
Depression in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis


 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
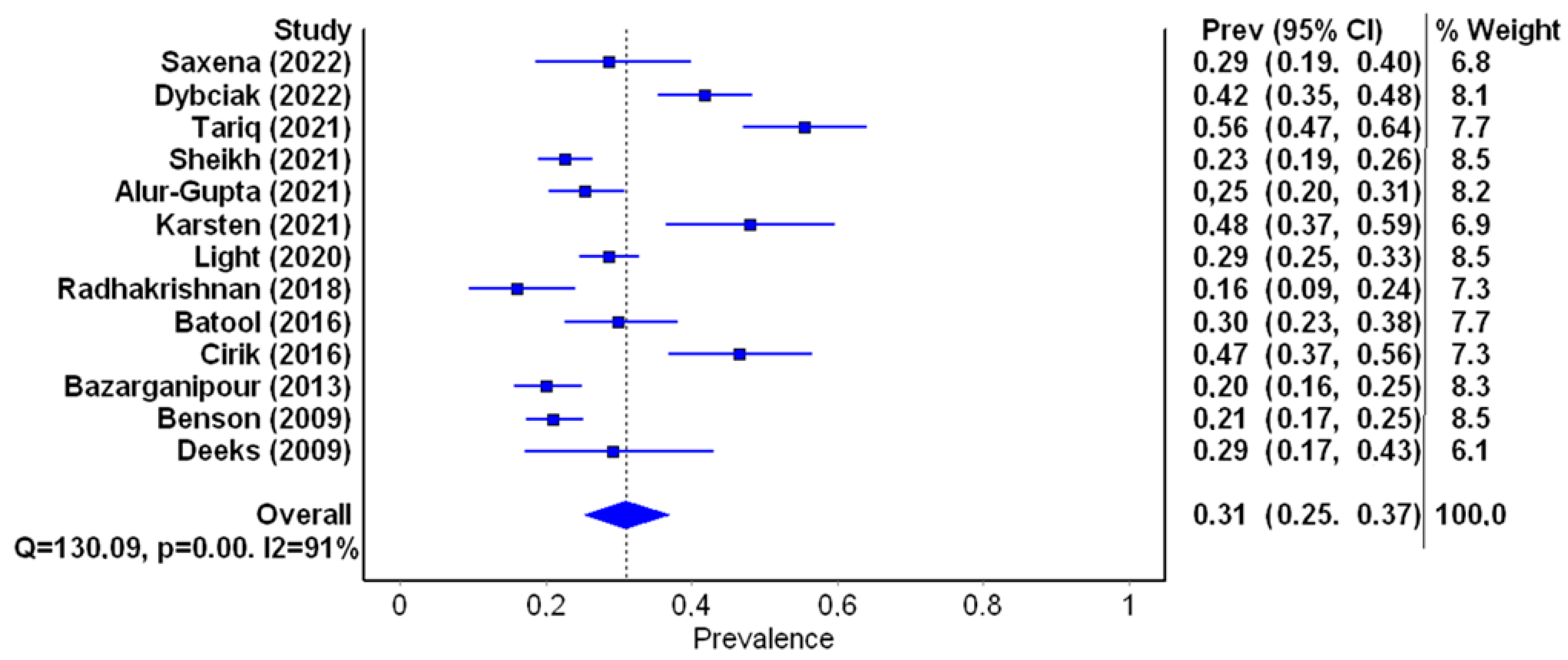
- Prevalence of depression;
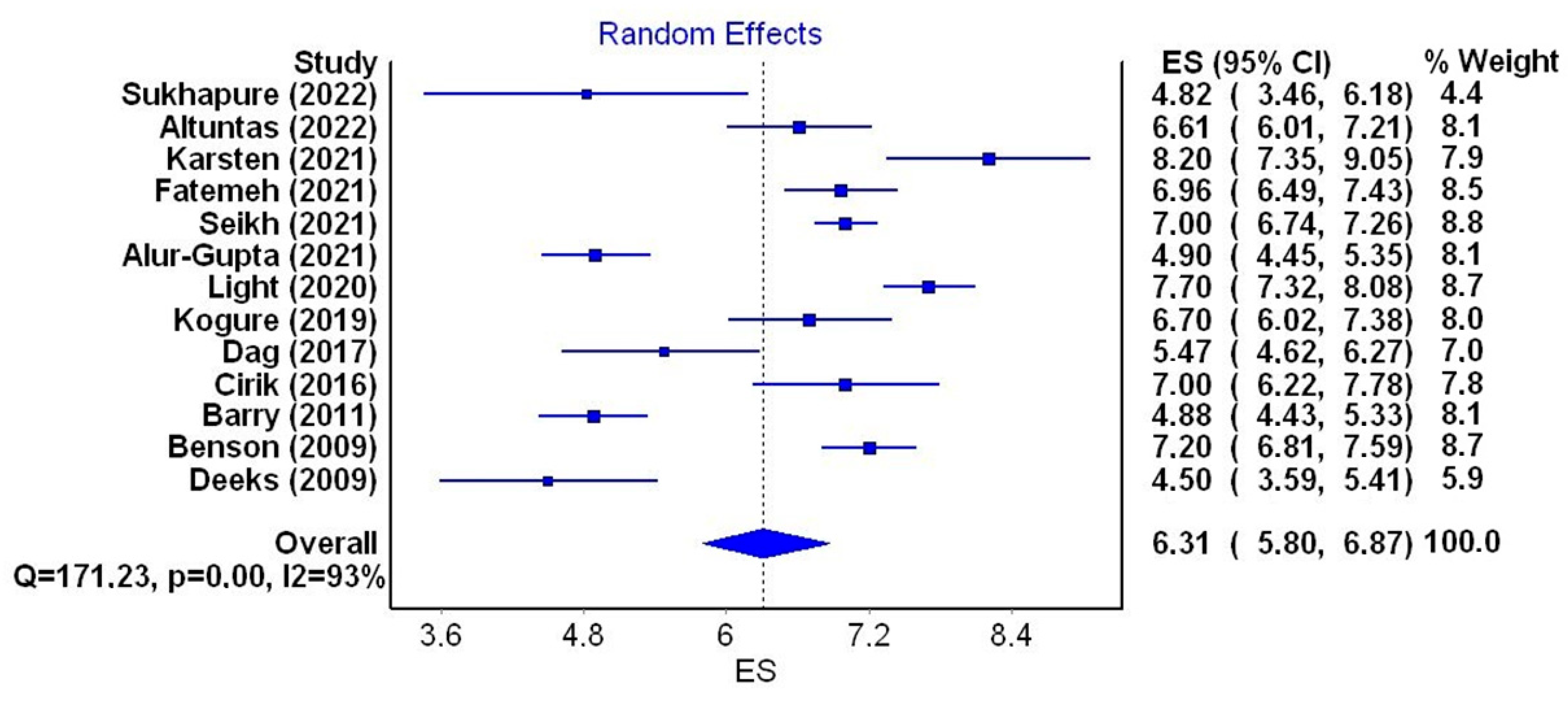
- Mean level of depression;
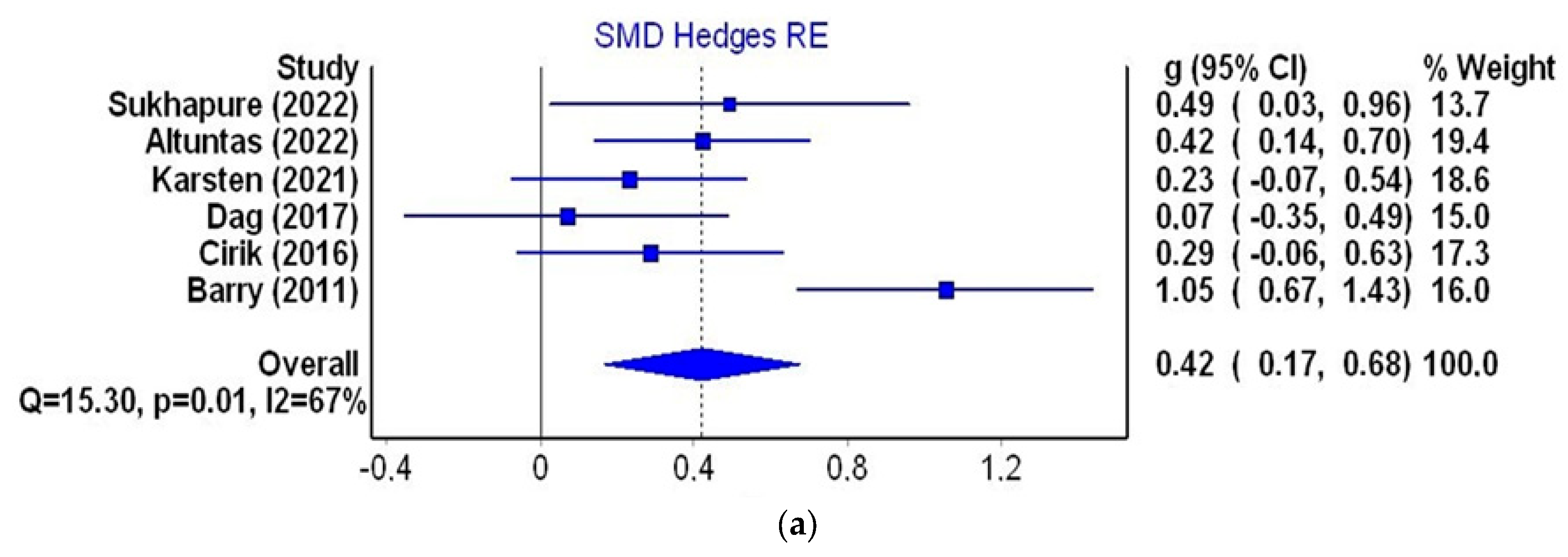
