross-sectional | Hemodialysis | Perceived (global) | MSPSS | HADS |
| Speer 1993 [110] United States | 26 | 67.3 (N/A) N/A | 15 | Cross-sectional | Parkinson | Perceived (emotional) | ISEL | GDS |
| Steffen 2002 [111] United States | 145 | 60.2 (13.3) 33.6–86.8 * | 80 | Cross-sectional | Dementia | Perceived (global) | PSS | BDI |
| Stevens 2013 [112] Mexico | 90 | 47.12 (12.7) 22–73 * | 92 | Cross-sectional | Traumatic brain injury | Perceived (global, emotional, instrumental) | ISEL | PHQ-9 |
| Tay 2022 [12] United States | 98 | 58.9 (14.24) 27–87 | 72.6 | Cross-sectional | Palliative care | Perceived (global) | MOS-SS | HADS |
| Tang 2015 [113] United States | 91 | 67 (12.2) 43–92 * | 70 | Cross-sectional | Dementia | Perceived (global) | ISEL | BDI-II |
| Thielemann 2001 [114] United States | 164 | 61.9 (10.8) 31–81 | 60 | Cross-sectional | Cancer | Perceived (global) | ISEL | CES-D |
| Verez Cotelo 2015 [115] Spain | 25 | 55 (12.8) 39–87 | 80 | Cross-sectional | Dementia | Perceived (global) | Duke-UNC | BDI-II |
| Yen 2006 [116] China | 55 | 54.3 (14.7) 20–83 | 70.9 | Cross-sectional | Mental health | Perceived (global) | Ad hoc | CES-D |
| Yoon 2003 [117] Korea | 311 | 56.1 (15.6) 24–92 | 81 | Cross-sectional | Frail older people | Received (global, emotional, instrumental) | PRQ-2000 | SDS |
| Yun 2023 [118] Korea | 396 | 80.7 (5.7) 69–96 | 57.6 | Cross-sectional | Frail older people | Perceived (global) | Ad hoc | SGDS-K |
| Zhong 2020 [13] China | 567 | 80.6 (8.8) 63–98 * | 54.2 | Cross-sectional | Frail older people | Perceived (global) | MSPSS | CES-D |
3. Results
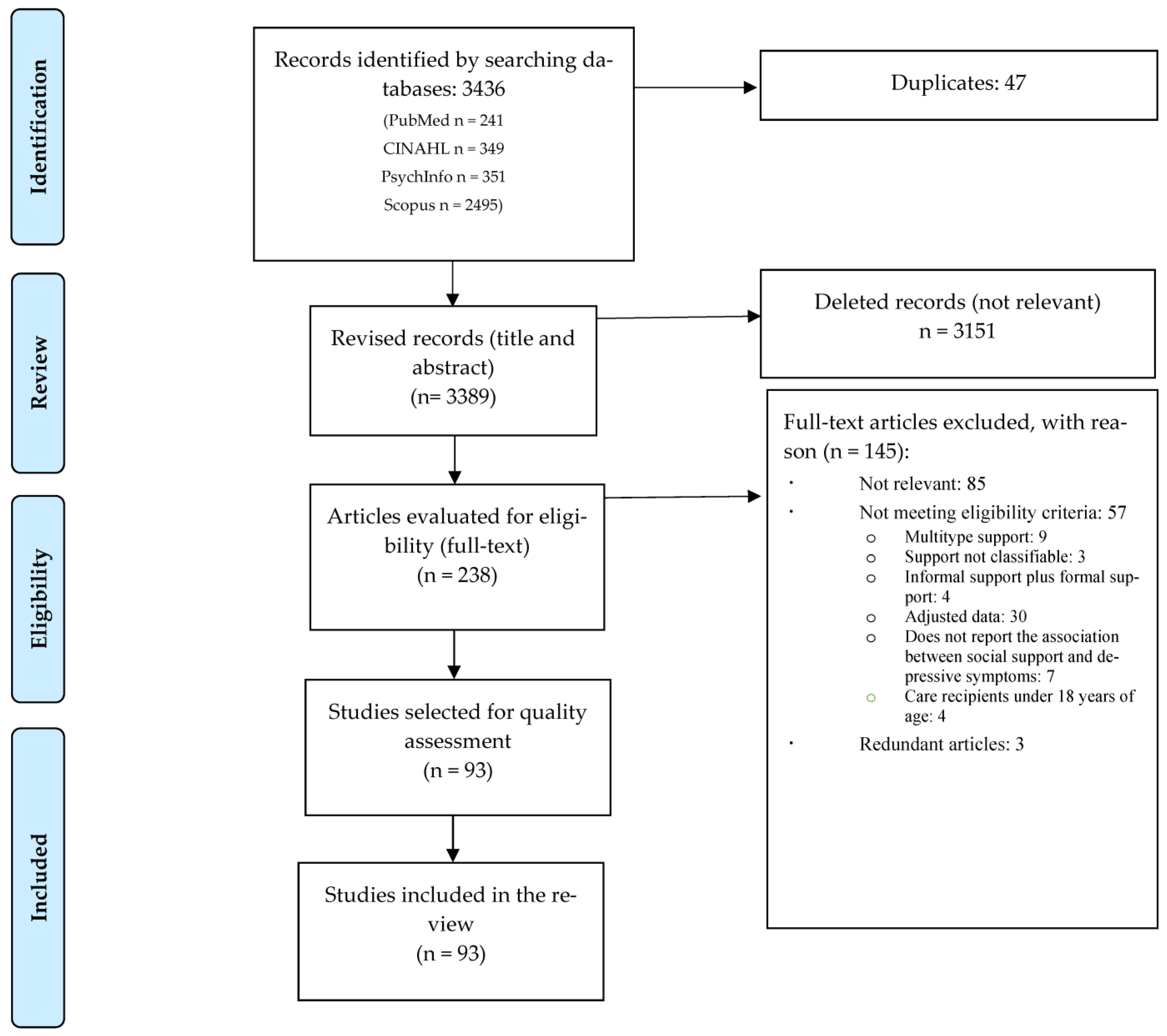
3.1. Description of Search Results
3.2. Description of Study Characteristics
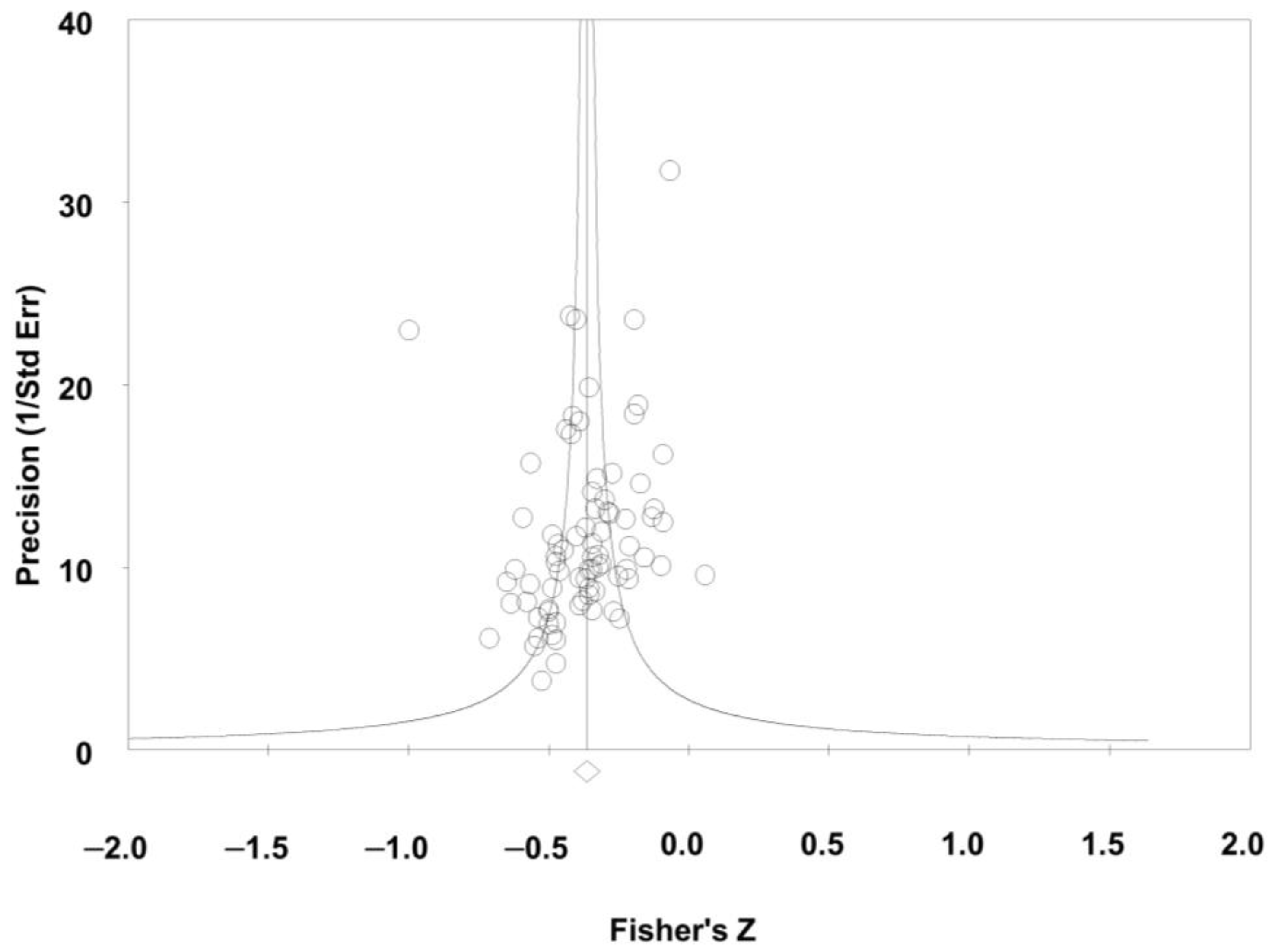
3.3. Quality Assessment
3.4. Results of the Different Meta-Analyses
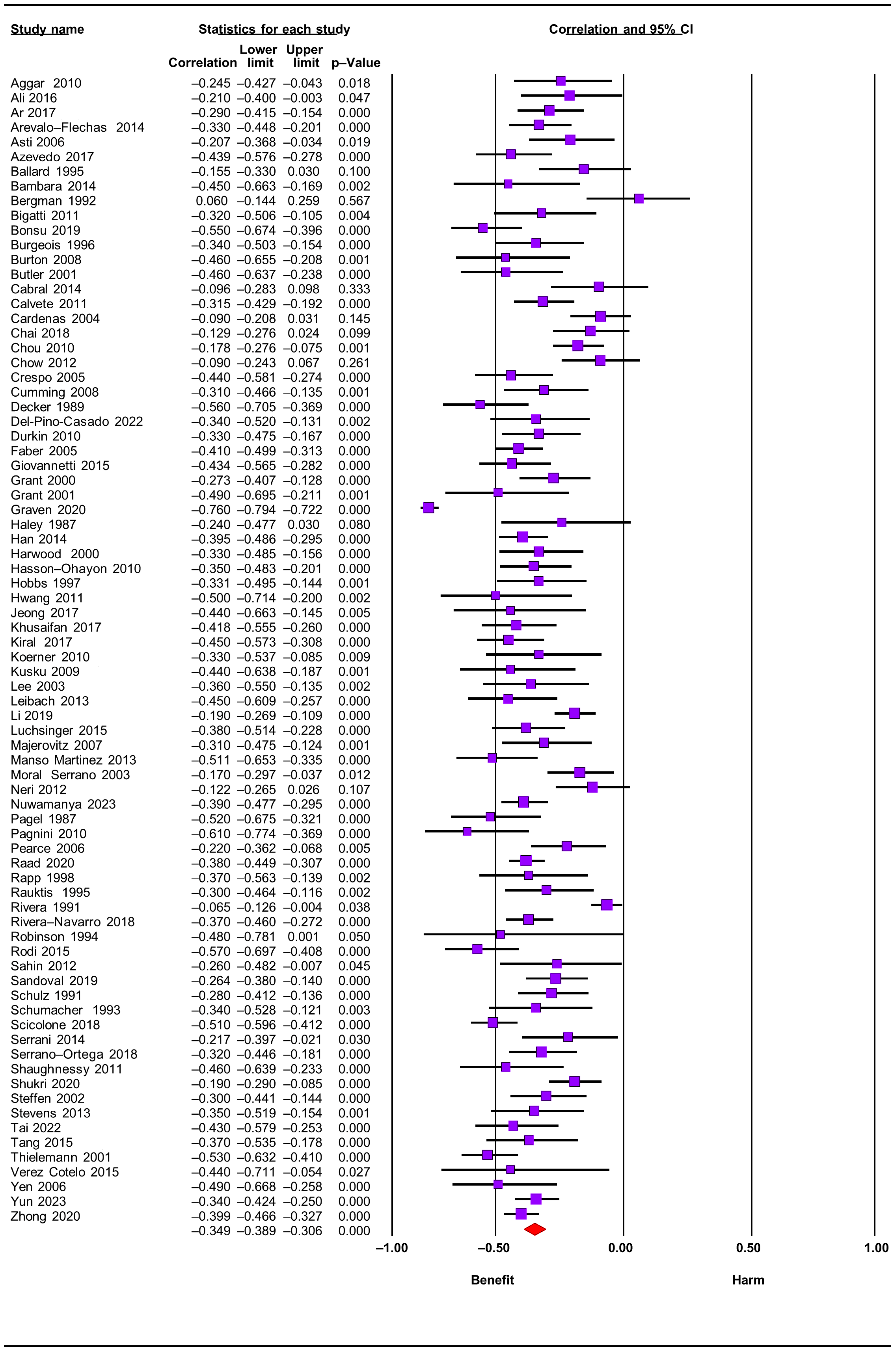
3.4.1. Perceived Social Support
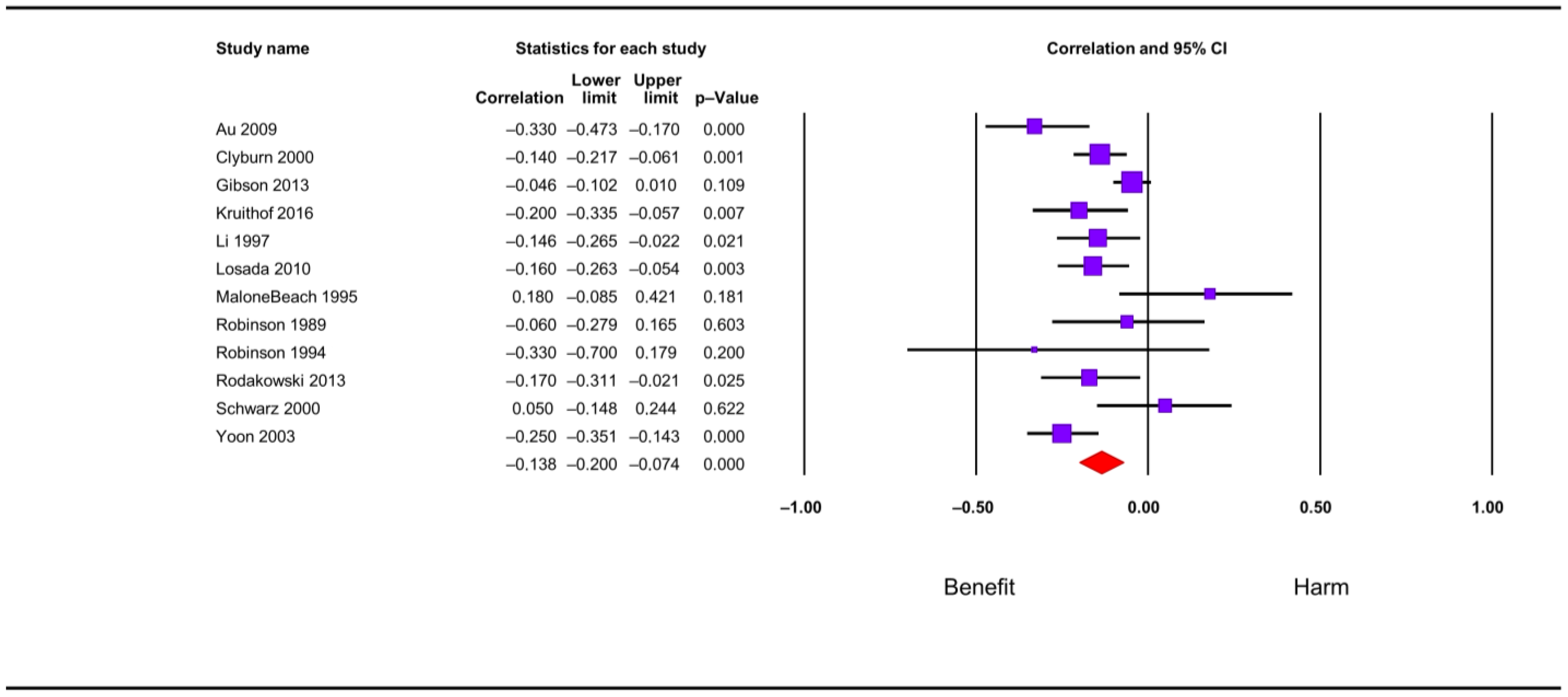
3.4.2. Received Social Support
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviations of Measures of: | |
| Social Support | |
| ASSIS | Arizona Social Support Interview Schedule |
| CRA | Caregiver Reaction Assessment |
| CPASS | Cancer Perceived Agent of Support Questionnaire |
| Duke-UNC | Duke-UNC functional social support questionnaire |
| ESSS | Satisfaction with Social Support Scale |
| FNQ | Family Needs Questionnaire |
| GSS | Global Satisfaction Scale |
| HDLS | Health and Daily Living Form |
| ISEL | Interpersonal Support Evaluation List |
| ISSB | Inventory of Socially Supportive Behavior |
| K & B-C | Krause and Borawski-Clark Scale |
| MG-SS | McGill Quality of Life- Social Support |
| MISSB | Modified Inventory of Social Support Behaviors |
| MOS-SS | Medical Outcome Study- Social Support Survey |
| MSPSS | Multidimensional Scale of Perceived Social Support |
| MSSS | Mac-Arthur Social Support Scale |
| NSIS | Negative Social Interaction |
| PESS | Pearling Expressive Support Scale |
| PRQ-85 | Personal Resource Questionnaire |
| PSI | Positive Social Interactions |
| PSS | Perceived Social Support Scale |
| PSQ | Psychosocial Support Questionnaire |
| QRI | Quality of Relationships Inventory |
| SOCSUP | Total Social Support Scale Score |
| SNL | Social Network List |
| SSL | Social Support List |
| SSNL | Stokes’ Social Network List |
| SSSQ | Sarason’s Social Support Questionnaire |
| SSRS | Social Support Rating Scale |
| SSS | Social Support Scale |
| SSSI | Social Stress and Social Interview |
| TBI-CareQOL | The Traumatic Injury Quality of Life |
| Walen & Lanchman | Walen & Lanchman Questionnaire |
| Depression | |
| BDI | Beck Depression Inventory |
| BSI | Brief Symptom Inventory |
| CES-D | The Center for Epidemiological Studies—Depression Scale |
| Cornell | Cornell Depression scale |
| DASS-42 | Depression Anxiety and Stress Scale |
| DSM-IV | Mayor Depressive Disorder and Anxiety Disorder Diagnoses by the Structured Clinical Interview. |
| EADS-21 | Escalas de Ansiedad, Depresión y Estrés [Anxiety, Depression and Stress Scales] |
| GDS | Global Deterioration Scale |
| GHQ | General Health Questionnaire |
| HADS | Hospital Anxiety and Depression Scale |
| HDRS | Hamilton Depression Rating Scale |
| HSC | Hopkins Symptom Checklist |
| IDA Scale | Irritability, Depression, and Anxiety Scale |
| PHQ-9 | Patient Health Questionnaire |
| POMS | Profile of Mood States |
| QIDS-SR 16 | Quick Inventory of Depressive Symptomatology |
| SCL-90 | Symptom Checklist |
| SDS | Self-Rating Depression Scale |
| SQD | Square Depression Scale |
| TBI-CareQOL | The Traumatic Injury Quality of Life |
References
- World Health Organization (WHO). Disability. Available online: https://www.who.int/es/news-room/fact-sheets/detail/disability-and-health (accessed on 1 March 2023).
- Fujisawa, R.; Colombo, F. The Long-Term Care Workforce: Overview and Strategies to Adapt Supply to a Growing Demand; OECD Health Working Papers, No. 44; OECD Publishing: Paris, France, 2009. [Google Scholar] [CrossRef]