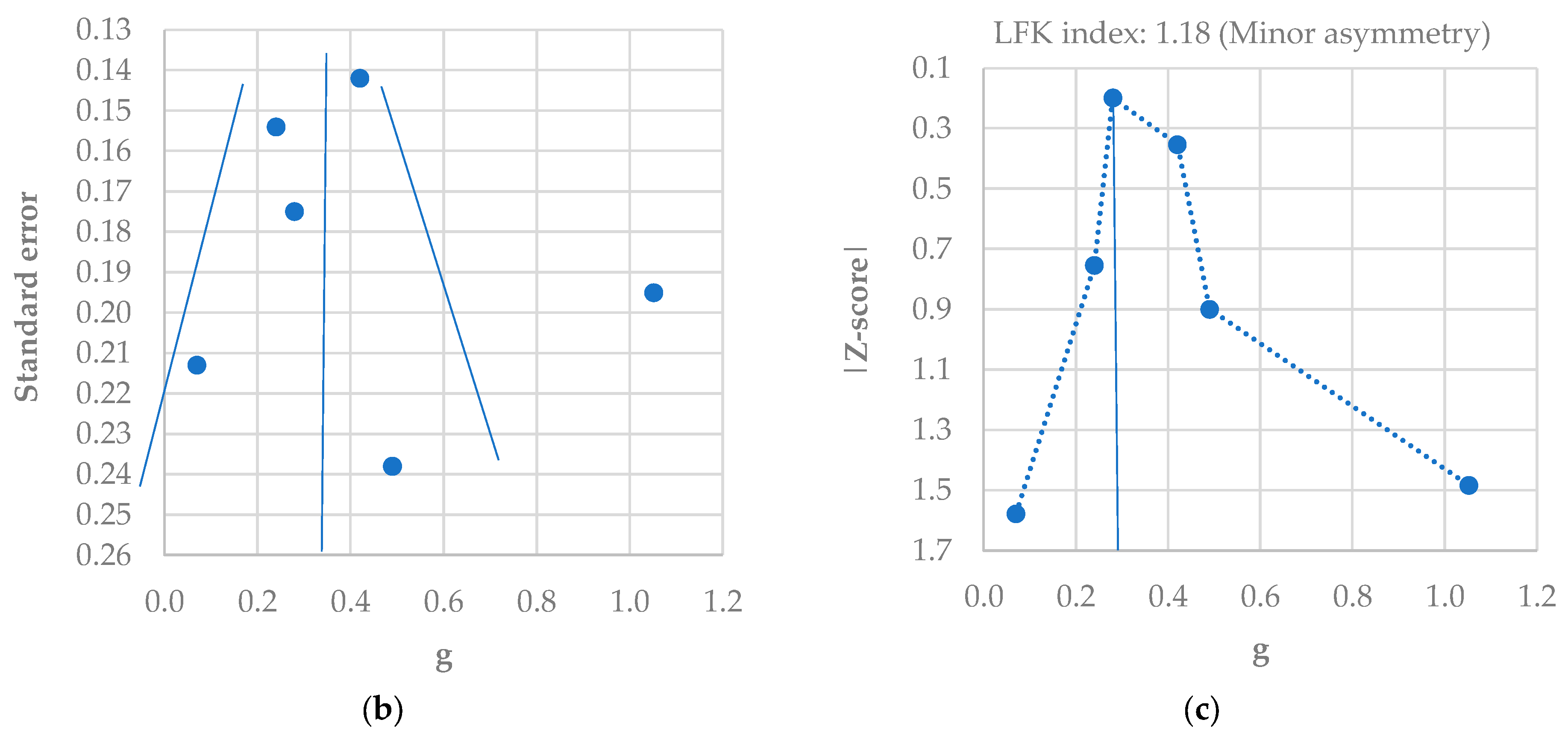
- Standardized difference in mean scores in groups of women with PCOS and healthy ones;
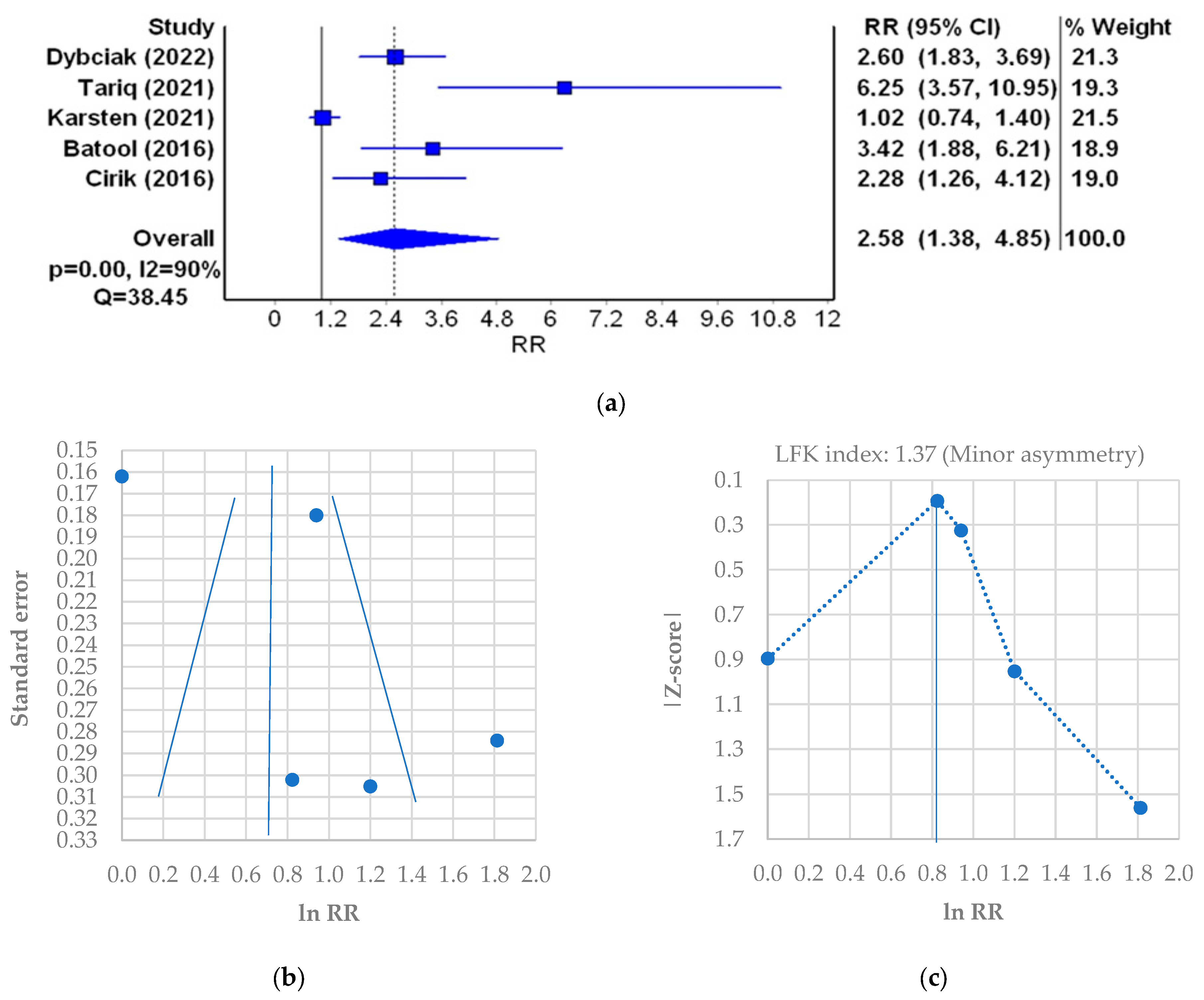
- Probability of depression based on studies performed using the Hospital Anxiety and Depression Scale (HADS).
2. Materials and Methods
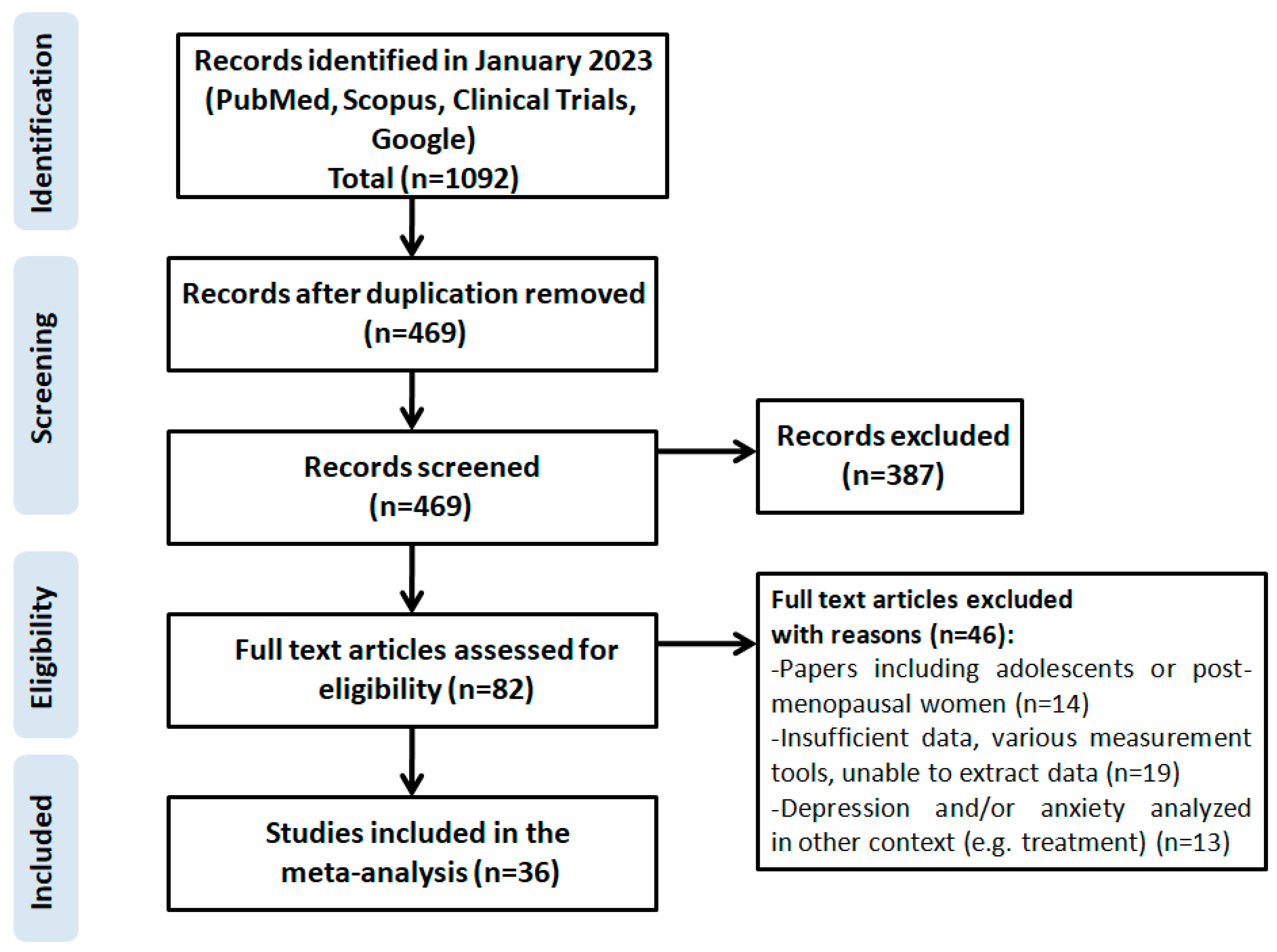
2.1. Search Methodology
2.2. Eligibility
- The study included adult women aged over 18 years;
- The study included pre-menopausal women;
- The study included women who were diagnosed with polycystic ovary syndrome based on the criteria developed by the National Institutes of Health (NIH), the Rotterdam consensus or others [41];
- It was possible to extract from the text the information about the prevalence of depressive symptoms in the study group;
- It was possible to extract the HADS-D score from the text;
- The study group included 30 patients or more;
- Abstracts were qualified if they contained all the needed information mentioned above.
- Review/case report/meta-analysis/systemic review;
- Studies not written in English;
- Studies in which adolescent or post-menopausal women were recruited;
- Studies that did not assess the level and prevalence of mental disorders using the HADS;
- Studies that assessed the effectiveness of a drug and one of the indicators was the level of depression;
- Studies in which depressive disorders were assessed only in terms of obesity, infertility, hirsutism or other symptoms of PCOS;
- Studies that included pregnant patients with PCOS.
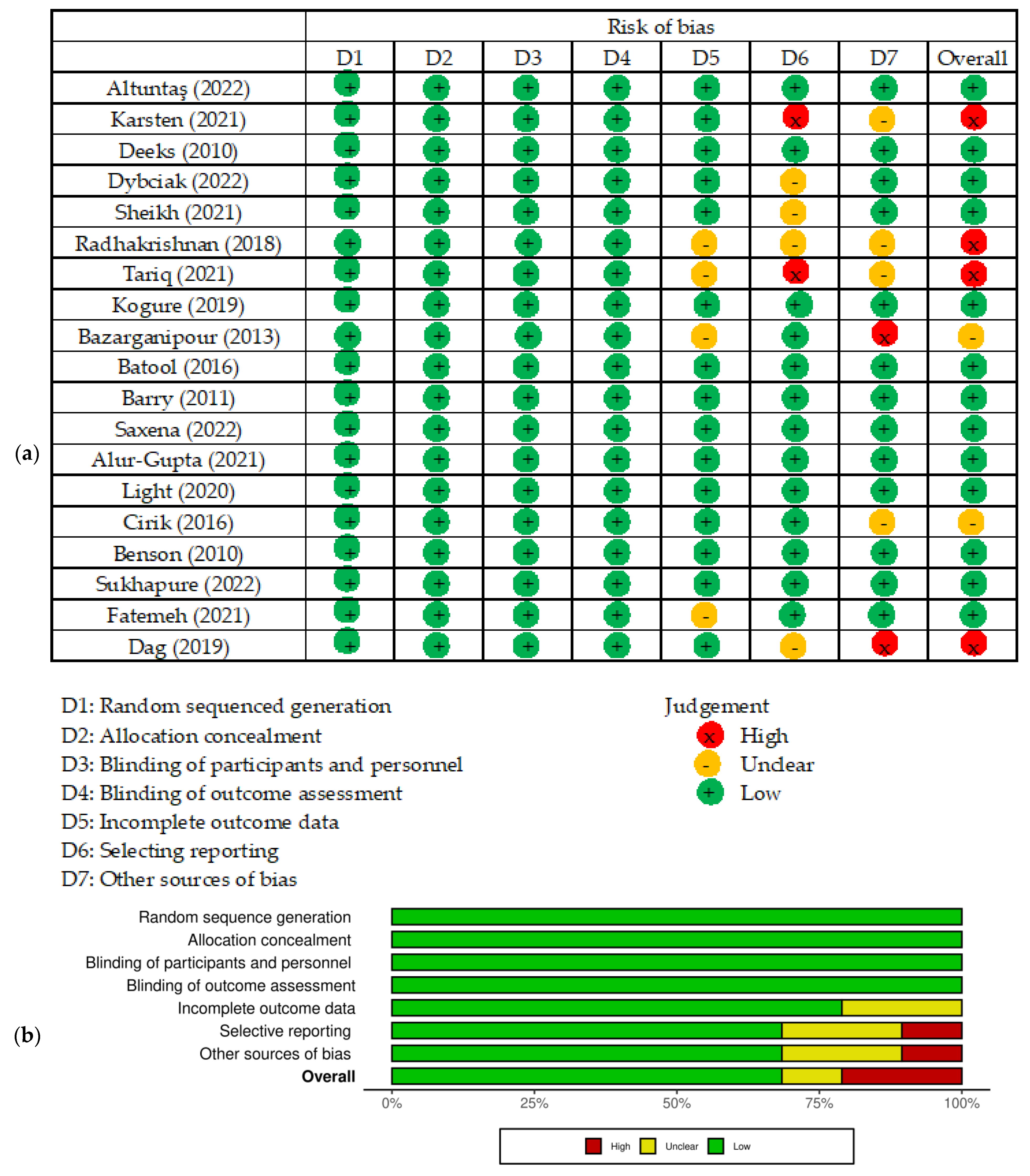
2.3. Data Analysis
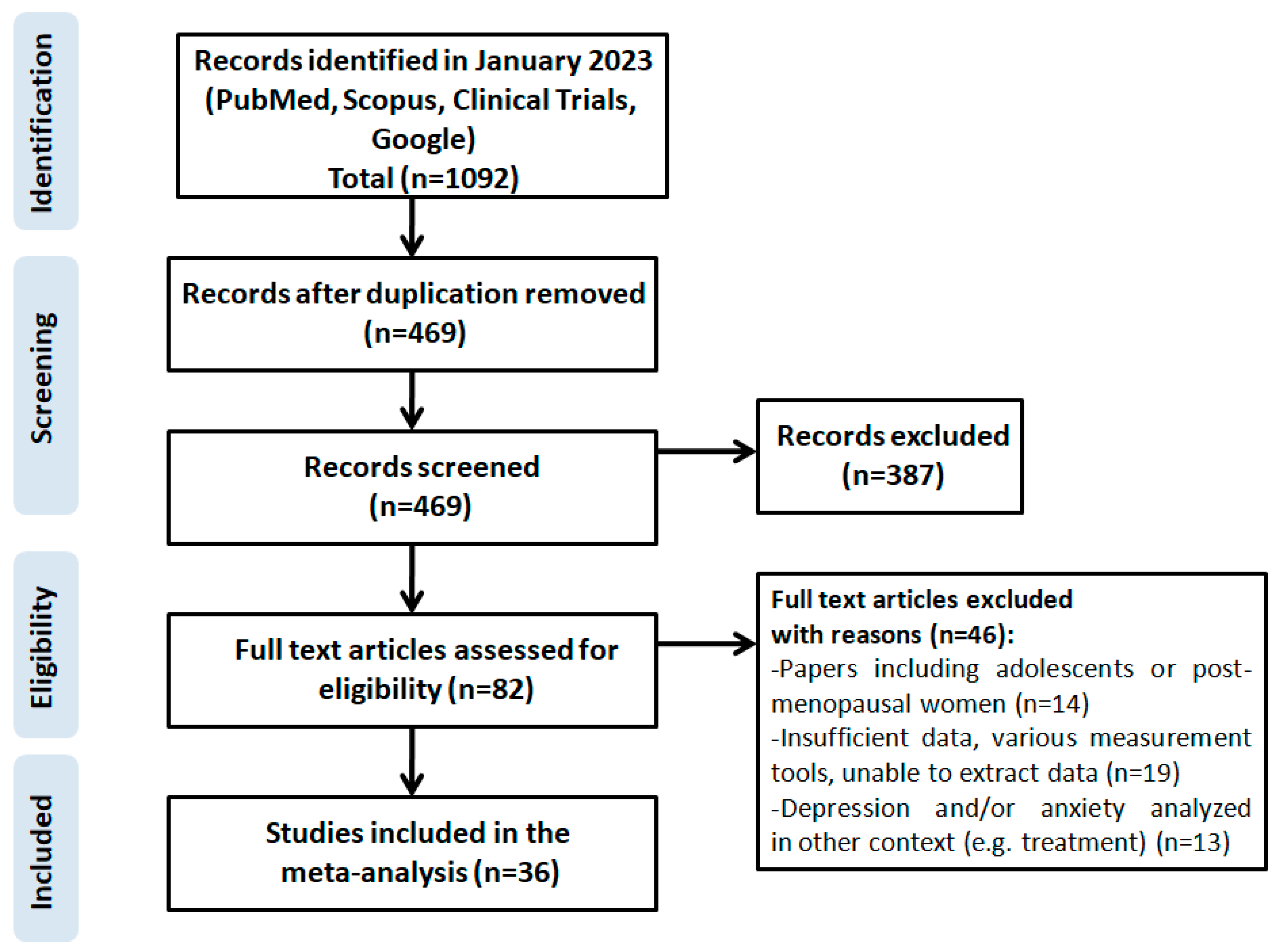
2.4. Search Results
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2016, 31, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Lizneva, D.; Suturina, L.; Walker, W.; Brakta, S.; Gavrilova-Jordan, L.; Azziz, R. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil. Steril. 2016, 106, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Nidhi, R.; Padmalatha, V.; Nagarathna, R.; Amritanshu, R. Prevalence of Polycystic Ovarian Syndrome in Indian Adolescents. J. Pediatr. Adolesc. Gynecol. 2011, 24, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Cedars, M.I. Current Guidelines for Diagnosing PCOS. Diagnostics 2023, 13, 1113. [Google Scholar] [CrossRef]
- Fauser, B.C.; Tarlatzis, B.C.; Rebar, R.W.; Legro, R.S.; Balen, A.H.; Lobo, R.; Carmina, E.; Chang, J.; Yildiz, B.O.; Laven, J.S.; et al. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): The Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil. Steril. 2012, 97, 28–38.e25. [Google Scholar] [CrossRef]
- Çetinkaya, A.S.; Çelik, Ö.; Özer, Ü.; Çolak, S. Depression, anxiety, body image scores, and sexual dysfunction in patients with polycystic ovary syndrome according to phenotypes. Gynecol. Endocrinol. 2022, 38, 849–855. [Google Scholar] [CrossRef]
- Karsten, M.D.A.; Wekker, V.; Groen, H.; Painter, R.C.; Mol, B.W.J.; Laan, E.T.M.; Roseboom, T.J.; Hoek, A. The role of PCOS in mental health and sexual function in women with obesity and a history of infertility. Hum. Reprod. Open. 2021, 2021, hoab038. [Google Scholar] [CrossRef]
- Ali, A.T. Polycystic ovary syndrome and metabolic syndrome. Ceska Gynekol. 2015, 80, 279–289. [Google Scholar]
- Borghi, L.; Leone, D.; Vegni, E.; Galiano, V.; Lepadatu, C.; Sulpizio, P.; Garzia, E. Psychological distress, anger and quality of life in polycystic ovary syndrome: Associations with biochemical, phenotypicalandsocio-demographic factors. J. Psychosom. Obstet. Gynecol. 2018, 39, 128–137. [Google Scholar] [CrossRef]
- Papalou, O.; Diamanti-Kandarakis, E. The role of stress in PCOS. Expert Rev. Endocrinol. Metab. 2017, 12, 87–95. [Google Scholar] [CrossRef]