- Suarez Cuba, M.Á. Identificación y utilidad de las herramientas para evaluar el apoyo social al paciente y al cuidador informal. Revista Médica La Paz 2011, 17, 60–67. [Google Scholar]
- Zhang, B.; Lv, X.; Qiao, M.; Liu, D. The Full Mediating Role of Loneliness on the Relationship Between Social Support and Depression Among Rural Family Caregivers of Persons with Severe Mental Illness. Front. Public Health 2021, 9, 729147. [Google Scholar] [CrossRef]
- Geng, H.; Chuang, D.; Yang, F.; Yang, Y.; Liu, W.; Liu, L.; Tian, H. Prevalence and determinants of depression in caregivers of cancer patients: A systematic review and meta-analysis. Medicine 2018, 97, 39. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Jiang, Y. A Meta-analytic Study of Predictors for Informal Caregiver Burden in Patients with Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 3636–3646. [Google Scholar] [CrossRef]
- Sallim, A.B.; Sayampanathan, A.A.; Cuttilan, A.; Chun-Man Ho, R. Prevalence of Mental Health Disorders Among Caregivers of Patients with Alzheimer Disease. J. Am. Med. Dir. Assoc. 2015, 16, 1034–1041. [Google Scholar] [CrossRef]
- Gottlieb, B.H.; Bergen, A.E. Social support concepts and measures. J. Psychosom. Res. 2010, 69, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1985. [Google Scholar]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Nuwamanya, S.; Nkola, R.; Najjuka, S.M.; Nabulo, H.; Al-Mamun, F.; Mamun, M.A.; Kaggwa, M.M. Depression in Ugandan caregivers of cancer patients: The role of coping strategies and social support. Ptiñizadas Sychooncol. 2023, 32, 113–124. [Google Scholar] [CrossRef]
- Tay, D.L.; Iacob, E.; Reblin, M.; Cloyes, K.G.; Jones, M.; Hebdon, M.C.T.; Mooney, K.; Beck, A.C.; Ellington, L. What contextual factors account for anxiety and depressed mood in hospice family caregivers? Psychooncology 2022, 31, 316–325. [Google Scholar] [CrossRef]
- Zhong, Y.; Wang, J.; Nicholas, S. Social support and depressive symptoms among family caregivers of older people with disabilities in four provinces of urban China: The mediating role of caregiver burden. BMC Geriatr. 2020, 20, 3. [Google Scholar] [CrossRef]
- Raad, J.H.; Tulsky, D.S.; Lange, R.T.; Brickell, T.A.; Sander, A.M.; Hanks, R.A.; French, L.; Miner, J.A.; Kisala, P.A.; Carlozzi, N.E. Establishing the Factor Structure of a Health-Related Quality of Life Measurement System for Caregivers of Persons Living with Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2020, 101, 1220–1232. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. La declaración PRISMA para informar revisiones sistemáticas y metanálisis de estudios que evalúan intervenciones de atención médica: Explicación y elaboración. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley Blackwell & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Berkman, N.D.; Dryden, D.M.; Hartling, L. Assessing Risk of Bias and Confounding in Observational Studies of Interventions or Exposures: Further Development of the RTI Item Bank; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. [Google Scholar]
- Boyle, M.H. Guidelines for evaluating prevalence studies. BMJ Ment. Health 1998, 1, 37–39. [Google Scholar] [CrossRef]
- Van der Lee, J.; Bakker, T.J.; Duivenvoorden, H.J.; Dröes, R. Multivariate models of subjective caregiver burden in dementia: A systematic review. Ageing Res. Rev. 2014, 15, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Aneshensel, C.S.; Pearlin, L.I.; Mullan, J.T.; Zarit, S.H.; Whitlatch, C.J. Perfiles en el Cuidado; Prensa Académica: San Diego, CA, USA, 1995. [Google Scholar]
- Pinquart, M.; Sörensen, S. Associations of stressors and uplifts of caregiving with caregiver burden and depressive mood: A meta-analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, 112–128. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490–1494. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, NY, USA, 2019. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ Br. Med. J. 2003, 327, 557. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Aggar, C.; Ronaldson, S.; Cameron, I.D. Reactions to caregiving of frail, older persons predict depression. Int. J. Ment. Health Nurs. 2010, 19, 409–415. [Google Scholar] [CrossRef]
- Ali, N.; Kausar, R. Social Support and Coping as Predictors of Psychological Distress in Family Caregivers of Stroke Patients. Pak. J. Psychol. Res. 2016, 31, 587–608. [Google Scholar]
- Amorim, L.; Pereira, M.G. Optimismo, suporte social e morbilidade psicológica em filhos adultos de doentes oncológicos. Psicol. Saúde E Doenças 2009, 10, 83–98. [Google Scholar]
- Ar, Y. Predictors of Depression, Anxiety, Grief and Growth among Turkish Offspring as Caregivers of Parents with Alzheimer’s Disease: A Multi-Method Study; Middle East Technical University: Ankara, Turkey, 2017. [Google Scholar]
- Arévalo-Flechas, L.; Acton, G.I.; Escamilla, M.N.; Bonner, P.L.; Lewis, S. Latino Alzheimer’s caregivers: What is important to them? J. Manag. Psychol. 2014, 29, 661–684. [Google Scholar] [CrossRef]
- Asti, T.; Kara, M.; Ipek, G.; Erci, B. The experiences of loneliness, depression, and social support of Turkish patients with continuous ambulatory peritoneal dialysis and their caregivers. J. Clin. Nurs. 2006, 15, 490–497. [Google Scholar] [CrossRef]
- Au, A.; Lau, K.M.; Koo, S.; Cheung, G.; Pan, P.C.; Wong, M.K. The effects of informal social support on depressive symptoms and life satisfaction in dementia caregivers in Hong Kong. East Asian Arch. Psychiatry 2009, 19, 57. [Google Scholar]
- Azevedo, C.; Pessalacia, J.D.R.; Mata, L.R.F.d.; Zoboli, E.L.C.P.; Pereira, M.d.G. Las interfaces entre apoyo social, calidad de vida y depresión en usuarios elegibles para cuidados paliativos. Rev. Esc. Enferm. USP 2017, 51, e03245. [Google Scholar]
- Baillie, V.; Norbeck, J.S.; Barnes, L.E. Stress, social support, and psychological distress of family caregivers of the elderly. Nurs. Res. 1988, 37, 217–222. [Google Scholar] [CrossRef]
- Ballard, C.G.; Saad, K.; Coope, B.; Graham, C.; Gahir, M.; Wilcock, G.K.; Oyebode, F. The aetiology of depression in the carers of dementia sufferers. J. Affect. Disord. 1995, 35, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Bambara, J.K.; Turner, A.P.; Williams, R.M.; Haselkorn, J.K. Social support and depressive symptoms among caregivers of veterans with multiple sclerosis. Rehabil. Psychol. 2014, 59, 230. [Google Scholar] [CrossRef]
- Bergman, B.F. Loneliness, Depression, and Social Support among Caregivers of Spouses with Alzheimer’s Disease: The Home versus the Nursing Home Care Experience; University of Nebraska Medical Center: Omaha, NE, USA, 1992. [Google Scholar]
- Bigatti, S.M.; Wagner, C.D.; Lydon-Lam, J.R.; Steiner, J.L.; Miller, K.D. Depression in husbands of breast cancer patients: Relationships to coping and social support. Support. Care Cancer 2011, 19, 455–466. [Google Scholar] [CrossRef]
- Bonsu, K.; Kugbey, N.; Ayanore, M.A.; Atefoe, E.A. Mediation effects of depression and anxiety on social support and quality of life among caregivers of persons with severe burns injury. BMC Res. Notes 2019, 12, 772. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, M.S.; Beach, S.; Schulz, R.; Burgio, L.D. When primary and secondary caregivers disagree: Predictors and psychosocial consequences. Psychol. Aging 1996, 11, 527. [Google Scholar] [CrossRef] [PubMed]
- Burton, A.M.; Haley, W.E.; Small, B.J.; Finley, M.R.; Dillinger-Vasille, M.; Schonwetter, R. Predictors of well-being in bereaved former hospice caregivers: The role of caregiving stressors, appraisals, and social resources. Palliat. Support. Care 2008, 6, 149–158. [Google Scholar] [CrossRef]
- Butler, S.S.; Turner, W.; Kaye, L.W.; Ruffin, L.; Downey, R. Depression and caregiver burden among rural elder caregivers. J. Gerontol. Soc. Work 2005, 46, 7–63. [Google Scholar] [CrossRef]
- Cabral, L.; Duarte, J.; Ferreira, M.; dos Santos, C. Anxiety, stress and depression in family caregivers of the mentally ill. Aten. Primaria 2014, 46, 176–179. [Google Scholar] [CrossRef]
- Calvete, E.; de Arroyabe, E.L. Depression and grief in Spanish family caregivers of people with traumatic brain injury: The roles of social support and coping. Brain Inj. 2012, 26, 834–843. [Google Scholar] [CrossRef]
- Cardenas, V. The Relationship between Social Support and Depression among Latina and Caucasian Dementia Caregivers. Ph.D. Thesis, Pacific Graduate School of Psychology, Palo Alto, CA, USA, 2004. [Google Scholar]
- Chai, Y.C.; Mahadevan, R.; Ng, C.G.; Chan, L.F.; Md Dai, F. Caregiver depression: The contributing role of depression in patients, stigma, social support and religiosity. Int. J. Soc. Psychiatry 2018, 64, 578–588. [Google Scholar] [CrossRef]
- Chou, Y.C.; Pu, C.; Fu, L.; Kröger, T. Depressive symptoms in older female carers of adults with intellectual disabilities. J. Intellect. Disabil. Res. 2010, 12, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.O.; Ho, H.C. The relationship between psychological resources, social resources, and depression: Results from older spousal caregivers in Hong Kong. Aging Ment. Health 2012, 16, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Clyburn, L.D.; Stones, M.J.; Hadjistavropoulos, T.; Tuokko, H. Predicting caregiver burden and depression in Alzheimer’s disease. J. Gerontol. B Psychol. Sci. Soc. Sci. 2000, 55, S2–S13. [Google Scholar] [PubMed]
- Crespo-López, M.; López-Martínez, J. Estrés y estado emocional en cuidadores de familiares mayores con y sin demencia. Rev. Esp. Geriatr. Gerontol. 2005, 40, 55–61. [Google Scholar] [CrossRef]
- Cumming, T.B.; Cadilhac, D.A.; Rubin, G.; Crafti, N.; Pearce, D.C. Psychological distress and social support in informal caregivers of stroke survivors. Brain Impair. 2008, 9, 152–160. [Google Scholar] [CrossRef]
- Decker, S.D.; Schultz, R.; Wood, D. Determinants of well-being in primary caregivers of spinal cord injured persons. Rehabil. Nurs. 1989, 14, 6–8. [Google Scholar] [CrossRef]