- Gholinezhad, M.; Golsorkhtabaramiri, M.; Esmaeilzadeh, S.; Ghanbarpour, A. Insulin resistance and adverse metabolic profile in overweight/obese and normal weight of young women with polycystic ovary syndrome. Casp. J. Intern. Med. 2018, 9, 260–267. [Google Scholar] [CrossRef]
- Legro, R.S.; Arslanian, S.A.; Ehrmann, D.A.; Hoeger, K.M.; Murad, M.H.; Pasquali, R.; Welt, C.K. Diagnosis and Treatment of Polycystic Ovary Syndrome: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocr. 2013, 98, 4565–4592. [Google Scholar] [CrossRef] [PubMed]
- Almeshari, W.K.; Alsubaie, A.K.; Alanazi, R.I.; Almalki, Y.A.; Masud, N.; Mahmoud, S.H. Depressive and Anxiety Symptom Assessment in Adults with Polycystic Ovarian Syndrome. Depress. Res. Treat. 2021, 2021, 6652133. [Google Scholar] [CrossRef] [PubMed]
- Brutocao, C.; Zaiem, F.; Alsawas, M.; Morrow, A.S.; Murad, M.H.; Javed, A. Psychiatric disorders in women with polycystic ovary syndrome: A systematic review and meta-analysis. Endocrine 2018, 62, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Deeks, A.A.; Gibson-Helm, M.E.; Teede, H.J. Anxiety and depression in polycystic ovary syndrome: A comprehensive investigation. Fertil. Steril. 2010, 93, 2421–2423. [Google Scholar] [CrossRef] [PubMed]
- Dybciak, P.; Humeniuk, E.; Raczkiewicz, D.; Krakowiak, J.; Wdowiak, A.; Bojar, I. Anxiety and Depression in Women with Polycystic Ovary Syndrome. Medicina 2022, 58, 942. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, J.; Hebbar, M.; Zia, N.; Wicks, S.; Jayaprakash, S.; Narendran, A.; Khalil, H.; Melson, E.; Busby, M.; Tahrani, A.; et al. Increased anxiety, depression and body dysmorphia in women with polycystic ovary syndrome: Results from blue morpho survey. Endocr. Abstr. 2021, 73, AEP175. [Google Scholar] [CrossRef]
- Zehravi, M.; Maqbool, M.; Ara, I. Depression and anxiety in women with polycystic ovarian syndrome: A literature survey. Int. J. Adolesc. Med. Health 2021, 33, 367–373. [Google Scholar] [CrossRef]
- Radhakrishnan, R.; Verghese, A. A study on anxiety and depression among patients with polycystic ovary syndrome. JDDT 2018, 8, 338–340. [Google Scholar] [CrossRef]
- Tariq, A.; Tariq, M.M.; Tariq, H.; Khattak, S.N.; Yazdani, T.; Malik, R.T.; Rauf, S.; Malik, T. Frequency and Risk Factors for Depression and Anxiety in Patients with Polycystic Ovary Syndrome Presenting in a Tertiary Care Hospital Karachi, Pakistan. J. Obstet. Gynaecol. 2021, 4, 196–202. [Google Scholar] [CrossRef]
- Mansson, M.; Holte, J.; Landin-Wilhelmsen, K.; Dahlgren, E.; Johansson, A.; Landén, M. Women with polycystic ovary syndrome are often depressed or anxious-A case control study. Psychneuroendocrinology 2008, 33, 1132–1138. [Google Scholar] [CrossRef]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [PubMed]
- Sadock, B.J.; Sadock, V.A. Mood disorders. In Kaplan & Sadock’s Synopsis of Psychiatry. Behavioral Sciences/Clinical Psychiatry, 10th ed.; WoltersKluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; pp. 527–568. [Google Scholar]
- Kowalczyk, M.; Kowalczyk, E.; Galita, G.; Majsterek, I.; Talarowska, M.; Popławski, T.; Kwiatkowski, P.; Lichota, A.; Sienkiewicz, M. Association of Polymorphic Variants in Argonaute Genes with Depression Risk in a Polish Population. Int. J. Mol. Sci. 2022, 23, 10586. [Google Scholar] [CrossRef] [PubMed]
- Gałecki, P.; Talarowska, M. Inflammatorytheory of depression. Psychiatr. Pol. 2018, 52, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Chu, J.; Zhang, X.; Ding, Z.; Song, Q.; Liu, Z.; Peng, W.; Cao, W.; Zou, T.; Yi, J. Psychologicalresilience and dailystressmediate the effect of childhood trauma on depression. Child Abus. Negl. 2022, 125, 105485. [Google Scholar] [CrossRef]