- Del-Pino-Casado, R.; López-Martínez, C.; Frías Osuna, A.; Orgeta, V. The relationship between perceived social support and psychological distress in carers of older relatives: A longitudinal cross-lagged analysis. J. Affect. Disord. 2022, 297, 401–406. [Google Scholar] [CrossRef]
- Durkin, D.W. Changes in Emotional Well-Being and Self-Perceived Physical Health over Time among African American and White Male Caregivers of Older Adults; The University of Alabama: Tuscaloosa, AL, USA, 2010. [Google Scholar]
- Faber, K.E. The Impact of Being a Caregiver to a Parent with Cancer: Daughters’ Correlates and Predictors of Coping; Teachers College, Columbia University: New York, NY, USA, 2005. [Google Scholar]
- Gibson, B.E. A Methodological Journey to Examine the Stress Process among Dementia Caregivers from Three Ethnoracial Groups: Caucasian, African American, and Hispanic; The University of North Carolina at Greensboro: Greensboro, NC, USA, 2003. [Google Scholar]
- Giovannetti, A.M.; Covelli, V.; Sattin, D.; Leonardi, M. Caregivers of patients with disorder of consciousness: Burden, quality of life and social support. Acta Neurol. Scand. 2015, 132, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.S.; Bartolucci, A.A.; Elliot, T.R.; Giger, J.N. Sociodemographic, physical, and psychosocial characteristics of depressed and non-depressed family caregivers of stroke survivors. Brain Inj. 2000, 14, 1089–1100. [Google Scholar] [PubMed]
- Grant, J.S.; Elliott, T.R.; Giger, J.N.; Bartolucci, A.A. Social problem-solving abilities, social support, and adjustment among family caregivers of individuals with a stroke. Rehabil. Psychol. 2001, 46, 44. [Google Scholar] [CrossRef]
- Graven, L.J.; Azuero, A.; Abbott, L.; Grant, J.S. Psychosocial factors related to adverse outcomes in heart failure caregivers: A structural equation modeling analysis. J. Cardiovasc. Nurs. 2020, 35, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Haley, W.E.; Levine, E.G.; Brown, S.L.; Bartolucci, A.A. Stress, appraisal, coping, and social support as predictors of adaptational outcome among dementia caregivers. Psychol. Aging 1987, 2, 323. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Hu, D.; Liu, Y.; Lu, C.; Luo, Z.; Zhao, J.; Lopez, V.; Mao, J. Coping styles and social support among depressed Chinese family caregivers of patients with esophageal cancer. Eur. J. Oncol. Nurs. 2014, 18, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Harwood, D.G.; Ownby, R.L.; Burnett, K.; Barker, W.W.; Duara, R. Predictors of appraisal and psychological well-being in Alzheimer’s disease family caregivers. J. Clin. Geropsychol. 2000, 6, 279–297. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Goldzweig, G.; Braun, M.; Galinsky, D. Women with advanced breast cancer and their spouses: Diversity of support and psychological distress. Psychooncology 2010, 19, 1195–1204. [Google Scholar] [CrossRef]
- Hobbs, T.R. Depression in the caregiving mothers of adult schizophrenics: A test of the resource deterioration model. Community Ment. Health J. 1997, 33, 387–399. [Google Scholar] [CrossRef]
- Hwang, B.; Howie-Esquivel, J.; Fleischmann, K.E.; Stotts, N.A.; Dracup, K. Family caregiving in pulmonary arterial hypertension. Heart Lung 2012, 41, 26–34. [Google Scholar] [CrossRef]
- Jeong, A.; An, J.Y. The moderating role of social support on depression and anxiety for gastric cancer patients and their family caregivers. PLoS ONE 2017, 12, e0189808. [Google Scholar] [CrossRef]
- Khusaifan, S.J.; El Keshky, M.E.S. Social support as a mediator variable of the relationship between depression and life satisfaction in a sample of Saudi caregivers of patients with Alzheimer’s disease. Int. Psychogeriatr. 2017, 29, 239–248. [Google Scholar] [CrossRef]
- Kiral, K.; Yetim, Ü.; Özge, A.; Aydin, A. The relationships between coping strategies, social support and depression: An investigation among Turkish care-givers of patients with dementia. Ageing Soc. 2017, 37, 167–187. [Google Scholar] [CrossRef]
- Koerner, S.S.; Shirai, Y.; Kenyon, D.B. Sociocontextual circumstances in daily stress reactivity among caregivers for elder relatives. J. Gerontol. B Psychol. Sci. Soc. Sci. 2010, 65, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Kruithof, W.J.; Post, M.W.M.; van Mierlo, M.L.; van den Bos, G.A.M.; de Man-van Ginkel, J.M.; Visser-Meily, J.M.A. Caregiver burden and emotional problems in partners of stroke patients at two months and one year post-stroke: Determinants and prediction. Patient Educ. Couns. 2016, 99, 1632–1640. [Google Scholar] [CrossRef] [PubMed]
- Kuscu, M.K.; Dural, U.; Onen, P.; Yaşa, Y.; Yayla, M.; Basaran, G.; Turhal, s.; Bekiroğlu, N. The association between individual attachment patterns, the perceived social support, and the psychological well-being of Turkish informal caregivers. Psycho-Oncol. 2009, 18, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Lakey, B.; Adams, K.; Neely, L.; Rhodes, G.; Lutz, C.J.; Sielky, K. Perceived support and low emotional distress: The role of enacted support, dyad similarity, and provider personality. Pers. Soc. Psychol. Bull. 2002, 28, 1546–1555. [Google Scholar] [CrossRef]
- Lee, H.J.; Seo, J.M.; Ahn, S.H. The role of social support in the relationship between stress and depression among family caregivers of older adults with dementia. J. Korean Acad. Nurs. 2003, 33, 713–721. [Google Scholar] [CrossRef]
- Leibach, G. Examining the Relations Between the Mental Health and Physical Health of Caregivers of MS in a Mexican Sample. Master’s Thesis, Virginia Commonwealth University, Richmond, VA, USA, 2013. [Google Scholar]
- Li, L.W.; Seltzer, M.M.; Greenberg, J.S. Social support and depressive symptoms: Differential patterns in wife and daughter caregivers. J. Gerontol. B Psychol. Sci. Soc. Sci. 1997, 52, S200–S211. [Google Scholar] [CrossRef]
- Li, M.; Mao, W.; Chi, I.; Lou, V.W. Geographical proximity and depressive symptoms among adult child caregivers: Social support as a moderator. Aging Ment. Health 2019, 23, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Losada, A.; Márquez-González, M.; Knight, B.G.; Yanguas, J.; Sayegh, P.; Romero-Moreno, R. Psychosocial factors and caregivers’ distress: Effects of familism and dysfunctional thoughts. Aging Ment. Health 2010, 14, 193–202. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Tipiani, D.; Torres-Patiño, G.; Silver, S.; Eimicke, J.P.; Ramirez, M.; Teresi, J.; Mittelman, M. Characteristics and mental health of Hispanic dementia caregivers in New York City. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 584–590. [Google Scholar] [CrossRef]
- Majerovitz, S. Predictors of burden and depression among nursing home family caregivers. Aging Ment. Health 2007, 11, 323–329. [Google Scholar] [CrossRef]
- Malone Beach, E.E.; Zarit, S.H. Dimensions of social support and social conflict as predictors of caregiver depression. Int. Psychogeriatr. 1995, 7, 25–38. [Google Scholar] [CrossRef]
- Manso Martínez, M.E.; Sánchez López, M.d.P.; Cuéllar Flores, I. Salud y sobrecarga percibida en personas cuidadoras familiares de una zona rural. Clin Salud 2013, 24, 37–45. [Google Scholar] [CrossRef][Green Version]
- Moral Serrano, M.; Juan Ortega, J.; López Matoses, M.J.; Pellicer Magraner, P. Perfil y riesgo de morbilidad psíquica en cuidadores de pacientes ingresados en su domicilio. Aten. Primaria 2003, 32, 77–83. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Neri, A.L.; Yassuda, M.S.; Fortes-Burgos, A.C.G.; Mantovani, E.P.; Arbex, F.S.; Torres, S.V.d.S.; Perracini, M.R.; Guariento, M.E. Relationships between gender, age, family conditions, physical and mental health, and social isolation of elderly caregivers. Int. Psychogeriatr. 2012, 24, 472–483. [Google Scholar] [CrossRef]
- Pagel, M.; Becker, J. Depressive thinking and depression: Relations with personality and social resources. J. Personal. Soc. Psychol. 1987, 52, 1043. [Google Scholar] [CrossRef]
- Pagnini, F.; Rossi, G.; Lunetta, C.; Banfi, P.; Castelnuovo, G.; Corbo, M.; Molinari, E. Burden, depression, and anxiety in caregivers of people with amyotrophic lateral sclerosis. Psychol. Health Med. 2010, 15, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.J.; Singer, J.L.; Prigerson, H.G. Religious coping among caregivers of terminally ill cancer patients: Main effects and psychosocial mediators. J. Health Psychol. 2006, 11, 743–759. [Google Scholar] [CrossRef]
- Rapp, S.R.; Shumaker, S.; Schmidt, S.; Naughton, M.; Anderson, R. Social resourcefulness: Its relationship to social support and wellbeing among caregivers of dementia victims. Aging Ment. Health 1998, 2, 40–48. [Google Scholar] [CrossRef]
- Rauktis, M.E.; Koeske, G.F.; Tereshko, O. Negative social interactions, distress, and depression among those caring for a seriously and persistently mentally III relative. Am. J. Community Psychol. 1995, 23, 279–299. [Google Scholar] [CrossRef]
- Rivera, P.A.; Rose, J.M.; Futterman, A.; Lovett, S.B.; Gallagher-Thompson, D. Dimensions of perceived social support in clinically depressed and nondepressed female caregivers. Psychol. Aging 1991, 6, 232. [Google Scholar] [CrossRef]
- Rivera-Navarro, J.; Sepúlveda, R.; Contador, I.; Fernández-Calvo, B.; Ramos, F.; Tola-Arribas, M.Á.; Goñi, M. Detection of maltreatment of people with dementia in Spain: Usefulness of the Caregiver Abuse Screen (CASE). Eur. J. Ageing 2018, 15, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.M. Predictors of depression among wife caregivers. Nurs. Res. 1989, 38, 359–363. [Google Scholar] [CrossRef]
- Robinson, K.M.; Kaye, J. The relationship between spiritual perspective, social support, and depression in caregiving and noncaregiving wives. Sch. Inq. Nurs. Pract. 1994, 8, 375–389. [Google Scholar]
- Rodakowski, J.; Skidmore, E.R.; Rogers, J.C.; Schulz, R. Does social support impact depression in caregivers of adults ageing with spinal cord injuries? Clin. Rehabil. 2013, 27, 565–575. [Google Scholar] [CrossRef]