- Accortt, E.E.; Freeman, M.P.; Allen, J.J.B. Women and Major Depressive Disorder: Clinical Perspectives on Causal Pathways. J. Womens Health 2008, 17, 1583–1590. [Google Scholar] [CrossRef]
- Blay, S.L.; Aguiar, J.; Passos, I.C. Polycystic ovary syndrome and mental disorders: A systematic review and exploratory meta-analysis. Neuropsychiatr. Dis. Treat. 2016, 12, 2895–2903. [Google Scholar] [CrossRef]
- Cooney, L.G.; Lee, I.; Sammel, M.D.; Dokras, A. High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2017, 32, 1075–1091. [Google Scholar] [CrossRef]
- Dokras, A.; Clifton, S.; Futterweit, W.; Wild, R. Increased Risk for Abnormal Depression Scores in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Obstet. Gynecol. 2011, 17, 145–152. [Google Scholar] [CrossRef]
- Wang, Y.; Ni, Z.; Li, K. The prevalence of anxiety and depression of different severity in women with polycystic ovary syndrome: A meta-analysis. Gynecol. Endocrinol. 2021, 37, 1072–1078. [Google Scholar] [CrossRef]
- Yin, X.; Ji, Y.; Chan, C.L.; Chan, C.H.Y. The mental health of women with polycystic ovary syndrome: A systematic review and meta-analysis. Arch. Womens Ment. Health 2021, 24, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Kogure, G.S.; Ribeiro, V.B.; Lopes, I.P.; Furtado, C.L.M.; Kodato, S.; de Sá, M.F.S.; Ferriani, R.A.; Lara, L.A.d.S.; dos Reis, R.M. Body image and its relationships with sexual functioning, anxiety, and depression in women with polycystic ovary syndrome. J. Affect. Disord. 2019, 253, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Bazarganipour, F.; Ziaei, S.; Montazeri, A.; Foroozanfard, F.; Kazemnejad, A.; Faghihzadeh, S. Psychological investigation in patients with polycystic ovary syndrome. Health Qual. Life Outcomes 2013, 11, 141. [Google Scholar] [CrossRef]
- Batool, S.; Ul Ain Ahmed, F.; Ambreen, A.; Sheikh, A.; Faryad, N. Depression and Anxiety in Women with Polycystic Ovary Syndrome and Its Biochemical Associates. JSAFOG 2016, 8, 44–47. [Google Scholar] [CrossRef]
- Xing, L.; Xu, J.; Wei, Y.; Chen, Y.; Zhuang, H.; Tang, W.; Yu, S.; Zhang, J.; Yin, G.; Wang, R.; et al. Depression in polycystic ovary syndrome: Focusing on pathogenesis and treatment. Front. Psychiatry 2022, 13, 1001484. [Google Scholar] [CrossRef]
- Barry, J.A.; Kuczmierczyk, A.R.; Hardiman, P.J. Anxiety and depression in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2011, 26, 2442–2451. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety And Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Lujan, M.E.; Chizen, D.R.; Pierson, R.A. Diagnostic Criteria for Polycystic Ovary Syndrome: Pitfalls and Controversies. J. Obstet. Gynaecol. Can. 2008, 30, 671–679. [Google Scholar] [CrossRef]
- Saxena, R.; Singh, P.; Verma, A.; Sharma, M. Relationship between anxiety, depression and quality of life in medical student with polycystic ovary syndrome. Int. J. Reprod. Contracept. Obstet. Gynecol. 2022, 11, 35. [Google Scholar] [CrossRef]
- Alur-Gupta, S.; Lee, I.; Chemerinski, A.; Liu, C.; Lipson, J.; Allison, K.; Gallop, R.; Dokras, A. Racial differences in anxiety, depression, and quality of life in women with polycystic ovary syndrome. F&S Rep. 2021, 2, 230–237. [Google Scholar] [CrossRef]