- Rodi, N. Understanding Posttraumatic Stress Symptoms in Caregivers and Relatives of Adults Surviving Cancer; Hofstra University: Hempstead, NY, USA, 2015. [Google Scholar]
- Sahin, Z.A.; Tan, M. Loneliness, depression, and social support of patients with cancer and their caregivers. Clin. J. Oncol. Nurs. 2012, 16, 2. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sandoval, F.; Tamiya, N.; Lloyd-Sherlock, P.; Noguchi, H. The relationship between perceived social support and depressive symptoms in informal caregivers of community-dwelling older persons in Chile. Psychogeriatrics 2019, 19, 547–556. [Google Scholar] [CrossRef]
- Schulz, R.; Williamson, G.M. A 2-year longitudinal study of depression among Alzheimer’s caregivers. Psychol. Aging 1991, 6, 569. [Google Scholar] [CrossRef]
- Schumacher, K.L.; Dodd, M.J.; Paul, S.M. The stress process in family caregivers of persons receiving chemotherapy. Res. Nurs. Health 1993, 16, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, K.A.; Roberts, B.L. Social support and strain of family caregivers of older adults. Holist. Nurs. Pract. 2000, 14, 77–90. [Google Scholar] [CrossRef]
- Scicolone, M.A. Examining Pathways of the Caregiver Burden-Health Relationship in Family Caregivers of Elderly Veterans: The Importance of Caregiver Self-Efficacy and Social Support; The University of Alabama: Tuscaloosa, AL, USA, 2018. [Google Scholar]
- Serrani, D. Influencia de apoyo social y uso de servicios de salud sobre la depresión en cuidadores de adultos mayores en zona rural. Rev. Chil. Salud Pública 2014, 18, 61–71. [Google Scholar] [CrossRef]
- Serrano-Ortega, N. Afrontamiento, Sobrecarga Subjetiva y Ansiedad y Síntomas Depresivos en Personas Cuidadoras de Familiares Mayores Dependientes. Ph.D. Thesis, University of Jaén, Jaén, Spain, 2017. [Google Scholar]
- Shaughnessy, V. The Impact of Mild Cognitive Impairment on Spouses: A Multi-Modal Investigation; York University: Toronto, ON, Canada, 2011. [Google Scholar]
- Shukri, M.; Mustofai, M.A.; Md Yasin, M.A.S.; Tuan Hadi, T.S. Burden, quality of life, anxiety, and depressive symptoms among caregivers of hemodialysis patients: The role of social support. Int. J. Psychiatry Med. 2020, 55, 397–407. [Google Scholar] [CrossRef]
- Speer, D.C. Predicting Parkinson’s Disease patient and caregiver adjustment: Preliminary findings. Behav. Health Aging 1993, 3, 139–146. [Google Scholar]
- Steffen, A.M.; McKibbin, C.; Zeiss, A.M.; Gallagher-Thompson, D.; Bandura, A. The revised scale for caregiving self-efficacy: Reliability and validity studies. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.F.; Perrin, P.B.; Gulin, S.B.; Rogers, H.L.; Cabrera, T.V.; Jiménez-Maldonado, M.; Arango-Lasprilla, J.C. Examining the influence of three types of social support on the mental health of Mexican caregivers of individuals with traumatic brain injury. Am. J. Phys. Med. Rehabil. 2013, 92, 959–967. [Google Scholar] [CrossRef]
- Tang, F.; Jang, H.; Lingler, J.; Tamres, L.K.; Erlen, J.A. Stressors and caregivers’ depression: Multiple mediators of self-efficacy, social support, and problem-solving skill. Soc. Work Health Care 2015, 54, 651–668. [Google Scholar] [CrossRef]
- Thielemann, P.A. Coping Style and Social Support Effects on Depression in Spousal Caregivers of Patients with Advanced Lung Cancer; University of South Florida: Tampa, FL, USA, 2001. [Google Scholar]
- Verez Cotelo, N.; Andrés Rodríguez, N.F.; Fornos Pérez, J.A.; Andrés Iglesias, J.C.; Ríos Lago, M. Burden and associated pathologies in family caregivers of Alzheimer’s disease patients in Spain. Pharm. Pract. 2015, 13, 2. [Google Scholar] [CrossRef]
- Yen, W.; Lundeen, S. The association between meaning of caregiving, perceived social support and level of depression of Taiwanese caregivers of mentally ill patients. Int. J. Psychiatr. Nurs. Res. 2006, 12, 1378–1392. [Google Scholar] [PubMed]
- Yoon, H. Factors associated with family caregivers’ burden and depression in Korea. Int. J. Aging Hum. Dev. 2003, 57, 291–311. [Google Scholar] [CrossRef]
- Yun, S. Application of the Sociocultural Stress and Coping Model on Spousal Caregivers of Korean Older Adults; University of Colorado Springs: Colorado Springs, CO, USA, 2023. [Google Scholar]
- Schiller, V.F.; Dorstyn, D.S.; Taylor, A.M. The Protective Role of Social Support Sources and Types Against Depression in Caregivers: A Meta-Analysis. J. Autism Dev. Disord. 2021, 51, 1304–1315. [Google Scholar] [CrossRef]
- Santini, Z.I.; Koyanagi, T.; Tyrovolas, S.; Mason, C.; Haro, J.M. The association between social relationships and depression: A systematic review. J. Affect. Disord. 2015, 175, 53–65. [Google Scholar] [CrossRef]
- Tengku Mohd, T.A.M.; Yunus, R.M.; Hairi, F.; Hairi, N.N.; Choo, W.Y. Social support and depression among community dwelling older adults in Asia: A systematic review. BMJ Open 2019, 9, e026667. [Google Scholar] [CrossRef] [PubMed]