- Light, R.S.; Chilcot, J.; McBride, E. Psychological Distress in Women Living with Polycystic Ovary Syndrome: The Role of Illness Perceptions. Women’s Health Issues 2020, 31, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Akdağ Cirik, D.; Dilbaz, B.; Aksakal, S.; Kotan, Z.; Özelçi, R.; Akpinar, F.; Mollamahmutoğlu, L. Do anxiety and depression statuses differ in differentpolycystic ovary syndrome phenotypes? Turk. J. Med. Sci. 2016, 46, 1846–1853. [Google Scholar] [CrossRef]
- Benson, S.; Hahn, S.; Tan, S.; Mann, K.; Janssen, O.; Schedlowski, M.; Elsenbruch, S. Prevalence and implications of anxiety in polycystic ovary syndrome: Results of an internet-based survey in Germany. Hum. Reprod. 2009, 24, 1446–1451. [Google Scholar] [CrossRef]
- Sukhapure, M.; Eggleston, K.; Fenton, A.; Frampton, C.; Porter, R.J.; Douglas, K.M. Changes in Mood, Anxiety, and Cognition with Polycystic Ovary Syndrome Treatment: A Longitudinal, Naturalistic Study. Neuropsychiatr. Dis. Treat. 2022, 18, 2703–2712. [Google Scholar] [CrossRef]
- Fatemeh, B.; Shahideh, J.S.; Negin, M. Health related quality of life and psychological parameters in different polycystic ovary syndrome phenotypes: A comparative cross-sectional study. J. Ovarian Res. 2021, 14, 57. [Google Scholar] [CrossRef]
- Dag, O.; Alpua, M.; Isik, Y.; Buturak, S.V.; Tulmac, O.B.; Turkel, Y. The evaluation of temperament and quality of life in patients with polycystic ovary syndrome. Gynecol. Endocrinol. 2017, 33, 250–253. [Google Scholar] [CrossRef]
- Veltman-Verhulst, S.M.; Boivin, J.; Eijkemans, M.J.C.; Fauser, B.J. Emotional distress is a common risk in women with polycystic ovary syndrome: A systematic review and meta-analysis of 28 studies. Hum. Reprod. Update 2012, 18, 638–651. [Google Scholar] [CrossRef]
- Sadeeqa, S.; Mustafa, T.; Latif, S. Polycystic Ovarian Syndrome-Related Depression in Adolescent Girls: A Review. J. Pharm. Bioallied Sci. 2018, 10, 55–59. [Google Scholar] [CrossRef]
- Fekadu, N.; Shibeshi, W.; Engidawork, E. Major depressivedisorder: Pathophysiology and clinical management. J. Depress. Anxiety 2017, 6, 1. [Google Scholar] [CrossRef]
- Miller, A.H.; Haroon, E.; Felger, J.C. TherapeuticImplications of Brain-ImmuneInteractions: Treatment in Translation. Neuropsychopharmacology 2017, 42, 334–359. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Morreale, H.F.; Luque-Ramírez, M.; González, F. Circulating inflammatory markers in polycysticovary syndrome: A systematic review and meta analysis. Fertil. Steril. 2011, 95, 1048–1058. [Google Scholar] [CrossRef]
- Nathan, R.S.; Sachar, E.J.; Asnis, G.M.; Halbreich, U.; Halpern, F.S. Relative insulin insensitivity and cortisolsecretion in depressedpatients. Psychiatry Res. 1981, 4, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Kolhe, J.V.; Chhipa, A.S.; Butani, S.; Chavda, V.; Patel, S.S. PCOS and Depression: Common Links and Potential Targets. Reprod. Sci. 2022, 29, 3106–3123. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.L.; US Preventive Services Task Force (USPSTF). Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 380. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.; Gibson-Helm, M.; Norman, R.J.; Boyle, J. Polycystic Ovary Syndrome: Perceptions and Attitudes of Women and Primary Health Care Physicians on Features of PCOS and Renaming the Syndrome. J. Clin. Endocr. 2014, 99, E107–E111. [Google Scholar] [CrossRef]
- Colwell, K.; Lujan, M.E.; Lawson, K.L.; Pierson, R.A.; Chizen, D.R. Women’s Perceptions of Polycystic Ovary Syndrome Following Participation in a Clinical Research Study: Implications for Knowledge, Feelings, and Daily Health Practices. J. Obstet. Gynaecol. Can. 2010, 32, 453–459. [Google Scholar] [CrossRef]
- Shrivastava, Y.; Jagdev, P. A Study to assess the Effectiveness of self Instructional module on Knowledge regarding Polycystic Ovarian Syndrome among B. Sc. Nursing students of Selected nursing college. Asian J. Nurs. Educ. Res. 2019, 9, 388. [Google Scholar] [CrossRef]
- Abdollahi, L.; Mirghafourvand, M.; Babapour, J.K.; Mohammadi, M. Effectiveness of cognitive-behavioral therapy (CBT) in improving the quality of life and psychological fatigue in women with polycystic ovarian syndrome: A randomized controlled clinical trial. J. Psychosom. Obstet. Gynaecol. 2019, 40, 283–293. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Application of the Criteria on the Present Study |
|---|---|
| Population | Adult and pre-menopausal women with PCOS |
| Intervention | None |
| Comparison | Studies included both with and without control group (healthy women) |
| Outcomes | Group size; depression measured by HADS-D score; relative risk of depression |
| Study Design | Case–control, cross-sectional, prospective and retrospective studies written in English |
| Study (Year) | Country | Number of Patients | PCOS Patients’ Age | |
|---|---|---|---|---|
| PCOS | Control | |||
| Altuntaş (2022) [6] | Turkey | 167 | 73 | 25.87 ± 5.64 |
| Karsten (2021) [7] | Netherlands | 73 | 100 | 34.1 ± 4.1 |
| Deeks (2010) [15] | Australia | 48 | - | 32.5 ± 7.98 |
| Dybciak (2022) [16] | Poland | 230 | 199 | 20–40 |
| Sheikh (2021) [17] | United Kingdom | 502 | - | - |
| Radhakrishnan (2018) [19] | India | 100 | - | 16–36 |
| Tariq (2021) [20] | Pakistan | 135 | 135 | 15–45 |
| Kogure (2019) [33] | Brazil | 120 | - | 28.8 ± 5.2 |
| Bazarganipour (2013) [34] | Iran | 300 | - | 26.56 ± 4.44 |
| Batool (2016) [35] | Pakistan | 137 | 137 | 25.0 ± 8.6 |
| Barry (2011) [37] | United Kingdom | 76 | 49 | 28.8 ± 4.81 |
| Saxena (2022) [42] | India | 70 | - | 25.7 ± 7.6 |
| Alur-Gupta (2021) [43] | United States of America | 272 | - | Median 28.9 |
| Light (2020) [44] | United Kingdom | 487 | - | 30.81 ± 7.65 |
| Cirik (2016) [45] | Turkey | 101 | 49 | 24.44 ± 4.23 |
| Benson (2010) [46] | Germany | 448 | - | 29.6 ± 5.5 |
| Sukhapure (2022) [47] | New Zealand | 33 | 41 | 29.24 ± 6.81 |
| Fatemeh (2021) [48] | Iran | 239 | - | 30.92 ± 5.49 |
| Dag (2019) [49] | Turkey | 53 | 38 | 22.69 ± 4.54 |
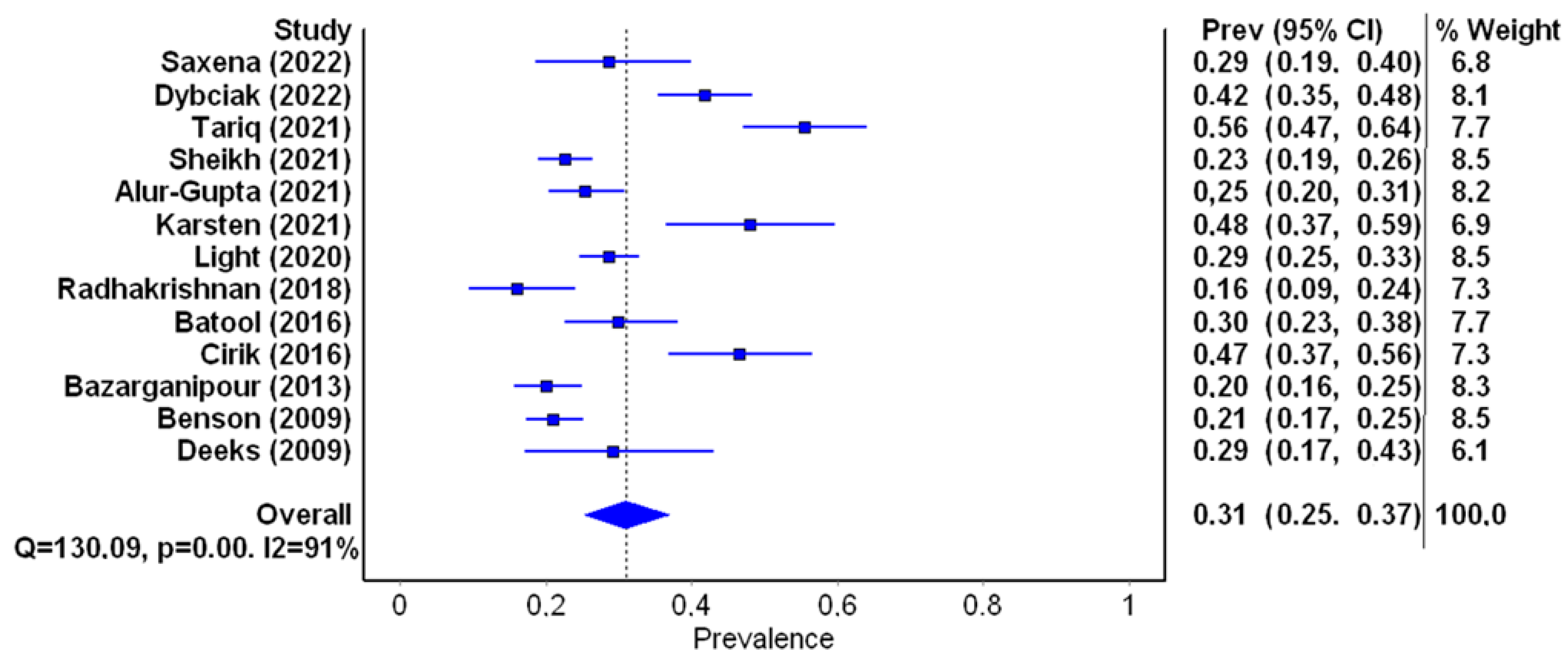
| Study (Year) | Number of Patients and Country | Age (Mean ± SD Years) | Depression (%) | Citation |
|---|---|---|---|---|
| Karsten (2021) | 73 The Netherlands | 34.1 ± 4.1 | 47.9% 35/73 | [7] |
| Deeks (2010) | 48 Australia | 32.5 ± 7.98 | 29.2% 14/48 | [15] |
| Dybciak (2022) | 230 Poland | Not specified | 41.7% 96/230 | [16] |
| Sheikh (2021) | 502 UK | Not specified | 22.5% 113/502 | [17] |
| Radhakrishnan (2018) | 100 India | Not specified | 16% 16/100 | [19] |
| Tariq (2021) | 135 Pakistan | Not specified | 55.6% 75/135 | [20] |
| Bazarganipour (2013) | 300 Iran | 26.56 ± 4.44 | 20% 60/300 | [34] |
| Batool (2016) | 137 Pakistan | 25.0 ± 8.6 | 30% 41/137 | [35] |
| Alur-Gupta (2021) | 272 USA | Median 28.9 | 25.4% 69/272 | [40] |
| Saxena (2022) | 70 India | Not specified | 28.5% 20/70 | [42] |
| Light (2020) | 487 UK | 30.81 ± 7.65 | 23.8% 116/487 | [44] |
| Cirik (2016) | 101Turkey | 24.44 ± 4.23 | 46.5% 47/101 | [45] |
| Benson (2010) | 448 Germany | 29.6 ± 5.5 | 21% 94/448 | [46] |
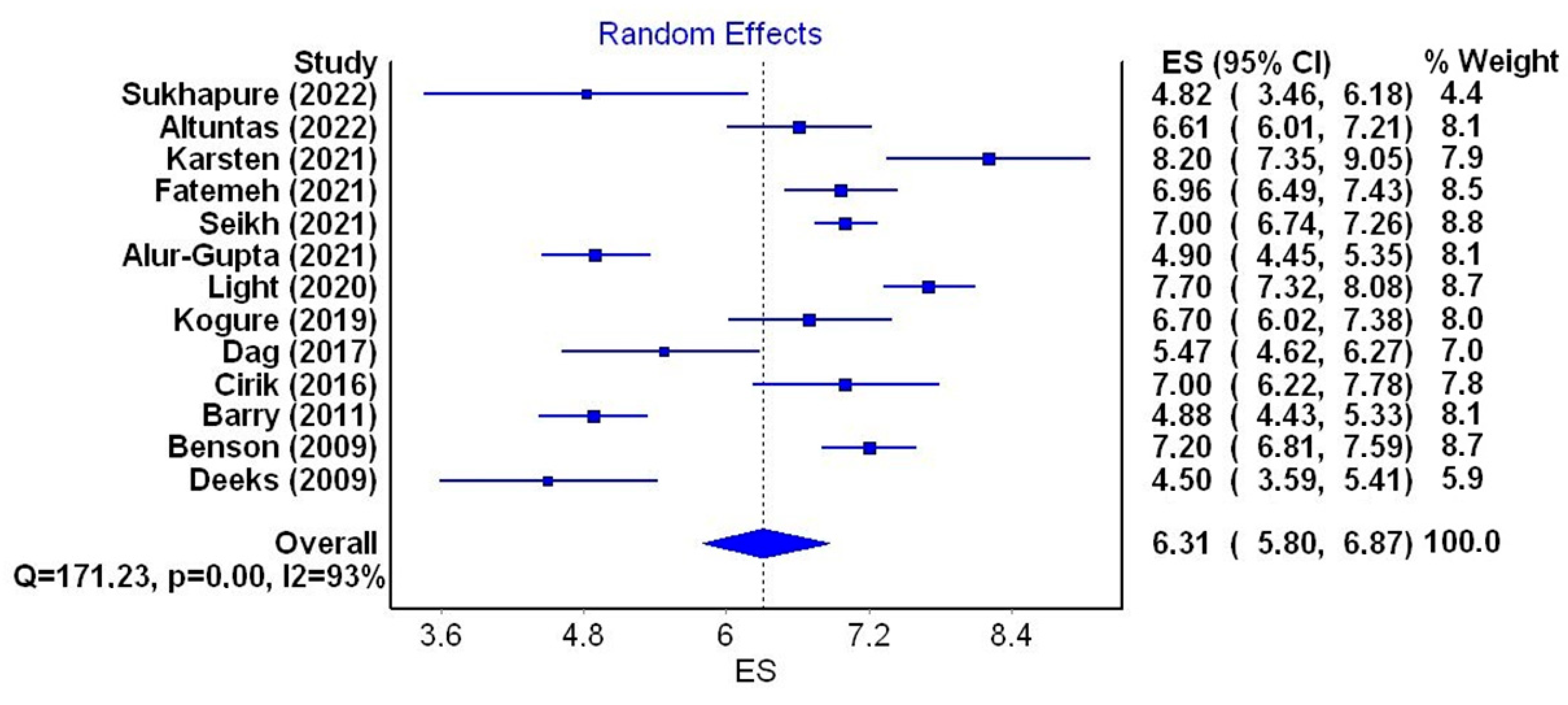
| Study (Year) | Number of Patients/Country | Age (Mean ± SD Years) | HADS-D Score (Mean ± SD) | Citation |