- Del-Pino-Casado, R.; Frias-Osuna, A.; Palomino-Moral, P.A.; Ruzafa-Martinez, M.; Ramos-Morcillo, A.J. Social support and subjective burden in caregivers of adults and older adults: A meta-analysis. PLoS ONE 2018, 13, e0189874. [Google Scholar] [CrossRef]
- Priego-Cubero, E.; Orgeta, V.; López-Martínez, C.; del-Pino-Casado, R. The Relationship between Social Support and Anxiety Symptoms in Informal Carers: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1244. [Google Scholar] [CrossRef]
- Cohen, S.; Gottlieb, B.H.; Underwood, L.G. (Eds.) Social relationships and health. In Social Support Measurement and Intervention: A Guide for Health and Social Scientists; Oxford University Press: New York, NY, USA, 2000; pp. 3–25. [Google Scholar]
- Dam, A.E.; de Vugt, M.E.; Klinkenberg, I.P.; Verhey, F.R.; van Boxtel, M.P. A systematic review of social support interventions for caregivers of people with dementia: Are they doing what they promise? Maturitas 2016, 85, 117–130. [Google Scholar] [CrossRef]
- Rui, J.R.; Guo, J. Differentiating the stress buffering functions of perceived versus received social support. Curr. Psychol. 2022, 42, 13432–13442. [Google Scholar] [CrossRef]
- Grey, I.; Arora, T.; Thomas, J.; Saneh, T.; Tohme, P.; Abi-Habib, R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020, 293, 113452. [Google Scholar] [CrossRef] [PubMed]
- Uchino, B.N. Understanding the links between social support and physical health: A life-span perspective with emphasis on the separability of perceived and received support. Perspect. Psychol. Sci. 2009, 4, 236–255. [Google Scholar] [CrossRef] [PubMed]





| Author and Year | Subgroup | Type | Selection | Classification | Confounding | Attrition |
|---|---|---|---|---|---|---|
| Aggar 2010 [30] | − | + | ? | NA | ||
| Ali 2016 [31] | − | + | + | NA | ||
| Amorim 2009 [32] | − | + | ? | NA | ||
| Ar 2017 [32] | − | + | ? | NA | ||
| Arevalo-Flechas 2014 [34] | − | + | ? | NA | ||
| Asti 2006 [35] | − | + | ? | NA | ||
| Au 2009 [36] | − | + | + | NA | ||
| Azevedo 2017 [37] | − | + | + | NA | ||
| Baillie 1988 [38] | − | + | ? | NA | ||
| Ballard 1995 [39] | − | + | ? | NA | ||
| Bambara 2014 [40] | − | + | + | NA | ||
| Bergman 1992 [41] | − | + | ? | NA | ||
| Bigatti 2011 [42] | − | + | ? | NA | ||
| Bonsu 2019 [43] | − | + | ? | NA | ||
| Burgeois 1996 [44] | − | + | ? | NA | ||
| Burton 2008 [45] | − | + | + | NA | ||
| Butler 2001 [46] | − | + | + | NA | ||
| Cabral 2014 [47] | − | + | + | NA | ||
| Calvete 2011 [48] | − | + | ? | NA | ||
| Cardenas 2004 [49] | − | + | ? | NA | ||
| Chai 2018 [50] | − | + | ? | NA | ||
| Chou 2010 [51] | − | + | ? | NA | ||
| Chow 2012 [52] | − | + | − | NA | ||
| Clyburn 2000 [53] | + | + | ? | NA | ||
| Crespo 2005 [54] | − | + | ? | NA | ||
| Cumming 2008 [55] | − | + | ? | NA | ||
| Decker 1989 [56] | − | ? | ? | NA | ||
| Del-Pino-Casado 2022 [57] | + | + | + | + | ||
| Durkin 2010 [58] | − | + | ? | ? | ||
| Faber 2005 [59] | − | + | ? | NA | ||
| Gibson 2013 [60] | − | + | − | NA | ||
| Giovannetti 2015 [61] | − | + | ? | NA | ||
| Grant 2000 [62] | − | + | ? | NA | ||
| Grant 2001 [63] | − | + | ? | NA | ||
| Graven 2020 [64] | − | + | + | NA | ||
| Haley 1987 [65] | − | + | ? | NA | ||
| Han 2014 [66] | − | + | ? | NA | ||
| Harwood 2000 [67] | − | + | + | NA | ||
| Hasson-Ohayon 2010 [68] | − | + | ? | NA | ||
| Hobbs 1997 [69] | + | + | ? | NA | ||
| Hwang 2011 [70] | − | + | ? | NA | ||
| Jeong 2017 [71] | − | + | ? | NA | ||
| Khusaifan 2017 [72] | − | + | ? | NA | ||
| Kiral 2017 [73] | − | + | ? | NA | ||
| Koerner 2010 [74] | − | + | + | NA | ||
| Kruithof 2016 [75] | − | + | ? | + | ||
| Kusku 2009 [76] | − | + | ? | NA | ||
| Lakey 2002 [77] | − | + | ? | NA | ||
| Lee 2003 [78] | + | + | + | NA | ||
| Leibach 2013 [79] | − | + | − | NA | ||
| Li 1997 [80] | Daughter | Emotional | + | + | + | NA |
| Li 1997 [80] | Daughter | Global | + | + | + | NA |
| Li 1997 [80] | Daughter | Instrumental | + | + | − | NA |
| Li 1997 [80] | Wife | Emotional | + | + | + | NA |
| Li 1997 [80] | Wife | Global | + | + | + | NA |
| Li 1997 [80] | Wife | Instrumental | + | + | − | NA |
| Li 2019 [81] | + | + | + | NA | ||
| Losada 2010 [82] | − | + | ? | NA | ||
| Luchsinger 2015 [83] | − | + | ? | NA | ||
| Majerovitz 2007 [84] | − | + | ? | NA | ||
| MaloneBeach 1995 [85] | − | + | ? | NA | ||
| Manso Martinez 2013 [86] | Men | − | + | − | NA | |
| Manso Martinez 2013 [86] | Women | − | + | + | NA | |
| Moral Serrano 2003 [87] | + | + | ? | NA | ||
| Neri 2012 [88] | − | + | ? | NA | ||
| Nuwamanya 2023 [11] | − | + | ? | NA | ||
| Pagel 1987 [89] | − | + | ? | NA | ||
| Pagnini 2010 [90] | − | + | + | NA | ||
| Pearce 2006 [91] | − | + | ? | NA | ||
| Raad 2020 [14] | − | + | ? | NA | ||
| Rapp 1998 [92] | − | + | − | NA | ||
| Rauktis 1995 [93] | + | + | − | NA | ||
| Rivera 1991 [94] | − | + | ? | NA | ||
| Rivera-Navarro 2018 [95] | − | + | + | NA | ||
| Robinson 1989 [96] | − | + | ? | NA | ||
| Robinson 1994 [97] | − | + | ? | NA | ||
| Rodakowski 2013 [98] | + | + | ? | NA | ||