|---|---|---|---|---|
| Altuntaş (2022) | 167 Turkey | 25.87 ± 5.64 | 6.61 ± 3.99 | [6] |
| Karsten (2021) | 73 The Netherlands | 34.1 ± 4.1 | 8.2 ± 3.7 | [7] |
| Deeks (2010) | 48 Australia | 32.5 ± 7.98 | 4.5 ± 3.2 | [15] |
| Sheikh (2021) | 502 UK | Not specified | 7 ± 3.0 | [17] |
| Kogure (2019) | 120 Brazil | 28.8 ± 5.2 | 6.7 ± 3.8 | [33] |
| Barry (2011) | 487 UK | 28.8 ± 4.81 | 4.88 ± 1.98 | [37] |
| Alur-Gupta (2021) | 272 USA | Median 28.9 | 4.9 ± 3.8 | [43] |
| Light (2020) | 487 UK | 30.81 ± 7.65 | 7.7 ± 4.3 | [44] |
| Cirik (2016) | 101 Turkey | 24.44 ± 4.23 | 7.0 ± 4.0 | [45] |
| Benson (2009) | 120 Brazil | 29.6 ± 5.5 | 7.2 ± 4.2 | [46] |
| Sukhapure (2022) | 33 New Zealand | 29.24 ± 6.81 | 4.82 ± 4.0 | [47] |
| Fatemeh (2021) | 239 Iran | 30.92 ± 5.49 | 6.96 ± 3.73 | [48] |
| Dag (2017) | 53 Turkey | 22.69 ± 4.54 | 5.47 ± 2.97 | [49] |
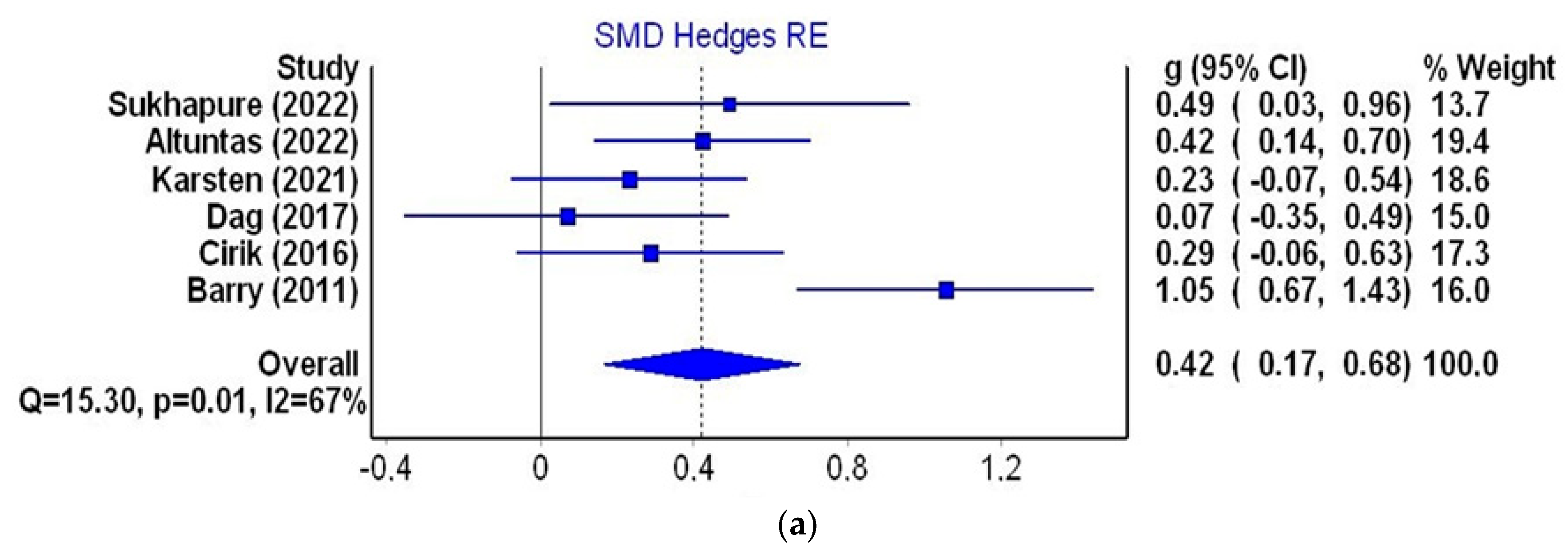
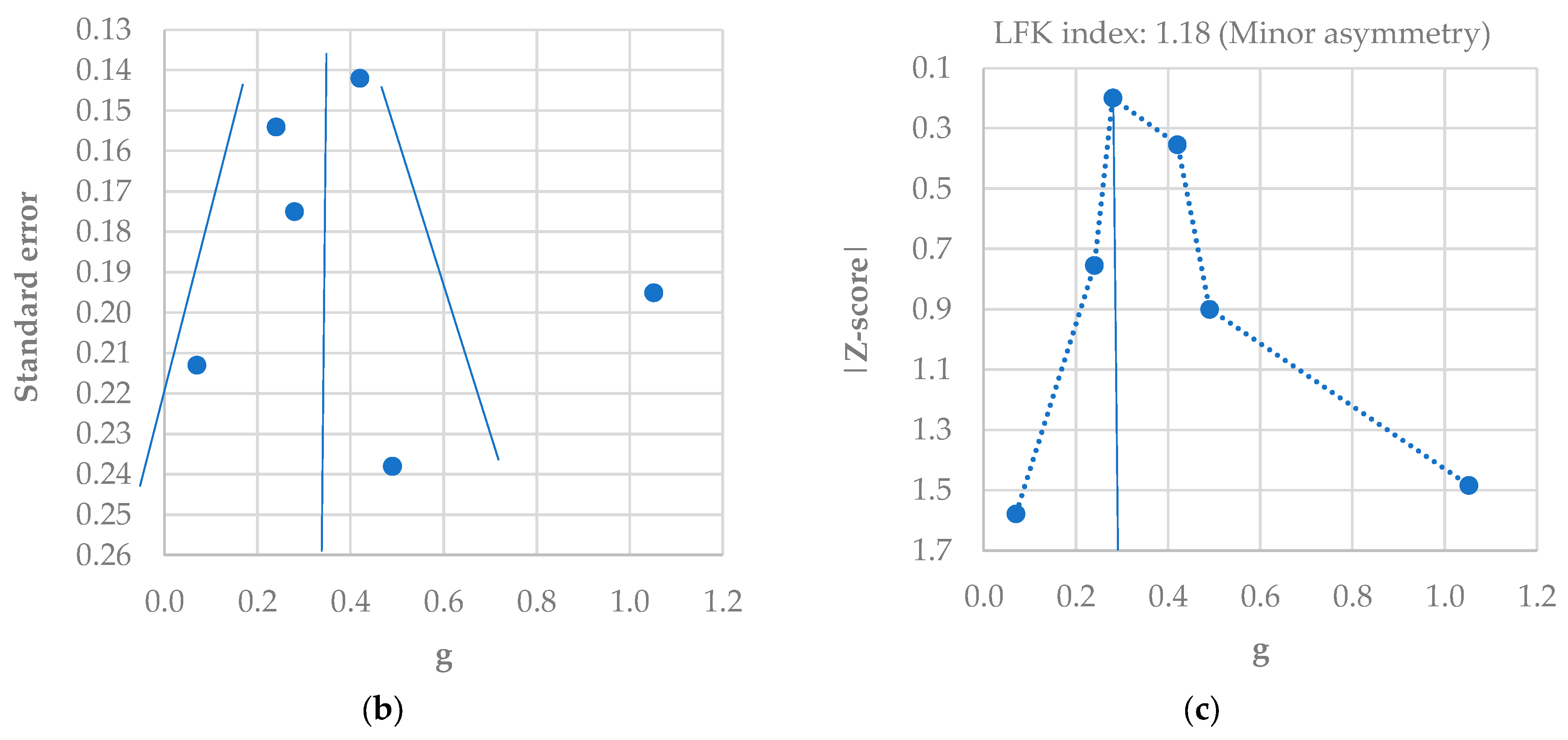
| Study (Year) Country | Number of Cases | Age (Years) (Mean ± SD) | HADS-D Score (Mean ± SD) | SMD (Hedge’s g) | Citation |
|---|---|---|---|---|---|
| Altuntaş (2022) Turkey | Study group—167 | 25.87 ± 5.64 | 6.61 ± 3.99 | 0.422 | [6] |
| Control—73 | 27.25 ± 5.85 | 4.99 ± 3.41 | |||
| Karsten (2021) Netherlands | Study group—73 | 34.1 ± 4.1 | 8.2 ± 3.7 | 0.233 | [7] |
| Control—100 | 35.1 ± 3.7 | 7.4 ± 3.2 | |||
| Barry (2011) UK | Study group—76 | 28.8 ± 4.81 | 4.88 ± 1.98 | 1.052 | [37] |
| Control—49 | 35.12 ± 4.37 | 2.76 ± 2.04 | |||
| Cirik (2016) Turkey | Study group—101 | 24.44 ± 4.23 | 7.0 ± 4.0 | 0.286 | [45] |
| Control—49 | 26.29 ± 5.17 | 6.0 ± 2.0 | |||
| Sukhapure (2022) New Zealand | Study group—33 | 29.24 ± 6.81 | 4.82 ± 4.0 | 0.492 | [47] |
| Control—41 | 29.29 ± 8.62 | 3.0 ± 3.36 | |||
| Dag (2017) Turkey | Study group—53 | 22.69 ± 4.54 | 5.47 ± 2.97 | 0.070 | [49] |
| Control—38 | 21.34 ± 2.12 | 5.23 ± 3.96 |
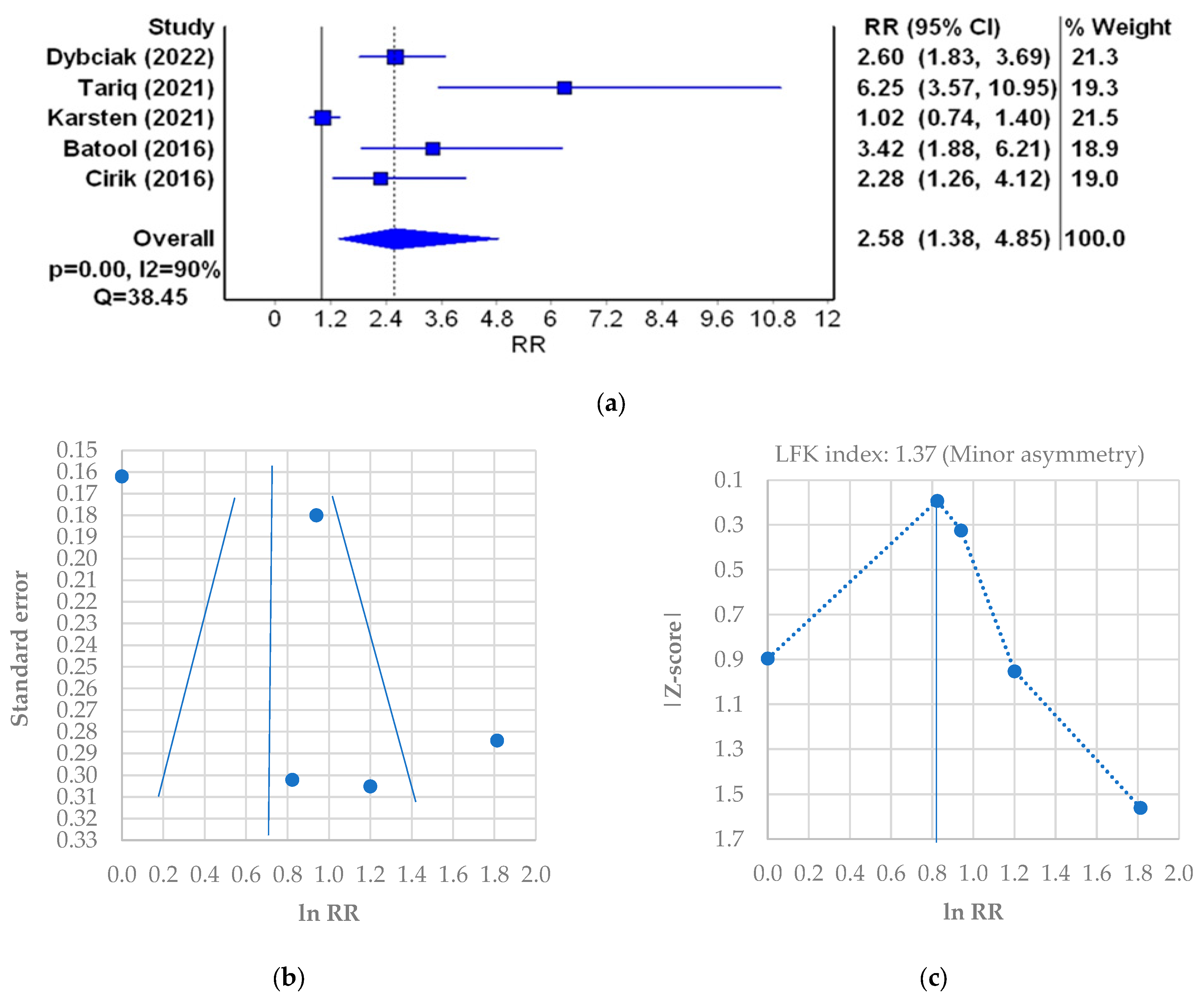
| Study (Year)/Country | PCOS (Active/Cases) | Control (Active/Cases) | RR [95%CI] | Citation |
|---|---|---|---|---|
| Karsten (2021)/UK | 47.9% (35/73) | 47% (47/100) | 1.02 [0.74–1.40] | [7] |
| Dybciak (2022)/Poland | 41.7% (96/230) | 16.1% (32/199) | 2.60 [1.83–3.69] | [16] |
| Tariq (2021)/Pakistan | 55.6% (75/135) | 8.9% (12/135) | 6.25 [3.57–10.95] | [20] |
| Batool (2016)/Pakistan | 30% (41/137) | 9% (12/137) | 3.42 [1.88–6.214] | [35] |
| Cirik (2016)/Turkey | 46.5% (47/101) | 20.4% (10/49) | 2.28 [1.26–4.12] | [45] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dybciak, P.; Raczkiewicz, D.; Humeniuk, E.; Powrózek, T.; Gujski, M.; Małecka-Massalska, T.; Wdowiak, A.; Bojar, I. Depression in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6446. https://doi.org/10.3390/jcm12206446
Dybciak P, Raczkiewicz D, Humeniuk E, Powrózek T, Gujski M, Małecka-Massalska T, Wdowiak A, Bojar I. Depression in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(20):6446. https://doi.org/10.3390/jcm12206446
Chicago/Turabian StyleDybciak, Paweł, Dorota Raczkiewicz, Ewa Humeniuk, Tomasz Powrózek, Mariusz Gujski, Teresa Małecka-Massalska, Artur Wdowiak, and Iwona Bojar. 2023. "Depression in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 20: 6446. https://doi.org/10.3390/jcm12206446
APA StyleDybciak, P., Raczkiewicz, D., Humeniuk, E., Powrózek, T., Gujski, M., Małecka-Massalska, T., Wdowiak, A., & Bojar, I. (2023). Depression in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(20), 6446. https://doi.org/10.3390/jcm12206446