| Rodi 2015 [99] | − | + | ? | NA | ||
| Sahin 2012 [100] | − | + | ? | NA | ||
| Sandoval 2019 [101] | − | + | − | NA | ||
| Schulz 1991 [102] | − | + | ? | NA | ||
| Schumacher 1993 [103] | − | + | − | NA | ||
| Schwarz 2000 [104] | − | + | ? | NA | ||
| Scicolone 2018 [105] | − | + | + | NA | ||
| Serrani 2014 [106] | + | + | ? | NA | ||
| Serrano-Ortega 2017 [107] | + | + | + | + | ||
| Shaughnessy 2011 [108] | − | + | ? | NA | ||
| Shukri 2020 [109] | − | + | ? | NA | ||
| Speer 1993 [110] | − | + | ? | NA | ||
| Steffen 2002 [111] | − | + | ? | NA | ||
| Stevens 2013 [112] | − | + | + | NA | ||
| Tay 2022 [12] | − | + | ? | NA | ||
| Tang 2015 [113] | − | + | + | NA | ||
| Thielemann 2001 [114] | − | + | + | NA | ||
| Verez Cotelo 2015 [115] | − | + | ? | NA | ||
| Yen 2006 [116] | − | + | ? | NA | ||
| Yoon 2003 [117] | Emotional | − | + | − | NA | |
| Yoon 2003 [117] | Global | − | + | ? | NA | |
| Yoon 2003 [117] | Instrumental | − | + | − | NA | |
| Yun 2023 [118] | + | ? | + | NA | ||
| Zhong 2020 [13] | + | + | ? | NA |
| Type of Social Support | Global/ Dimensions | Whole Sample/Subgroups | K | N | Average N | Combined Effect | Heterogeneity | Sensitivity Analyses | Publication Bias | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | Lower Limit | Upper Limit | Q (df) | p | I2 | Funnel | Egger’s | Trim & Fill | ||||||||||
| Criterion | Categories | r Max | % | p-Value | r | % | ||||||||||||
| Perceived | Global | Whole sample | -- | 78 | 11,835 | 151.7 | −0.35 | −0.39 | −0.31 | 49.6 (77) | 0.99 | 0.0 | −0.33 | 5.7 | Asym | 0.19 | −0.3 | 14.3 |
| Type of care-recipient | Dementia | 20 | 2507 | 125.4 | −0.31 | −0.37 | −0.26 | 18.4 (19) | 0.5 | 0.0 | −0.33 | 5.2 | Asym | 0.38 | −0.29 | 7.6 | ||
| Frail older p | 17 | 1753 | 103.1 | −0.30 | −0.38 | −0.23 | 12.1 (16) | 0.73 | 0.0 | −0.29 | 4.7 | Asym | 0.08 | −0.3 | 0.0 | |||
| Cancer | 13 | 1813 | 139.5 | −0.37 | −0.44 | −0.31 | 11.1 (12) | 0.52 | 0.0 | −0.39 | 5.4 | Sym | 0.53 | −0.37 | 0.0 | |||
| Mental Illness | 5 | 530 | 106.0 | −0.26 | −0.38 | −0.12 | 4.4 (4) | 0.35 | 9.4 | −0.21 | 19.2 | NV | NV | NV | NV | |||
| Stroke | 4 | 298 | 74.5 | −0.29 | −0.38 | −0.20 | 2.8 (3) | 9.42 | 0.0 | −0.27 | 7.4 | NV | NV | NV | NV | |||
| Design | Cross-sectional | 75 | 11,447 | 152.6 | −0.35 | −0.39 | −0.31 | 48.0 (74) | 0.99 | 0.0 | −0.33 | 4.9 | Asym | 0.2 | −0.3 | 14.3 | ||
| Longitudinal | 3 | 388 | 129.3 | −0.33 | −0.41 | −0.24 | 0.029 (2) | 0.99 | 0.0 | −0.32 | 1.1 | NV | NV | NV | NV | |||
| Sampling | Prob | 10 | 2368 | 236.8 | −0.30 | −0.36 | −0.23 | 6.2 (9) | 0.72 | 0.0 | −0.32 | 4.8 | Asym | 0.95 | −0.27 | 11.3 | ||
| Non-prob | 68 | 9467 | 139.2 | −0.36 | −0.40 | −0.31 | 40.7 (67) | 0.99 | 0.0 | −0.34 | 4.1 | Asym | 0.22 | −0.3 | 15.7 | |||
| Control of confounders | Yes | 20 | 876 | 43.8 | −0.40 | −0.50 | −0.29 | 9.3 (19) | 0.97 | 0.0 | −0.37 | 8.9 | Asym | 0.45 | −0.45 | 11.7 | ||
| No | 58 | 10,959 | 188.9 | −0.32 | −0.36 | −0.29 | 49.3 (57) | 0.76 | 0.0 | −0.33 | 1.5 | Asym | 0.002 | −0.29 | 10.2 | |||
| Emotional | Whole sample | -- | 7 | 624 | 89.1 | −0.35 | −0.45 | −0.25 | 7.4 (6) | 0.29 | 19.1 | −0.38 | 9.4 | Asym | NV | −0.35 | 0.0 | |
| Instrumental | Whole sample | -- | 3 | 365 | 121.7 | −0.35 | −0.44 | −0.26 | 0.012 (2) | 0.99 | 0.0 | −0.36 | 0.8 | NV | NV | NV | NV | |
| Received | Global | Whole sample | -- | 12 | 3470 | 289.2 | −0.14 | −0.20 | −0.07 | 12.8 (11) | 0.31 | 13.8 | −0.12 | 12.9 | Asym | 0.48 | −0.13 | 7.1 |
| Emotional | Whole sample | -- | 3 | 620 | 206.7 | −0.15 | −0.23 | −0.07 | 1.4 (2) | 0.5 | 0.0 | −0.20 | 28.2 | NV | NV | NV | NV | |
| Instrumental | Whole sample | -- | 3 | 620 | 206.7 | −0.14 | −0.26 | −0.02 | 2.0 (2) | 0.37 | 1.9 | −0.20 | 36.3 | NV | NV | NV | NV | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Sánchez, B.; Orgeta, V.; López-Martínez, C.; del-Pino-Casado, R. Association between Social Support and Depressive Symptoms in Informal Caregivers of Adult and Older Dependents: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6468. https://doi.org/10.3390/jcm12206468
Gutiérrez-Sánchez B, Orgeta V, López-Martínez C, del-Pino-Casado R. Association between Social Support and Depressive Symptoms in Informal Caregivers of Adult and Older Dependents: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(20):6468. https://doi.org/10.3390/jcm12206468
Chicago/Turabian StyleGutiérrez-Sánchez, Belén, Vasiliki Orgeta, Catalina López-Martínez, and Rafael del-Pino-Casado. 2023. "Association between Social Support and Depressive Symptoms in Informal Caregivers of Adult and Older Dependents: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 20: 6468. https://doi.org/10.3390/jcm12206468
APA StyleGutiérrez-Sánchez, B., Orgeta, V., López-Martínez, C., & del-Pino-Casado, R. (2023). Association between Social Support and Depressive Symptoms in Informal Caregivers of Adult and Older Dependents: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(20), 6468. https://doi.org/10.3390/jcm12206468